Article Text

Abstract
Background Patellofemoral osteoarthritis (PF OA) is more prevalent than previously thought and contributes to patient’s suffering from knee OA. Synthesis of prevalence data can provide estimates of the burden of PF OA.
Objective This study aims to conduct a systematic review and meta-analysis on the prevalence of PF OA and structural damage based on radiography and MRI studies in different populations.
Methods We searched six electronic databases and reference lists of relevant cross-sectional and observational studies reporting the prevalence of PF OA. Two independent reviewers appraised methodological quality. Where possible, data were pooled using the following categories: radiography and MRI studies.
Results Eighty-five studies that reported the prevalence of patellofemoral OA and structural damage were included in this systematic review. Meta-analysis revealed a high prevalence of radiographic PF OA in knee pain or symptomatic knee OA (43%), radiographic knee OA or at risk of developing OA (48%) and radiographic and symptomatic knee OA (57%) cohorts. The MRI-defined structural PF damage in knee pain or symptomatic population was 32% and 52% based on bone marrow lesion and cartilage defect, respectively.
Conclusion One half of people with knee pain or radiographic OA have patellofemoral involvement. Prevalence of MRI findings was high in symptomatic and asymptomatic population. These pooled data and the variability found can provide evidence for future research addressing risk factors and treatments for PF OA.
Trial registration number PROSPERO systematic review protocol (CRD42016035649).
- OA
- X-ray
- MRI
- Knee
- Trauma
Statistics from Altmetric.com
Introduction
Knee osteoarthritis (OA) is a leading cause of pain and disability worldwide.1 The patellofemoral joint (PF) is commonly affected in symptomatic knee OA2 and is a substantial source of symptoms associated with knee OA.3 Further to this, the PF is often affected by OA before the tibiofemoral (TF) joint and increases the risk of TF OA development and progression.4 5
With a recent increase in radiography and magnetic resonance imaging (MRI) based studies focused on PF joint, the evidence on the prevalence of PF OA is expanding rapidly. A 2013 narrative literature review concluded that the prevalence of radiographic PF OA in individuals’ post-ACL and/or meniscus ruptures was approximately 50%.6 A recent systematic review described the prevalence of radiographic PF OA in population-based and in cohorts of people with knee pain.7 A large number of studies have reported PF OA in different populations (eg, post-traumatic and healthy individuals), and knowledge of population-specific prevalence is relevant for clinicians and researchers. An updated review with inclusion of different study samples (eg, post-traumatic, occupation-based, high risk of OA and healthy individuals) builds considerably on the previous systematic review7 and extends our current knowledge of PF OA.
MRI is the modality of choice to assess structural damage in epidemiological studies to detect early and subtle features of OA (eg, abnormal cartilage morphology and bone marrow lesions) not seen on radiography.8 Thus, the prevalence of PF structural damage using MRI may be higher than the prevalence determined by radiography. Including radiography and MRI-based studies in community and specific study, populations provide a comprehensive evaluation of the prevalence of PF OA and PF structural damage and extends prior reviews in this area. Thus, the objective of this study was to perform a systematic review and meta-analysis with the aim to determine the prevalence of PF OA using radiographs and MRI-defined structural PF damage in a variety of study populations.
Methods
The study protocol was developed in consultation with guidelines provided by the Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) statement. The protocol was prospectively registered on the PROSPERO International prospective register for systematic reviews website (http://www.crd.york.ac.uk/PROSPERO) (Registration no: CRD42016035649). The reporting of this study followed the PRISMA checklist.
Literature search strategy
Using guidelines provided by the Cochrane Collaboration, a comprehensive search strategy was devised from the following electronic databases with no date restrictions: (1) MEDLINE via OVID, (2) EMBASE via OVID, (3) CINAHL via EBSCO, (4) Scopus, (5) Web of Science and (6) SPORTDiscus. The primary search strategy included search for original publications. The search strategy was deliberately simplified to ensure inclusion of all relevant papers, with all terms searched as free text and key words (where applicable): Concept 1, Patellofemoral (Patello-femoral, PF, PFJ, knee joint); Concept 2, Osteoarthritis (OA, arthritis, degenerative arthritis, bone marrow lesion); and Concept 3, Prevalence (prevalence, morbidity, epidemiology, diagnosis, incidence). All search terms were exploded and scope notes from each database were examined for other possible terms for modification of search strategies. The MEDLINE search strategy was adapted for other databases (online supplementary file table 1). The search strategy was limited to English language and full text. All potential references were imported into Endnote X7 (Thomson Reuters, Carlsbad, California, USA) and duplicates were removed. Two reviewers (HFH, NW) reviewed all titles returned by the database searches and retrieved suitable abstracts. Where abstracts suggested that papers were potentially suitable, the full-text versions were screened and included in the review if they fulfilled the selection criteria. Reference lists of all publications considered for inclusion were hand searched recursively and citation tracking was completed using Google Scholar until no additional eligible publications were identified. A third reviewer was consulted in case of disagreements (JJS).
