Article Text

Abstract
Objective To identify the factors associated with 12-month mental health service use in primary care patients with depressive symptoms.
Design Cross-sectional followed by 12-month cohort study.
Setting and participants 10 179 adult patients were recruited from the waiting rooms of 59 primary care clinics across Hong Kong to complete a questionnaire which screened for depression. 518 screened-positive participants formed the cohort and were telephoned at 3, 6 and 12 months to monitor mental health service use.
Primary and secondary outcomes ▸ Help-seeking preferences;
▸ Intention to seek help from a healthcare professional;
▸ 12-month mental health service use.
Results At baseline, when asked who they would seek help from if they thought they were depressed, respondents preferred using friends and family (46.5%) over a psychiatrist (24.9%), psychologist (22.8%) or general practitioner (GP; 19.9%). The presence of depressive symptoms was associated with a lower intention to seek help from family and friends but had no effect on intention to seek help from a healthcare professional. Over 12 months, 24.3% of the screened-positive cohort reported receiving services from a mental health professional. Factors associated with service use included identification of depression by the GP at baseline, having a past history of depression or other mental illness, and being a public sector patient. Having a positive intention to seek professional help or more severe depressive symptoms at baseline was not associated with a greater likelihood of receiving treatment.
Conclusions Mental health service use appears to be very low in this setting with only one in four primary care patients with depressive symptoms receiving treatment from a psychiatrist, GP or psychologist over a year. To help reduce the burden of illness, better detection of depressive disorders is needed especially for patients who may be undertreated such as those with no prior diagnosis of depression and those with more severe symptoms.
- PRIMARY CARE
- EPIDEMIOLOGY
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Strengths and limitations of this study
Participants were recruited from a wide variety of primary care settings, reflecting the delivery of primary care in Hong Kong, and were monitored prospectively to examine the correlations between intention and subsequent actual behaviour.
We relied on the patient's self-report for collection of information on help seeking actions. It is possible that general practitioners or other providers may have provided psychological care as part of a general consultation, but that patients did not perceive this as receiving mental health treatment, resulting in an under-reporting of mental health service use.
The study's findings are only applicable to our study population any may not reflect the whole of Hong Kong's primary care population.
Introduction
Depression is a common condition affecting the quality of life and contributing to the global burden of disease.1 In many countries, depression is mainly managed in the primary care setting and primary care clinicians are well placed to detect, initiate and coordinate care.2 Unfortunately, many adults experiencing a depressive episode will not seek help immediately, and worldwide, delays or complete failure in seeking treatment for depression are common.3 Studies have shown that in those reporting an intention to seek help to overcome depression, most would prefer to receive support from within their social network than from a healthcare provider.4 As a consequence, even in the primary care setting where patients already have access to a clinician, many patients may not disclose their mood symptoms and subsequently fail to be identified by the doctor as having depression or to receive appropriate medical care.5
The decision whether or not to seek help, and whom to seek help from, may be influenced by culture, demography, service accessibility, symptom severity and personal attitudes towards mental illness such as the individual's understanding of the illness, their perceived usefulness of treatments and impressions from their own past help-seeking experiences.6–8 It has been identified that the Chinese underutilise mental health services; however, low service demand does not necessarily reflect low service need.9 ,10 Despite living in a relatively westernised society, the health beliefs and behaviours of most Hong Kong Chinese are strongly influenced by traditional cultural values where emotional problems may not be perceived as an illness and strong stigmatising attitudes towards mental illness are highly prevalent.7 ,11 Aside from personal attitudinal and sociocultural barriers, there are also many practical barriers to receiving help for mental health. Detection rates for depression are relatively low in primary care12 ,13 and access to psychosocial services is difficult due to the user-pay system in the private sector,14 and long waiting times in the public sector.11 ,10
To gain a better understanding about the help-seeking behaviours of Chinese primary care patients, the objectives of this study were to explore where patients prefer to go for psychological care; to identify the factors associated with a positive intention to seek help from a healthcare professional; and to identify the predictors for 12-month mental health service use among patients with depressive symptoms.
