Article Text

Abstract
Objective To determine whether drugs used in treatment of cardiovascular diseases (CVD-drugs), including hypertension, increase the risk of fragility fractures in individuals above the age of 65 years.
Design Retrospective nationwide cohort study.
Setting Danish nationwide national registers.
Participants All individuals in Denmark ≥65 years who used specified CVD-drugs in the study period between 1999 and 2012.
Main outcomes measures Time-dependent exposure to CVD-drugs (nitrates, digoxin, thiazides, furosemide, ACE inhibitors, angiotensin receptor antagonists, β-blockers, calcium antagonists and statins) was determined by prescription claims from pharmacies. The association between use of specific CVD-drugs and fragility fractures was assessed using multivariable Poisson regression models, and adjusted incidence rate ratios (IRRs) were calculated.
Results Overall, 1 586 554 persons were included, of these 16.1% experienced a fall-related fracture. The multivariable Poisson regression analysis showed positive associations between fracture and treatment with furosemide, thiazide and digoxin. IRRs during the first 14 days of treatment were for furosemide IRR 1.74 (95% CI 1.61 to 1.89) and for thiazides IRR 1.41 (1.28 to 1.55); IRR during the first 30 days of treatment with digoxin was 1.18 (1.02 to 1.37).
Conclusions Use of furosemide, thiazides and digoxin was associated with elevated rates of fragility fractures among elderly individuals. This may warrant consideration when considering diuretic treatment of hypertension in elderly individuals.
- accidental falls
- fragility fractures
- cardiovaslular drugs
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Strengths and limitations of this study
Large nationwide study including all individuals above the age of 65 years.
Owing to the large number of individuals included, it has been possible to investigate adverse events of specific drugs at specific time periods.
Linking between several national registers made it possible to adjust the analysis for comorbidity.
Observational design.
Bias due to confounding by indication cannot be fully excluded.
Introduction
Fragility fractures are fractures that result from mechanical forces that would not ordinarily result in fracture, known as low-level (or ‘low energy’) trauma. The WHO has quantified this as forces equivalent to a fall from a standing height or less.1 Fragility fractures are a major health problem for elderly people. Approximately 90% of all fragility fractures are due to falls.2 Among community-dwelling elderly populations, 30–60% fall at least once every year and serious injuries occur in 5–10% of all falls.3
With a growing elderly population, the prevalence of fragility fractures is increasing throughout the western world.4 At the same time, the prevalence of a number of chronic diseases is increasing and leads to an increase in use of medications, a situation which has led several researchers to speak of the ‘treatment burden’.5–7 With ageing, the ability to maintain homoeostasis declines and the risk of adverse effects when the organism is challenged by external or internal stimuli, like medications or diseases, increases.8 Furthermore, ageing is associated with a number of factors that influence pharmacokinetics and pharmacodynamics.9–12 Taken together, this makes the elderly individual susceptible to adverse effects from medical treatment. However, due to vague and atypical presentation of symptoms and diseases in elderly individuals, the adverse effects may not be recognised as such.13 Several drugs used in treatment of cardiovascular disease have been associated with falls and fragility fractures.14–16 However, the evidence is sparse.17 ,18 There are no randomised controlled studies, and the existing observational studies generally include small populations and are heterogeneous concerning populations, settings and definition of falls.14 ,15 ,19
Several methodological difficulties can explain the lack of randomised trials in this group of patients. The randomised controlled trial design builds on the assumption that it is possible to have two groups of patients who are comparable apart from the intervention that the study seeks to investigate. This assumption may be difficult to meet when studying frail elderly individuals, since genetic differences, lifelong living habits and different environments all contribute to increase interindividual heterogeneity with ageing. Elderly patients tend to have comorbidity, which means that they are excluded from the majority of clinical trials.20 ,21 Even a study designed to investigate the effect of antihypertensive treatment in persons >80 years included the healthiest segment and the authors stated, “it would be premature to extrapolate the results from HYVET to patients in this age group who are more frail”.22 Furthermore, it may be too demanding for frail elderly individuals to participate in randomised trials. Taken together, these difficulties lead to randomised trials not including the clinical relevant patients.23–29 Commonly used end points in trials investigating effects of CVD drugs are cardiovascular mortality, cerebrovascular events and all-cause mortality. Fractures leading to hospitalisation will be registered as adverse events, but the trials are not powered to investigate falls or fractures as an end point.
