Article Text

Abstract
Background MRI is frequently used in addition to clinical evaluation for predicting time to return to sport (RTS) after acute hamstring injury. However, the additional value of MRI to patient history taking and clinical examination remains unknown and is debated.
Aim To prospectively investigate the predictive value of patient history and clinical examination at baseline alone and the additional predictive value of MRI findings for time to RTS using multivariate analysis while controlling for treatment confounders.
Methods Male athletes (N=180) with acute onset posterior thigh pain underwent standardised patient history, clinical and MRI examinations within 5 days, and time to RTS was registered. A general linear model was constructed to assess the associations between RTS and the potential baseline predictors. A manual backward stepwise technique was used to keep treatment variables fixed.
Results In the first multiple regression model including only patient history and clinical examination, maximum pain score (visual analogue scale, VAS), forced to stop within 5 min, length of hamstring tenderness and painful resisted knee flexion (90°), showed independent associations with RTS and the final model explained 29% of the total variance in time to RTS. By adding MRI variables in the second multiple regression model, maximum pain score (VAS), forced to stop within 5 min, length of hamstring tenderness and overall radiological grading, showed independent associations and the adjusted R2 increased from 0.290 to 0.318. Thus, additional MRI explained 2.8% of the variance in RTS.
Summary There was a wide variation in time to RTS and the additional predictive value of MRI was negligible compared with baseline patient history taking and clinical examinations alone. Thus, clinicians cannot provide an accurate time to RTS just after an acute hamstring injury. This study provides no rationale for routine MRI after acute hamstring injury.
Trial registration number ClinicalTrials.gov Identifier: NCT01812564.
- Hamstring
- Injuries
- MRI
Statistics from Altmetric.com
Introduction
Acute hamstring injury is the most prevalent non-contact muscle injury in football1–8 and other sports involving high-speed running.9–13 The incidence of acute hamstring injuries remains high,10 ,14 causing a significant loss of time from competition14 ,15 and a high risk of sustaining a reinjury.10 ,12 ,13 ,16–19
Following acute hamstring injury, the immediate question posed by the athlete, coaches, medical staff and media is: ‘When can the athlete be cleared for competition?’
In the literature, the predictive value of patient history and clinical examinations for time to return to sport (RTS) has received little attention. As the majority of previous studies have reported findings based only on univariate statistical analyses,20–25 the inter-relationship between the possible predictors and their independent associations with time to RTS cannot be discerned.26 Among the studies using a multivariate approach,27–31 differences in study population and design, inadequate control for treatment confounders, and the lack of distinct definitions and time to RTS outcomes make a direct comparison between studies difficult.
In the clinical setting, MRI is frequently used in addition to clinical evaluation for predicting time to RTS after acute hamstring injury.32 ,33 Several studies have reported associations between MRI variables and time to RTS using univariate analyses.15 ,20–25 ,31 ,32 ,34–38 By contrast, a recent systematic review concluded that, due to the considerable risk of bias in the majority of these studies, there is no strong evidence that any MRI finding has prognostic merit for predicting time to RTS.39
Whether MRI adds predictive information over and above patient history taking and clinical examination is unknown (and debated).28 ,39 ,40 Therefore, we aimed to investigate the predictive value of patient history taking and clinical examination at baseline alone, and again with the addition of MRI findings for time to RTS after acute hamstring injuries in male athletes using multivariate analyses, and controlling for potential confounders.
Methods
Study design
This study is based on pooled data from a randomised controlled trial (RCT) on the effect of platelet-rich plasma (PRP) in hamstring injuries41 and a prospective case series of acute hamstring injuries. Both studies were conducted at Aspetar Orthopaedic and Sports Medicine Hospital.
The study was approved by the Ethics Committee of Aspetar Orthopaedic and Sports Medicine Hospital and the Shafallah Medical Genetics Centre Ethics Committee, and written informed consent was obtained.
Participants
To be eligible, athletes were required to meet the inclusion criteria presented in table 1. Eligibility was assessed and determined at the Outpatient Department by the treating sports medicine physician. Between January 2011 and June 2014, athletes were recruited consecutively from sporting clubs and federations in Qatar, mainly through the Qatar National Sports Medicine Program (to which the study centre provides sports medicine and orthopaedic services).
Eligibility criteria
Baseline assessments
The treating sports medicine physician performed standardised patient history taking and clinical examination within 5 days after injury.