Our three hypotheses were:
Patients experiencing depressive symptoms are less likely to report a positive intention to seek help from a healthcare professional for their mental health;
In patients experiencing depressive symptoms, a positive intention to seek professional help for mental health is a predictor for subsequent 12-month mental health service use;
Severity of depressive symptoms is a predictor for subsequent 12-month mental health service use.
Methods
This was a 12-month prospective longitudinal cohort study (figure 1). It was conducted as part of a larger epidemiological study to examine the naturalistic outcomes of depressive disorders in Hong Kong's primary care.12 ,15
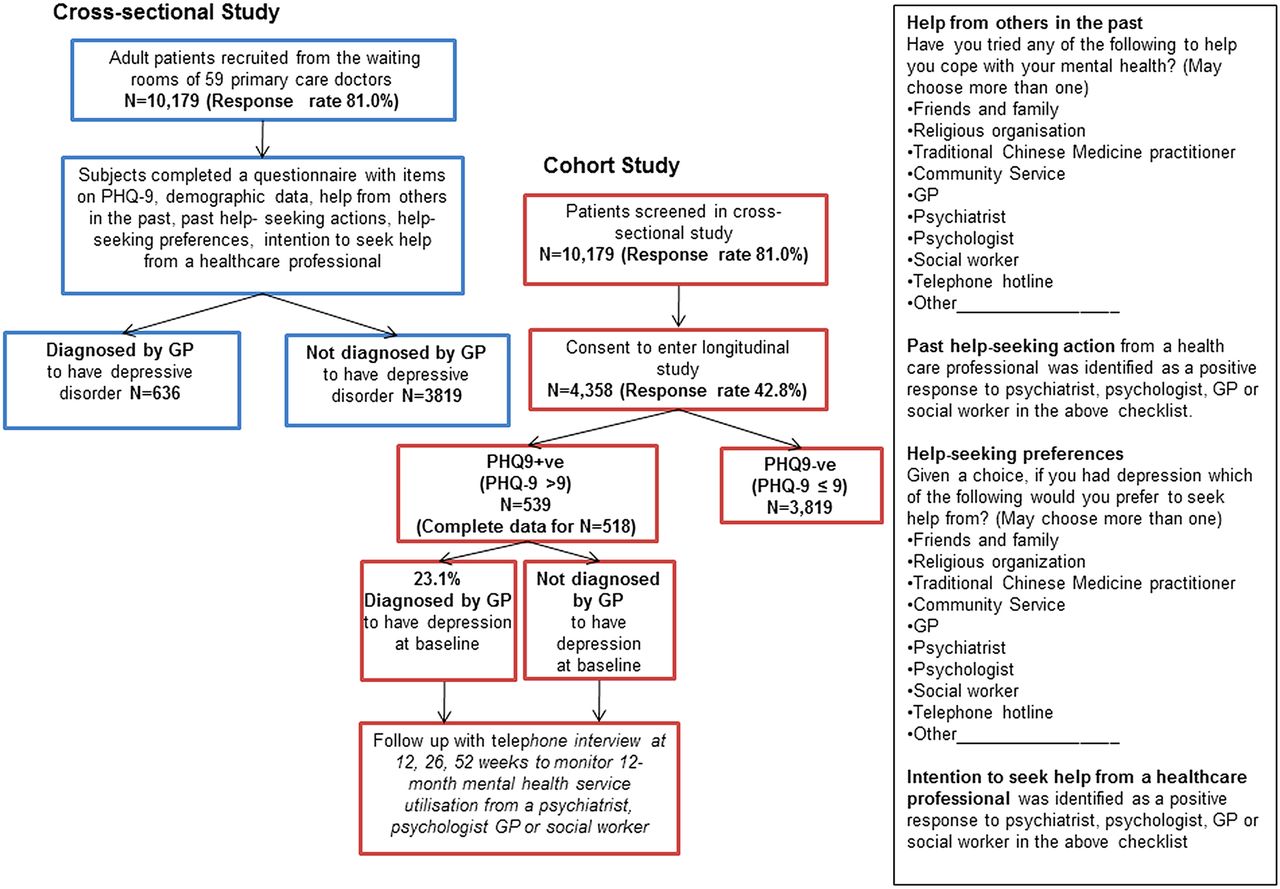
{kind=link}
Study design (GP, general practitioner; PHQ, Patient Health Questionnaire).
