Effect of antihypertensive treatment at different blood pressure levels in patients with diabetes mellitus: systematic review and meta-analyses
BMJ 2016; 352 doi: https://doi.org/10.1136/bmj.i717 (Published 25 February 2016) Cite this as: BMJ 2016;352:i717
- Mattias Brunström, PhD student,
- Bo Carlberg, associate professor
- Department of Public Health and Clinical Medicine, Medicine, Umeå University, SE-901 87 Umeå, Sweden
- Correspondence to: M Brunström mattias.brunstrom{at}umu.se
- Accepted 12 January 2016
Abstract
Objective To assess the effect of antihypertensive treatment on mortality and cardiovascular morbidity in people with diabetes mellitus, at different blood pressure levels.
Design Systematic review and meta-analyses of randomised controlled trials.
Data sources CENTRAL, Medline, Embase, and BIOSIS were searched using highly sensitive search strategies. When data required according to the protocol were missing but trials were potentially eligible, we contacted researchers, pharmaceutical companies, and authorities.
Eligibility criteria Randomised controlled trials including 100 or more people with diabetes mellitus, treated for 12 months or more, comparing any antihypertensive agent against placebo, two agents against one, or different blood pressure targets.
Results 49 trials, including 73 738 participants, were included in the meta-analyses. Most of the participants had type 2 diabetes. If baseline systolic blood pressure was greater than 150 mm Hg, antihypertensive treatment reduced the risk of all cause mortality (relative risk 0.89, 95% confidence interval 0.80 to 0.99), cardiovascular mortality (0.75, 0.57 to 0.99), myocardial infarction (0.74, 0.63 to 0.87), stroke (0.77, 0.65 to 0.91), and end stage renal disease (0.82, 0.71 to 0.94). If baseline systolic blood pressure was 140-150 mm Hg, additional treatment reduced the risk of all cause mortality (0.87, 0.78 to 0.98), myocardial infarction (0.84, 0.76 to 0.93), and heart failure (0.80, 0.66 to 0.97). If baseline systolic blood pressure was less than 140 mm Hg, however, further treatment increased the risk of cardiovascular mortality (1.15, 1.00 to 1.32), with a tendency towards an increased risk of all cause mortality (1.05, 0.95 to 1.16). Metaregression analyses showed a worse treatment effect with lower baseline systolic blood pressures for cardiovascular mortality (1.15, 1.03 to 1.29 for each 10 mm Hg lower systolic blood pressure) and myocardial infarction (1.12, 1.03 to 1.22 for each 10 mm Hg lower systolic blood pressure). Patterns were similar for attained systolic blood pressure.
Conclusions Antihypertensive treatment reduces the risk of mortality and cardiovascular morbidity in people with diabetes mellitus and a systolic blood pressure more than 140 mm Hg. If systolic blood pressure is less than 140 mm Hg, however, further treatment is associated with an increased risk of cardiovascular death, with no observed benefit.
Introduction
Blood pressure goals in people with diabetes mellitus have been extensively debated during the past decade.1 2 3 For many years, guidelines have recommended treating patients to achieve a blood pressure of less than 130/80 mm Hg.4 5 6 Systematic reviews have questioned the evidence for these recommendations.7 8 During 2013 multiple hypertension guidelines were updated.9 10 11 Generally, the treatment goals for people with diabetes were changed to less than 140/90 mm Hg, but some guidelines still opt for lower targets in certain patient groups.9 12 Last year, a new systematic review was published,13 concluding that treating people with a systolic blood pressure (SBP) already less than 140 mm Hg is associated with a reduced risk of stroke and albuminuria, and therefore challenged the relaxation of guidelines. All previous systematic reviews only analysed previously published data.7 8 13
We assessed the effect of blood pressure lowering treatment in people with diabetes mellitus, including previously unpublished data. Although people with diabetes have been included in many trials of blood pressure lowering treatment, for most of these trials data on people with diabetes have not been published separately. We contacted authors, pharmaceutical companies, and authorities to get access to this data. To assess the effect of treatment at different blood pressure levels, we stratified meta-analyses according to baseline and attained SBP. Baseline SBP is important because it reflects the clinical situation better than attained SBP. Although blood pressure before treatment is known, the attained blood pressure with treatment may vary substantially. Also, attained SBP can be regarded as a product of baseline SBP and SBP lowering. Therefore, trials included in each stratum will be more homogenous for clinical characteristics if stratification is based on baseline values.
