Article Text

Abstract
Background: Anterior cruciate ligament (ACL) injury is a devastating injury that puts an athlete at high risk of future osteoarthritis. Identification of risk factors and development of ACL prevention programmes likely decrease injury risk. Although studies indicate that sagittal plane biomechanical factors contribute to ACL loading mechanisms, it is unlikely that non-contact ACL injuries occur solely in a sagittal plane. Some authors attempt to ascribe the solely sagittal plane injury mechanism to both female and male ACL injuries and rebuff the concept that knee “valgus” is associated with isolated ACL injury. Prospective studies that utilise coupled biomechanical and epidemiological approaches demonstrated that frontal knee motions and torques are strong predictors of future non-contact ACL injury risk in female athletes. Video analysis studies also indicate a frontal plane “valgus collapse” mechanism of injury in women. As load sharing between knee ligaments is complex, frontal as well as sagittal and transverse plane loading mechanisms likely contribute to non-contact ACL injury. The purpose of this review is to summarise existing evidence regarding ACL injury mechanisms and to propose that sex-specific mechanisms of ACL injury may occur, with women sustaining injuries by a predominantly “valgus collapse” mechanism.
Conclusion: Prevention programmes and interventions that only target high-risk sagittal plane landing mechanics, especially in the female athlete, are likely to be less effective in ameliorating important frontal and transverse plane contributions to ACL injury mechanisms and could seriously hamper ACL injury prevention efforts. Programmes that target the reduction of high-risk valgus and sagittal plane movements will probably prove to be superior for ACL injury prevention.
Statistics from Altmetric.com
Anterior cruciate ligament (ACL) injuries place an athlete at greatly increased risk of developing knee osteoarthritis later in life. In addition to knee pain and instability, ACL injury may cause a substantial financial burden and lead to long-term disability for young athletes. Using a conservative cost of US$17 000 per patient for surgery and rehabilitation, the estimated cost for treatment in ACL-injured patients in the USA is over 1.7 billion dollars annually.1 2 Although many advances have been made in terms of surgical and rehabilitation interventions for ACL-injured patients, long-term outcome studies show that these patients are at a high risk of developing osteoarthritis 10–15 years after ACL injury, regardless of the treatment.3–5 Identification of high-risk manoeuvres that lead to ACL injury would aid in the development of neuromuscular training programmes targeted at decreasing dangerous knee loading patterns and preventing ACL injury.
It is well established that women have a higher risk of ACL injury, and ACL studies have often focused on the determination of differences between the sexes that may increase a female athlete’s risk of injury.6 7 Whereas anatomical, hormonal and neuromuscular differences may be observed between the sexes,8 it remains a challenge to correlate what is studied in the laboratory setting to what actually occurs during an ACL injury event, and it may not follow that these sex differences are the underlying cause of increased ACL injury risk in women. There is even evidence to indicate that women may injure their ACL by an entirely different mechanism than men.9 10
WHAT IS THE INCITING EVENT IN NON-CONTACT ACL INJURY?
A great deal of controversy and current research surrounds the inciting event and the biomechanical mechanisms underlying non-contact ACL injury. Whereas the intrinsic and extrinsic risk factors for ACL injury have been explored extensively, the factors surrounding the inciting event and the biomechanical mechanisms underlying non-contact ACL injury require greater analysis. Methods to describe ACL loading and injury mechanisms have included athlete interviews, in-vivo arthroscopic, clinical, video analysis, cadaveric, motion analysis, electromyographic and mathematical modelling studies. However, these studies have provided contradictory and inconclusive results and thus widely varying interpretations as to the inciting event.9
Observational studies indicate that most non-contact ACL injuries occur during lateral pivoting, landing or deceleration manoeuvres during sports play.11 However, the planes of knee motion that lead to non-contact ACL injury are not completely clear and remain a controversial issue in the literature. Video studies of ACL injuries provide evidence that supports two predominant loading patterns: injury as a result of knee valgus collapse (a combination of knee valgus, hip internal rotation and tibial rotation) or by anterior tibial shear (although the biomechanical evaluation of anterior tibial shear by video analysis is difficult).9–13
The ACL provides approximately 85% of the knee joint’s total restraint to anterior tibial translation at 20–30° of knee flexion14–17 and as studies have shown that sagittal plane knee angles near full extension and large quadriceps muscle forces increase ACL loading, many clinicians support a predominantly sagittal plane ACL injury mechanism.18 In contrast, pure frontal (valgus–varus) or transverse (internal–external) plane knee loads have a less obvious effect on ACL strain, and the MCL, not the ACL, is reportedly the primary restraint against valgus stress in the knee joint.14 19 In contrast to this accepted dogma, both in-vivo biomechanical data and video analyses indicate that increased lower extremity valgus loads and movements in the frontal plane are probably associated with an increased risk of ACL injury.11 20 21 Although the ACL may be subject to large forces during various loading conditions,22 load sharing among knee joint ligaments is complex and there is strong evidence that non-contact ACL injuries likely occur as a result of increased motion and loading in the sagittal, frontal, transverse and/or multiplanar conditions.9–11 22–27 The purpose of this review is to highlight the evidence for a frontal plane (“valgus collapse”) mechanism, because of its important implications for relative risk prediction and ACL intervention programmes.