Participants and sampling
Patients were recruited from the waiting rooms of 59 primary care clinicians across Hong Kong and consisted of patients from the private sector, public sector and non-governmental organisations, reflecting the delivery of primary care services in this setting. The doctors were identified through the mailing list of the Hong Kong College of Family Physicians and joined this study voluntarily as part of a mental health primary care practice-based research network.
All eligible adult patients consulting the study doctor on one randomised day each month over 12 months were consecutively recruited to complete a baseline questionnaire. Participants who screened positive for depression and who consented to longitudinal follow-up formed the cohort sample and were subsequently monitored by telephone interview at 3, 6 and 12 months. Patients were excluded if they were aged <18 years, unable to communicate in English, Cantonese or Mandarin, or unable to complete the questionnaire due to cognitive difficulties.
Study instruments
The Patient Health Questionnaire-9 (PHQ-9) is a nine-item questionnaire used to screen, monitor, diagnose and measure the severity of depressive symptoms. A cut-off score >9 was used to define a case of screened-positive depression (‘PHQ+ve’). The Chinese version of PHQ-9 has been validated in Hong Kong among 357 adult participants from 14 primary care clinics using the Chinese Hamilton Depression Scale (CHDS) as the gold standard. Using a cut-off point >9, PHQ-9 was found to have a sensitivity of 80% and specificity of 92%. PHQ-9 can also be used to measure the severity of symptoms (score 1–4 minimal; 5–9 mild; 10–14 moderate; 15–19 moderately severe; 20–27 severe).16
Items on sociodemography and comorbidity were adapted from previously used health services research surveys on the Hong Kong primary care population.17
Help from others in the past: To examine past help-seeking behaviours, respondents were asked: “Have you tried any of the following to help you cope with your mental health?” Response options included: friends/family; religious organisation; traditional Chinese medicine (TCM) practitioner; community services; general practitioner (GP); psychiatrist; psychologist; social worker; telephone hotline; other (please explain). Respondents were permitted to choose more than one option.
Past help-seeking action was defined as a patient's self-report of having received a mental health service from a healthcare professional in the past and was identified by a checked response to the GP, psychiatrist, psychologist or social worker options in the item on ‘help from others in the past’.
Help-seeking preferences: To examine help-seeking preferences, respondents were asked: “Given a choice, if you had depression, which of the following would you prefer to seek help from?” Response options included: friends/family; religious organisation; TCM practitioner; community services; GP; psychiatrist; psychologist; social worker; telephone hotline; other (please explain). Respondents were permitted to choose more than one option.
Intention to seek help from a healthcare professional: was defined as a patient's self-reported intention to seek help from a healthcare professional if they thought they were depressed and was identified as checked response to the GP, psychiatrist, psychologist or social worker options in the item on ‘help-seeking preferences’.
Subsequent 12-month mental health service use: Participants who consented to longitudinal follow-up were telephoned at 12, 26 and 52 weeks to monitor for subsequent mental health service use. Respondents were asked to report whether they had received mental health treatment or psychological counselling from a psychiatrist, GP, psychologist or social worker in the previous 3 months. The subset of the cohort sample who had screened positive for depression at baseline was used to identify predictors for 12-month mental health service use.
Doctor's case report form: At baseline, study doctors blinded to their patient's PHQ-9 screening scores were asked to document on a case report form whether or not they thought their patient had depression. This was used to examine detection rates for depression.
Analysis
Using a PHQ-9 cut-off score of >9 to define a screened-positive case, the prevalence of depression was estimated with a 95% CI taking into account the clustering effect by the study doctor.
Proportional differences in help-seeking between the patient subgroups that screened PHQ-9 positive and negative were examined using χ2 tests of independence.