Patient history
By interviewing the athlete, we obtained information about: type of sport, maximal pain experienced at the onset of injury (using a visual analogue scale (VAS), where 0 reflected no pain and 10 reflected maximal pain), type of injury mechanism, occurrence during training or competition, forced to stop playing or training within 5 min at the onset of injury, a previous history of hamstring injury and previous low back pain.
Clinical examination
Clinical examination included hamstring range of motion (ROM) testing, manual muscle resistance testing, active slump test and palpation.
Pain with ROM testing was assessed with trunk flexion, the passive straight leg raise test and the active knee extension test. During a progressive trunk flexion from a standing position with knees extended towards the level of maximal flexion, the physician registered presence or absence of recognisable pain at the injury site. For the passive straight leg raise test, the athlete was supine and the physician raised the athlete's leg with extended knee until the first point of reported stretch or pain at the site of injury,31 ,24 and absence or presence of pain was noted. Active knee extension ROM was performed with the athlete supine and 90° hip flexion of the tested leg, while the other leg remained flat on the examination table.31 ,42 The physician instructed the athlete to gradually extend his knee to the point of resistance to further extension, or the onset of pain at the site of the injury, and registered presence or absence of pain.
Manual muscle resistance was examined with the athlete lying supine. Painful resisted knee flexion with 90° hip and knee flexion was examined with the physician's hand against the posterior heel, asking the athlete to actively contract the hamstring muscles while performing isometric knee flexion with maximum force. Pain was registered as yes or no. Painful resisted hip extension with 30° hip and knee flexion was examined with the physician's hand against the posterior heel, asking the athlete to actively contract the hamstring muscles while performing an isometric knee flexion with maximum force. Pain was registered as yes or no.
The active slump test was included to assess the mobility of pain-sensitive neuromeningeal structures, suggested as a potential source of pain in the posterior thigh presenting after acute hamstring injuries43 ,44 and previously used in other relevant studies.30 ,31 The test was examined with the athlete seated with hands behind his back while maintaining a neutral spine position. We asked the athlete to tuck the chin towards the chest and to slump, bringing the shoulders towards the hips with full cervical, thoracic and lumbar flexion. Then we asked the athlete to perform a full active dorsiflexion of the foot of the injured leg and thereby actively extend the knee until a stretch or pain was felt in the hamstring muscle due to the original pain. The athlete was then asked to extend his neck to a neutral position and describe the change in sensation that occurred in the hamstring muscle. The test was considered positive if the athlete's original hamstring pain was decreased and then reproduced with cervical flexion.
Length and width of the region of tenderness (palpation pain) was examined with the patient prone. We identified the origin of the hamstring muscles on the ischial tuberosity and palpated the complete posterior thigh starting from the hamstring origin at the ischial tuberosity, and moving continuously inferiorly to the hamstring muscle insertions, as described by Askling et al.24 Using a ruler, we measured the longitudinal cranial-to-caudal length and the medial-to-lateral width (cm) of the tender area. Throughout the study period, 19 physicians, all with a minimum 5 years of sports medicine experience, performed the baseline assessments.
MRI examination
MRI was performed using the same protocol as previously described.45 With the athlete lying supine, we obtained images of the injured hamstring muscle from the ischial tuberosity to the knee, using a 1.5 Tesla magnet system (Magnetom Expert, Siemens, Erlangen, Germany) with a body matrix coil. We attached a vitamin E capsule to the athlete's posterior thigh corresponding with the point of maximal tenderness indicated by the athlete. Coronal and axial proton density-weighted images were first obtained (time to repetition (TR)/time to echo (TE) 3000/30 ms, field of view (FOV) of 220–240 mm, slice thickness of 3.5 mm and a 333×512 matrix) with an echo train length (ETL) of 9 for the coronal images and 6 for the axial. Subsequent coronal and axial fast-spin echo proton density fat saturation images (PD-FS) (TR/TE of 3000/32 ms, FOV of 240 mm, slice thickness of 3.5 mm, a 326×512 matrix for the coronal images and TR/TE of 3490/27 ms, FOV of 320 mm, slice thickness of 3.5 mm, a 333×512 matrix for the axial images) with an ETL of 6 were acquired. We considered a hamstring muscle injured if the MRI demonstrated increased signal abnormalities on fluid-sensitive sequences (PD-FS). If more than one muscle was injured, the muscle with the greater extent of signal abnormality was defined as the ‘primary’ injury.