Methods
We conducted a systematic review and meta-analyses guided by recommendations of the Cochrane Collaboration.14 The methods, including search strategy, inclusion criteria, and preliminary analyses were prespecified (see web appendix for protocol). We included randomised controlled trials with a mean follow-up of 12 months or more and including 100 or more participants with diabetes mellitus. Trials had to compare any antihypertensive agent against placebo, any two agents against one, or any blood pressure target against another. We excluded strictly comparative trials, evaluating one agent against another, as well as trials with combined interventions.
During February 2013, we searched CENTRAL, Medline, Embase, and BIOSIS using broad strategies to maximise sensitivity. CENTRAL was searched using the MeSH terms “antihypertensive agent” and “blood pressure”, exploded and combined, without restrictions in publication year or language (see the web appendix for full search strategies in each database). We also browsed reference lists in, and citations of, systematic reviews and guidelines in the discipline, including a more recently updated review.7 8 13 15 16 17 Using EndNote reference software, we combined the search results and removed duplicate records. MB screened titles and abstracts to exclude apparently irrelevant publications. Both authors independently checked the abstracts and full text articles for eligibility and resolved any disagreements by discussion. Data were extracted into specially designed Excel sheets, pretested on 10 included trials and then modified to increase functionality. Risk of bias was assessed at study level using the Cochrane Collaboration’s risk of bias tool.18 Both authors independently extracted data and assessed risk of bias, with disagreements resolved by a recheck of the original data and discussion.
Prespecified outcomes of interest were all cause mortality, cardiovascular and non-cardiovascular mortality, myocardial infarction, stroke, heart failure, end stage renal disease, amputation, blindness, adverse events, and quality of life. Given the poor reporting of adverse events and quality of life in the original trials, we excluded these outcomes before extraction of any data. We collected data on baseline characteristics at trial level and blood pressure data for the intervention and control groups separately. When any data required according to the protocol were missing, but the trial was potentially eligible, we contacted the authors. If they did not respond to the first email, we reminded them at least once. Where data were available, we calculated relative risks for each outcome in each trial, and pooled results using random effects meta-analysis. We chose the random effects model over the fixed effects model because the included trials differed to some extent, both clinically and methodologically. The results of random and fixed effects models in analyses with low heterogeneity are the same, and if heterogeneity is present the random effects model is generally more conservative. We performed non-stratified meta-analyses for all outcomes, based on all trials. Prespecified stratified analyses were performed based on mean baseline SBP and diastolic blood pressure (DBP) in all participants, mean in-treatment SBP and DBP for the intervention group, and mean differences in SBP and DBP between groups during follow-up. Cochran Q statistics were used to assess the interaction between blood pressure levels and treatment effect on outcomes, testing the null hypothesis that there is no difference between groups. We carried out prespecified metaregression analyses between each blood pressure variable and the treatment effect on each outcome.
In the stratified analyses, we excluded trials predominantly including patients with heart failure because of the risk of assessing effects independent of blood pressure. Also, we were unable to stratify analyses of amputation and blindness because too few trials reported these outcomes. The blood pressure strata were slightly modified from those given in the protocol. For reasons of power, we excluded the baseline stratum for SBP less than 135 mm Hg and for attained SBP greater than 150 mm Hg. DBP stratification was done to achieve as equal a number of trials in each stratum as possible. Because SBP has the strongest association with cardiovascular disease, explaining more than 95% of events,19 we report on this in the review. DBP is problematic because it might be confounded by differences in pulse pressure, as seen between included trials. (See web appendix for analyses stratified according to DBP and to differences in SBP and DBP between groups.)
Heterogeneity was assessed by visually inspecting the forest plots, and through I2 statistics. When heterogeneity was present, we scrutinised baseline characteristics, blood pressure data, and risk of bias assessments of the included trials for possible explanations. If such explanations were found, we carried out sensitivity analyses if we suspected a potential effect on the main results. Publication bias was assessed using funnel plots for all outcomes separately, and for mortality in the stratified analyses. Analyses were performed using STATA v12.