VALGUS COLLAPSE MECHANISM: A MORE RECENT DISCOVERY AND PROBABLE MECHANISM OF INJURY IN WOMEN
“Valgus” refers to the outward angulation of the distal segment of a bone or joint. At the knee joint, valgus may occur from a pure abduction motion of the distal tibia relative to the femur or from transverse plane knee rotation motions (femoral/tibial internal and external rotations). Hollis and colleagues28 described the axial rotation of the tibia relative to the femur during a “valgus” load application and found that at increasing knee flexion angles, the internal tibial rotation increased with a maximum of up to 21° of rotation at 90° of flexion. Therefore, describing an injury mechanism as a valgus collapse does not necessarily indicate that the injury occurs solely in the frontal plane and contributions of other planar movements should also be considered.
Typical postures at the time of ACL injury
Non-contact ACL injuries often exhibit a common body posture that involves a valgus collapse of the knee joint, with the knee near full extension (between 0° and 30°), external tibial rotation with the foot planted during a deceleration manoeuvre.9 11 Video studies by Olsen et al21 and Krosshaug et al9 found that dynamic valgus collapse was the most common ACL injury mechanism for female handball and basketball athletes. Krosshaug et al9 also found that female basketball players demonstrated a 5.3 times higher relative risk of valgus collapse during ACL injury compared with male basketball players.
Female athletes exhibit more knee valgus motion and torque during athletic movements than men and these altered mechanics are predictors of future ACL injury risk.20 29–32 We prospectively screened athletes before their athletic seasons and discovered that during landing, athletes who went on to experience ACL injury had knee valgus angles more than 8° greater than athletes who completed the season uninjured. Our preseason measure of dynamic valgus moments predicted ACL injury with 73% sensitivity and 78% specificity.20
It is conceivable that men and women have different primary underlying mechanisms of ACL injury, with women experiencing more injuries as a result of valgus collapse than men (figs 1 and 2). Over 50% of the women in a Norwegian handball study demonstrated a valgus knee collapse during the injury event, whereas only 20% of the men showed a similar collapse.9 A recent study by Boden et al10 corroborated these findings, showing that women had higher valgus angles than their male counterparts during ACL injury.10 Mathematical modelling studies demonstrate that perturbations to the lower extremity during a side-step cutting manoeuvre can lead to external valgus loads that are capable of rupturing the ACL and these valgus loads occur more frequently in women than men.33 34

Multiplanar loading mechanism in women.

More sagittal plane-oriented loading mechanism in men?
What additional evidence is there that valgus collapse is an important contributor to ACL injury?