One experienced radiologist assessed and scored the MRIs, and determined the localisation and extent of the injury using a standardised scoring form based on the literature.15 ,24 ,34 ,36 ,46 ,47 In a previous study, we reported good to excellent intratester reliability with the same radiologist.45 The radiologist was blinded to the clinical status of the injury and the time to RTS outcome. Recording included describing the involved muscle(s) and scoring an overall grading (grade 0–3) of the injury using an MRI modification15 of Peetrons’ classification47 (grade 0: no abnormalities, grade 1: oedema without architectural distortion, grade 2: oedema with architectural disruption, grade 3: complete tear). In addition, the length (craniocaudal extent), width (mediolateral extent) and depth (anteroposterior extent) of increased signal intensity on the fluid-sensitive sequences (PD-FS) was recorded. The distance from the most cranial pole of the injury to the caudal part of the ischial tuberosity24 and any disruption of the central tendon as described by Comin et al46 were noted. The involved cross-sectional area of oedema was calculated as a percentage of the total muscle cross-sectional area in the transversal plane. We approximated the volume of the total oedema using the formula for a prolate ellipsoid ([π/6]×anteroposterior×mediolateral×craniocaudal extent).24 ,34
Treatment received
Athletes included in the RCT study were randomised into three groups: one group received a PRP injection, one group received an injection of platelet-poor plasma (PPP) and one group received no injection.41 All three groups followed a six-stage criteria-based physiotherapy programme including three final stages of sports-specific functional field testing supervised by an experienced sports rehabilitator, where the final session was aimed to mimic fatigue and competitiveness as during full unrestricted training at requested training volume and intensity.48 The study showed no benefit of PRP compared with no injection and a delayed time to RTS for PPP compared with PRP. The athletes included in the prospective case series received either rehabilitation at the study centre, as described above, or custom-made rehabilitation at the study centre or in their club or federation. Four athletes in the prospective case series received a single PRP injection.
Outcome measure
Time to RTS was defined as the number of days from initial injury until the athlete was cleared by one of the physicians at the study centre or cleared by the treating physician or physiotherapist at the club or federation, to resume full unrestricted training. The RTS decision makers, who were either the treating sports medicine physicians at the study centre or the physicians or the physiotherapists in the clubs or the federations, were not blinded to the baseline assessments or the MRI findings.
For athletes receiving rehabilitation at the study centre, RTS evaluation took place after the patient completed the final stage of the sports-specific functional field testing and isokinetic strength testing.48 The treating physician took a structured history and performed clinical assessments including palpation, ROM and resistance testing. Based on the clinical evaluation, the strength tests, the reports from the treating sports physical therapist and the sports rehabilitator and, in addition, sports risk modifiers and decision modifiers,49 the physician made a final decision on whether the athlete should be cleared for RTS, or to resume rehabilitation and perform new measurements prior to the ultimate clearance for RTS.
For athletes receiving rehabilitation in club or federation, we registered time to RTS once the athlete returned to full, unrestricted training. The number of days until RTS registered was provided by the club medical staff at weekly phone calls or via emails. The criteria for RTS were decided by the team/federation physiotherapist or physician.
Data management and statistical analysis
We performed the statistical analysis using SPSS software (V.21.0; SPSS, Chicago, Illinois, USA). Continuous variables were tested for normality and presented as mean values (±SD) unless otherwise stated. To analyse the association between the potential predictive baseline variables and time to RTS, we constructed a general linear model. In the first step, we analysed the relationship between each of the potential predictive variables and time to RTS in a univariate model. Variables with a p value of <0.2 in the univariate model were included in the multiple regressions analysis. The potential predictive variables were also checked for multicollinearity and the variable with the highest association with the time to RTS was included in the multiple regression analysis. In the multiple regression analyses, we used a backward stepwise technique keeping treatment variables (PRP or PPP injection received and rehabilitation received at study centre vs in club) fixed to control for confounding. We created two multiple regression models that included the patient history and clinical examination variables. In the first model, we did not include MRI variables. In the second model, we included the MRI variables. Regression coefficients are presented as unstandardised β-coefficients with 95% CIs. p Value <0.05 was considered as statistically significant.
Results
Between January 2011 and June 2014, we included 199 athletes with clinical diagnosis of acute hamstring injury. For 19 cases, the RTS date was not available and they were therefore excluded from the analyses (figure 1). Of the 180 athletes included in the final analyses, 177 were registered as professional athletes and 3 as competitive athletes. The athletes represented 37 different nationalities, the majority from the Middle East (59.4%). By ethnicity, 49.2% were Arabic, 29.6% black, 5.6% Caucasian, 5.0% South and East Asian, 3.9% Persian and 6.7% other. The majority played football (77.2%), while others competed in futsal (6.7%), handball (4.4), basketball (3.3%), volleyball (2.2%), athletics (2.2%) or other sports (6.2%). There were no significant differences between the 180 athletes included in the final analysis and the 19 athletes (18 registered as professional athletes and 1 competitive) lost to follow-up with regard to the key baseline characteristics age (26 years, SD±6, p=0.81, independent t test), height (175 cm, SD±8, p=0.17), weight (73 kg, SD±11, p=0.58) or type of sports (football vs non-football, p=0.25).