Patient involvement
No patients were involved in setting the research question or the outcome measures, nor were they involved in developing plans for design or implementation of the study. No patients were asked to advice on interpretation or writing up of results. Since we used only aggregated data from previous trials, we are unable to disseminate the results of the research to study participants directly.
Results
Overall, 49 trials corresponding to 73 738 participants fulfilled the inclusion criteria and provided enough data to be included in at least one meta-analysis (fig 1⇓).20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 41 42 43 44 45 46 47 48 49 50 51 52 53 54 55 56 57 58 59 60 61 62 63 64 65 66 67 68 69 70 71 72 Twenty five trials (26 625 participants) comprised diabetic subgroups from larger trials, and 24 trials (47 113 participants) were confined to people with diabetes. Unpublished data for 12 studies (8916 participants) were obtained through contact with the authors, pharmaceutical companies, or authorities.30 32 36 40 44 50 52 54 63 65 71 72 The mean duration of follow-up was 3.7 years, and most of the participants had type 2 diabetes. Table 1⇓ lists the characteristics of the included studies, including comorbidities.

{kind=link}
Characteristics of included studies
Figures 2 and 3⇓ present the meta-analyses stratified according to baseline SBP and attained SBP, respectively. The mean difference in SBP between baseline and follow-up in the intervention groups was 10.2 mm Hg. Because of this, the trials included in each baseline SBP strata generally ended up in the strata for 10 mm Hg lower attained SBP. Figure 4⇓ presents the metaregression analyses for baseline SBP.

Fig 2 Results from meta-analyses stratified according to baseline systolic blood pressure (SBP), reported for each outcome separately
{kind=link}

Fig 3 Results from meta-analyses stratified according to attained systolic blood pressure (SBP), reported for each outcome separately
{kind=link}

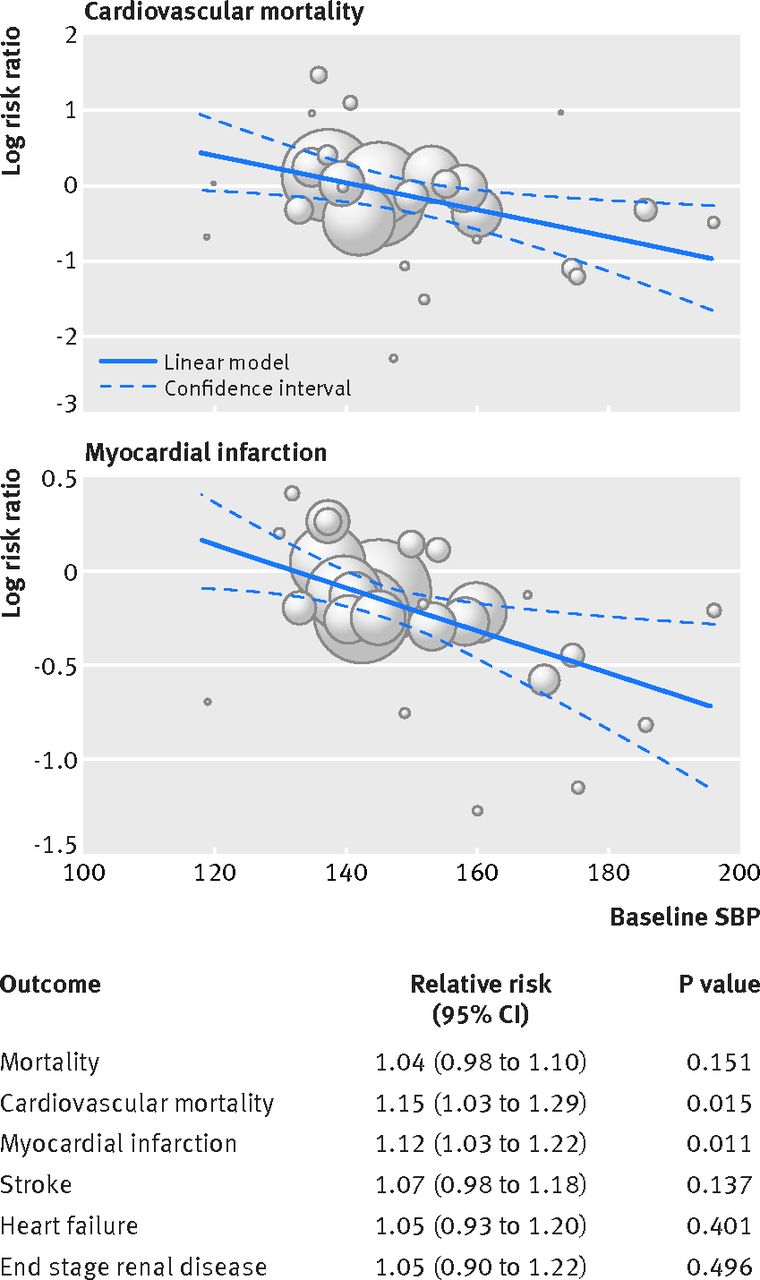
Fig 4 Results from metaregression analyses of treatment effect in relation to baseline systolic blood pressure (SBP). Relative risk is expressed as change in treatment effect for each 10 mm Hg lower baseline SBP. See table for results of all outcomes (those with significant results also presented as graphs). Each circle represents one trial and the size of each circle represents the weight given to the trial in metaregression
{kind=link}
