Article Text

Abstract
Background Experiences in the first 1000 days of life have a critical influence on child development and health. Health services that provide support for families need evidence about how best to improve their provision.
Methods We systematically reviewed the evidence for interventions in high-income countries to improve child development by enhancing health service contact with parents from the antenatal period to 24 months postpartum. We searched 15 databases and trial registers for studies published in any language between 01 January 1996 and 01 April 2016. We also searched 58 programme or organisation websites and the electronic table of contents of eight journals.
Results Primary outcomes were motor, cognitive and language development, and social-emotional well-being measured to 39 months of age (to allow the interventions time to produce demonstrable effects). Results were reported using narrative synthesis due to the variation in study populations, intervention design and outcome measurement. 22 of the 12 986 studies identified met eligibility criteria. Using Grading of Recommendations Assessment, Development and Evaluation (GRADE) working group criteria, the quality of evidence overall was moderate to low. There was limited evidence for intervention effectiveness: positive effects were seen in 1/6 studies for motor development, 4/11 for language development, 4/8 for cognitive development and 3/19 for social-emotional well-being. However, most studies showing positive effects were at high/unclear risk of bias, within-study effects were inconsistent and negative effects were also seen. Intervention content and intensity varied greatly, but this was not associated with effectiveness.
Conclusions There is insufficient evidence that interventions currently available to enhance health service contacts up to 24 months postpartum are effective for improving child development. There is an urgent need for robust evaluation of existing interventions and to develop and evaluate novel interventions to enhance the offer to all families.
PROSPERO registration number CRD42015015468.
- child development
- social and emotional wellbeing
- universal health services
- early intervention
This is an Open Access article distributed in accordance with the terms of the Creative Commons Attribution (CC BY 4.0) license, which permits others to distribute, remix, adapt and build upon this work, for commercial use, provided the original work is properly cited. See: http://creativecommons.org/licenses/by/4.0/
Statistics from Altmetric.com
Strengths and limitations of this study
To our knowledge, this is the first systematic review of interventions that enhance health services to improve child development outcomes including social and emotional well-being outcomes in the very early years.
We used a broad systematic search of the extensive literature in this field and searched many sources in addition to database searches.
We reviewed a larger number of primary studies than previous reviews of interventions in the early years. Our conclusion is consistent with these reviews.
It was not possible to conduct a meta-analysis due to the variation in the types of interventions and methods used to measure outcomes.
We do not report parental outcomes and cannot comment on whether parents benefited from these enhancements.
Introduction
Experiences in the first 1000 days of life have a crucial influence on child development and health.1 Appropriate early child development (including physical, social and emotional, language and cognitive domains) has consistently been shown to be associated with good health and educational outcomes in childhood and consequent health and employment outcomes in adulthood.2–4 Adopting a life course approach, including early intervention, is essential,5 and investment is therefore needed in effective prenatal and postnatal services to optimise child health, well-being and developmental resilience.6
The content of health services to promote maternal and child health, delivered during pregnancy and the early years through primary care and home visits, varies across countries. A recent review suggested that the best services in Europe are ‘characterized by personalised ongoing support during pregnancy, choice in birth arrangements, postnatal support and advice, and paid parental leave for mothers and fathers’.7 In most high-income settings, early years services also work to a ‘proportionate universalism’ model where care is available to all, irrespective of need, with enhanced support offered to families at high risk of adverse outcomes.1
There is high-quality global evidence to support the effectiveness of many components of early years services including elements of antenatal care and centre-based preschool provision.7 8 Interventions to promote child development by enhancing routine health services in the early years have also been developed. However, most have been targeted at and evaluated with high-risk families or children with an identified condition.9–11 An unacceptably high proportion of children in both high and low-income settings do not achieve expected early learning goals before they start school,12 and it has been argued that targeted approaches alone may not be sufficient.13 Interventions to enhance contacts with all parents in existing services may be more effective in improving child development outcomes for several reasons. First, not all children who need support are identified by a targeted approach.14 Targeting can lead to stigmatisation resulting in poor uptake or adherence.15 Embedding interventions within an existing service, such as health visiting, which provides ongoing and consistent support for parents, may also improve the interaction between health professionals and parents and improve access to care at a crucial time in their child’s development, leading to improvements in child development outcomes.11 A review of interventions in low and middle-income settings noted that there was great diversity in both the scope and focus of research in this area and concluded that parents in such settings ‘need to be supported in providing nurturing care and protection in order for young children to achieve their developmental potential’.16 However, the effectiveness of such interventions to enhance existing multidisciplinary services in high-income settings is not known.