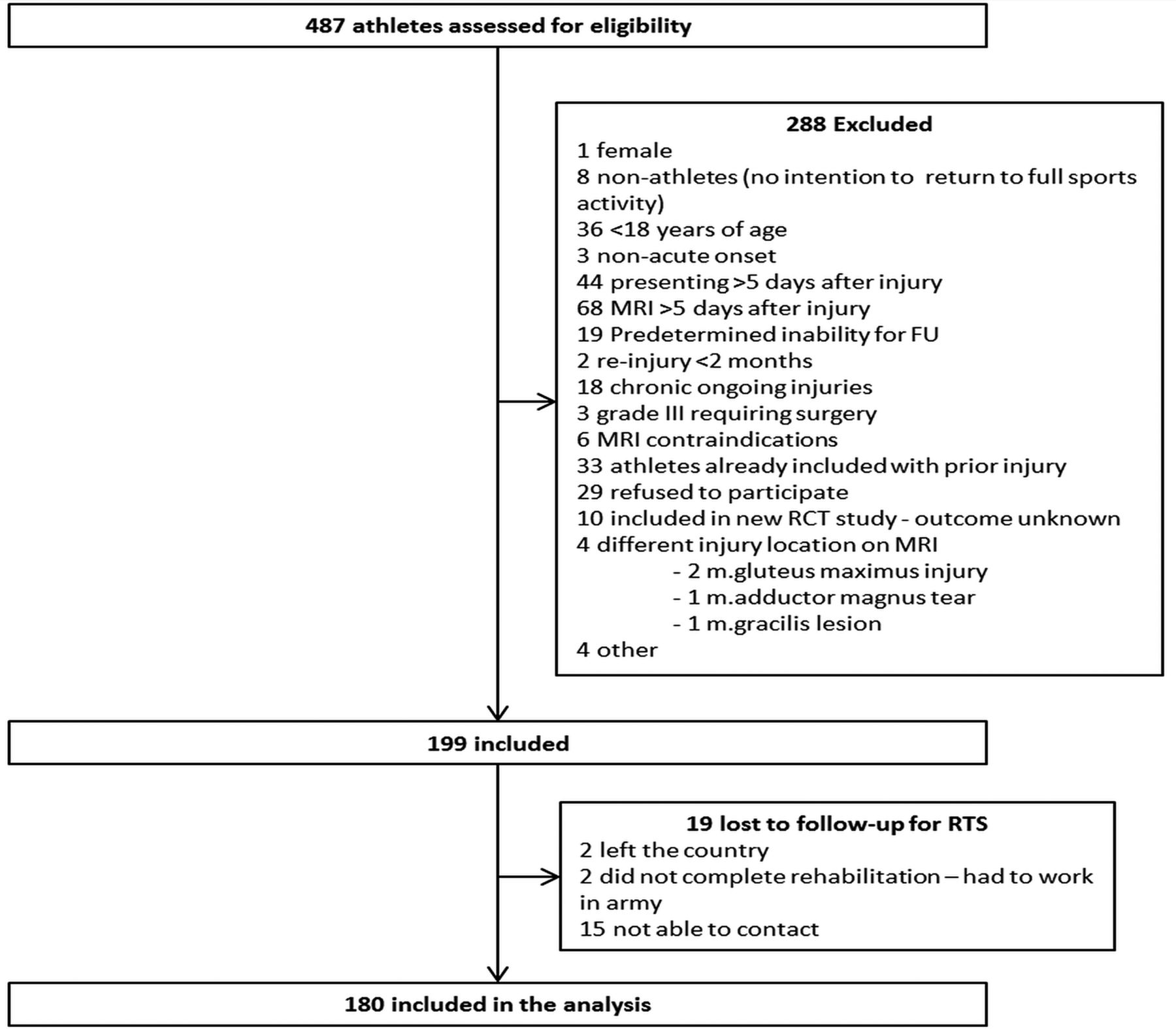
Flow chart. (FU, follow-up; RCT, randomised controlled trial; RTS, return to sport).