All cause mortality was reduced if SBP before treatment was more than 140 mm Hg and if SBP with treatment was 130-140 mm Hg. If baseline SBP was less than 140 mm Hg, the point estimate shifted towards an increased risk with treatment, albeit not statistically significant (relative risk 1.05, 95% confidence interval 0.95 to 1.16). The same trend was observed if attained SBP was less than 130 mm Hg. Both baseline and attained SBP significantly interacted with treatment effect on all cause mortality (P=0.019 and 0.009, respectively), indicating that the treatment effect is worse with lower SBP.
Cardiovascular mortality was reduced if baseline SBP was more than 150 mm Hg. If baseline SBP was 140-150 mm Hg, the effect of treatment was not significant, and if baseline SBP was less than 140 mm Hg, treatment increased the risk of cardiovascular death by 15% (relative risk 1.15, 95% confidence interval 1.00 to 1.32). Results were not significant for the attained SBP analyses but showed similar patterns, towards risk reduction if SBP was more than 130 mm Hg and towards harm if SBP was less than 130 mm Hg. Both baseline and attained SBP significantly interacted with the effect of treatment in the same direction as for all cause mortality (P=0.002 and 0.010, respectively). Metaregression analyses showed 15 percentage points worse treatment effect on cardiovascular mortality for each 10 mm Hg lower baseline SBP (P=0.015), crossing the zero line from benefit towards harm at 141 mm Hg.
For myocardial infarction, treatment was beneficial if baseline SBP was more than 140 mm Hg and attained SBP was more than 130 mm Hg. If SBP was less than 140 mm Hg at baseline or less than 130 mm Hg during treatment, however, there was no association between treatment and risk. Interaction was significant between baseline SBP and treatment effect, but not for attained SBP (P=0.017 and P=0.476, respectively). Metaregression showed 12 percentage points worse treatment effect on myocardial infarction for each 10 mm Hg lower baseline SBP (P=0.011), crossing from benefit towards harm at 132 mm Hg.
The risk of stroke was reduced if baseline SBP was more than 140 mm Hg and attained SBP was less than 140 mm Hg. The lowest SBP stratum, for both baseline and attained SBP, had wide confidence intervals, reflecting low numbers of events. Both interaction analyses and metaregression analyses were not significant for both baseline and attained SBP.
The risk of heart failure decreased with treatment if baseline SBP was more than 140 mm Hg and attained SBP was more than 130 mm Hg. For the lowest stratum, however, the effect of treatment was not significant. For end stage renal disease, the only subgroup showing a positive effect of treatment was that with a baseline SBP of more than 150 mm Hg. For both the baseline and attained analyses, the point estimate in the lowest strata was close to 1. Interaction tests and metaregression analyses were negative for heart failure and end stage renal disease.