To overcome some of these gaps in current knowledge, we performed a nationwide register-based study in order to investigate the effect of medical treatment for cardiovascular disease on the occurrence of fragility fractures in elderly individuals. The large population allowed us to investigate the effect of specific drugs and time intervals.
Methods
Study population
We included all residents in Denmark aged 65 years or older between 1 January 1999 and 31 December 2012. Individuals were followed from either 1 January 1999, their 65th birthday, or at their date of immigration (if older than 65 years at immigration) until a diagnosis of a fall-related fracture, emigration, death or 31 December 2012, whichever occurred first.
Databases
This study is a nationwide register-based Danish cohort study. For administrative purposes, every person in Denmark has been given a unique personal identification number since 1968. This enables individual-level linkage of Danish citizens through several national registries. In the present study, we used data from the Danish Civil Registration System, the Danish National Patient Registry, and the Danish Registry of Medicinal Products Statistics. The Danish Civil Registration System contains information about dates of birth and death of all Danish citizens since 1968.30 The Danish National Patient Registry contains records of all hospitalisations in Denmark since 1977.31 The Danish Registry of Medicinal Products Statistics contains data on all prescriptions dispensed in Denmark since 1994, including information about medicine strength, quantity dispensed and dispensing date. Prescriptions are classified according to the Anatomical Therapeutic Chemical (ATC) system.32
Outcome assessment
Fragility fractures were identified in the Danish National Patient Registry if individuals were hospitalised with the diagnosis of one of the following diagnoses classified with the International Classification of Diseases, 10th revision (ICD-10): fracture of sacrum (S321), fracture of coccyx (S322), fracture of ilium (S323), fracture of acetabulum (S324), fracture of pubis (S325), fracture of shoulder and arm (S42), fracture of forearm (S52), fracture at wrist and hand level (S62) and fracture of femur (S72).
Pharmacotherapy and duration of treatment
From the Danish Registry of Medicinal Products, we identified commonly used cardiovascular drugs. In this study, we investigated the following classes of cardiovascular drugs (ATC codes in brackets): nitrates (C01DA08, C01DA14), digoxin (C01AA05), thiazide (C03AB01), ACE inhibitors (C09AA01, C09AA02, C09AA03, C09AA04, C09AA05, C09AA10), furosemide (C03CA01), calcium antagonists (C08CA01, C08CA02, C08DA01, C08DB01), β-blockers (C07AA05, C07AB02, C07AB03, C07AB07, C07AG02), statins (C10AA01, C10AA03, C10AA05, C10AA07) and angiotensin receptor antagonists (C09CA01, C09CA03, C09CA04, C09CA06, C09CA07, C09CA08).
Treatment status was determined in a time-dependent manner by prescription claims from the Danish pharmacies, implying that individuals were only considered exposed if covered by claimed prescriptions. To determine treatment length, up to three consecutive prescriptions were considered in a retrospective manner. We created an algorithm for each drug and tablet strength in which minimum, maximum and typical daily dosages of the medication were defined. From patients’ initial prescriptions, the typical daily dosage was assigned, and treatment length was calculated by dividing the amount of first-claimed medications by that daily dosage. For patients who were covered by a previous prescription at the time of claiming a new prescription, the daily dosage was reset and a new daily dosage was calculated as the amount of claimed medications during the previous period divided by time between prescription claims (based on up to 3 previous prescriptions without treatment breaks). If calculated dosages exceeded the predefined highest daily dosages, patients were assigned the maximum osages, and the exceeding tablets were assumed to be stored and consumed during the immediate period following the end of the last prescription.
Furthermore, the date of the first prescription from 1 year prior to inclusion and throughout the study period was identified in order to define time since initiating treatment. Time since initiating treatment was grouped into periods of 0–14, 15–30, 31–90, 91–180 or >180 days. These time periods were chosen in order to discriminate between acute effects possibly due to direct cardiovascular effects, and later effects possibly due to effect on bones or muscles. Persons who were on a specific drug at inclusion were included and placed in the relevant time period according to date of the first prescription.
Comorbidities
We identified comorbidities known to be associated with falls: ischaemic heart disease, stroke, hypertension, heart failure, chronic obstructive pulmonary disease, cancer, diabetes, depression, dementia, osteoporosis, Parkinson's disease and previous fragility fractures.33 We used inhospital diagnoses from the Danish National Patient Registry to identify comorbidities. Some diseases are diagnosed primarily in an outpatient setting and we, therefore, included relevant medications from the Danish Registry of Medicinal Products Statistics to identify these comorbidities. We did this for the following diseases (ATC codes in brackets): depression (N06A), dementia (N06D), diabetes (A10), osteoporosis (M05B) and Parkinson's disease (N04). All comorbidities were identified from 1977 and throughout the observation period. Previous fragility fractures were defined as any fracture 5 years prior to inclusion.
