Article Text

Abstract
Objectives To investigate the heterogeneous transmission patterns of Middle East respiratory syndrome (MERS) in the Republic of Korea, with a particular focus on epidemiological characteristics of superspreaders.
Design Retrospective epidemiological analysis.
Setting Multiple healthcare facilities of secondary and tertiary care centres in an urban setting.
Participants A total of 185 laboratory-confirmed cases with partially known dates of illness onset and most likely sources of infection.
Primary and secondary outcome measures Superspreaders were identified using the transmission tree. The reproduction number, that is, the average number of secondary cases produced by a single primary case, was estimated as a function of time and according to different types of hosts.
Results A total of five superspreaders were identified. The reproduction number throughout the course of the outbreak was estimated at 1.0 due to reconstruction of the transmission tree, while the variance of secondary cases generated by a primary case was 52.1. All of the superspreaders involved in this outbreak appeared to have generated a substantial number of contacts in multiple healthcare facilities (association: p<0.01), generating on average 4.0 (0.0–8.6) and 28.6 (0.0–63.9) secondary cases among patients who visited multiple healthcare facilities and others. The time-dependent reproduction numbers declined substantially below the value of 1 on and after 13 June 2015.
Conclusions Superspreaders who visited multiple facilities drove the epidemic by generating a disproportionate number of secondary cases. Our findings underscore the need to limit the contacts in healthcare settings. Contact tracing efforts could assist early laboratory testing and diagnosis of suspected cases.
- EPIDEMIOLOGY
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Strengths and limitations of this study
An explicit assessment of the transmission dynamics of Middle East respiratory syndrome (MERS) was conducted estimating the time-dependent and type-specific reproduction number.
The analysis rests on the transmission network of MERS.
Common features of superspreaders were explored.
The study was based on analysing secondary data, and the way by which we identified a potential association of superspreader with social or behavioural factors is regarded as being derived from a type of ecological study in causal inference.
Background
An outbreak of the Middle East respiratory syndrome (MERS) caused by MERS-associated coronavirus (MERS-CoV) occurred in the Republic of Korea from May to July, 2015.1 The transmission was amplified in healthcare settings, leading the country to record the second largest number of confirmed MERS cases among nations, following the Kingdom of Saudi Arabia, since 2012. The natural history of infection including the incubation period and serial interval have been well characterised in a real time study,2 which has also highlighted the clinical features of infection that are in line with those documented in prior studies of MERS outbreaks in the Middle East countries.3
The basic reproduction number, R0, defined as the average number of secondary cases produced by a typical primary case during its entire period of infectiousness in a fully susceptible population, has been estimated to be below the epidemic threshold at 1.0 for MERS, indicating the lack of potential to trigger a large-scale epidemic in the community.4–8 Such a notion is also supported by the fact that past and ongoing outbreaks have been confined to healthcare settings,6 but the confinement to healthcare facilities has also made it difficult to assess the communitywide risk of MERS.9 The number of secondary transmissions produced by a single primary case has been shown to be highly variable,10 ,11 and, in fact, based on contact tracing efforts, several superspreaders during the Korean outbreak have been linked to multiple secondary cases that comprise large nosocomial clusters.2
Although the end of the outbreak has been declared by the South Korean government,12 ,13 it is crucial to gain a detailed understanding of the time-dependent transmission dynamics including the effectiveness of interventions. Moreover, whereas superspreading events have been documented for outbreaks of MERS and other emerging diseases,4 ,14 it is essential to identify the factors and mechanisms behind superspreading events in order to guide countermeasures in anticipation of potential future outbreaks. For instance, in addition to close contacts within households and healthcare facilities (that are, in the present study, defined as ‘social’ or ‘behavioural’ factors that characterise the elevated risk of secondary transmissions), certain aerosol producing procedures, for example, nebuliser treatments, emergency intubations and a ventilation system, as well as delayed diagnosis, have been identified as major factors giving rise to superspreading events of severe acute respiratory syndrome (SARS).15–17 Such factors during medical treatment should be defined as ‘procedural’ or ‘mechanical’ factors that have the potential to generate superspreading events. Other than social/behavioural and procedural/mechanical, it is possible that ‘biological’ or ‘intrinsic’ factors such as specific immune reactions that allow the virus to be viable for longer periods of time or increased viral load among certain infected individuals, could play a role in generating superspreaders. While superspreaders may not easily be fully classified in one of abovementioned categories, it is vital to identify common features of those producing secondary cases. The present study aims to analyse the time-dependent and host type-specific characteristics of MERS-CoV transmission in the Republic of Korea, using epidemic modelling, thereby epidemiologically exploring mechanisms of heterogeneous transmission.