Selection criteria
Cross-sectional and longitudinal studies reporting the prevalence or frequency of PF OA or PF structural damage were included. No restrictions were placed on age, sex or method of recruitment. Reviews, case reports and unpublished studies, as well as non-human studies were excluded.
Assessment of methodological quality and risk of bias
Two independent reviewers (NW and ZM), who remained blind to authors, affiliations and the publishing journal, rated the methodological quality of included studies using the Critical Appraisal tool.9 The Critical Appraisal tool was developed to appraise prevalence and incidence-based studies and consists of eight items (maximum score possible 8). Final study ratings for each reviewer were collated and examined for discrepancies. Any inter-rater disagreement was discussed in a consensus meeting, and unresolved items were taken to a third reviewer (HFH) for consensus. Total scores were normalised to a scale ranging from 0 to 2, for each study to assign level of methodological quality. Studies were then classified as high quality (≥1.4), moderate quality (1.1–1.4) or poor quality (<1.1) based on normalised scores.10
Data management and statistical analysis
For the purposes of this systematic review, we defined prevalence as the prevalence of PF OA in community-based studies and the reported frequencies of PF OA in other populations. Data pertaining to population, sample size, sex, age, type of imaging (MRI, radiography), grading criteria, units of analysis (number of participants affected or number of knees affected) and prevalence of radiographic PF OA and MRI-defined PF structural damage (isolated PF OA/PF structural damage; combined PF OA and TF OA/PF and TF structural damage; and unclear, not clearly described whether the prevalence was isolated or combined) were independently extracted and entered into an Excel spreadsheet. If sufficient data were not reported in the published article or supplementary material provided, the corresponding author was contacted to request further data. If multiple studies presented data from one cohort, the study with the most complete data was included. PF OA and MRI-defined PF structural damage prevalence data were reported for: (1) isolated, (2) combined (PF and TF) and (3) any (isolated, combined and unclear). Meta-analysis for proportions with random effects model were performed using MedCalc for Windows, V.16.8. Heterogeneity tests were also conducted and interpreted as follows: I2 ≤ 25%, low heterogeneity; I2=25 to≤50%, moderate heterogeneity; and I2 ≥75%, high heterogeneity.11 Data were divided into two categories based on imaging technique used: (1) radiography and (2) MRI
Radiography studies
The Kellgren and Lawrence (KL) grading criteria12 and Osteoarthritis Research Society International (OARSI) atlas13 are used to define radiographic OA in the TF compartments. There is no KL or OARSI atlas definition of PF OA based on radiographs; however, both criteria are often used to quantify the severity of radiographic OA in the PF using the skyline and/or lateral radiography views. For the purposes of this systematic review and meta-analysis, osteophytes and joint space narrowing were used to define PF OA. If prevalence for multiple radiographic OA features (eg, prevalence based on osteophytes and joint space narrowing) was reported, then prevalence based on osteophytes was chosen. Data were pooled based on the following study populations: (1) community-based (individuals randomly recruited from community), (2) knee pain/ symptomatic (individuals recruited based on knee-related symptoms), (3) radiographic and symptomatic OA (individuals recruited based on symptoms and radiographic OA), (4) healthy individuals (no pain, injury or OA), (5) radiographic or high risk of OA (individuals recruited based on radiographic OA or risk of developing radiographic OA without regard to knee pain/symptoms), (6) occupational-based (individuals recruited based on their occupation/sports) and (7) post-traumatic (individuals with previous knee-related trauma, such as ACL injury or reconstruction or meniscal injury). Given that individuals recruited based on high risk of OA may or may not have had previous trauma; data from individuals with high risk of OA were not included in the post-traumatic category. The occupation-based category included different sporting and occupational activities such as long distance runners, shooters, graphic designers and monks. To determine the prevalence in individuals exposed to different activities, the data from sports and occupational activities were pooled together. Data were stratified based on intensity of activity (eg, high: soccer graphic and low: graphic designers) activities. For longitudinal studies, data from the latest time point (rather than baseline) were included. Within the eight study population categories, sensitivity analyses were conducted when >1 study reported sufficient data for pooling based on disease severity, compartment-specific OA pattern, age and sex. Disease severity was defined as mild, presence of at least mild radiographic PF OA; and definite, presence of definite radiographic PF OA (online supplementary file table 2). Compartment-specific OA pattern was defined as: (1) isolated PF OA, (2) combined PF OA and TF OA and (3) any PF OA. Age groups for sensitivity analyses were categorised as: (1) mean age: <50 years, (2) mean age: ≥50 years. These sensitivity analyses are presented in text for any PF OA and in supplementary material (online supplementary file table 3 for the isolated and combined TF OA and PF OA groups. Where possible, medial and lateral PF OA prevalence was described.