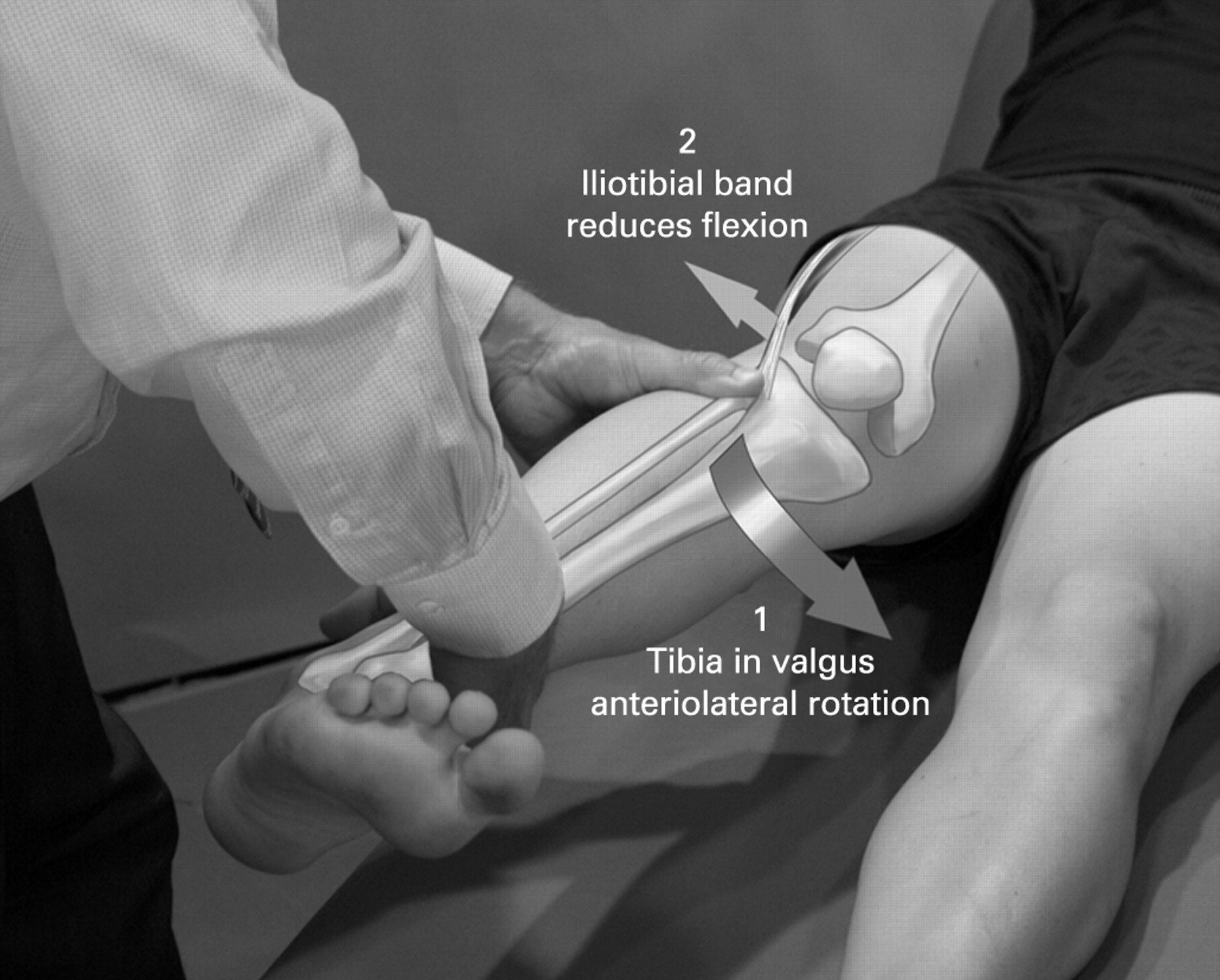
Consider how clinical tests of knee stability parallel the forces that potentially occur at the knee during an inciting event. The Lachman’s and anterior drawer tests indicate the importance of the ACL in restraining anterior tibial translation. Similarly, the pivot shift test (fig 3) is the most specific clinical test for ACL deficiency; it has 98% specificity (95% CI 96 to 99).35 When comparing the relative importance of these motions, note that ACL-deficient patients can generally function well when they limit themselves to sagittal plane movements; however, rotational movements often lead to feelings of instability and symptomatic “giving way” episodes. The pivot shift test stresses the rotational restraint of the ACL and a large pivot shift predicts a poor outcome following injury.36 We postulate that the pivot shift probably reproduces the luxations that occur during an ACL injury.