The majority of the athletes (90%) were examined clinically between day 0 and 3 after injury (mean: 1.9 days, SD 1.1) and 94% of the athletes had their MRI examination within 4 days (mean: 2.5, SD±1.3). There were 141 (78%) MRI-positive and 39 (22%) MRI-negative cases. The primary injury was observed to the long head of the biceps femoris (n=112, 79.4%), semimembranosus (n=24, 17.0%), semitendinosus (n=4, 2.8%) or the short head of the biceps femoris (n=1, 0.7%). In 26 cases, two muscles were involved and in 1 case, three.
Time to RTS ranged from 1 to 72 days, with a mean of 21 (SD±12) days for all cases, 13 (SD±8) days for MRI-negative cases and 24 (SD±12) days for MRI-positive cases. Table 2 shows the univariate associations between baseline assessments from patient history and clinical examination, and time to RTS.
Univariate analysis: baseline characteristics of patient history and clinical examination findings and their associations with time to RTS
Regression model without MRI
In the first multiple regression model examining patient history and clinical examination, 13 candidate variables were included: maximal pain score (VAS), type of sports (football vs other sports), type of injury (sprinting vs non-sprinting), forced to stop training/playing within 5 min after injury, pain on trunk flexion, pain with active knee flexion, length and width of hamstring tenderness, pain with straight leg raise, pain with passive active knee extension, painful resisted knee flexion (90°), painful resisted knee flexion (30°) and active slump. After manual backward stepwise regression analysis and controlling for potential confounders, four variables were retained in the final model and independently associated with time to RTS (table 3). The total variance in time to RTS explained by this model was 29% (analysis of variance (ANOVA), F=11.291, p<0.001).
Model 1: multiple regression analysis of patient history and clinical examination as predictors for time to RTS after controlling for potential treatment confounders (n=180)
Univariate MRI analyses
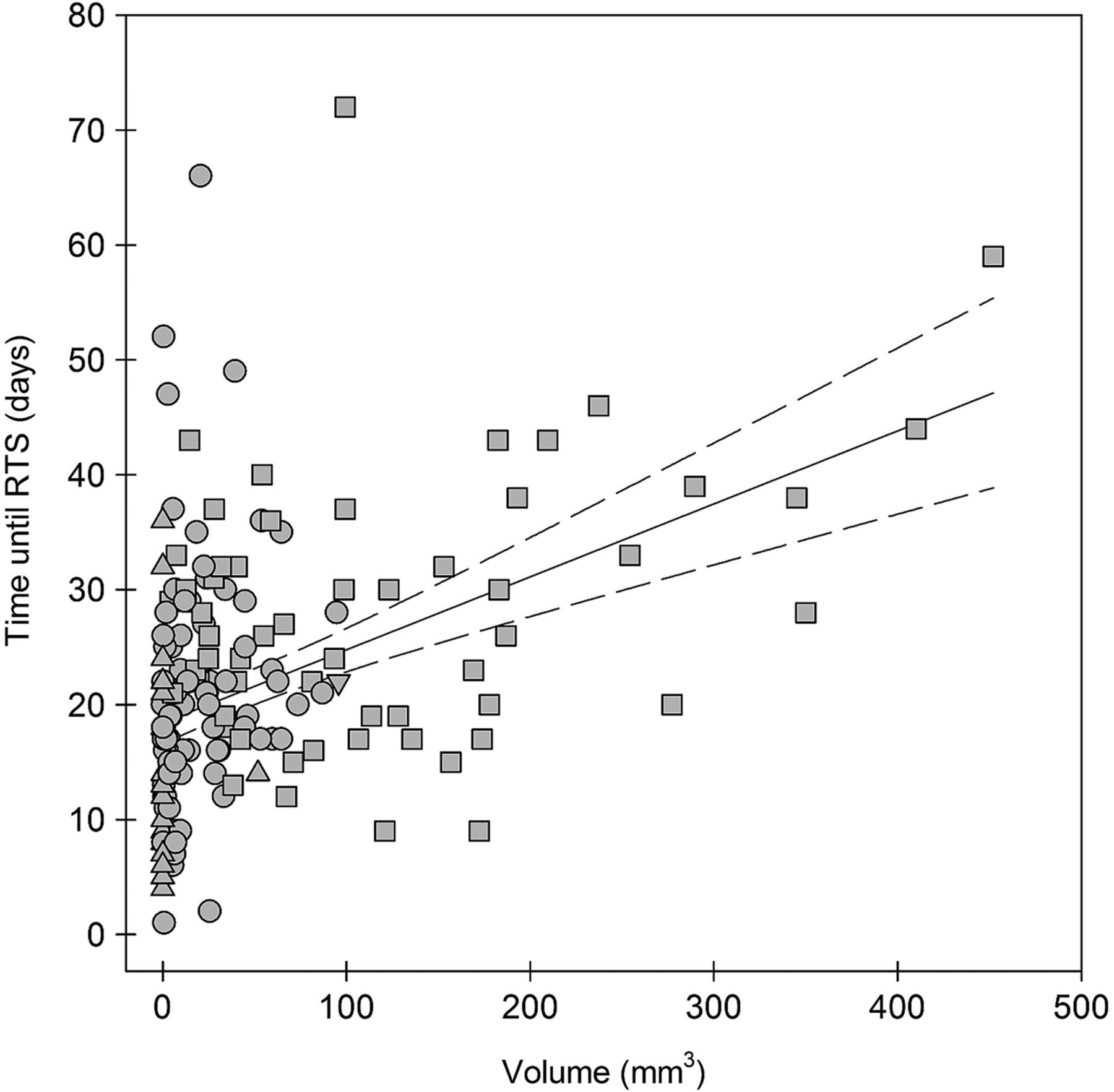
Table 4 shows the univariate associations between baseline MRI variables and time to RTS. There was a wide range in the distribution of time to RTS independent of the MRI results. The median time to RTS for grade 0 injuries was 13 days (range 4–36), for grade 1 injuries 21 days (range 1–66) and for grade 2 injuries 28 days (range 9–72). In the univariate analysis, there were significant differences in time to RTS between grades 0 and 1 (p≤0.001), grades 0 and 2 (p≤0.001) and grades 1 and 2 (p=0.001; one-way ANOVA, Tukey post hoc comparisons). The relationship between volume of oedema and time to RTS (linear R2: 0.19) is illustrated in figure 2, revealing the substantial variation between time to RTS and volume for each individual athlete.
Univariate analysis: MRI variables at baseline and associations with time to RTS in univariate analysis
{kind=link}