MRI studies
Currently, there is no accepted definition of MRI-defined PF OA. A definition was proposed by Hunter et al 14 which included a definite osteophyte and partial or full thickness cartilage loss. However, this proposed definition of MRI-defined PF OA has not been further validated. Furthermore, most previous studies do not provide data on osteophytes to enable calculation of PF OA prevalence using this definition. Therefore, for the purposes of this systematic reviewwe will report MRI-defined structural damage. Data were pooled based on study populations described above (except for occupational-based population) as well as general population (studies that could not be categorised into one of the categories described above). Within each study population category, data were pooled based on cartilage defect and bone marrow lesions (BML) MRI features. Authors used the following terms to define cartilage defect: cartilage abnormalities, cartilage defect, full cartilage thickness loss, cartilage pathology and cartilage lesion; and the following terms were used to define BML, marrow abnormalities, marrow lesion and bone marrow oedema. To allow data pooling where possible other scoring systems were compared with the Whole-Organ MRI Score (WORMS)15 and MRI Osteoarthritis Knee Score (MOAKS)16 based on the explanation of the scoring system provided in the paper. Data were stratified based on compartment-specific OA pattern (isolated PF OA, combined PF OA and TF OA and any PF OA). Where possible, stratified analyses were conducted based on age (mean age: <50 years, ≥50 years) and sex. If possible, medial and lateral PF OA prevalence was described. Most longitudinal MRI studies provided most complete data at baseline rather than at later time points (dropouts or only ORs data for later time points); thus, this review included baseline data.
Results
Search strategy, methodological quality and risk of bias
The comprehensive search strategy identified 2681 titles, with the last search conducted on 25 February 2016. Following removal of duplicate publications and conference proceedings, titles of 1105 publications were evaluated. Thirteen titles were obtained from other resources (Google Scholar and hand searching). The full texts of 144 articles were retrieved, with 117 articles meeting the selection criteria. Following removal of studies with duplicate data, 85 studies (63 radiography studies,2 17–78 24 MRI studies39 79–101) were included in this systematic review (tables 1 and 2, figure 1). There was one study that reported data on radiographic PF OA and MRI-defined PF structural damage.35 The methodological quality scores ranged from 0 to 2 (out of 2) (online supplementary file table 4). There were 15 studies of high quality, 16 were moderate and 54 were low quality. Most studies scored negatively on items 1 (ie, study design/sampling method) and 6 (ie, response rate) and positively on items 4 (ie, measurement criteria) and 8 (ie, study subjects described) of the critical appraisal tool. A high level of heterogeneity was noted within radiography and MRI studies (I2 range 96%–100%). The level of heterogeneity remained high (I2 range 70%–100%) when studies were further subgrouped based on population, OA severity pattern, age and sex. Exclusion of low methodological quality studies did not decrease the heterogeneity levels.