Statistics
We applied time-dependent multivariable Poisson regression models to test the association between the different cardiovascular drugs and fall-related fractures. Prior to analysis, observational time was divided into bands of 1-year intervals and age was updated at the start of each time band. To ensure timely correct categorisation of comorbidities and exposure, all comorbidities were included as time-dependent variables. The importance of time since initiation of the different CVD-drugs was explored by including variables as use versus no use of a specific agent in a specific time window (eg, ‘nitrates 0–14 days’, ‘digoxin 91–180 days’, etc). The Poisson regression model was adjusted for age, gender, calendar year, comorbidities and exposure to the other classes of CVD-drugs. In order to address possible confounding by indication, we performed a subanalysis stratified by heart failure.
All analyses were conducted using SAS, V.9.2 (SAS Institute, Cary, North Carolina, USA), a two-sided p value of <0.05 was considered as statistically significant.
Ethics
No ethics approval is required for retrospective register-based studies in Denmark.
Results
Overall, 1 586 554 individuals were included in the study cohort with a maximum follow-up time of 14 years. The mean follow-up time was 6.7 years, and loss to follow-up due to emigration was 0.3%.
During follow-up, 255 936 individuals (16.1%) experienced a fragility fracture; of these, 90 994 (5.7%) were in treatment with CVD-drugs at the time of the fracture. Numbers ever exposed to the different CVD-drugs are presented in table 1. Individuals treated with CVD-drugs were older, and they generally had more comorbidity compared with the general population. Further population characteristics regarding gender, age and comorbidities in relation to the classes of CVD-drugs are shown in table 1.
Baseline characteristics of the study population
Total exposure time, and numbers of fractures for each group of drugs and for those unexposed are given in table 2. Crude fracture rates were highest among patients treated with loop diuretics, digoxin or thiazides; in the remaining CVD-drugs, the crude fracture rates were similar to the unexposed.
Incidence rates and 95% CIs, observation time, and number of events according to exposure status
Multivariable Poisson regression analysis yielded similar patterns. The association between drug use and fragility fractures was generally strongest in the time interval of 0–14 days after drug initiation. Diuretics were significantly associated with fractures in this initial treatment period: furosemide with incidence rate ratio (IRR) 1.74 (CI 1.61 to 1.89), and thiazides with IRR 1.41 (CI 1.04 to 1.16). Digoxin was significantly associated with falls only in the period between 15 and 30 days after treatment start, and the association was weak (IRR 1.18, CI 1.02 to 1.37), data shown in figures 1⇓–3.