Methods
Epidemiological data
The present study used published data sets of laboratory-confirmed MERS cases in the Republic of Korea, in 2015.2 ,12 ,18 ,19 The confirmatory diagnosis was performed by reverse transcription PCR. Publicly available case information includes age, gender, date of illness onset, date of laboratory confirmation, date of hospitalisation, and the most likely source of infection that shapes the transmission network (ie, linking who acquired infection from whom), including superspreading events.2 The latest date on which the data were compiled was 31 August 2015, with a total of 185 confirmed cases (excluding one case diagnosed in China). Whenever the date of illness onset was missing, we substituted it by the date of laboratory confirmation.20 ,21 However, this substitution has limited impact because the great majority of suspected cases in Korea have been closely monitored so that, since the index case was identified, suspected cases developing symptoms have been rapidly tested for MERS-CoV.
Reconstruction of transmission network
The transmission network has linked the majority of cases to their most likely sources of infection, but an analysis that rests solely on the observed network (or the network that may be regarded as ‘originally reconstructed’) could underestimate the transmissibility of MERS-CoV infection (eg, if the analysis rests on counting existing edges only). Thus, while trusting the observed transmission network, we have also deterministically reconstructed a part of the untraced transmission network using the serial interval, that is, the time from illness onset in a primary case to illness onset in the secondary case who has directly acquired infection from the primary case. An analysis of epidemiological data in South Korea estimated the mean and SD of the serial interval at 12.6 and 2.8 days, respectively.2 Based on the information of shared healthcare facility and using the probability density function of the serial interval, g(s), of length s, which was assumed to follow a gamma distribution, each pair of cases without known link but with known dates of illness onset t1 and t2 (for t1<t2), was deterministically connected identifying the pair that yields the highest probability of connection given by g(t2−t1). During the reconstruction, the observed network was trusted and dealt with as the subset of reconstructed network, and the most likely source of infection among secondary cases without incoming link but with known date of illness onset t2 was explored. There were no multiple pairs of cases that yielded an identically highest probability, and, thus, the abovementioned rule of deterministic reconstruction was not violated. Due to the reconstruction, two offspring distributions, namely, the distribution of secondary cases per single primary case, were obtained, for the observed network only and for a partially reconstructed (‘modelled’) network.
Type-specific modelling
As the first analytical inspection, we explored the host specificity of secondary transmission, aiming to identify characteristic factors of secondary transmission and superspreaders. Based on the percentile (eg, 95 centile) and visual inspection of the offspring distribution, superspreaders in the present study were defined as those causing eight or more secondary cases. Specifically, the type-specific transmission dynamics were examined, classifying diagnosed cases into two or more types according to their occupation (healthcare workers vs others), hospital admission status (inpatients or outpatients vs others) and contact behaviour (visiting multiple healthcare facilities vs others), so that specific characteristics of primary cases who frequently produced secondary cases could be identified. Patients who visited multiple healthcare facilities were defined as confirmed cases who experienced exposures at two or more facilities shortly before and after the date of illness onset. In addition, any statistical association was explored between superspreader and time delays, from illness onset to diagnosis and from illness onset to hospital admission. Presence of secondary transmission and being a superspreader was dichotomised, so that the association of these two features with dichotomous types of cases (eg, visiting multiple healthcare facilities) was examined using χ2 test. The association between secondary transmission/superspreader and time delays was examined using t tests.