{kind=link}
Scatterplot and line of best fit (solid line) with 95% CI (dotted lines) depicting the linear relationship between volume of oedema (cm3) and time to RTS (days). The square labels represent injuries scored as grade 2, the circles represent injuries scored as grade 1 and the triangles represent injuries scored as a grade 0.
Adding MRI to the regression model
In the second multiple regression model, adding MRI variables to those from patient history and clinical examination, 18 candidate variables were included. In addition to the 13 patient history and clinical examination variables described above, five MRI variables were added: distance from most caudal aspect of the ischial tuberosity to the injury, presence of central tendon disruption, volume of oedema, number of muscles involved and overall grading. After controlling for possible treatment confounders, four variables were included in the final model (table 5). The total variance in time to RTS explained by the model (including MRI variables) was 31.8% (ANOVA, F=11.222, p<0.001).
Model 2: multiple regression analysis of patient history, clinical examination and MRI variables as predictors for time to RTS including both MRI-positive and MRI-negative injuries (n=180)
Discussion
This prospective study showed that patient history and clinical examinations at baseline explained 29% of the total variance in time to RTS. Addition of MRI explained only 2.8% of the variance. There was wide individual variability in time to RTS and our findings, mirroring the limited ability of baseline assessments to predict ultimate time to RTS after acute hamstring injuries.
Predicting time to RTS using patient history taking and clinical examination
To our knowledge, five studies have investigated patient history and clinical examination variables for the accuracy of predicting time to RTS after acute hamstring injuries using multivariate analysis.27–31 However, several methodological differences such as a retrospective study design,29 dichotomous reporting of time to RTS outcome27 ,30 and pooling of several clinical tests into an overall clinical grading,31 limit the ability to compare our results with these findings.
Maximum pain score (VAS) at the time of injury was independently associated with a longer time to RTS in our first regression model including only patient history and clinical variables; increasing the pain score by 1 unit resulted in 1.6 days longer time to RTS (95% CI 0.8 to 2.4). Despite discrepancies in study methodologies and populations, this result supports and extends previous findings.25 ,27 For example, Guillodo et al27 reported that initial VAS pain score greater than 6 was independently associated with later recovery (>40 days).
Being forced to stop within 5 min of the onset of pain was independently associated with increased time to RTS duration in our multivariate analysis. No previous studies have examined this variable and the association with time to RTS.