The web appendix presents non-stratified meta-analyses, meta-analyses stratified according to baseline and in-treatment DBP, and meta-analyses stratified according to differences in SBP and DBP between groups. We observed similar patterns in the DBP analyses as in the SBP analyses. There was a significant interaction between baseline and attained DBP and cardiovascular mortality. Metaregression showed the risk of cardiovascular mortality to increase by 28 percentage points for each 10 mm Hg lower baseline DBP (P=0.013), crossing from benefit towards harm at 78 mm Hg. Non-cardiovascular mortality was analysed according to protocol, and was not affected by treatment in any subgroup.
The web appendix presents risk of bias assessment, with explanatory text.
In our overall meta-analyses we judged the risk of bias as low, although it was high for some trials. One trial (DIabetic REtinopathy Candesartan Trials-Protect 2, DIRECT-P2) was judged to have high risk of bias in three domains. We performed sensitivity analyses excluding this trial from the stratified analyses. This shifted the effect measures of all cause and cardiovascular mortality slightly more towards harm, but did not change the significance level for any outcome.
Discussion
This systematic review and meta-analyses confirms that blood pressure lowering treatment is associated with reduced mortality and cardiovascular morbidity in people with diabetes mellitus, if systolic blood pressure (SBP) before treatment is more than 140 mm Hg. If SBP is less than 140 mm Hg, however, we found no benefit, but potential harm, with an increased risk of cardiovascular death. This fits well with our analyses stratified by attained SBP. Treatment reduced the risk of all cause mortality, myocardial infarction, stroke, and heart failure, if SBP was treated to 130-140 mm Hg, but was associated with a non-significant increase in all cause and cardiovascular mortality if SBP was lowered to less than 130 mm Hg. The results are further supported by metaregression analyses showing that treatment effect on cardiovascular mortality and myocardial infarction is worse for each unit decrease in baseline SBP, and harmful below certain levels.
Strengths and limitations of this review
This review has some limitations that are general to meta-analyses without access to individual patient data, including not being able to account for patient characteristics in a sophisticated way or analyse blood pressure levels within trials. Six other considerations should be borne in mind. Firstly, we identified more potentially eligible trials than could be included in the final analyses. These were trials in which we either knew there were people with diabetes but did not receive data on these participants, or trials in which there were no data on inclusion but participation by people with diabetes could not be excluded. Hence, despite our efforts, additional data exist that are not included in our analyses. Secondly, our analyses are stratified on mean baseline and attained blood pressure within trials. This is an aggregated variable, which opens our results to potential ecological bias. One way to reduce this risk of bias would have been to stratify on eligibility criteria or blood pressure targets instead of on measured values. However, the blood pressure range accepted in each trial is usually wide, with great overlap between trials, making stratification on this variable virtually impossible. Thirdly, we see no increase in the risk of myocardial infarction or stroke, corresponding to the increase in cardiovascular mortality in the lowest SBP strata. This could have two possible explanations. Case fatality might increase with intensive treatment, reflecting lower margins to handle an event with lower blood pressure. It could also reflect stricter definitions for myocardial infarction and stroke in the included trials than those used for cardiovascular mortality. For example, all unexpected deaths, deaths out of hospital, and deaths without known causes, usually qualify as cardiovascular mortality, but not as any specific event. Fourthly, most of the included trials were not designed to test different blood pressure targets but rather randomised patients to drug versus placebo. Thus, if blood pressure independent drug effects were present, they could affect our results. A recent systematic review showed no difference in treatment effect between drug classes for all cause and cardiovascular mortality.73 Also, all trials that randomised patients to specific drugs in the lowest blood pressure strata used renin angiotensin system (RAS) blockers. It has been suggested that these agents have a positive effect beyond that of blood pressure lowering,48 but still the main results in this stratum were negative. It is thus unlikely that the observed treatment effects in this review are related to drug class. Fifthly, the ALiskiren Trial In Type 2 Diabetes Using Cardio-Renal Endpoints (ALTITUDE) is given large weight in all meta-analyses within the baseline SBP stratum of less than 140 mm Hg. This was a trial of aliskiren, a renin inhibitor, in addition to previous inhibition of RAS.28 Double RAS blocker treatment is no longer recommended as standard treatment in any patient group.9 10 11 We therefore performed a sensitivity analysis, excluding ALTITUDE from the cardiovascular mortality analysis, to test its impact. Importantly, this did not change the point estimate but widened the confidence intervals, indicating that the treatment effect is consistent across trials but that the power to establish such an effect is insufficient without ALTITUDE. In line with this, the shift in significance for cardiovascular mortality and stroke, between the baseline and attained SBP analyses, can also be attributed to ALTITUDE. Although baseline SBP was less than 140 mm Hg, this trial did not lower SBP to below 130 mm Hg. Sixthly, the majority of participants in the included trials in our meta-analyses had type 2 diabetes and were already treated with one or more antihypertensive agents. Therefore, generalisability to people with type 1 diabetes, and people naive to treatment, is probably limited.