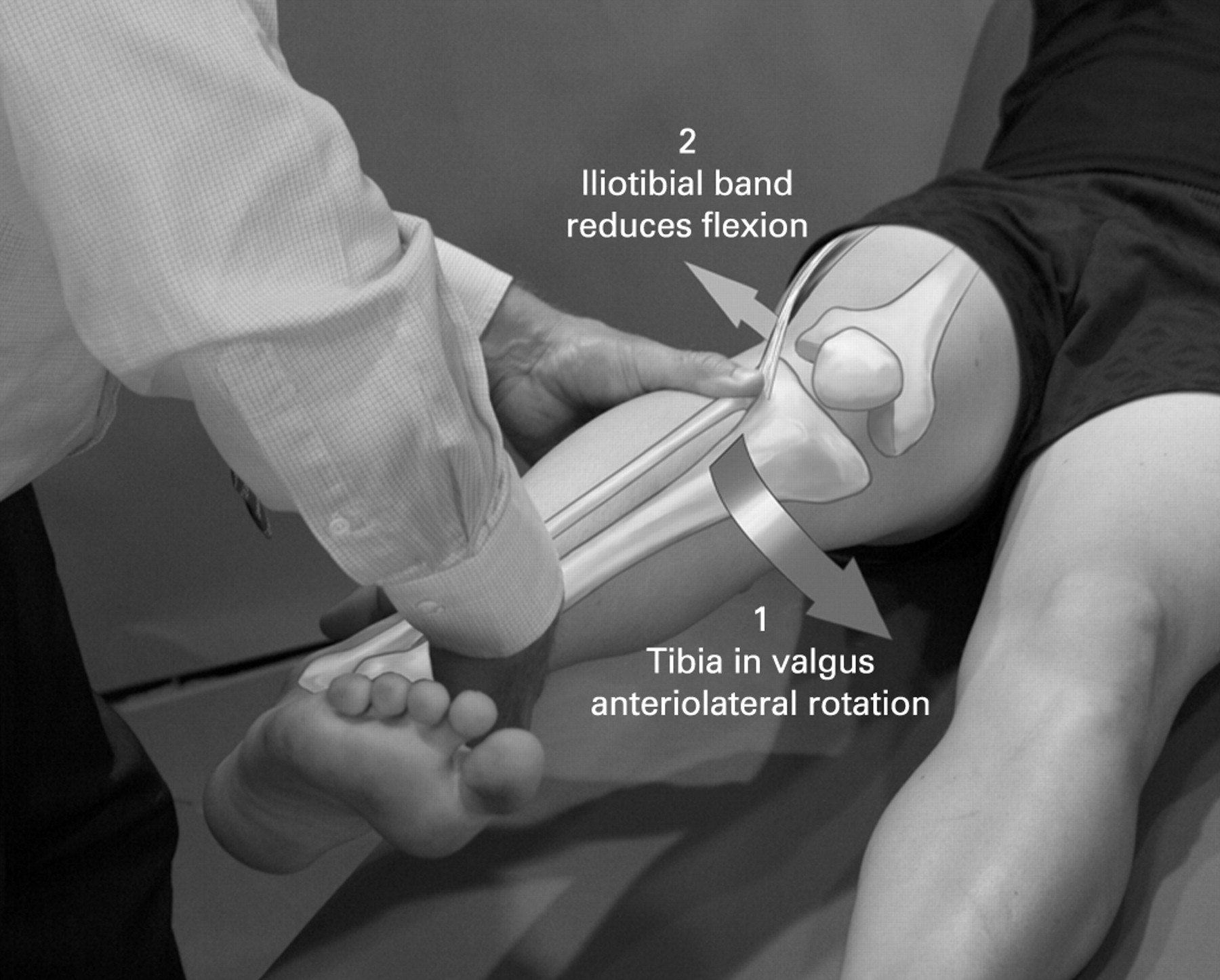
The pivot shift test is performed with the patient lying supine with their hip passively flexed to 30°. Approximately 20° of internal rotation is applied to the tibia and the knee is placed in full extension. A valgus force is applied to the knee as it is slowly flexed. An anterior cruciate ligament-deficient knee will remain reduced in full extension but will sublux around 20–30° of knee flexion and then will reduce again in deeper flexion.
Clinical imaging and diagnostic studies also indicate that valgus collapse probably occurs during ACL injury. Bone bruises of the lateral femoral condyle or posterolateral portions of the tibial plateau occur approximately 80% of the time in magnetic resonance imaging (MRI) studies after acute ACL injury (fig 4).37–40 Lateral tibial and femoral bone bruises associated with acute ACL injuries indicate that compression occurs laterally while the medial aspect of the joint unloads. Posterior tibial plateau bone bruises could result from internal tibial rotation, femoral external rotation, abduction and/or anterior tibial translation.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
(A) Magnetic resonance imaging of bone bruise pattern (lateral femoral condyle and posterolateral tibial plateau) associated with acute anterior cruciate ligament (ACL) injury. (B) Femoral and tibial articulation pressure distribution during simulated ACL injury mechanism as a result of combined valgus and anterior tibial translation. (C) Posterolateral tibial plateau and (D), (E) lateral femoral condyle articular pressure distribution patterns. The sections for the tibia and femur are divided into anterior lateral (AL), middle lateral (ML), posterior lateral (PL), anterior medial (AM), middle medial (MM) and posterior medial (PM).