Subsequently, a multitype branching process model was employed, assuming that the transmission from one type of host to the other type follows a Poisson distribution (because using the multitype model, it is ideal to assume that the heterogeneity was well captured). Let λi,j represent the average number of secondary transmissions in subgroup i generated by a single primary case in subgroup j. Since the contact tracing practice has enabled us to track the number of secondary cases for each primary case x, the likelihood function to estimate λ, and, thus, the so-called next generation matrix is 1where mix is the observed number of secondary cases in subgroup i generated by an individual x. λi,j(x) represents the parameter that governs the average number of secondary transmissions in subgroup i generated by single primary case j(x), where j(x) represents the host type j to which the individual x belongs, and N represents the total number of participants (N=185). This analysis discarded the time-dependence in the transmission dynamics. Thus, the reproduction number estimates derived from equation (1) would be underestimated to be perceived as similar to the so-called ‘next generation matrix’, but the estimation of the heterogeneous transmission matrix was aimed to identify individuals who have produced a substantial number of secondary cases rather than attempting to provide precise estimates of the reproduction number.
1where mix is the observed number of secondary cases in subgroup i generated by an individual x. λi,j(x) represents the parameter that governs the average number of secondary transmissions in subgroup i generated by single primary case j(x), where j(x) represents the host type j to which the individual x belongs, and N represents the total number of participants (N=185). This analysis discarded the time-dependence in the transmission dynamics. Thus, the reproduction number estimates derived from equation (1) would be underestimated to be perceived as similar to the so-called ‘next generation matrix’, but the estimation of the heterogeneous transmission matrix was aimed to identify individuals who have produced a substantial number of secondary cases rather than attempting to provide precise estimates of the reproduction number.
Time-dependent and type-specific model
We devised a time-dependent multitype transmission model to explore the temporal dynamics of the outbreak. We estimated two different effective reproduction numbers, that is, the period and cohort reproduction numbers.22 ,23 Let ci(t) be the expected number of new MERS cases of type i at calendar time t. The multivariate renewal equation model is written as 2where Aij(t,s) describes the rate of secondary transmissions in type i caused by a single infected individual of type j at calendar time t and time since infection s. The period reproduction number is given by
2where Aij(t,s) describes the rate of secondary transmissions in type i caused by a single infected individual of type j at calendar time t and time since infection s. The period reproduction number is given by 3yielding the average number of secondary cases that occurs exactly at calendar time t. The cohort reproduction number is given by
3yielding the average number of secondary cases that occurs exactly at calendar time t. The cohort reproduction number is given by 4which gives the average number of secondary cases caused by a primary case who was ‘born’ at calendar time t. Both quantities were estimated in the present study. Rc,ij(t) gives the generation-based arguments and facilitates an analysis of the contribution of superspreaders to secondary transmissions, and the contribution of other cases. Rij(t) is useful, as it detects any abrupt decline in the secondary transmission associated with extrinsic factors, most notably public health interventions.
4which gives the average number of secondary cases caused by a primary case who was ‘born’ at calendar time t. Both quantities were estimated in the present study. Rc,ij(t) gives the generation-based arguments and facilitates an analysis of the contribution of superspreaders to secondary transmissions, and the contribution of other cases. Rij(t) is useful, as it detects any abrupt decline in the secondary transmission associated with extrinsic factors, most notably public health interventions.
As for Rc,ij(t), this quantity is directly estimated from the number of observed edges of the transmission tree as a function of the date of illness onset. Subsequently, assuming that Aij(t,s) is decomposable to Rij(t)g(s),19 ,20 Rij(t) was computed using the following relationship, 5
5
To roughly assess the temporal dynamics of the outbreak, especially the impact of public awareness about the outbreak and the implementation of extensive contact tracing, we employed a step-function model for Rij(t), 6where t0 and t1 denote the dates on which the time-dependent dynamics dramatically changed, namely 25 May and 13 June 2015, respectively. The former corresponds to the recognition of multiple clusters within Korea, which led to a dramatic increase in contact tracing efforts while the latter corresponds to the date on which the World Health Organization (WHO) and the Republic of Korea jointly announced the outbreak situation, significantly increasing the awareness about the outbreak among the general public. Piecewise constants are denoted as k1, k2 and k3. These parameters were estimated by numerically solving the equation (5). The uncertainty of Rij(t) (ie, 95% CI) was computed using the bootstrap method. The statistical package R V.3.1.3 was used for all analysis (http://cran.r-project.org).