Comparison with other studies
Our results are mostly in line with those of a recently published review by Emdin and colleagues.13 Both reviews confirm the protective effect of treatment if SBP is more than 140 mm Hg, and that the benefit decreases with decreasing blood pressure. However, the results differ on three important findings. Firstly, we show an increased risk of cardiovascular death, an outcome not analysed by Emdin and colleagues. Secondly, Emdin and colleagues showed a decreased risk of stroke, even if baseline SBP was less than 140 mm Hg, which we do not. Thirdly, Emdin and colleagues showed a decreased risk of albuminuria, an outcome we did not analyse. The reviews differ on two methodological points: we include data from 21 additional trials, compared with the stratified analyses in the previous review; and Emdin and colleagues standardised risk ratios and weights according to SBP reduction within trials, whereas we used non-standardised data. In the case of stroke, the difference in results between the two reviews can be explained by the standardisation used by Emdin and colleagues. In their standardised model, the Action to Control Cardiovascular Risk in Diabetes (ACCORD) trial is given more than 90% weight in the meta-analysis, although it contributed less than 25% of the events in the included trials.23 On the other hand, ALTITUDE is given only 2% weight in the meta-analysis, although it contributed more than 60% of the events.28 This strongly suggests a study weight bias in the standardised model. Albuminuria should be regarded as a surrogate for end stage renal disease. In our analyses of trials with baseline SBP less than 140 mm Hg, there was no tendency towards reduction of this outcome (relative risk 0.97, 95% confidence interval 0.80 to 1.17). Even if the best possible scenario, with respect to confidence intervals for end stage renal disease, was true, the absolute number of cardiovascular deaths exceeds that of end stage renal disease, and hence the numbers needed to treat would exceed the numbers needed to harm. The absence of a beneficial effect on stroke if baseline SBP is less than 140 mm Hg also differs compared with another review, including both people with diabetes and people with impaired fasting glucose.8 It is reasonable to think that the vessels of people with impaired fasting glucose are less affected than those of people with manifest diabetes, and hence they might be less sensitive to, and perhaps more helped by, additional blood pressure lowering. Recently, the results of the Systolic Blood Pressure Intervention Trial (SPRINT) were published.74 This was a randomised controlled trial comparing a systolic blood pressure target of less than 120 mm Hg with one less than 140 mm Hg, in high risk patients with moderately elevated blood pressure. The trial was stopped preterm owing to a highly significant reduction in all cause mortality, suggesting that this population might benefit from very aggressive blood pressure treatment. Importantly, patients with diabetes mellitus were excluded from the trial. Thus our results, combined with those from SPRINT, suggest that blood pressure treatment targets should be less aggressive in people with diabetes than in those without diabetes.
Potential explanation of findings
The concept of a J-shaped, or U-shaped, curve for the relation between blood pressure and cardiovascular disease has been shown previously in observational settings.75 76 This has often been dismissed as due to possible confounding.77 It is highly unlikely, however, that our results would be due to confounding. This is because we analyse relative risks between groups with the same baseline blood pressure but randomised to different blood pressure levels, thereby preserving the element of randomisation in our meta-analyses.
