Article Text

Abstract
Background and aims High birth weight (HBW) increases the risk of maternal and fetal morbidity and mortality. Its prevalence and adverse outcomes may be reduced if risk factors are identified and managed during pregnancy. The cut-off value for HBW remains debatable. The objectives of this study were to identify the optimal cut-off value and determine the prevalence, predictors and adverse outcomes of HBW in a suburban area of Cameroon.
Design A 6-year retrospective register analysis and a 3-month prospective phase.
Setting A secondary care level (regional) hospital in the city of Buea (southwest region of Cameroon).
Participants Women who delivered in this hospital over a 6-year period (retrospective phase) and consenting pregnant mothers and their infants (singletons, born at >28 weeks gestation) (prospective phase).
Outcome measures 90th centile of birth weights; prevalence of HBW defined as birth weight above the 90th centile; sociodemographic, maternal and obstetrical factors associated with HBW; maternal and neonatal adverse outcomes of HBW.
Results Of the 4941 newborns reviewed in registers, the 90th centile of birth weights was 3850 g. Using this new cut-off, we obtained a prevalence of 14.0% for HBW in the 200 newborns included in the prospective phase. This was significantly higher than the prevalence (9.5%) yielded when the traditional cut-off of 4000 g was used (p=0.003). None of the factors assessed was independently associated with HBW. Newborns with HBW were more likely to have shoulder dystocia (p<0.01), and their mothers more likely to suffer from prolonged labour (p=0.01) and postpartum haemorrhage (p<0.01).
Conclusions The results of this study suggest that the cut-off for HBW in this population should be 3850 g. Thus, 3 of every 10 babies born with HBW in this hospital are likely not receiving optimal postnatal care because 4000 g is currently used to qualify for additional support.
- NEONATOLOGY
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Strengths and limitations of this study
The study uses nearly 5000 newborns to provide a statistically accurate cut-off value for high birth weight (HBW) that may be useful in clinical practice.
The study showed the extent to which using the traditional ‘developed-world’ cut-off value for HBW may underestimate the prevalence of HBW in developing countries.
The study had a retrospective component, which was subject to a potential risk of incorrectly completed records.
As a hospital-based study, neonates born at home could not be included.
Introduction
High birth weight (HBW) is defined as any birth weight found above the 90th centile of weight for that gestation.1 The prevalence and trend of HBW vary across countries. Studies have shown an apparent decreasing trend in the prevalence of HBW from 10.2% in 1996 to 9.2% in 2002, in the USA,2 whereas in Denmark, the prevalence is reported to have increased from 16.7% in 1990 to 20.0%, in 1999.3 It is generally accepted that HBW occurs in about 3–15% of all pregnancies;4 recent studies in sub-Saharan Africa (SSA) have reported a prevalence of 14.7%.5
HBW is an emerging problem in developing countries. This is due to the growing burden of obesity and diabetes in these societies, attributed to urbanisation and changes in lifestyle patterns.5 ,6 Despite the fact that such factors increase the risk of having babies with HBW, there are few reports on the topic in SSA. HBW is associated with perinatal morbidity and mortality. Studies have shown a significant association between HBW and traumatic births, perineal tears, prolonged labour, postpartum haemorrhage, increased rates of operative deliveries, neonatal hypoglycaemia, shoulder dystocia, birth asphyxia and death.7–9
Furthermore, whether the traditional cut-off value of 4000 g is suitable for clinical use everywhere remains unanswered. The WHO recommends that such cut-off values be used only for epidemiological purposes, and that each population should identify its specific cut-off for clinical use.10 In this study, we sought to establish a cut-off value for HBW in a suburban hospital, using the definition of HBW as all weights that fall above the 90th centile for the local newborn population. We also prospectively assessed the prevalence, predictors and adverse outcomes of HBW, using the new cut-off.
Methods
Study design and setting
We carried out a two-phase descriptive study at the Buea Regional Hospital (BRH): a retrospective register audit to identify the cut-off value for HBW, followed by a prospective study to determine the prevalence, predictors and adverse outcomes of HBW.
The BRH is situated in the Buea Health District (BHD) in the Fako Division. The BRH is the referral hospital in the health district and it performs more deliveries than all the other health facilities in the district combined. The hospital uses all standard units of general medicine. An obstetrician and a paediatrician run the maternity and paediatric units, respectively, but there is no neonatal intensive care unit.
Participants and sampling
The recruitment of participants was described in a previous study by the same authors.11 For the retrospective phase, the records of all pregnant women who gave birth from January 2007 to December 2012 (6 years) were reviewed, and data of mother–infant pairs were included if they fulfilled the inclusion criteria. Information was said to be complete if it contained maternal age, marital status, gestational age, type of delivery, birth weight, newborn gender and Apgar score at the first minute.