Details of included radiography studies
Details of included MRI studies
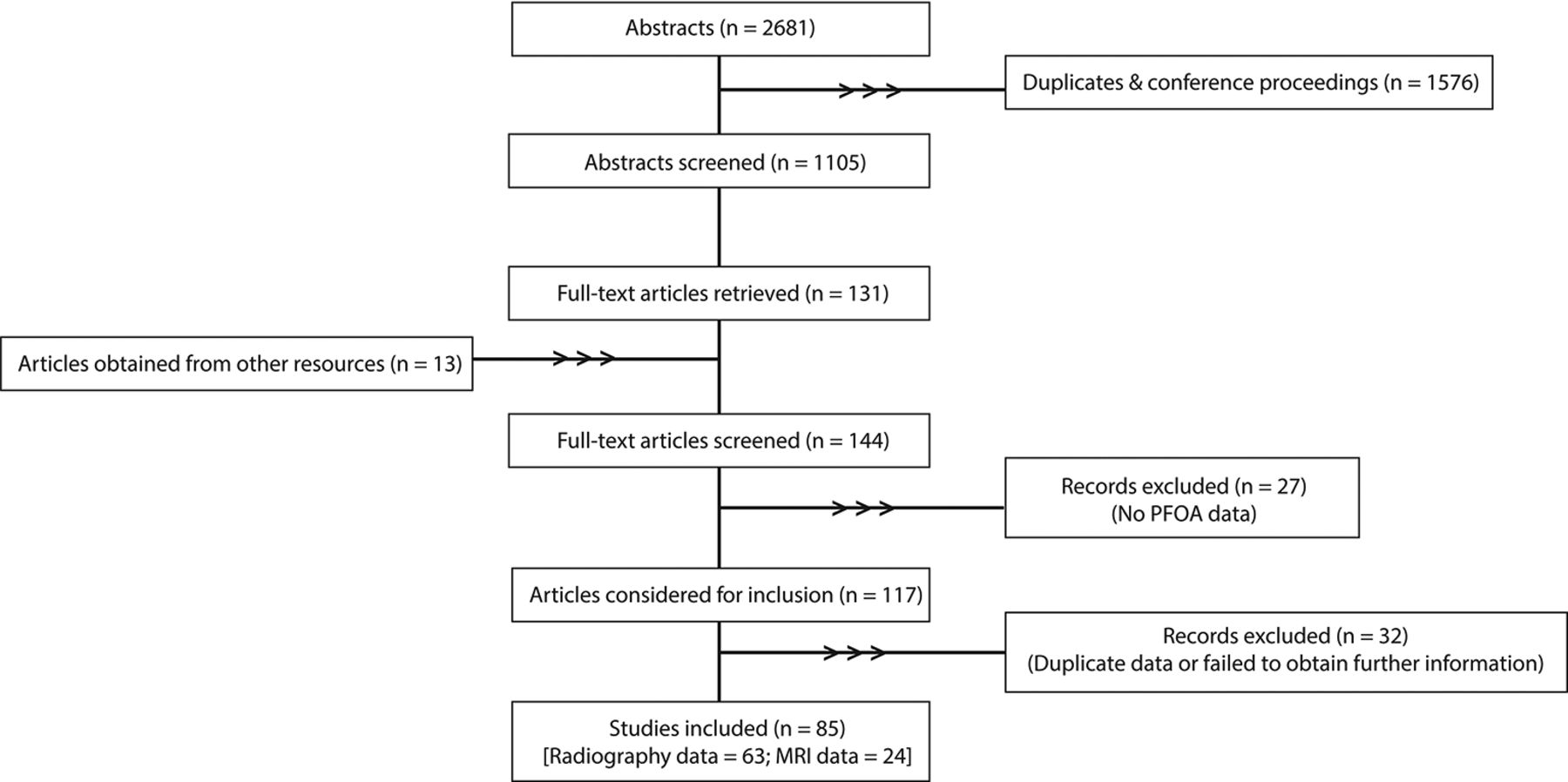
Flow chart of the study selection process. PFOA, patellofemoral osteoarthritis.
Prevalence of patellofemoral OA based on radiography
Community-based population
In community-based populations, the overall prevalence of isolated PF OA from four studies19 24 26 28 was (mean proportion: (95% CI)) 7% (5 to 10), combined PF OA and TF OA from four studies19 24 26 28 was 17% (10 to 26), and any PF OA based on nine studies18 19 24 26 28 39 46 54 75 was 38% (28 to 50) (figure 2A-C). In the any PF OA group, the prevalence of mild OA severity was 33% (17 to 51) from three studies28 46 75 and definite OA severity was 40% (28 to 53) from six studies.18 19 24 26 39 54 The prevalence of any PF OA in community-based population was 32% (24 to 42) in those aged 50 years or over from eight studies.19 24 26 28 39 46 54 75 Only one study described prevalence of isolated compartment-specific PF OA,26 with prevalence of medial PF OA at 0.3% in women and 0.7% in men, and the prevalence of lateral PF OA at 1.6% in women and 3.7% in men. Sensitivity analyses based on sex revealed that the prevalence of any PF OA in women was 41% (31 to 51) from six studies18 19 24 26 28 75 and 47% (23 to 71) in men from four studies.18 19 24 26

Prevalence of patellofemoral osteoarthrits (PF OA) in community, knee pain or symptomatic and radiographic and symptomatic OA populations. TF, tibiofemoral.