Previous reviews of early interventions in high-income settings fail to provide a full picture of interventions relevant to public health policy and practice because they do not provide a comprehensive examination of child development outcomes in the very early years (ie, the period during which the human brain develops most rapidly17). Neither does the evidence base to date include social and emotional well-being outcomes nor are these consistently defined and articulated. The objective of this systematic review is to fill these gaps, by examining the effect of interventions designed to enhance health service contacts with all parents and children in the very early years (defined as the antenatal period to 24 months postpartum) on child development and social and emotional well-being outcomes. Our research question was developed in partnership with local policy-makers and provides evidence for policy.18
Methods
Protocol and registration
The protocol for this systematic review was registered in the International Prospective Register of Systematic Reviews (PROSPERO CRD42015015468) on 12 January 2015. This review is reported in accordance with Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines.19
Inclusion and exclusion criteria
We included randomised controlled trials (RCT; with individual or cluster randomisation) in any language that were published or unpublished. The interventions of interest were ones delivered within existing multidisciplinary healthcare services that are the cornerstone of early years programmes and are available to all. The interventions may be delivered by a range of staff within these services. We included studies from the 76 countries and territories classified by the World Bank in July 2014 as ‘high-income economies’. Studies published in any language were eligible for inclusion.
To capture the effects of interventions delivered in the very early years, we included programmes that were delivered at any time from the antenatal period to 24 months postpartum. Given that some programmes continue beyond the child’s second birthday, we specified that studies would be included if the mean age of the children at the start of the intervention was less than or equal to 24 months. To allow time for these interventions to produce demonstrable effects, we included studies that examined outcomes to 39 months of age (given that not all studies would manage to assess children on their third birthday exactly).
Studies that selected participants from the general population or included all individuals from a specific neighbourhood (eg, an area-based programme defined on the basis of postcode or zip code, known as ‘geographically targeted’ programmes in this review) were included. Studies were excluded if they selected participants based on individual risk factors (eg, an individually assessed income threshold for participating families or parental illness) or specific clinical subgroups (such as preterm babies or children with specific diagnoses).
Interventions
We included interventions that were provided within the framework of the existing healthcare system. They could be designed to augment routine healthcare provision for all children in different ways, for example, by improving the skills or parental capacity of the parents or the family, improving the interaction between health professionals and parents, improving access to healthcare for the parents or the child or including elements designed to promote a specific area of child development. These included training modules designed to be delivered to parents with the intention of improving child development outcomes or any resources (such as printed materials, films, Apps) that health professionals or their support workers could use in their work with parents. Interventions could be delivered at home, in group-based settings (eg, in general, obstetric or paediatric practice, in hospitals or community settings), through telemedicine or via a combination of different methods.
There is an argument that these different approaches should be separated into different systematic reviews (or indeed separated by outcome). We, like others,10 16 chose to include these in a single review to avoid divisions that were arbitrary from a developmental or service delivery perspective and to avoid multiple overlapping, small and/or empty reviews in a field with limited literature.
Outcomes
The outcomes were motor development (fine and gross), cognitive development, language development (receptive and expressive), social and emotional well-being and global child development. We included studies that used validated tools to measure these outcomes. Where unvalidated tools were used, we considered these to be secondary outcomes. Studies were included if they measured outcomes at any time between 3 months of age and 39 months postpartum (specifically, where the average age of the children at outcome measurement was 39 months or less).