For the prospective phase, the target study population included all pregnant mother–infant pairs who gave birth at the BRH from 2 January to 23 March 2013 (3 months); we excluded women who delivered at a gestational age below 28 weeks, those who had a multiple pregnancy and those who did not consent to take part in the study.
Data collection, variables and measurements
In the retrospective phase, we collected sociodemographic and clinical data from registers that had been filled in by the obstetrician, midwives and nurses who worked in the maternity unit.
In the prospective phase, pregnant women who were about to give birth were monitored making sure that they were provided with standard care, and the following data were extracted from their hospital records and completed by a history taken after delivery:
Sociodemographic characteristics: average income per day and level of education.
Obstetric history (gravid status, previous formula feeding and previous birth weights).
Medical history (personal and family history of diabetes and prepregnancy weight).
We measured participants' weight to the nearest kilogram, using a Camry bathroom scale, and height to the nearest centimetre, using a locally made stadiometer, calibrated to the Butterfly tape. A standard physical examination was performed. Throughout the labour, the fetus was monitored for the presence of acute fetal distress (fetal heart rate <120 bpm or persistently above 160 bpm and/or green meconium-stained amniotic fluid at delivery).
After delivery, the neonates were assessed for viability (breathing, heartbeat, pulsation of the umbilical cord or definite movements of voluntary muscles), and their Apgar scores at the 1st, 5th and 10th minutes were assessed. The presence of birth injuries was evaluated and the baby's weight was measured to the nearest gram, using a Holtex+ digital baby scale. The babies were monitored for the presence of respiratory distress (which was identified by any one of the following: respiratory grunting, nasal flaring, intercostal recessions, subxiphoid recession, thoracoabdominal asynchrony or respiratory rate >60 bpm). Any neonatal death occurring during the period of monitoring was also noted.
Informed consent was then obtained after delivery. The newborns and their mothers were observed until the day of discharge, which could be up to 10 days for complicated deliveries that included caesarean sections or instrumental deliveries.
Data management and statistical analysis
Data were cross-checked for errors and stored securely in a private location; all data were kept confidential. Data were analysed using Epi Info V.3.5.4. Means (SD) were used to summarise continuous variables, and frequencies were used for categorical variables. Frequencies were compared using the Fisher's exact test. The McNemar test was used to assess the prevalence of HBW, comparing the traditional cut-off (4000 g) to that obtained by the newly identified cut-off, so as to account for dependency. Predictors of HBW were determined using bivariate and multiple logistic regression models. The models included all variables with p values≤0.25 in the bivariate analyses.12 For all these analyses, the significance was set at 0.05.
Ethical considerations
The study received administrative clearance from the Regional Delegation of Public Health for the South West region and from the Director of the BRH. Confidentiality was ensured during the whole process. Participants were referred to only by identification numbers, and identifiable information (consent form) was kept separate from the data collection forms; it was only possible to link both through a coding sheet—available solely to the research team.
Results
Demographic and obstetrical characteristics
A total of 4941 newborn records were included in the retrospective phase and 200 pregnant women enrolled during the prospective phase. The mean age of the mothers was 26.4 (5.5) and 26.4 (5.8) years, respectively, for the retrospective and prospective phases of the study. The majority were married, half were unemployed, 99% had received at least a primary level of education and 93.4% of the women reported spending more than US$1 a day (table 1). In regard to obstetrical characteristics in the prospective phase, 34.5% were primigravidae.