Knee pain or symptomatic population
Overall prevalence of isolated PF OA was 19% (11 to 29) from eight studies,2 21 32 42 52 53 59 69 combined PF OA and TF OA was 34% (25 to 43) from seven studies2 32 42 52 53 59 69 and any PF OA was 43% (32 to 55) from 12 studies2 21 22 32 42 52 53 59 60 64 69 77 (figure 2D–F). For any PF OA, the prevalence of mild and definite OA severity was 37% (24 to 51) from seven studies2 21 22 32 52 60 69 and 49% (30 to 67) from six studies,2 42 53 59 64 77 respectively. Age-based prevalence of any PF OA in individuals under 50 years was 54% (16 to 90) from two studies69 77 and in those 50 years or over was 43% (31 to 56) from eight studies.2 21 22 42 53 59 60 64 Sex-based prevalence of any PF OA was 46% (23 to 70) in women53 60 and 58% (27 to 86) in men.53 60 69
Radiographic and symptomatic knee osteoarthritis
Overall prevalence of isolated PF OA was 20% (11 to 32) from four studies,25 30 33 55 combined PF OA and TF OA was 43% (8 to 83) from two studies25 55 and any PF OA was 57% (43 to 70) from 13 studies25 27 30 33 35 37 41 45 50 55 61 74 78 (figure 2G–I). In the any PF OA group, the prevalence of mild severity was 56% (41 to 70) from 12 studies.25 30 33 35 37 41 45 50 55 61 74 78 The prevalence in individuals 50 years or over was 58% (42 to 72) from 12 studies25 27 30 33 35 37 41 45 55 61 74 78 and the prevalence of any PF OA in women was 36% (33 to 38)27 45 and men was 35% (16 to 58) from two studies.27 45
Healthy individuals
Data from four studies were included in meta-analyses to determine the prevalence of PF OA in healthy individuals.34 60 63 72 Overall prevalence of any PF OA in healthy individuals (no pain, injury or OA) was 17% (6 to 33) (figure 3A). Sensitivity analyses based on sex could only be performed in women revealing the prevalence of PF OA in healthy women at 15% (1 to 43) from two studies.60 72

Prevalence of PF OA in healthy individuals, radiographic OA, occupation-based OA and post-traumatic OA populations. PF OA, patellofemoral osteoarthritis; TF, tibiofemoral.
Radiographic knee OA or at risk of developing OA
Overall prevalence of any PF OA in individuals with radiographic OA or at risk of OA was 48% (35 to 61) from four studies36 38 43 48 (figure 3B), with prevalence based on mild and definite OA severity as follows: 54% (17 to 89) from two studies36 48 and 45% (30 to 60) from two studies,38 43 respectively. In this group, the prevalence of any PF OA in women was 41% (8 to 80) from two studies.38 43