Painful resisted knee flexion with hips and knees in 90° was independently associated with time to RTS and remained in our final regression model. In our study, painful resisted knee flexion with hips and knees in 90° associated with a 4.7 days longer time to RTS compared with athletes reporting no pain. However, the 95% CI for this variable ranges from 0 to 9 days suggesting unclear clinical utility for this examination. In contrast, three other studies using multivariate analysis did not find any association between pain on isometric contraction testing and time to RTS.27 ,28 ,30 In two of these studies, the isometric contraction was performed in a prone position with knee flexion at 15°,28 ,30 and in one study, the exact testing procedure was not reported.27 Variations in the testing position make comparisons with the current work difficult.
Length of the area of tenderness (pain to palpation) was independently associated with time to RTS in our study; a 1 cm longer area of tenderness associated with time to RTS being 0.3–1.1 day longer. Moen et al28 did not find such an association in 74 athletes with MRI-positive injuries, nor did two other studies of 18 sprinters24 and 15 dancers22 with hamstring injuries,22 ,24 using univariate analysis. However, the absence of associations in these two studies by Askling et al might reflect a low sample size.
Although four variables from patient history and clinical examination were independently associated with time to RTS, the final model could only explain 29% of the total variance in time to RTS. Therefore, 71% of the total variance in time to RTS remains unexplained. To illustrate the clinical relevance of this finding, we created a ‘dummy case’ with the following values allocated for each of the variables in the final model: maximum pain score 6, forced to stop playing within 5 min yes, length of tenderness 4 and pain on knee flexion 90° yes. The predicted time to RTS for this specific case is 21.3 days with a 95% CI between 1.2 and 41.4. Thus, the physician or physiotherapist on training camp without access to imaging, and using the factors from the clinical examination remaining in our final model, can give the athlete the following prognosis: ‘There is 95% chance that you will return to play between 1 and 41 days from now’. For a professional athlete, this wide range is essentially useless. Nevertheless, as we only performed baseline assessments, we cannot comment on whether repeating these assessments regularly after the injury (eg, weekly) would provide a greater accuracy for predicting time to RTS.
The additional predictive value of MRI
Of the MRI variables tested in our second regression model, only categorical MRI grading (grades 0, 1 and 2) remained in the final model. However, there was substantial variability in time to RTS within each of the grading categories and considerable overlap between grading categories. Therefore, the additional predictive value of MRI was negligible beyond that possible based on history and physical examination alone. Revisiting our ‘dummy case’, adding an MRI grading of 2 to our final regression model, the predicted time to RTS would be 25 days with a 95% CI between 5.4 and 44.7. In this case, the message to the athlete would be: ‘There is a 95% chance that you will return to play between 5 and 45 days from now’.
Our finding of variability in time to RTS within each of the grading categories, and overlap between each of the grading categories, parallels reports that examined this variable in larger cohorts.15 ,32 MRI grading (alone) is unhelpful for predicting time to RTS. Our results add further weight to the conclusions of a systematic review, which stated that recovery time cannot be predicted based on MRI findings.39
Of the 180 athletes in our study, 22% had no radiological signs of injury. MRI-negative scans in patients with clinical signs of acute hamstring injury have been reported in previous studies in the range of 12–31%.15 ,20 ,21 ,25 ,31 ,32
We based MRI measurements on previous literature. However, we were only able to perform measurements and calculations based on two-dimensional images on a 1.5 T machine; we do not know whether using more advanced MRI techniques and software50 ,51 would have provided more accurate information. We used a simple categorical grading system that is based on severity, and widely used in clinical practice and research.15 ,47 ,52 More comprehensive classification systems incorporate the location of injury within the muscle.53 ,54 Whether such classification systems will improve our model substantially, needs to be researched.52
What are the implications of our study for clinical practice? Although MRI did not provide additional data to predict time to RTS, this is not a call to abandon MRI in clinical practice. MRI might have value for confirming the clinical diagnosis (including total ruptures) and informing the athlete (showing images might provide the athlete with a better understanding of the injury). Although time to RTS cannot be predicted from current knowledge, it might be that future research focusing on new imaging techniques and/or repeated clinical measurements throughout the course of rehabilitation may reveal more promising predictors.
Strengths of the study
The strengths of this study include the large sample size of 180 athletes evaluated in standard manner using a prospective study design. Also, we used multiple regression models to examine the independent associations between each of the baseline variables and time to RTS. Furthermore, the baseline assessments were performed at the same study centre, increasing the consistency of our examination procedures (and the internal validity of our study). The physicians used the same standardised physical examination procedures. MRIs were all performed using the same 1.5 T MRI scanner and the MRIs were all reviewed and scored by the same radiologist (EA).