Sociodemographic characteristics and obstetric history of mothers
Distribution of birth weight and prevalence of HBW
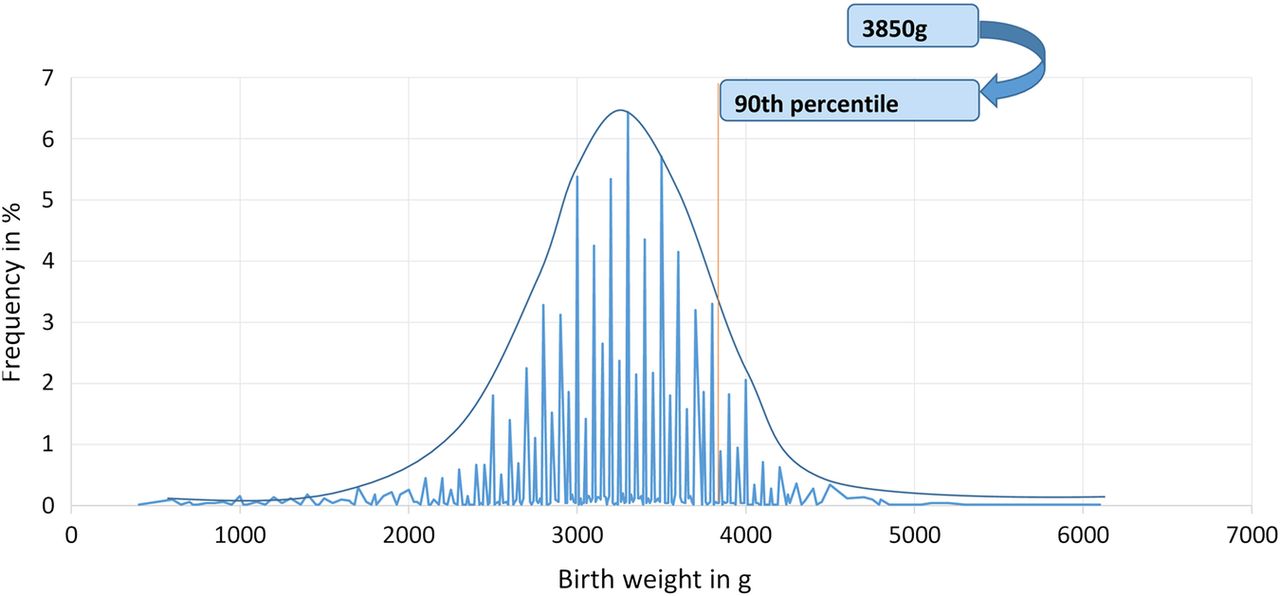
The cut-off to define HBW (90th centile of birth weights) in the 4941 newborns during the retrospective phase was 3850 g (figure 1). Term deliveries accounted for 89.9% of the total deliveries and the 90th centile among this subgroup was also 3850 g. In the prospective study, 28 babies had birth weights ≥3850 g, giving a prevalence of 14.0% (95% CI 9.5% to 19.6%). Using the cut-off of 4000 g, the prevalence was 9.5% (95% CI 5.8% to 14.4%). There was a significant difference in prevalence using the two cut-off levels (p=0.003).
{kind=link}
Distribution of birth weights and cut-off for high birth weight (n=4941). The bell-shaped blue curve shows that the birth weights in the Buea Regional Hospital have a Gaussian distribution. The red line corresponds to the 90th centile of birth weights in our population (3850 g), while the blue lines show the frequencies for the various birth weights.
Predictors of HBW
In the bivariate analysis, spending ≥US$1 a day (p=0.05), a history of a previous HBW pregnancy (p<0.01) and maternal prepregnancy body mass index (BMI) ≥25 kg/m2 (p=0.03) were significantly associated with HBW (table 2).
Bivariate analysis of potential associations with HBW (>3850 g) deliveries
In multivariate analysis, none of the variables tested were independently associated with HBW (table 3).
Multivariate analysis of potential predictors of high birth weight (HBW; >3850 g) deliveries
Adverse outcomes of HBW
Compared with mothers of babies with normal or low birth weight, mothers of neonates with HBW were about twice as likely to have prolonged labour (p=0.01) and five-fold more likely to have postpartum haemorrhage (p<0.01). Furthermore, HBW neonates were 15-fold more likely to have shoulder dystocia during delivery (p<0.01) (table 4).
Neonatal and maternal complications of HBW (>3850 g) deliveries
When comparing the neonates who fell within the birth weight category of 3850–4000 g to those in the category <3850 g, the only excess complication found was in maternal postpartum haemorrhage (2/9 vs 5/172; p=0.04).
Discussion
In this study, we found that the 90th centile of birth weights that defines HBW in babies born in the BRH was 3850 g. Using this as the cut-off value for HBW yielded a prevalence of 14.0%, which was significantly higher than the prevalence obtained when using the traditional cut-off value of 4000 g (9.5%). Newborns with HBW (≥3850 g) were more likely to suffer from shoulder dystocia, while their mothers were more likely to have prolonged labour and postpartum haemorrhage.
Few studies have attempted to generate locality-specific cut-off values for the definition of HBW. Most studies either established several values for large for gestational age, for specific gestational ages,13–15 or used the arbitrary cut-off values of 4000 or 4500 g.8 ,16 Developed countries across Europe, and the USA and Australia, with high mean birth weights ranging from 3400 to 3600 g,16–18 usually adopt the higher arbitrary cut-off value of 4500 g. Meanwhile, less-developed countries such as Nigeria, Cameroon and Tanzania, with lower mean birth weights, ranging from 3000 to 3100 g,19–21 adopt the lower arbitrary value of 4000 g for HBW.22 However, such disparities in trends for birth weight emphasise the need for locality-specific cut-off values for HBW. Our study, therefore, provides a statistically valid cut-off value for HBW for suburban use in Cameroon. This is in compliance with recent WHO recommendations for the adoption of region-specific cut-off values for birth weight distribution.