Occupation-based population
Four studies reported occupation-based prevalence of PF OA.51 68 72 76 Overall prevalence of any PF OA in individuals in occupations or sports such as long distance running, soccer, shooting, floor layers, graphic designers and monks was 21% (9 to 37) (figure 3C). For any PF OA, the prevalence based on mild OA severity was 29% (10 to 52) from three studies.68 72 76 The prevalence of any PF OA in individuals 50 years and over was 18% (9 to 28) from three studies.51 68 72 Sensitivity analyses based on sex revealed the prevalence of any PF OA in men was 14% (9 to 20) from two studies.51 68 Analysis could not be performed in women. For any PF OA, the prevalence of any PF OA in high-intensity activity population was 19% (11 to 29) from one study51 and 19% (3 to 45) in low-intensity activity population based on three studies.51 68 76
Post-traumatic population
The overall prevalence of isolated PF OA from two studies was 17% (5 to 34) from two studies49 65 (figure 3D). In the injured knee, the overall of prevalence of any PF OA in post-traumatic population (range: 5 to 22 years) was 27% (19 to 34) from 19 studies17 20 23 29 31 34 40 44 47 49 56–58 62 65 66 70 71 73 (figure 3E). For any PF OA, the prevalence of mild OA severity was 26% (18 to 34) from 18 studies.17 23 29 31 34 40 44 47 49 56–58 62 65 66 70 71 73 Sensitivity analyses based on age revealed the prevalence of any PF OA was 27% (18 to 36) in individuals under 50 years17 20 23 29 31 40 47 49 56–58 65 66 70 71 73 and 26% (17 to 35) in those 50 years or over.34 44 In the uninjured knee, overall prevalence of any PF OA was 18% (3 to 42) from three studies,20 56 62 with prevalence of mild OA severity at 25% (2 to 87) from two studies.56 62
Prevalence of PF OA based on MRI
Community-based population
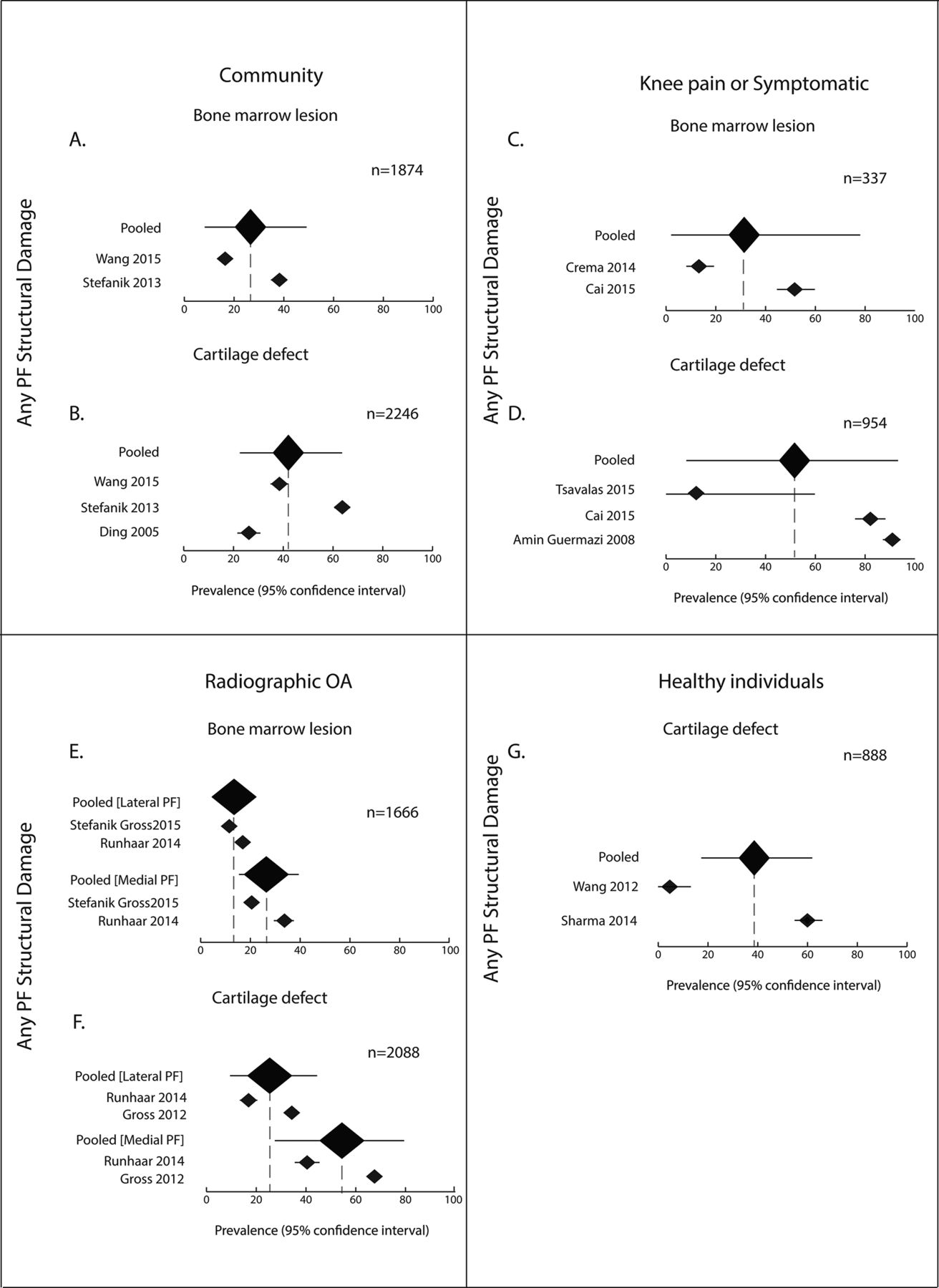
The prevalence of isolated PF structural damage and combined PF and TF structural damage based on cartilage defect were 20% and 44% (respectively) and BML was 18% and 22% (respectively) based on a single study.95 The prevalence of any PF structural damage based on cartilage defects was 44% (25 to 65) from three studies86 95 99 and BML was 29% (11 to 51) from two studies95 99 (figure 4A-B).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Prevalence of MRI-defined PF structural damage in community, knee pain or symptomatic, radiographic OA and healthy individual populations. PF OA, patellofemoral osteoarthritis.