Adjusted incidence rate ratios (IRR), 95% CIs, p value, and number of events for digoxin, furosemide, and thiazides.
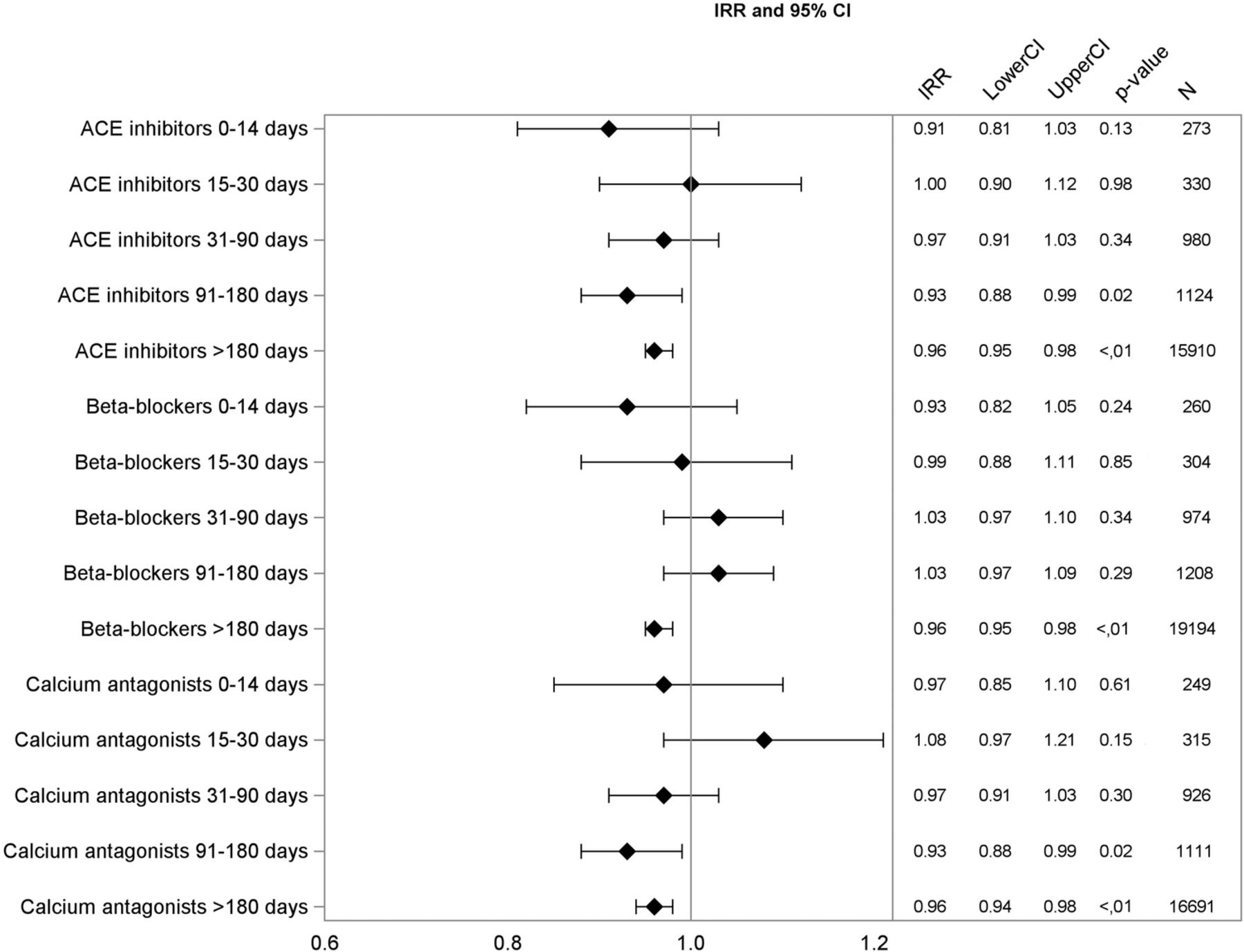
Adjusted incidence rate ratios (IRR), 95% CIs, p value, and number of events for ACE inhibitors, beta-blockers, and calcium antagonists.

{kind=link}
{kind=link}
{kind=link}
Adjusted incidence rate ratios (IRR), 95% CIs, p value, and number of events for angiotensin receptor blockers (ARBs), nitrates, and statins.
Analysis stratified by heart failure showed no significant change in risk estimates for individuals with prior diagnosis of heart failure compared with individuals with no prior diagnosis of heart failure.
Discussion
In this nationwide study including individuals aged ≥65 years, we investigated the association between different cardiovascular drugs and incidence of fragility fractures. We observed that use of loop diuretics and thiazides were significantly associated with fragility fractures, while the remaining antihypertensive drugs, statins and nitrates were not. The fact that the association between drugs and fragility fractures was strongest during the first 2 weeks of treatment and thereafter, gradually declined suggests that the increase in fragility fractures is due to increase in falls rather than changes in bone health. The finding that only diuretics were associated with fragility fractures is new. In a register-based study, we cannot conclude anything on the mechanism of a possible association. However, hyponatremia has been shown to increase the risk of fractures independent of osteoporosis, probably due to the cognitive effect and the effect on balance measures of even mild hyponatremia.34 ,35 Diuretic-associated hyponatremia may, therefore, partly explain the association.
Other studies
Other studies have found that long-term thiazide use reduces the risk of fractures possibly due to the calcium-retaining effect in the renal tubules.36 Our study is concerned with the risk of fragility fractures in the initial treatment period and does not contradict this finding.
A meta-analysis including studies performed in the period 1966–1996 found association between falls and use of diuretics, digoxin and type1A antiarrhythmic agents.14 However, the authors explain that the results may be biased due to few people taking each drug class and few people falling, resulting in very wide CIs in the included studies. A recent meta-analysis, an update of the previous one, included another 22 studies published during 1997–2007; this found no significant associations between use of any cardiovascular drug and falls.15 All studies included in the two meta-analyses are observational studies and are heterogeneous concerning study methods, settings, power and fall definition. In a comprehensive systematic review of risk factors for falls, Deandrea et al37 found an OR 1.25 (CI 1.05 to 1.44) for use versus non-use of antihypertensive drugs.