6where t0 and t1 denote the dates on which the time-dependent dynamics dramatically changed, namely 25 May and 13 June 2015, respectively. The former corresponds to the recognition of multiple clusters within Korea, which led to a dramatic increase in contact tracing efforts while the latter corresponds to the date on which the World Health Organization (WHO) and the Republic of Korea jointly announced the outbreak situation, significantly increasing the awareness about the outbreak among the general public. Piecewise constants are denoted as k1, k2 and k3. These parameters were estimated by numerically solving the equation (5). The uncertainty of Rij(t) (ie, 95% CI) was computed using the bootstrap method. The statistical package R V.3.1.3 was used for all analysis (http://cran.r-project.org).
Ethical considerations
The present study reanalysed the publicly available secondary data from the Korean Government and the WHO, which collected the notification data with ethical approval and written consent from patients and adhering to the International Health Regulations. The secondary data were de-identified by these organisations in advance of our access. As such, the data sets employed in our study have been deemed exempted of review by the ethics committee review board.
Data sharing policy
The present study fully rests on published data, and essential components of the data consisting of dates of illness onset and death have been downloadable from the WHO website.12 The authors are willing to guide readers wanting access to the publicly available secondary data, on request.
Results
Transmission dynamics
Figure 1A displays the epidemic curve of MERS cases in Korea from 11 May to 2 July 2015. The highest incidence was observed on 1 June 2015, followed by a sharp decline in the number of cases. The date of illness onset was unknown among a total of 11 cases. Of these, three were inpatients and four were outpatients, including those already exhibiting fever on exposure, and, thus, it was not feasible to manually determine the first date of fever caused by MERS-CoV infection.
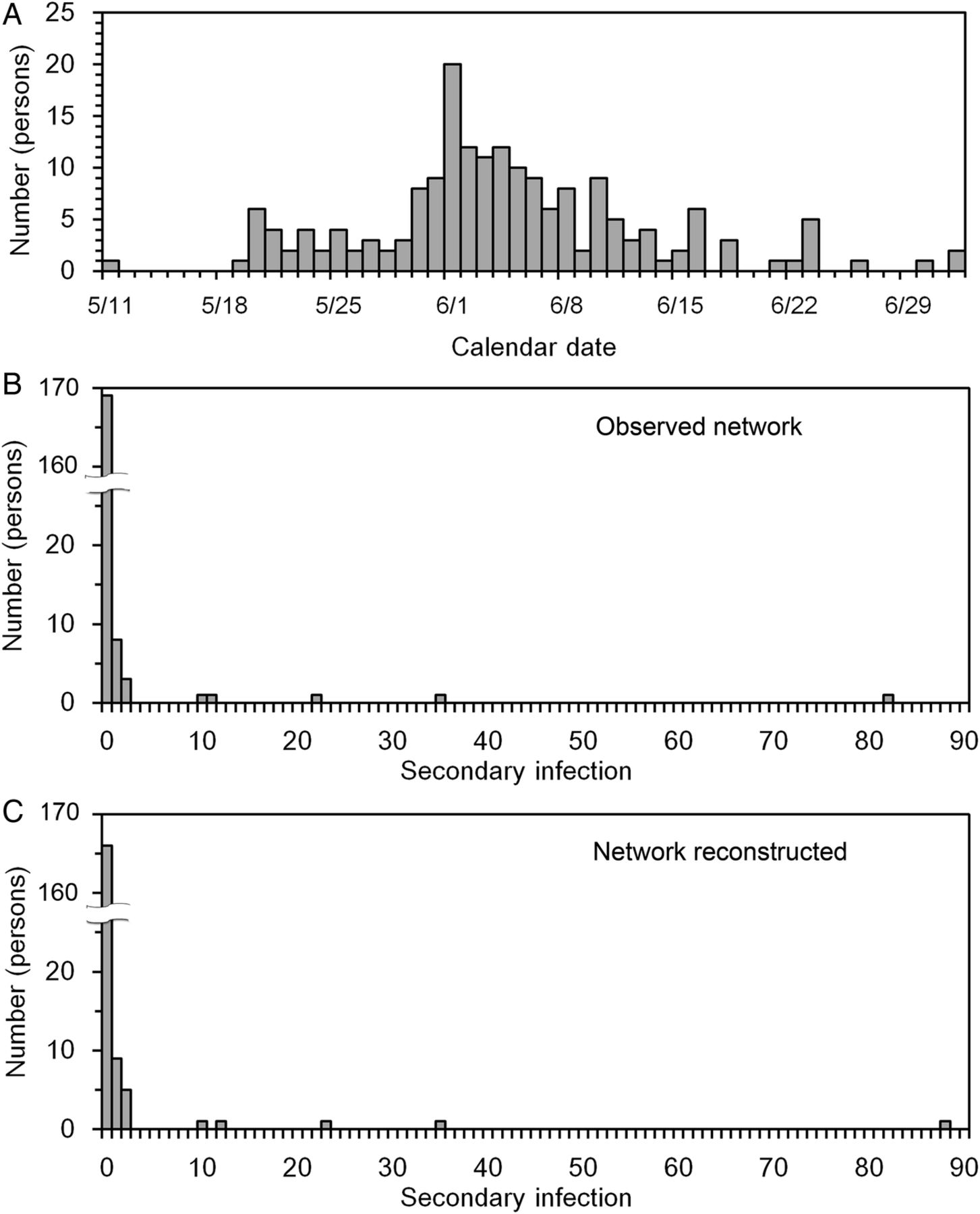