Adding to the argument that there may be sex-specific mechanisms of injury, Fayad et al41 reported that women more commonly acquired posterolateral tibial bone bruises after ACL injury, whereas men had more medial meniscus, lateral collateral ligament and posterior cruciate ligament injuries. This sex difference in concomitant injuries associated with ACL ruptures is consistent with women having more valgus-driven injury mechanisms and men experiencing more sagittal plane-oriented ACL injury mechanisms. As women demonstrate greater knee valgus postures and moments compared with men during jumping, landing and cutting activities, their risk of dangerous knee valgus mechanics is elevated.42 43
An underrecognised, but unmodifiable factor that may increase the risk of ACL injury as a result of valgus collapse is the slope of the posterior tibial plateau. ACL-injured patients may have greater posterior lateral tibial plateau slopes compared with controls (but not medial tibial slopes). This may predispose them to more transverse plane rotation during high-risk manoeuvres.44 Both Kujala et al45 and Brandon et al46 found that greater posterior tibial slopes were associated with higher pivot shift grades and an increased likelihood of experiencing symptomatic giving way episodes in ACL-deficient patients. Therefore, a large posterior tibial plateau slope combined with greater lateral femoral condylar translation on the tibia compared with the medial condyle increases the likelihood of transverse plane rotations and probably increases an individual’s risk of ACL injury as a result of valgus collapse.47
Several cadaveric studies demonstrate that the ACL experiences increased force during valgus loads.22 48 Quadriceps force coupled with a valgus load increases the ACL force up to 100% compared with valgus loads without a quadriceps force.22 Similarly, coupled valgus loading with anterior tibial force leads to higher ACL forces and strains than isolated anterior tibial force.48 Withrow et al49 demonstrated that valgus knee alignment led to 30% greater ACL strains compared with knees in neutral alignment when subjected to impulsive compression loads.
Why is there controversy in the literature regarding a “valgus collapse” mechanism?
In a recent review paper, Yu and Garrett18 disputed the idea that knee abduction could be associated with isolated ACL injury. They argued that “valgus” cannot cause ACL injuries, because they believe that the ACL is not the major load-bearing structure during valgus loads. Yu and Garrett18 also questioned the validity of our prospective coupled biomechanical–epidemiological studies that demonstrated that knee abduction was a strong predictor of future non-contact ACL injury risk in female athletes. However, we did not claim that the ACL injury was caused by a “pure” valgus mechanism. Our experimental analysis demonstrated a strong and clear association between prospectively measured variables, knee abduction motion and torque, and subsequent ACL injuries in female athletes. These observations may be interpreted in different ways, but the statistical and clinical significance of this association is well established in the peer-reviewed literature. Yu and Garrett18 may be correct in supporting a primarily “sagittal plane” ACL injury mechanism for male athletes. However, ignoring the increasing evidence for valgus collapse as a mechanism for injury, especially in female athletes, could seriously impede ACL injury intervention efforts if dangerous frontal plane biomechanics are ignored in prediction and prevention programmes.
Are studies of non-weightbearing ACL strain and isolated bundles relevant?
Yu and Garrett18 suggested that in-vivo arthroscopic ACL strain measurements indicate that passive valgus torques or external tibial rotations do not significantly increase strains in the ACL.50 However, weightbearing conditions can significantly increase the ACL strain (2–4%) during external tibial torques in the range 0–10 Nm. As ACL injuries occur during weightbearing conditions, it may be feasible that an external rotation torque could damage the ACL.50 Although a passive valgus torque during weightbearing conditions increases ACL strain compared with non-weightbearing conditions, the strain remains relatively constant over a wide range of torques.
It is important to note that the strain in the posteromedial ACL bundle cannot be measured using current arthroscopic techniques. Cadaveric studies indicate that when a valgus load is applied to the knee joint from 0° to 90° of knee flexion, the posterolateral ACL bundle shows a nearly fourfold greater change in length compared with the anteromedial bundle.28 Therefore, measuring only the anteromedial bundle of the ACL may not appropriately assess the amount of strain that occurs in the total ACL during a valgus load.
Why are not more medial collateral ligament injuries associated with non-contact ACL injuries?
As Yu and Garrett18 pointed out in their review, clinical observation and epidemiology studies suggest that concomitant ACL/medial collateral ligament (MCL) injuries are relatively rare and occur in less than 30% of total ACL injuries.1 51 52 Therefore, the valgus motion and torque at the knee joint that are associated with increased ACL injury risk may present a conundrum to clinicians and researchers. The predominance of isolated ACL injury during non-contact mechanisms is a challenge for clinicians to explain. If non-contact ACL injuries occur as a result of valgus collapse of the knee joint, higher combined ACL/MCL injury patterns would be expected, particularly in women.