Multiple logistic regression analyses were conducted to inspect the predictive significance of each of the patient demographic variables and self-reported clinical characteristics towards (1) a positive intention to seek help from a healthcare professional (reported at baseline), (2) having received psychological help from a psychiatrist, psychologist, GP or social worker in the past (reported at baseline) and (3) use of mental health services during the 12-month follow-up period (among the subset of follow-up cohort who screened PHQ-9 positive at baseline). In view of the relatively large sample size and possible data distortion with using missing data treatments, complete-case analysis was adopted for all regression models. All patient variables were entered in a single block and all were retained in the final model since the purpose of this study is not to build the most parsimonious predictive models. Nevertheless, the Hosmer and Lemeshow test statistics were reported to show how well each model fit the data, with a non-significant χ2 goodness of fit at p>0.05 to indicate an adequate model fit. The statistical software SPSS V.21 was used for all quantitative analysis.
Sample size calculation
Previous literature showed that 33% of people with mental disorders were treated in the USA.18 Applying a well-known rule of thumb (1 in 10 rule)19 and with a total of 16 potential predictors considered, at least 485 patients were needed to evaluate the predictors for 12-month mental health service use. The full study protocol including sample size calculations for the larger epidemiological study has been published previously.15
Results
A total of 10 179 patients completed the survey at baseline (response rate of 81.0%). Respondents were recruited from public settings (26.0%) and private settings (74.0%) in alignment with the overall delivery of primary care services in Hong Kong.20 From the participants of the baseline survey, 4358 respondents consented to longitudinal follow-up (response rate of 42.8%) consisting of 539 participants who screened PHQ-9 positive (‘PHQ+ve’) and 3819 participants who screened PHQ-9 negative (‘PHQ−ve’). Complete data were available for 518 of the PHQ+ve participants forming the cohort sample for analysis. The demographic characteristics of the cross-sectional and cohort participants stratified by their PHQ-9 screening status are shown in table 1. In terms of demographic characteristics, the overall cohort sample was marginally older (mean age 49.6 vs 49 years); marginally more educated; and there were slightly more females than in the overall baseline sample. In terms of severity, 68.1% of the PHQ+ve cohort were categorised as being of moderate severity (PHQ-9 score 10–14), and 31.9% were categorised as being moderately severe or severe (PHQ-9 scores 15–19 and 20–27).
Characteristics of the cross-sectional and cohort participants by PHQ-9 status
Prevalence and detection of depression
The cross-sectional prevalence of PHQ+ve screening was 10.69% (95% CI 9.71% to 11.67%). Among the PHQ+ve participants, study doctors identified 23.1% as having depression. The prevalence of patient self-reported history of depression diagnosed by a doctor was 6.64%.
Past help-seeking behaviours
Among the cross-sectional survey respondents (N=10 179), 54.1% (n=5503) overall and 65.6% of those who screened PHQ+ve reported having sought help from others in the past to cope with their mental health from either friends/family; religious organisation; TCM practitioner; community services; GP; psychiatrist; psychologist; social worker; telephone hotline or ‘other not otherwise specified’. From these responses, it was observed that 6.9% (n=697) of all respondents and 17.5% of those who screened PHQ+ve reported at least one prior help-seeking action from a healthcare professional (either a psychiatrist, psychologist, GP and/ or social worker). A multiple logistic regression identifying the characteristics of patients who had sought help in the past from a psychiatrist, psychologist or GP is shown in table 2. Characteristics of patients who had received help in the past from a GP included: lived on Hong Kong Island (relative to living in the New Territories and Outlying Islands); had one or more medical comorbidities; had a history of depression or other mental illness; had a PHQ-9 score >9 at baseline; was a public sector patient. Characteristics of patients who had received help from a psychiatrist in the past included: had a history of depression or other mental illness. Characteristics of patients who had received mental healthcare from a psychologist in the past included: younger age; had attained a secondary education or above; non-married (single, divorced or widowed); had a household income >HK$30 000; had a history of depression or other mental illness. Parallel analyses for social workers could not be reliably estimated due to the small group size.