Epidemiological dynamics of the Middle East respiratory syndrome (MERS) in the Republic of Korea. (A) An epidemic curve of MERS in the Republic of Korea. The curve of daily cases is based on the date of illness onset. (B and C) Distributions of the number of secondary cases produced by each primary case. Using the percentile point, superspreaders were defined as cases that produced more than eight secondary cases. B was based on observed network data with 169 known links, while panel C rested on a partially reconstructed network with 182 links.
The offspring distributions are shown in figure 1B, C. There were 16 cases whose source of infection was unidentified. Of these, a total of 13 were linked to a possible primary case through our reconstruction. The observed network connects 169 pairs of cases, while the partially reconstructed network has linked 182 pairs among a total of 185 cases. In the partially reconstructed network, only the index case and two other cases with unknown contact history (ie, who did not indicate any contact history at healthcare facility and yielded only the date of illness onset) were not accompanied by clear incoming links. These distributions are highly skewed. As many as 169 and 166 cases were not linked to any secondary cases in observed and partially reconstructed networks, respectively, and, thus, the majority of cases did not produce any secondary cases. The offspring means were 0.9 and 1.0, while the variance was as large as 44.6 and 52.1 for observed and partially reconstructed networks, respectively.
Figure 2A, B illustrate the transmission tree that describes the pattern of MERS-CoV transmission in Korea. Supporting the abovementioned findings, the tree is composed of several large clusters produced by a total of five superspreaders. Five large clusters at hospital settings are grouped together in figure 2. Partial reconstruction of the transmission network helped to link cases who mainly developed illness at the latter half of the outbreak, helping us to avoid underestimation of the reproduction number during the corresponding stage of the outbreak. Five identical superspreaders were detected using both, observed and reconstructed networks, and slightly varying cut-off values of the number of secondary cases in the corresponding offspring distributions (figures 1B, C) did not alter our findings on the identification of superspreaders. One among five superspreaders resulted in fatal outcome, while 35 non-superspreaders (among 180) died (p=1.00; OR=1.04 (95% CI 0.15 to 7.20)).