The most likely biological explanation for our findings is that intensive treatment impairs blood flow to end organs, leading to ischaemia.77 In patients with stenosis of the coronary arteries, decreased diastolic blood pressure (DBP) has been shown to lead to lower fractional flow reserve over the stenosed segment, in turn leading to myocardial hypoperfusion.78 In arterial stiffening, commonly present in people with diabetes, myocardial perfusion is increasingly dependent on SBP.79 This could, at least partly, explain the association between low SBP and worse treatment effect in our analyses. Impaired myocardial perfusion, compared with the superior autoregulation of cerebral blood flow, could also explain the different effects of blood pressure levels on myocardial infarction and stroke. Another potential explanation for our findings is that low blood pressure leads to less coronary collateral circulation. It has been hypothesised that low blood pressure leads to reduced endothelial stress, the driver of arteriogenesis, and an association between DBP and coronary collaterals has been shown in cross sectional data of patients with coronary occlusion.80 This could explain not only an increased number of events with treatment but also a worse prognosis when having an event, as reflected by the possible increase in case fatality suggested by our analyses.
Conclusions and implications
This systematic review and meta-analyses included a large amount of previously unpublished data, thereby increasing precision compared with previous research. Results from the analyses stratified by baseline SBP are largely consistent with those stratified by attained SBP. The interaction between blood pressure and treatment effect is reproducible across exposure variables and outcomes, indicating a robust dose-response relation. Together with a possible biological mechanism, our results suggest that SBP before treatment modifies the effect of treatment in a causal way.
The results are important both conceptually for research on hypertension and for clinicians. Firstly, we show that not only the absolute, but also the relative benefit of blood pressure lowering is attenuated at lower blood pressures. This suggests that the linear relation between blood pressure and cardiovascular disease seen in some observational studies cannot be extrapolated to assumed benefit of treatment. Stretching this further, we show, based on randomised comparisons, that treatment below a certain blood pressure level might be harmful. Secondly, and contrary to what has previously been recommended, our results, combined with those from the SPRINT trial, suggest that blood pressure treatment goals should be less aggressive in people with diabetes than without diabetes. This review strongly supports blood pressure treatment in people with diabetes mellitus if SBP is more than 140 mm Hg. If SBP is already less than 140 mm Hg, however, adding additional agents might be harmful.
What is already known on this topic
Hypertension is the most important risk factor for mortality and cardiovascular disease worldwide
People with diabetes mellitus are at increased risk of cardiovascular disease and often have concomitant hypertension
Antihypertensive treatment reduces the risk of cardiovascular disease in people with diabetes mellitus, but the optimal blood pressure level has been debated
What this study adds
In people with diabetes mellitus and a systolic blood pressure of more than 140 mm Hg, antihypertensive treatment is associated with a reduced risk of mortality and cardiovascular disease
In people with diabetes mellitus and a systolic blood pressure of less than 140 mm Hg, however, antihypertensive treatment is associated with an increased risk of cardiovascular death
The interaction between systolic blood pressure before treatment and the treatment effect is significant
Footnotes
We thank the following authors for sharing previously unpublished data, without receiving economic imbursement or any other personal gain: Piero Ruggenenti (BENEDICT), Kathy Wolski (CAMELOT), Lutgarde Thijs (EWPHE and Syst-Eur), Yuhei Kawano (JATOS), Stephan Lüders (PHARAO), Hisatomi Arima (PROGRESS), Lars Hjalmar Lindholm (STOP), Inder Anand (VAL-HEFT), and Hiromi Rakugi (VALISH). We also thank AstraZenica for sharing data from HOT, and the National Heart, Lung, and Blood Institute for sharing data from PEACE, SHEP, and SOLVD.
Contributors: Both authors contributed equally to all aspects of study design and conduct, and the writing of the manuscript. BC is guarantor.
Funding: This study was funded by Västerbotten County Council. The design and conduct of the study, the interpretation of data, and the writing of the manuscript, was done solely by the authors, independent of the funder.
Competing interests: All authors have completed the ICMJE uniform disclosure form at www.icmje.org/coi_disclosure.pdf and declare: no support from any organisation for the submitted work; no financial relationships with any organisations that might have an interest in the submitted work in the previous three years; no other relationships or activities that could appear to have influenced the submitted work.
Ethical approval: This study was approved by the regional ethical review board at Umeå University.
Data sharing: Results from all meta-analyses are presented in appendix. Additional data, including full forest plots are available on request.
Transparency: The lead author (MB) affirms that the manuscript is an honest, accurate, and transparent account of the study being reported; that no important aspects of the study have been omitted; and that any discrepancies from the study as planned have been explained.
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 3.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/3.0/.