In SSA, Lawoyin,23 in Nigeria, used a cut-off value for HBW at 3800 g among term babies, in 1993. Our study has established a value of 3850 g for term babies, which is similar. However, these different cut-off values further suggest disparities in birth weight trends and emphasise the need for country/locality-specific HBW cut-off values for clinical management.
The prevalence of HBW, using the traditional cut-off value in our study (9.5%), was higher than that obtained by Abena Obama et al9 (6.0%) and Tebeu et al24 (4.3%) in 1995 and 2005, respectively, in Cameroon, suggesting that HBW is becoming more prevalent over time.
When 3850 g was used to define HBW, a higher prevalence (14.0%) was obtained. This suggests that about 3 of every 10 newborns with HBW and their mothers may be excluded from receiving appropriate care while in hospital. The prevalence of HBW is underestimated using the traditional cut-off. These findings need confirming in further studies.
Although overweight or obesity before pregnancy, previous HBW and spending ≥US$1 a day were associated with HBW in bivariate analysis, none of these were independent predictors of HBW in multivariate analysis. This may be due to the small number of HBW babies, which potentially decreased the power of multivariate analysis.
Several reports have stressed the phenomenon of repeat outcomes from one pregnancy to the next.25 In our study, pregnant women with a previous HBW newborn were more likely to have another in the current pregnancy. However, a previous study carried out by Defo and Partin26 showed that previous birth weight had a significant effect on later birth weight in the USA but not in Cameroon.
Women in our study who were overweight or obese before pregnancy were more likely to have a HBW neonate. Lawoyin,23 in Nigeria, showed that maternal BMI was positively associated with the delivery of large babies. Few studies have tried to assess the impact of maternal income level on birth weight. Women who regularly spent more money were more likely to have a HBW neonate. This could be because these women were more overweight or obese, or had access, more than others, to protein and calorie-rich diets adding to the growth of their fetuses.
Neonates with HBW were more likely to suffer from shoulder dystocia during delivery. Abena Obama et al,9 in Cameroon, also found that shoulder dystocia was a leading complication of macrosomia, and Anya and Anya7 found the same. Additionally, in our study, mothers who had HBW neonates were more likely to have prolonged labour and postpartum haemorrhage. Mocanu et al8 pointed out in their study that women who had macrosomic babies were more likely to have prolonged labour especially if they were primiparae. Anya and Anya7 also indicated that postpartum haemorrhage was a common complication among women who had HBW infants.
Mothers of neonates who fell within the birth weight category of 3850–4000 g in our study were more likely to have complications (postpartum haemorrhage) than those in the category of <3850 g. It might therefore be prudent for clinicians to be more watchful when dealing with birth weights >3850 g.
Our study had the following potential limitations: it was carried out in a single health facility, therefore a substantial number of babies born at home were not included. Thus, the results may not reflect the situation in the whole district. Also, the retrospective phase is subject to a potential risk of inaccurate data recording. Some risk factors (mother's income and history of diabetes) were subjective, since they were based on mother's recall. Some relevant neonatal complications, such as hypoglycaemia, were not assessed because we were not granted ethical approval for testing. The relatively small sample size of the prospective phase may not be sufficient for multivariate analysis to identify the independent predictors of HBW. However, to the best of our knowledge, this is the first study to have generated a statistical and clinically relevant cut-off value for HBW for local application, using a sample of almost 5000 babies.
Conclusions
On the basis of suggested new cut-off value, one of every seven babies born in the hospital has HBW. Mothers of neonates who fall within the newly defined category of HBW (3850–4000 g) are more likely to have complications than those who fall below this cut-off. It is therefore reasonable to suggest that the definition of HBW in suburban areas in Cameroon be lowered to allow all babies ≥3850 g to benefit from appropriate surveillance and care. In addition, because of the well-established association of HBW with diabetes, mothers of these neonates may benefit from diabetes screening after delivery, and should have their neonates tested for hypoglycaemia. We require further studies to confirm these preliminary findings.
Acknowledgments
The authors express their gratitude to the Buea Regional Hospital for allowing them to use the hospital premises, and to the pregnant women who took part in this study.
References
Footnotes
Contributors S-PC, TN, JA and RM contributed to the study concept and design. SPC, TN and JA contributed to the acquisition of data. SPC, TN, JA and JPH-S contributed to data interpretation and analysis. S-PC, TN, JA, JPH-S and RM contributed to manuscript writing and revisions.
Funding The 2HD Research Group is supported by a Cruddas Link Fellowship to S-PC (Tseu Medical Institute, Harris Manchester College, University of Oxford, UK), and receives technical assistance from the NIHR-Bristol Biomedical Research Unit (BRU) in Nutrition, University of Bristol, UK.
Competing interests None declared.
Ethics approval Ethical approval was obtained from the Institutional Review Board of the Faculty of Health Sciences, University of Buea.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement No additional data are available.