Characteristics of patients with past help-seeking actions from a GP, psychiatrist or psychologist*
Help-seeking preferences and intention to seek help for depression
Among the 10 179 cross-sectional survey respondents, 69.6% (n=7080) reported that they would seek help from other people if they thought they were depressed, preferring friends and family (46.5%) to a psychiatrist (24.9%), psychologist (22.8%) or a primary care physician (19.9%). The patient's self-reported help-seeking preferences for depression stratified by PHQ-9 screening status are shown in table 3. Overall, there were no significant differences in the proportion of respondents who screened PHQ-9 positive or negative for any of the healthcare profession categories; however, it was observed that those who screened positive for depression were less likely to report that they would seek help from family and friends, but more likely to report that they would seek help from a TCM practitioner. In relation to the first hypothesis, it appears that the presence of depressive symptoms may have an impact on the patient's intention to seek help from informal and alternative sources but not on their intention to seek help from healthcare professionals.
Patient help-seeking preferences by PHQ-9 status*
Characteristics associated with a positive intention to seek help from a healthcare professional (psychiatrist, psychologist, GP or social worker) were identified using logistic regression analysis (table 4). The most significant predictor of a positive intention to seek help from a healthcare professional was having received help in the past from a healthcare professional. Other demographic factors associated with a positive intention to seek help from a healthcare professional included: higher household income; family history of mental illness; being female; being aged 18–34 years (compared with being aged >55 years); higher educational levels and being married. There was no relationship between PHQ-9 score and intention to seek help from a healthcare professional.
Factors associated with patient-reported intention to seek help from a healthcare professional*
Predictors for subsequent 12-month mental health service use in patients with depressive symptoms
Baseline respondents who had consented to longitudinal follow-up were recruited into the cohort study and were monitored by telephone interview at 12, 26 and 52 weeks and asked about mental health service use in the previous 3 months. Among the cohort sample who had screened PHQ+ve at baseline and who had complete follow-up data (N=518), 24.3% (n=126) reported receiving mental healthcare from a healthcare professional during the subsequent 12-month follow-up. Cumulatively over 12 months, 21.7% reported that they had consulted a psychiatrist or psychiatric clinic, 11.6% reported having received psychological treatment or counselling from a GP, and 3.6% from a psychologist. Multiple logistic regression analyses were performed to identify the predictors for subsequent mental health service use from a healthcare professional (table 5). Predictors included: having a history of depression or other mental illness; identified as being depressed at baseline by the study doctor; attended a public sector clinic; having received help from a healthcare professional to help with their mental health in the past. In relation to the second hypothesis, a positive intention to seek help from a healthcare professional at baseline did not predict subsequent mental health service use and over 12 months, and there was no association between a positive intention to seek help from a healthcare professional at baseline and subsequent 12-month mental health service use.
Factors associated with a 12-month subsequent mental health service use*
In relation to the third hypothesis, there was no correlation between the PHQ-9 severity and 12-month mental health services and patients with moderately severe or severe symptoms of depression were not more likely to receive a mental health service than those who had only mild or moderate symptoms of depression.
Characteristics of patients who reported having received mental health services from a GP and from a psychiatrist are also shown in table 5. Detection of depression by the primary care doctor was associated with an increased likelihood of receiving 12-month mental health services; however, on subgroup analysis, detection was not associated with subsequent GP-provided mental health services, but was associated with subsequent psychiatrist-provided mental health services. Parallel analyses of health service use from a psychologist or social worker could not be reliably estimated due to the small group size and incomplete data.
Discussion
The purpose of this study was to explore where Chinese primary care patients go to seek help for depression, and to identify the predictors for mental health service use. By using a cohort design, we were able to examine the factors associated with 12-month mental health service use and test the relationship between intention to seek help and subsequent service uptake.