Transmission trees of the Middle East respiratory syndrome (MERS) in the Republic of Korea. The transmission trees describing who acquired infection from whom. Tree A was based on observed network data with 169 known links, while tree B rested on a partially reconstructed network with 182 links. Squares represent individual MERS cases, plotted according to their date of illness onset. Grey squares denote the superspreaders and the dotted squares are secondary cases caused by non-superspreaders. Each outer square represents the cluster of cases infected by a single super spreader at a particular healthcare facility. Cases without a known pathway of infection were grouped in the bottom within the dotted square. One unlinked case is known to have been infected by one of 13 cases in a single cluster in a hospital,2 but the corresponding case remains unlinked in this figure as it was not linked to any specific individual.
Type-specificity
Table 1 shows the demographic characteristics of superspreaders and list of healthcare facilities that each superspreader visited during the course of the outbreak. It was common for a superspreader to visit at least two different facilities three or more times. Among a total of 22 cases who visited multiple healthcare facilities, 5 (22.7%) acted as superspreaders. There were a total of 163 cases who did not fulfil the criteria to be categorised as visitors to multiple healthcare facilities and all of them were not superspreaders. The association between visits to multiple healthcare facilities and being a superspreader appeared to be significant (p<0.001). Because all superspreaders were categorised as patients visiting multiple healthcare facilities, we compensated by 0.5 to all frequencies of the 2-by-2 table just for the sake of calculation, and the OR of visitors to multiple healthcare facilities to become a superspreader was estimated at 102.8 (95% CI 5.5 to 1937.8). We also found a significant association between those who produced at least one secondary case and behaviour to visit multiple hospitals (p<0.001): in the partially reconstructed network, 12 cases among a total of 19 cases with secondary transmission visited multiple healthcare facilities, while 10 cases among a total of 166 cases without secondary transmission visited the facilities, yielding an OR of 26.7 (95% CI 8.6 to 82.8). On average, superspreaders generated 4.0 (95% CI 0.0 to 8.6) and 28.6 (95% CI 0.0 to 63.9) secondary cases among patients who visited multiple healthcare facilities and others.
Healthcare facilities that each superspreader of Middle East respiratory syndrome (MERS) has visited in the Republic of Korea, 2015
In the partially reconstructed network, the time from illness onset to diagnosis was not significantly different between those with and without secondary transmission (mean 5.8 vs 5.1 days, p=0.42). Nor was a difference observed between superspreaders and others (mean 7.6 vs 5.1 days, p=0.20). Similarly, there was no significant difference in the time delay from illness onset to hospitalisation between those with/without secondary transmission (p=0.59) and superspreaders/others (p=0.29). These findings were consistent with those obtained from the observed network.
Table 2 shows the estimates of each element of the 2-by-2 next generation matrix. If we divide the population into patients who visited multiple healthcare facilities and others, it appears that, on average, 6.9 (95% CI 0.0 to 14.5) secondary cases in the others category were caused by each single primary case who visited multiple facilities. The secondary cases among the others category caused by a primary case in the same subgroup was as small as 0.1 (95% CI 0.0 to 0.1). The reproduction number originating from patients who visited multiple facilities dominates the transmission dynamics. No clear patterns of transmission were found when we divided the population into healthcare workers versus others as well as hospital patients versus others (Results not shown).
Type-specific reproduction numbers for the transmission of Middle East respiratory syndrome (MERS) in the Republic of Korea, based on a multi-type branching process
Time-dependent heterogeneous dynamics
Figure 3A–H summarise the cohort reproduction numbers of MERS as a function of the date of illness onset of primary cases, using the partially reconstructed network. No obvious pattern of the emergence of superspreaders was seen as a function of time, although it was certain that the emergence occurred during the early phase of the epidemic (as has been implicated in network study), and it is evident that the emergence abruptly stopped in the midst of the outbreak. Among non-superspreaders, it is extremely rare to observe secondary cases: there were in total seven primary cases generating one secondary case, and four primary cases generating two secondary cases each. Investigating the cohort reproduction number over the course of the outbreak, a clear declining trend was observed. Similar patterns were observed when we distinguished cases by those who visited multiple healthcare facilities and others, supporting our finding that visitor mainly characterised secondary transmission dynamics. Qualitative findings were identical when we used the observed network data (see online supplementary figures 1A–H).