Limitations of the study
We report several limitations. First, the physicians who made the RTS decision (and thus, the time to RTS) were not blinded to the baseline characteristics. When studying the prognostic variables, the outcome measure (time to RTS) should ideally be independent of the prognostic variable of interest to prevent bias. One might expect that an unblinded clinician with knowledge of the baseline prognostic variables is likely to be influenced by information from the baseline examination and not only the clinical findings and functional test results at the time of RTS. Therefore, our findings may overestimate the predictive value of the variables examined.
Second, the athletes received either standardised or customised rehabilitation, and the clearance for time to RTS was performed either by physicians who worked at the study centre or at the specific sports clubs or sporting federation headquarters. Although the guidelines for time to RTS at the study centre were well defined, the criteria for time to RTS in the clubs or federations depended on the treating club physiotherapist or physician. However, these factors were included as possible confounders (study center vs club) and this was controlled for in the regression analysis. Although a number of randomised controlled trials have recently tested the effect of different treatment/rehabilitation protocols after acute hamstring injuries,20 ,21 ,38 ,55–57 there is still no consensus regarding the optimal treatment or uniform guidelines for RTS clearance. Hence, our study largely reflects the real life situation, and the variability in treatment received increases the generalisability of our findings.
Some measures previously investigated for associations with RTS, such as time to walk pain free,30 patient predicted time to RTS,28 peak tenderness and its distance from the ischial tuberosity,20–24 ,27 ,28 passive straight leg raise and active ROM deficits in degrees,27 ,28 ,30 ,42 were not examined. As we only performed MRI of the injured leg, we were not able to evaluate the involvement of the proximal tendon, as described by Askling et al.20 ,21 Whether some of these variables would have improved our regression models remains unknown. We appreciate that factors such as external pressure on the athlete for a quick time to RTS, the number of important games or competitions in the period after the injury and experience from previous injuries, might influence the time to RTS; however, we were not in a position to investigate those factors.
Finally, the study population essentially consisted of professional athletes training and competing in the Middle East (Qatar). This pool of athletes represents a wide range of nationalities and ethnicities. We do not know whether our findings apply to women or athletes in other settings.
Summary and conclusion
There was a wide variation in time to RTS, and the additional predictive value of MRI for time to RTS was negligible compared with baseline patient history taking and clinical examinations alone. Based on our findings, clinicians cannot provide an accurate time to RTS based on patient history and clinical examinations just after an acute hamstring injury. Routine MRI examination has limited additional value and cannot be recommended.
What are the new findings?
There was a wide range in time to return to sport (RTS), independent of injury severity, reflecting the difficulty of predicting time to RTS after acute hamstring injuries based on baseline assessments.
MRI did not add any additional predictive value for time to RTS compared with baseline patient history and clinical examinations alone after acute hamstring injury.
Patient history and clinical examinations alone explained 29% of the total variance in time to RTS, and adding MRI only increased the predictive value by 2.8%.
How might it impact on clinical practice in the near future?
Expert clinicians cannot provide an accurate time to RTS estimate at baseline after acute hamstring injuries based on patient history taking and clinical examination. This study provides no rationale for routine MRI after acute hamstring injury, the most prevalent soft tissue injury in football codes.
Acknowledgments
The authors would like to thank the Sports Medicine Physicians and the staff in the Outpatient Department, the staff in the Radiology Department, the Rehabilitation Department and the Orthopaedic Department at Aspetar, and the staff of the Qatar National Sports Medicine Program (NSMP), for their contribution to the study.
References
Footnotes
Correction notice This paper has been amended since it was published Online First. There was an error in the last line on page 6. In the previous version it was “(grades 1 and 2)”, this has now been replaced with “(grades 0, 1 and 2)”.
Twitter Follow Arnlaug Wangensteen at @arnlaugw
Contributors AW designed the study, monitored data collection, analysed and interpreted the data, and drafted the article. JLT and RB designed the study, interpreted the data, revised the article and approved the final revision of the article. EA analysed the MRIs, interpreted the data, revised the article and approved the final revision of the article. SB monitored data collection, interpreted the data, revised the article and approved the final revision of the article. AF, BH and RW interpreted the data, revised the article and approved the final revision of the article.
Competing interests None declared.
Patient consent Obtained.
Ethics approval Ethics Committee of Aspetar Orthopaedic and Sports Medicine Hospital and the Shafallah Medical Genetics Centre Ethics Committee.
Provenance and peer review Not commissioned; externally peer reviewed.