Only few relevant studies have been published after the latest meta-analysis. Butt et al38 ,39 studied the association between use of antihypertensive drugs and the occurrence of falls and hip fractures in an elderly population in Ontario, Canada, using a self-controlled design. Sample size in the fracture study was smaller (1463 cases) than in the falls study (8893 cases), and the association in the falls study was stronger for all drugs. In the falls study, there were significant associations between falls and new use of thiazide diuretics, calcium channel blockers, ACE inhibitors and β-blockers, but not for angiotensin receptor antagonists. Gribbin et al used a self-controlled design and found significant association between use of thiazide diuretics and falls, IRR 2.8 (CI 1.7 to 4.6), but not for β-blockers, calcium channel blockers or ACE inhibitors. The authors mention that results may be diluted by misclassification of exposure periods, and that the falls outcome represents a small subset of self-reported falls.40
Berry et al found a significant association between starting a loop diuretic and incident hip fracture, with OR 1.8 (CI 1.2 to 2.7) for hip fracture during days 1–7 after treatment start. The maximum effect of a thiazide diuretic on the acute risk of hip fracture occurred 8–14 days following drug initiation (OR=2.2, 95% CI 1.2 to 3.9).41 Tinetti et al42 followed 4961 elderly individuals for 3 years and found association between serious falls and moderate intensity use of antihypertensive drugs with OR 1.40 (CI 1.03 to 1.9). In a propensity matched subgroup, the association did not reach significance.
In summary, our results are similar to the findings in the most recent and self-controlled studies. Results from earlier studies included in the two meta-analyses are more diverse.14 ,15
Strengths and limitations
A major strength of this study is the large population, which allowed us to examine the association between fractures and exposure to specific cardiovascular drugs. However, it is an observational study, and we cannot fully exclude the effect of unmeasured confounders. There are several risk factors for falls and fragility fractures that we have not been able to include; however, we have no reason to believe that these risk factors influence the exposure to CVD-drugs. In a Poisson analysis we cannot distinguish between the risk of starting medication and the risk of the disease, which was the reason for the medication. This means that the associations may merely reflect the underlying condition. However, the diversity of results concerning drugs used for the same indications, that is, hypertension and heart failure, indicates that the results are not driven by confounding by indication. We have further minimised the risk of confounding by controlling for comorbidity known to be associated with falls and fractures, including previous fragility fractures.
We have investigated the association with single drugs. Since elderly persons will often use several drugs at the same time, our estimates of association are possibly lower than in real life.
IRRs for all drugs became lower with time. Owing to the observational design, we cannot rule out that this is partly caused by healthy user bias.
Conclusion and clinical implications
Our study supports previous concerns about the risk of falls and fractures associated with antihypertensive treatment in elderly individuals. However, the association between fragility fractures and use of antihypertensive treatment seems only to be true for diuretic treatment.
We suggest that the effect of diuretic treatment in hypertension should be carefully controlled, and use of alternative antihypertensives should be considered in elderly individuals.
The association between digoxin and fragility fractures was so weak that we would not consider this finding as basis of any clinical implication on its own; however, the finding do contribute to recently reported concerns regarding the use of digoxin.43
References
Footnotes
Contributors MT and EH had full access to all of the data in the study and take responsibility for the integrity of the data and the accuracy of the data analysis. MT, CT-P and EH were involved in study concept and design. CT-P and GG were involved in acquisition of data. All authors were involved in analysis and interpretation of data. MT and EH were involved in drafting of the manuscript. All authors were involved in critical revision of the manuscript for important intellectual content. MT was involved in statistical analysis. GG, CT-P and EH were involved in study supervision.
Funding This research was supported by a grant from the public Regional Research Foundation, Region Zealand.
Competing interests All authors have completed the Unified Competing Interest form at http://www.icmje.org/coi_disclosure.pdf (available on request from the corresponding author), and CT-P reports grants and personal fees from Cardiome, grants and personal fees from Merck, grants and personal fees from Sanofi, grants and personal fees from Daiichi, grants from BMS, all outside the submitted work.
Ethics approval This study was approved by the Danish Data Protection Agency (j.nr:2007-58-0015 / local j.nr. GEH-2014-013 I-Suite nr: 02731).
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement No additional data are available.