The ACL and MCL both provide restraint to external valgus. Cadaveric studies show that the ACL appears to restrain knee valgus by limiting axial tibial rotation, whereas the MCL restrains knee valgus by limiting medial joint space opening.53 At low flexion angles, ACL deficiency produces greater increases in knee valgus rotation than isolated MCL deficiency. However, medial joint space opening in ACL-deficient knees is relatively small compared with the medial joint space opening in MCL-deficient knees.53 Therefore, both the ACL and MCL are important restraints to valgus loads and either one may potentially be injured during high knee valgus loading.
Depending upon the age of the specimen, rate and orientation of loading, ACL failure loads are reported to range from approximately 640 to 2100 Newtons (N).54–56 In contrast, cadaveric MCL failure loads have been reported to be as high as 2300 N for complete MCL disruption.57 These disparities in relative failure loads may help to explain why the ACL may fail earlier than the MCL during external valgus loading. In addition, the reported cadaveric failure loads were determined by applying pure distraction to each ligament individually, with loads applied along the fibre lines. During pure valgus loading, the MCL takes stress along its fibre lines, whereas the ACL may be loaded in a suboptimal orientation to handle high stresses. Mommersteeg et al58 found that orientation of loading at the knee is more critical in the cruciate ligaments compared with the collaterals and that loading orientation may affect the tensile stiffness of the ACL. Mommersteeg and colleagues59 also showed that collagen density is different between human ACL and MCL, with the ACL showing significantly lower collagen density compared with the MCL. Variations in collagen density have been shown to correspond to differences in Young’s modulus for the ACL and MCL.60 Therefore, even if the MCL is the primary restraint to an external valgus load, suboptimal orientation loading and collagen property differences may place the ACL at risk of failure before the MCL.
Few studies have examined ACL and MCL loading concurrently during a valgus load, and cross-referencing of studies to determine how the ACL and MCL behave simultaneously is complex due to the variability in laxity between specimens and different testing conditions. Yasuda et al61 demonstrated that during a valgus impact load, the ACL and MCL never elongated simultaneously during impact, and the time to peak elongation in the MCL occurred before the ACL at full extension. In contrast, at 30° of knee flexion, the ACL reached maximum elongation approximately 16 ms earlier than the MCL. As ACL injury probably occurs near initial foot contact (within the first 50 ms after contact) with the ground,9 a longer time to peak elongation could potentially explain how the ACL becomes at risk before the MCL during a valgus load. Shin et al62 conducted a modelling study that found that the MCL may only resist valgus loading effectively after some degree of medial joint opening. Valgus collapse that incorporates transverse plane rotations or that is combined with anterior tibial translations before the medial joint opens enough to strain the MCL may thus also potentially explain how the ACL could tear without MCL injury.22 48
Despite the epidemiological evidence that combined ACL/MCL injuries are relatively less common than isolated injuries,1 51 52 combined ACL/MCL injuries may be underreported or underdiagnosed. A valgus load sufficient to rupture the ACL may not result in observable injury to the MCL. Cellular damage may occur, but not at a level that may be indicated by clinical examination, imaging or arthroscopy. In direct contrast to most imaging studies examining the incidence of ACL/MCL injury, Viskontas et al40 reported that 70% of ACL tears had associated grade 1–3 MCL injuries. The discrepancy between previous reports and the study by Viskontas et al40 may be due to the differences in the methods used to determine MCL injury. Many of the previous studies reporting ACL/MCL injuries did not include grade 1 injuries of the MCL or did not report injury grading schemes. Moreover, many studies relied exclusively on a clinical examination (valgus stress test) to determine injury to the MCL. Grood et al14 examined the ability of a valgus stress test to determine the “grade” of MCL injury and found that knees with complete MCL disruption only registered a motion increase of 5.5 mm; which by most clinical grading systems is a borderline grade 2 ligament injury (5–10 mm).
The clinical perception of a relatively low incidence of combined ACL/MCL injuries may be more related to the challenges of diagnosing minor sprains of the MCL compared with the more traumatic disruption of the ACL.63 The diagnostic sensitivity of an MRI for determining MCL injury is less than 60%, compared with the relatively high sensitivity (86%) and specificity (92%) for diagnosing an ACL injury.64 Whereas complete traumatic midsubstance ruptures of the ACL are common, complete MCL midsubstance disruptions are rare. The majority of diagnosed MCL injuries are partial ligament tears in which the MCL often splinters at the deep femoral or tibial insertions rather than sustaining midsubstance disruption. Moreover, the complex anatomy of the medial and posteromedial structures of the knee joint makes it difficult to determine isolated MCL injury. Previous studies that examined MCL injury have often differed in their description of MCL injury, with regard to the inclusion of superficial MCL, deep MCL structures and/or the posterior oblique ligament, as a result of the difficulty in differentiating between the structures during physical and imaging examinations.65 Also, clinicians may not be highly motivated to diagnose an MCL injury, especially a relatively minor sprain, with an ACL rupture because it does not significantly alter the course of treatment. The low reported incidence of combined ACL/MCL injury thus does not necessarily indicate that ACL injuries do not occur as a result of knee valgus collapse.