Supplementary figures

Cohort reproduction numbers of the Middle East respiratory syndrome (MERS) in the Republic of Korea, in 2015. Scatterplot of illness onset date and the number of secondary transmissions. The left panels distinguish cases into superspreaders and others, while the right panels show the distribution by visitors to multiple healthcare facilities and others. In each panel, the dashed grey line represents the value of unity below which the corresponding case does not contribute to the growth of the epidemic. A continuous line represents the time-dependent trend line.
Figure 4A–F illustrate the estimated period reproduction numbers using the partially reconstructed network. Rt originating from superspreaders to others was estimated to be 4.4 (95% CI 3.6 to 5.3), 2.2 (95% CI 1.4 to 3.0) and 0.2 (95% CI 0.0 to 0.9), respectively, for the three abovementioned time periods. Despite a transient increase in secondary transmission from others to others in the second time period, an overall time-dependent declining pattern was seen. Qualitatively, similar patterns were observed when we distinguished cases by those who visited multiple healthcare facilities and others. Again, the analysis of observed network yielded identical findings (see online supplementary figure 2A–F). Varying the time-intervals in equation (6) did not yield qualitatively different patterns. Exclusion of cases without known date of illness onset did not yield qualitatively different findings.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Period reproduction numbers of the Middle East respiratory syndrome (MERS) in the Republic of Korea, in 2015. Estimated period reproduction number (Rt). The left panels distinguish cases into superspreaders and others, while the right panels show the distribution by visitors to multiple healthcare facilities and others. The observation period (from 11 May–29 June) is divided into three periods, and the reproduction number is assumed to be invariant in each period. The 95% CIs are indicated by dotted lines. A grey line shows the value of Rt=1.
Discussion
The present study analysed the heterogeneous transmission dynamics of the MERS outbreak in the Republic of Korea, in 2015, focusing on the epidemiological characteristics of superspreaders. The offspring distribution of the secondary cases per single primary case was highly skewed to the right, enabling us to visually identify five superspreaders. When analysing type-specific patterns of transmission, having visited multiple healthcare facilities was a common feature of the superspreaders and those causing secondary transmission during the outbreak. Through our analysis based on the multitype branching process model, it was shown that superspreaders who visited multiple facilities drove the epidemic by generating a disproportionate number of secondary cases. Examining the time-dependent dynamics, it was shown that the majority of secondary transmissions were caused by the superspreaders, and the maximum likelihood estimate of the reproduction number originating from non-superspreaders remained below 1. The reproduction numbers declined as a function of time, and were substantially below the value of 1 on and after 13 June 2015. Whereas the reconstruction of the transmission tree was conducted deterministically, we have obtained qualitatively identical results even after stochastically reconstructing the network (results not shown).
An important finding from this study is that patient's behaviour to have visited multiple healthcare facilities with an increased number of infectious contacts was significantly associated with the presence of superspreaders. Of course, our analysis does not exclude procedural/mechanical (eg, the use of nebulisers and poor ventilation) and biological/intrinsic factors (eg, increased viral shedding), and, in fact, there has been a suspicion that a part of superspreading events in Korea was facilitated by limited ventilation,24 our time-dependent and type-specific analyses were consistent with the presence of extraordinary large number of contacts caused by specific patients who visited multiple healthcare facilities. The time delays from illness onset to diagnosis or hospitalisation did not appear to be a significant predictor of secondary transmission. Our finding echoes published evidence documented during the SARS outbreak from 2002 to 2003,16 ,17 supporting the design of countermeasures that target unnecessary prolonged contacts caused by patients with non-specific symptoms including fever and respiratory symptoms. Emergency departments in the presence of such patients should institute specific infection control protocols (eg, the outpatient clinic may direct any suspected patients to limit contacts) and triage patients appropriately in order to minimise unnecessary contacts between infectious individuals and other patients, visitors and healthcare workers in the facility.