Help-seeking preferences and intention to seek help from a healthcare professional for depression
Our first hypothesis was that patients experiencing depressive symptoms are less likely to report a positive intention to seek help from a healthcare professional. On the one hand, depression can diminish self-efficacy and make individuals question their ability to accomplish tasks, such as booking a doctor's appointment.5 On the other hand, depression can cause impairment to quality of life motivating people to seek help to alleviate their distress. In our study sample, the presence of depressive symptoms had no effect on intention to seek help from a healthcare professional. This was similar to a previous study conducted in Hong Kong which found no significant effect of mental health status on help-seeking intention.11 One possibility is that the social stigma associated with mental illness may be so strong in the Chinese culture that sociocultural factors have a greater influence on help-seeking intention than actual service need.
Although it was observed that depressive symptoms did not have any effect on intention to seek help from a healthcare professional, our findings revealed that depressive symptoms did affect intention to seek help from family and friends. For most individuals, seeking help from friends and family is less threatening and more readily accessible than seeking professional help and Chinese patients often consult their family to confirm concerns and receive endorsement before seeking professional help.7 When an individual is not depressed, they may be more optimistic about the effect of family and friends in supporting them to cope with mental health issues. In the presence of a depressed mood, however, the associated negative thinking may make individuals less likely to want to share their problems with family and friends as they may feel that they are just an added burden, their perception of the usefulness of family and friends may be altered, or the poor quality of life may make them preferentially seek other sources of help.7
Although only a small number of participants reported that they would seek help from a TCM practitioner, the presence of depressive symptoms also appeared to have an effect. This may be related to the nature of TCM, which is philosophically more holistic and aims to achieve balance rather than cure. One possibility is that patients who are experiencing depressive symptoms may perceive themselves as feeling ‘out of balance’ or having a lack of well-being, which may make them more likely to report that they would seek help from a TCM practitioner. As many patients in our setting use both western and Chinese medicine, greater exploration is needed to understand why patients may prefer to seek help from a TCM practitioner for depression and the role of TCM in the delivery of depression care.
Overall, while 70% of respondents reported that they would seek help from others, around 30% appear to not want any outside help. Although this group was not studied in detail, it is apparent that a significant proportion of primary care patients do not intend to seek help from any external source if depressed. Further exploration is needed to better understand the unmet needs of patients who do not wish to seek help and how they can be addressed.
Predictors for subsequent 12-month mental health service use
Our second and third hypotheses related to predictors for 12-month mental health service utilisation in patients with depressive symptoms. We hypothesised that a positive intention to seek help from a healthcare professional and severity of depression could predict subsequent 12-month mental health service use. From our findings, however, a positive intention to seek help from a mental health professional and a higher severity of depression had no effect on subsequent mental health service use. Using Ajzen's theory of planned behaviour,6 an individual's behaviour may be influenced by their own personal beliefs (patient's own attitudes), subjective norms (the social norms) and control beliefs (perceived practical barriers).6 ,21 In our study population, it appears that the patient's intentions regarding help-seeking was an insignificant contributor to subsequent mental health service utilisation. Conversely, identification of depression by a doctor was a very strong predictor for subsequent action. It seems that being told that you have depression by a doctor can enable people who would otherwise not seek help to receive mental health treatments. One possible explanation is that when individuals are given the diagnosis of depression by doctor, they may be more accepting about seeking mental health treatments. Another possibility is that doctor detection facilitates access to care by overcoming some of the practical barriers to treatment such as knowing where to go.
Unfortunately, we found that PHQ severity was not a predictor for subsequent health service utilisation and that higher severity of symptoms at baseline was not associated with a greater likelihood of receiving subsequent mental health services as hypothesised. This suggests that patients with moderately severe to severe depressive symptoms, who potentially could benefit the most from mental health interventions, are not more likely to receive mental health services in our setting. Translated to quality of care, this potentially has quite serious repercussions in terms of suicide prevention and poor quality of life. A wider exploration of interventions may help to promote detection, and service uptake for these patients is needed to help reduce the burden of depressive illnesses in our community.