Cumulatively, and in direct contrast with the assertions of the review by Yu and Garrett,18 this evidence indicates that valgus collapse can potentially lead to non-contact ACL injury. As described above, the knee probably experiences high loading conditions simultaneously in multiple planes, particularly in sporting manoeuvres such as landing, jumping and cutting, all of which require movements in multiple planes. It is thus unlikely that a non-contact ACL injury occurs in a single isolated plane, especially in the female athlete.
SAGITTAL PLANE MECHANISM: UNLIKELY TO BE THE SOLE PLANAR ACL INJURY MECHANISM IN WOMEN
During sagittal plane movements at the knee joint, anterior shear force at the proximal end of the tibia through the patella tendon can be produced by quadriceps muscle contractions.24 66 Anterior shear of the proximal tibia relative to the femur directly loads the ACL, and sagittal plane knee angles near full extension (0–30° of flexion) increase this anterior tibial shear force.22 24 66 67 Theoretically, a powerful quadriceps force near full knee extension could thus produce enough anterior shear force at the tibia to cause ACL rupture.22 68
Cadaveric, diagnostic and in-vivo arthroscopy studies demonstrate that the ACL is a primary restraint to anterior shear loading14 16 22 and ACL-deficient knees have significantly more anterior tibial translation compared with ACL intact conditions.69 70 These findings indicate that a function of the ACL is to prevent sagittal plane translations, and large anterior tibial shear forces could potentially compromise the ACL. However, it is important to consider that most of these studies solely evaluated anterior tibial translation and did not consider other planes in the diagnostic evaluation. Publication biases towards the sagittal plane restraints of the ACL have driven many of the oversimplified assumptions of sagittal plane proponents to ACL injury.
The bone bruise data strongly contradict a solely sagittal plane mechanism of ACL rupture, most especially in women. As described above, bone bruises of the lateral femoral condyle or posterolateral portions of the tibial plateau are common after acute ACL injury, and these bone bruising patterns may indicate that the tibia shifts anteriorly relative to the femur during ACL injury.37–40 The slope of the tibial plateau may also contribute to sagittal plane ACL injury mechanisms, as pure compression across a tibial access with 5–15° of posterior slope could increase anterior tibial translation and ACL strain.46 Brandon et al46 found an association between increased posterior tibial slope and ACL injury. However, if the injury mechanism was solely as a result of anterior tibial shear, the bone bruise patterns on MRI after ACL injury would most likely be located along the medial tibial plateau as well as the lateral tibial plateau. As the bone bruises are most often located laterally, in addition to the posterior tibial pattern, lateral compression and valgus probably occur during these ACL injuries.
The relationship between the knee flexion angle and the potential for ACL injury has also been explored extensively in the literature. Interview and video studies indicate that ACL injury usually occurs at shallow (0–30°) knee flexion angles.9–12 21 71 72 Cadaveric studies show that the knee joint has the potential to translate more in the sagittal plane during shallow knee flexion angles, and anterior tibial shear forces generate the greatest ACL loads during 20–40° of knee flexion.22 69 73 At the same time, women have been suggested to have shallow knee flexion angles during landing, jumping and cutting tasks compared with men.31 74 75 However, other studies show no sex difference or even greater knee flexion in women during athletic tasks.30 76 77 Furthermore, the knee flexion angle at landing does not appear to predict ACL injury risk,20 and videos of ACL injuries indicate that women may have similar or even greater knee flexion angles than men during the injury event.9 10
What is already known on this topic
ACL injury is a common problem in young athletes. Identification of risk factors and the development of ACL prevention programmes may help decrease injury risk. Although studies indicate that sagittal plane biomechanical factors contribute to ACL loading mechanisms, it is unlikely that non-contact ACL injuries occur solely in a sagittal plane.