An extensive contact tracing effort by Korean authorities has been carried out since late May 2015, facilitating early diagnosis, a control effort that was directly reflected in the time-dependent dynamics derived from our analyses. Such intervention precluded the generation of superspreaders and the reproduction number declined over time. Although not specifically implemented to target superspreaders, the corresponding countermeasures put in place by the government of the Republic of Korea should be commended for its direct effectiveness in quickly stemming the outbreak. The implementation of extensive contact tracing in order to rapidly diagnose suspected cases and isolate infectious individuals to break the chain of infections has proven to be an effective non-pharmaceutical tool to mitigate MERS outbreaks, as it was for SARS back in 2003.25–27
Several limitations must be discussed. First, our study was based on analysing secondary data, and the way by which we identified the cause of the superspreader as social or behavioural is regarded as a type of ecological study in causal inference. That is, our finding is likely vulnerable to confounding, and, indeed, other explanations (eg, biological factors including the use of a nebuliser and importance of each comorbidity, and clinical course in characterising secondary transmission) cannot be ruled out. In fact, while it is well known that the offspring distribution is overdispersed,10 ,11 biological mechanisms behind both social/behavioural and biological/intrinsic factors, for example, increased virus replications, high frequency/dose of pathogen shedding, or some other unknown host-pathogen relationship, which may be completely different in superspreaders than in all others, have yet to be identified. It is worth noting that a recent study isolated MERS-CoV from a variety of environmental samples within two hospitals.28 Second, the number of cases was limited, and, thus, we employed a piecewise constant model for estimating the time-dependent reproduction numbers, while the determination of time intervals might not have been fully objective. Third, we had to deal with missing information that we substituted or discarded. As noted in the Methods section, the illness onset date was not fully available. Fourth, our reconstruction of the transmission tree has yet to be validated. Evolutionary genomic data can shed light on this validation task. For instance, strain-specific variations in spike glycoprotein genes of MERS-CoV during the outbreak have been detected.29
Despite these limitations, we believe that the present study successfully characterised the heterogeneous transmission of MERS-CoV in the Republic of Korea, through epidemiological analysis that included model-based inferences. Overall, our findings highlight the importance of setting up systems that support infection control measures via triage and care of suspected cases in order to limit unnecessary contacts caused by patients with non-specific respiratory symptoms.30 ,31 Contact tracing that leads to early laboratory testing and diagnosis would be the core component of countermeasures against MERS in order to minimise unnecessary contacts that could turn into superspreading events.32–34 Considering the recent increase in human-to-human transmission events of MERS-CoV, it is vital to build up and intensify coordinated research on MERS-CoV, so that social and biological mechanisms that generate superspreaders and superspreading events can be fully characterised.
References
Footnotes
Contributors HN conceived the transmission dynamics study, proposing and directing each component of analysis, and drafted the early version of the manuscript. AE, KM, RK, RU and SN assessed the temporal dynamics, analysing the data, and drafting the corresponding text and figures in advance of HN. AE, MS, YM and YD developed and quantified the multitype branching process model, updating the data in real time, and drafting the corresponding text and figures in advance of HN. All the authors discussed and critically assessed the early draft of the manuscript. GC gave comments on the early version of the manuscript. All the authors have read and approved the final version of the manuscript.
Funding HN received funding support from the JSPS KAKENHI Grant, numbers 26670308 and 26700028, Japan Agency for Medical Research and Development, the Japan Science and Technology Agency (JST) CREST programme and RISTEX programme for Science, of the Science, Technology and Innovation Policy. GC acknowledges financial support from the Division of International Epidemiology and Population Studies, The Fogarty International Center, US National Institutes of Health, funded in part by the Office of Pandemics and Emerging Threats at the US Department of Health and Human Services, as well as support from NSF Grant number 1414374, as part of the joint NSF-NIH-USDA Ecology and Evolution of Infectious Diseases programme, UK Biotechnology and Biological Sciences Research Council Grant number BB/M008894/1 and NSF-IIS Grant number 1518939. The funders had no role in study design, data collection and analysis, decision to publish, nor in preparation of the manuscript.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement No additional data are available.