In the analyses of the factors associated with 12-month mental health service use, it was identified that detection of depression by a primary care doctor at baseline was associated with subsequent mental health service use; however, on further subgroup analysis, no association was found between GP detection and subsequent 12-month GP-provided mental health service use. Instead, GP detection was positively associated with receiving specialist psychiatric services. This suggests that after patients are diagnosed by the GP, they subsequently receive mental health services from a psychiatrist rather than from the primary care doctor. One possible explanation is that the respondents in this study were not aware that their GP provided a mental health service. On the other hand, some GPs may not have exhibited sufficient empathy or skill in treating the patient's mood disturbance, causing them to seek treatment from other sources.14 The WHO recommends that common mental illness should be treated in primary care and that specialist psychiatric services should be reserved for more severely ill patients.22 In Hong Kong, the role of the primary care doctor is poorly delineated, and patients can directly consult specialists in the private sector without a GP referral.14 This has significant service implications as many patients bypass the gatekeeping function of the primary care doctor causing further burden to an already stretched specialist psychiatric service sector where the population to specialist ratio is approximately 1:44 202.23 A closer examination of management practices by GPs may be warranted to identify whether it is feasible to transfer the delivery of care for depressive illnesses away from the specialist sector and into the primary care sector.
Strengths and weaknesses
This was the first wide scale epidemiological study to examine depressive disorders in Hong Kong's primary care. A major strength of this study was our success in enlisting a large number of primary care doctors to collaborate. Our wide sampling of practice types is reflective of the diverse service options available to patients seeking primary care in Hong Kong.
Our study has a number of notable limitations. Identification of patients with depressive symptoms was based on a screening instrument and a clinical diagnosis of depression was not confirmed by a diagnostic interview. We relied on the patient's self-report for collection of information on 12-month mental health service use, which incurs a risk of recall bias. It is possible that GPs or other providers may have provided psychological care as part of a general consultation, but that patients did not perceive this as receiving mental health treatment resulting in an underestimation of mental health services provided by GPs. Our study was restricted to patients recruited through a primary care research network in Hong Kong, and may not be generalisable to other primary care settings. The cohort sample was self-selected, which incurs a risk of self-selection bias. The findings are only applicable to our study population and may not reflect the whole of Hong Kong's primary care population. Finally, our study only collected data on patient demographics and preferences for seeking help. As we did not include any items to assess personal attitudes to mental health treatments or regarding stigmatism, we were unable to examine the relationship between specific patient attitudes and subsequent health service uptake, which is an area that warrants further study.
Conclusion
Although much has been written about what influences mental health help-seeking attitudes, much less is known about what influences actual behaviour. Of particular interest to mental health service research is how we can help people who experience mental health problems but who do not receive appropriate medical attention. In Hong Kong, patients prefer to seek help from close family and friends above that of a healthcare professional, and prefer to seek help from a psychiatrist for depression over that of a GP. Almost three-quarters of patients experiencing a depressive episode will not receive any mental health services over a year, and patients with more severe symptoms are not more likely to receive medical attention. GPs need to maximise opportunities to enhance the mental health of their patients by improving their detection rates for depression so that delays in initiation of treatment can be reduced.
Acknowledgments
The authors wish to acknowledge all the doctors of our Primary Care Research Network for their contribution to this study.
References
Footnotes
Contributors CLKL initially conceived the study. CLKL, TPL and WYC collectively designed and drafted the study protocol and sought funding and ethical approval. EYFW led the statistical analyses and contributed to the drafting of the manuscript. CLKL, TPL and KTYC contributed to recruitment and data collection. KTYC was the project coordinator, recruited and trained the fieldworkers, assisted with recruitment of study doctors, coordinated the data collection, and contributed to the drafting of the manuscript. WYC was the principal investigator of the funding application; he coordinated the research network and research team and drafted the manuscript. All authors have read the draft critically and approved the final manuscript.
Funding This work was supported by the Hong Kong Food and Health Bureau's Commissioned Research on Mental Health Policy and Service grant Reference No. SMH-27.
Competing interests None.
Ethics approval The Institutional Review Board of the University of Hong Kong/Hospital Authority Hong Kong West Cluster and all relevant regional and institutional ethics review boards.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement The data set is available on request by emailing the corresponding author at chinwy@hku.hk