Knee pain or symptomatic population
The prevalence of overall isolated PF structural damage and combined PF and TF structural damage could not be calculated for this study population. The prevalence of any PF structural damage was 52% (9 to 93) based on cartilage defect81 82 97 and 32% (3 to 72) based on BML82 84 (figure 4C, D). Data from one study could not be pooled because of WORMS definition used for OA diagnosis (cartilage damage defined as ≥1 grade in this study compared with ≥2 grade used in other studies),90 with PF structural damage prevalence of 94%, 16% and 81% based on cartilage defect, BML and osteophytes, respectively. Data stratified based on age revealed that the prevalence of any PF structural damage was 71% (33 to 97) in individuals 50 years or over based on cartilage defect.81 82 97
Radiographic knee osteoarthritis or at risk of developing OA
An overall prevalence of isolated PF structural damage, combined PF and TF structural damage and any PF structural damage based on cartilage defect or BML could not be determined for this study population. Two studies reported prevalence of isolated PF structural damage in the medial and lateral PF compartments based on cartilage defect39 91 and BML.39 101 The prevalence of isolated medial and lateral PF structural damage was 56% (29 to 81) and 27% (11 to 46), respectively,39 91 based on cartilage defect and 28% (17 to 41) and 15% (11 to 20), respectively,39 101 based on BML (figure 4E,F). A single study described PF structural damage prevalence based on PF compartment regions (not based on number of individuals or knees)94 and reported prevalence of any PF structural damage based on cartilage defect and BML in women (51% and 29%, respectively) and men (43% and 23%, respectively).94 No further analyses could be conducted in this study population.
Healthy individuals
The overall prevalence of any PF structural damage based on cartilage defect was 40% (19 to 63)92 100 (figure 4G). Since there were only two studies included in this study population, no further analyses could be conducted.
Radiographic and symptomatic knee OA
The prevalence of combined PF and TF structural damage was 75% based on cartilage defect and osteophytes from a single study,83 and no further analyses could be conducted.
Post-traumatic population
Two studies reported prevalence based on osteophytes in ACL injured or reconstructed,85 98 with the prevalence of any PF structural damage at 29%98 and compartment-specific prevalence of medial and lateral PF structural damage at 23% and 7%, respectively.85 The prevalence of medial and lateral PF structural damage based on BML were 2% and 3%, respectively.85 The prevalence of any PF structural damage was 36% in an ACL ruptured population based on cartilage defect.98 In individuals 2 years post arthroscopic partial medial meniscectomy, the prevalence of isolated PF structural damage was 19% based on cartilage defect.100
General population
Five studies were included in the general population category.87–89 93 96 The cartilage defect based prevalence of any PF structural damage was 49% (36 to 62) from two studies using the WORMS87 96 and was 75% (56 to 91) from three studies using the KOSS.88 89 93 The prevalence of any PF structural damage based on BML and osteophytes were 45% and 56%, respectively.93
Discussion
Summary of findings
This systematic review with meta-analysis synthesised prevalence of PF OA and included 85 studies. Meta-analysis revealed the prevalence of any radiographic PF OA in knee pain or symptomatic, radiographic TF OA or at risk of developing TF OA, and radiographic and symptomatic knee OA cohorts was 43%, 48% and 57%, respectively. The prevalence of any MRI-defined PF structural damage in knee pain or symptomatic population was 32% and 52% based on BML and cartilage defect, respectively. This systematic review and meta-analysis highlights the high prevalence of PF OA/ PF structural damage in a wide range of study populations using different imaging tools.
One half (43%–57%) of people with symptoms and/or established radiographic TF OA had PF OA based on radiography. Similarly, a high prevalence of post-traumatic population exhibited signs of PF OA (~30). With such a high prevalence of PF OA, treatments designed specifically for the PF compartment may be required in the OA management strategy.102 103 Clinicans should assess for symptoms of PF pain or PF OA and treat patients accordingly. The few studies that specifically evaluated interventions such as exercise, physical therapy, taping and bracing to address PF OA98 99 104 provide some evidence for their use. While some studies hypothesise that there is a potential continuum of PF pain to PF OA105; no high-quality evidence has supported the association between PF pain in younger individuals to the development of PF OA.106 Unfortunately, studies included in the knee pain or symptomatic OA population category did not differentiate between PF pain and generalised knee pain. Therefore, in the current systematic review, we were not able to determine the prevalence of PF OA in a PF pain population.
Healthy and community cohorts are also likely to demonstrate some PF OA, with radiographic PF OA evident in 17% and 38%, respectively. Since most studies in the community-based meta-analysis were conducted in individuals over the age of 50 years, it appears that radiographic PF OA may be a natural accompaniment to ageing. The only study with a mean age of ≤50 years (but a large range 20 to 93 years), described a particularly high PF OA prevalence in women (81%) and men (88%). The authors hypothesised that cultural factors in Saudi Arabia, such as sitting cross-legged, squatting and praying with knees fully flexed on the ground, may contribute to the high prevalance. Exclusion of this data from meta-analysis revealed the prevalence of any PF OA was 32% in the community population.