Many sports manoeuvres induce large quadriceps forces at relatively shallow knee flexion angles, which may increase anterior tibial shear and ACL strain.24 78–83 Isolated quadriceps contractions increase ACL strain and force during shallow knee flexion angles,79 81–83 and electromyographic studies show that women have significant neuromuscular imbalances between quadriceps and hamstrings recruitment, which create difficulty for deceleration from a landing and control of anterior tibial translation.84 85 Withrow et al86 showed that ACL strain is proportional to increased quadriceps forces during high impact loads. Strong quadriceps contraction can produce anterior tibial translation great enough to injure the ACL during shallow knee flexion angles.24 87 When a 4500 N quadriceps force was applied to cadaveric specimens, six of the 11 specimens sustained a partial or complete ACL rupture.24 However, quadriceps contraction appeared to affect ACL loading in more than one plane of motion, with knee internal rotation and valgus moments occurring coincident with anterior tibial translation.24 Cadaveric and mathematical modelling studies indicate that hamstrings co-contraction with quadriceps contraction can lead to joint compression, decrease anterior tibial translation and effectively reduce excessive forces in the ACL, particularly between 15° and 60° of knee flexion.66 88 89
Shin et al90 reported that large ground reaction forces directed posterior relative to the proximal tibia help protect the ACL during landing from a jump and during a run-to-stop simulation. Moreover, several mathematical models have demonstrated that sagittal plane mechanisms alone cannot account for ACL forces high enough to rupture the ACL.33 91 McLean and colleagues32–34 used forward dynamic musculoskeletal models to simulate random perturbations during cutting movements and found that peak anterior drawer forces never led to ACL forces high enough to cause ACL injury. Therefore, despite the evidence that sagittal plane mechanics can cause large ACL loads, it is highly unlikely that non-contact ACL injuries result exclusively from a sagittal plane mechanism (especially in the female athlete).
What this study adds
The purpose of this review is to summarise existing evidence about ACL injury mechanisms and to propose that sex-specific mechanisms of ACL injury may occur, with women sustaining injuries predominantly as a result of a “valgus collapse” mechanism.
ACL INJURY PREVENTION PROGRAMMES
There is increasing evidence that neuromuscular training programmes can reduce the risk of ACL injury.8 These programmes have included plyometric, biomechanical analysis and technique feedback, proprioceptive/balance and strength training in various combinations.2 92–94 However, which types of interventions and which biomechanical risk factors should be targeted to reduce ACL injury risk most effectively remains a topic of debate. Prevention and intervention programmes that only target high-risk sagittal plane biomechanics such as shallow knee flexion angles, large distal tibia posterior ground reaction forces and large quadriceps muscle forces may not address other underlying risk factors in the frontal and transverse planes.95 96 Failing to incorporate rotational, multidirectional training exercises during training programmes may hamper ACL injury prevention efforts.
We hypothesise that non-contact ACL injury results from multiplanar knee joint loading during three-dimensional sports movements, encompassed by more than simply anterior shear. The load sharing between knee ligaments is complex and it seems plausible that anterior tibial shear force and axial rotation torque also contribute to the resultant ACL loading during the “valgus” collapse of the knee so often observed during injury, especially in female athletes.
SUMMARY AND CONCLUSIONS
In summary, the load sharing between knee ligaments is complex. Frontal plane “valgus collapse”, as well as sagittal and transverse plane biomechanical factors, likely contribute to ACL injury events. Non-contact ACL injuries almost certainly occur during complex, multiplanar knee joint load states during multiplanar sports movements, rather than during single sagittal planar mechanisms of injury. Although studies indicate that sagittal plane biomechanical factors are probably a part of the ACL loading mechanism, it is highly doubtful that these injuries occur solely as a result of sagittal plane loading mechanisms, especially in the female athlete. Prevention programmes that solely target high-risk sagittal plane landing mechanics fail to address the important frontal and transverse plane contributions to ACL injury mechanisms. Multiplanar training exercises that focus on lowering risky biomechanics in multiple planes such as large knee valgus, internal/external knee rotations and shallow knee flexion angles are needed to minimise hazardous knee loading conditions that cause ACL injury.
Acknowledgments
The authors would like to thank the staff at the Cincinnati Children’s Hospital Sports Medicine Biodynamics Center for the many thoughtful, and sometimes raucous, discussions pertaining to this topic.
REFERENCES
Footnotes
Competing interests: None.
Funding: The authors would like to acknowledge funding support from the University of Toledo College of Medicine Pre-Doctoral Fellowship and the Plus One Active Research Grant on Wellness Using Internet Technology from the American College of Sports Medicine Foundation (CEQ). This work was also partly supported by National Institutes of Health grants R01-AR049735 and R01-AR055563 (TEH) and R01-AR056259 (CEQ and TEH).