The prevalence of MRI-defined PF structural damage in knee pain or symptomatic population was 52%, which was similar to the healthy (40%), community (44%) and general population (49%) cohorts. The high prevalence of MRI-defined PF structural damage may reflect the ability of MRI to detect early changes in the joint that are not visible on radiographs. However, it is unclear whether these findings represent PF OA, as there is no accepted and validated MRI definition of OA. MRI features such as cartilage damage and BMLs can predict incident radiographic OA,107 development of knee pain108 and future total knee replacement.109 Thus, it is plausible that these MRI findings may represent early stages of the PF OA disease process. Further research is needed to investigate the clinical relevance of MRI-defined PF structural damage.
The current systematic review extends on the results from a prior study.7 The previous systematic review reported the radiographic prevalence of PF OA in population-based and symptom- based population; whereas, the current review reported prevalence of PF OA in multiple different populations. Thus, an additional 32 studies were included in the meta-analysis. Further to this, the current review included meta-analysis on prevalence of MRI-defined PF structural damage. Furthermore, the current study extends on the findings from the earlier review by categorising data into multiple study populations and data pooling with subanalysis based on age, sex, compartment-specific OA pattern and OA severity pattern to obtain more accurate estimations of prevalence.
Limitations
This systematic review is not without limitations. First, a very high level of heterogeneity was noted, particularly in the any PF OA group. The inclusion of isolated PF OA, combined PF OA and TF OA, and unclear PF OA (isolated or combined) data in the any PF OA group may explain the high level of heterogeneity. Other potential sources of heterogeneity include differences in diagnostic criteria, populations and case definitions. Second, all relevant studies were included in this systematic review, regardless of methodological quality. Data from 54 low methodological quality studies were included in this review. While this systematic review is subject to bias through the inclusion of low-quality studies, the levels of evidence applied to the pooled data take into account quality, quantity and homogeneity of studies. Third, we restricted the search to studies published in English. Inclusion of data from non-English language studies may alter the outcomes. Fourth, a number of diagnostic criteria were converted to allow data pooling, which may have influenced the results of this systematic review. Fifth, PF structural damage based on MRI should be interpreted with some caution, as fewer studies contributed to meta-analysis within each study population. Lastly, we recognise that there is no accepted and validated definition of radiographic or MRI defined PF OA. Because of this the prevalence data will largely differ in any given study based on different definitions, which may have influenced the results.
Recommendations
While conducting this systematic review, we identified that prevalence data were not well presented in many studies. We recommend that future studies more clearly describe prevalence data based on OA patterns (eg, isolated PF OA vs combined PF OA and TF OA, medial vs lateral PF OA), OA severity (eg, none, mild and moderate) and subgroups (eg, age, sex). Further to this, discrepancies in diagnostic criteria definitions and reporting were noted; therefore, the PF OA definitions should be clearly stated. Better standardisation of data presentation in future studies will help to better understand PF OA epidemiology.
Implications for research and practice
PF OA is an important source of symptoms in knee OA, and is strongly associated with disability.60 Our systematic review and meta-analysis revealed the prevalence of PF OA is highly based on radiography and MRI in community, symptomatic, radiographic knee OA and traumatic knee OA populations. Therefore, well-designed studies are required to evaluate biomechanical, functional and psychological impairments associated with PF OA. Addressing potentially modifiable risk factors for PF OA may reduce the risk of development and progression of PF OA and may have implications for TF disease. This systematic review also revealed a higher prevalence of combined PF OA and TF OA pattern than isolated PF OA; therefore, it is important to explore interventions that target both PF and TF joints.
Conclusions
Synthesis of prevalence data on PF OA and MRI-defined PF structural damage indicates that signs of PF damage are common and should not be ignored in research or clinical practice. In the future, MRI might become highly relevant to identify patients at early disease stages where the disease process may still be reversible and amenable to interventions.
What are the new findings?
Patellofemoral OA is prevalent in individuals in a very wide range of settings—in asymptomatic individuals and in patients with knee pain.
The prevalence rates are influenced by different diagnostic criteria.
MRI-defined patellofemoral structural damage criteria may assist in identifying patients at early disease stages.
References
Footnotes
Contributors All authors were fully involved in the study and preparation of the manuscript. Each author has read and concurs with the content in the final manuscript.
Study conception: HFH, KMC, JJS.
Protocol: HFH, KMC, JJS.
Search strategy: HFH, KMC, JJS.
Abstract screening: HFH, NW.
Data extraction: HFH, JJS, KMC.
Methodological quality ratings: NW, ZM.
Data analysis and interpretation: HFH, JJS, KMC.
Manuscript preparation: HFH, JJS, KMC, NW, ZM.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.