Search strategy
We searched for articles published in any language between 01 January 1996 and 01 April 2016 in the following databases: Cochrane Central Register of Controlled Trials, Medline, Embase, Cumulative Index to Nursing and Allied Health Literature, PsycINFO, Web of Science, Scopus, Applied Social Sciences Index and Abstracts, Literatura Latino Americana em Ciências da Saúde, Sociological Abstracts, Social Services Abstract and OpenGrey; and the following trial registers: ClinicalTrials.gov, UK Clinical Trials Gateway, UK Clinical Trials Gateway and WHO International Clinical Trials Registry Platform. Given our focus on enhancement of existing health services, we restricted to studies published within 20 years of our study inception since health service change has been substantial in the mid to late 20th century. We used a combination of medical subject headings and free text including terms for interventions to enhance health service contacts combined with terms relating to child development outcomes. Terms for the interventions included those that listed the professional delivering the programme (including ‘health visitor’, ‘community nurse’, ‘nurse’, ‘midwife’, ‘general practitioner’, ‘early years educator’, ‘parent educator’) and programme names that were already known to the review team. The Medline search strategy is shown in online supplementary web appendix A. We also searched websites of 58 relevant programmes and organisations and the electronic table of contents (eTOC) of eight key journals for relevant studies published within the last 2 years (see online supplementary web appendix B for a full list). Reference lists of included and key papers were reviewed, and authors contacted for additional data where necessary.
Supplementary file 1
Study selection
All references identified by the searches were downloaded into Endnote and duplicates removed. Titles and abstracts were screened for inclusion independently by two of three reviewers (LH and LJG or SP). Full-text versions were obtained for the papers potentially meeting the inclusion criteria and were screened independently by two of three reviewers (LH and LJG or SP). Disagreements were resolved through discussion and in consultation with others in the review group.
Data abstraction process
A data extraction form designed for the requirements of this review was used, which included details on the characteristics of the included studies, the interventions studied and assessment of risk of bias and Grading of Recommendations, Assessment, Development and Evaluations (GRADE) working group criteria. Multiple publications and reports from the same trial were linked and compared for completeness and contradictions. Data from each paper were extracted independently and in duplicate (completed by LH and LJG or SG or SP or TP).
Analysis
Risk of bias was assessed following Cochrane guidelines.20 Due to variation in (1) the populations studied, (2) the design of the interventions and (3) the wide range of outcome measures used (both in terms of the child development domains and/or the instruments used to assess the outcomes), it was not possible to conduct a meta-analysis and results were reported using narrative synthesis. We specified a priori that we would examine the results stratified by (1) risk of bias, (2) the intensity of the intervention, (3) the age of the child at which the intervention was delivered, (4) whether the programme was available to all or geographically targeted and (5) sociodemographic characteristics of the families in the trial. We selected these variables as we hypothesised that they would help to identify the characteristics of the interventions most likely to be effective (eg, if high-intensity interventions were more effective than low-intensity ones) or the populations in which they were most likely to be effective (eg, if programmes recruiting from defined neighbourhoods were more effective than those made available to all).
An assessment of the intensity of each intervention was conducted independently and in duplicate (completed by LH and LJG or SG or SP or TP) based on seven criteria: (1) total number of visits; (2) total duration of the programme; (3) total number of contact hours; (4) frequency of visits; (5) number of components; (6) whether components were delivered directly to parents and/or children and (7) whether the components were delivered on a one-to-one basis or in a group session. Using these seven characteristics, we categorised the overall intensity for each intervention as ‘low’, ‘moderate’ or ‘high’. Two review authors made this assessment using subjective determination (as used in reference 21) rather than a predefined algorithm or a scoring system to allow for the diversity and complex combinations of components to be reflected in the categorisation. Finally, the quality of the overall evidence for each outcome was assessed using GRADE criteria.22
Public involvement
This work was conducted in collaboration with the Bristol Network for Early Years Health and Well being (www.bonee.org) and a range of stakeholders have been involved in the design and conduct of this initiative. Parents were not involved in the design and conduct of the review, but we are discussing the results and interpretation with parents.
Results
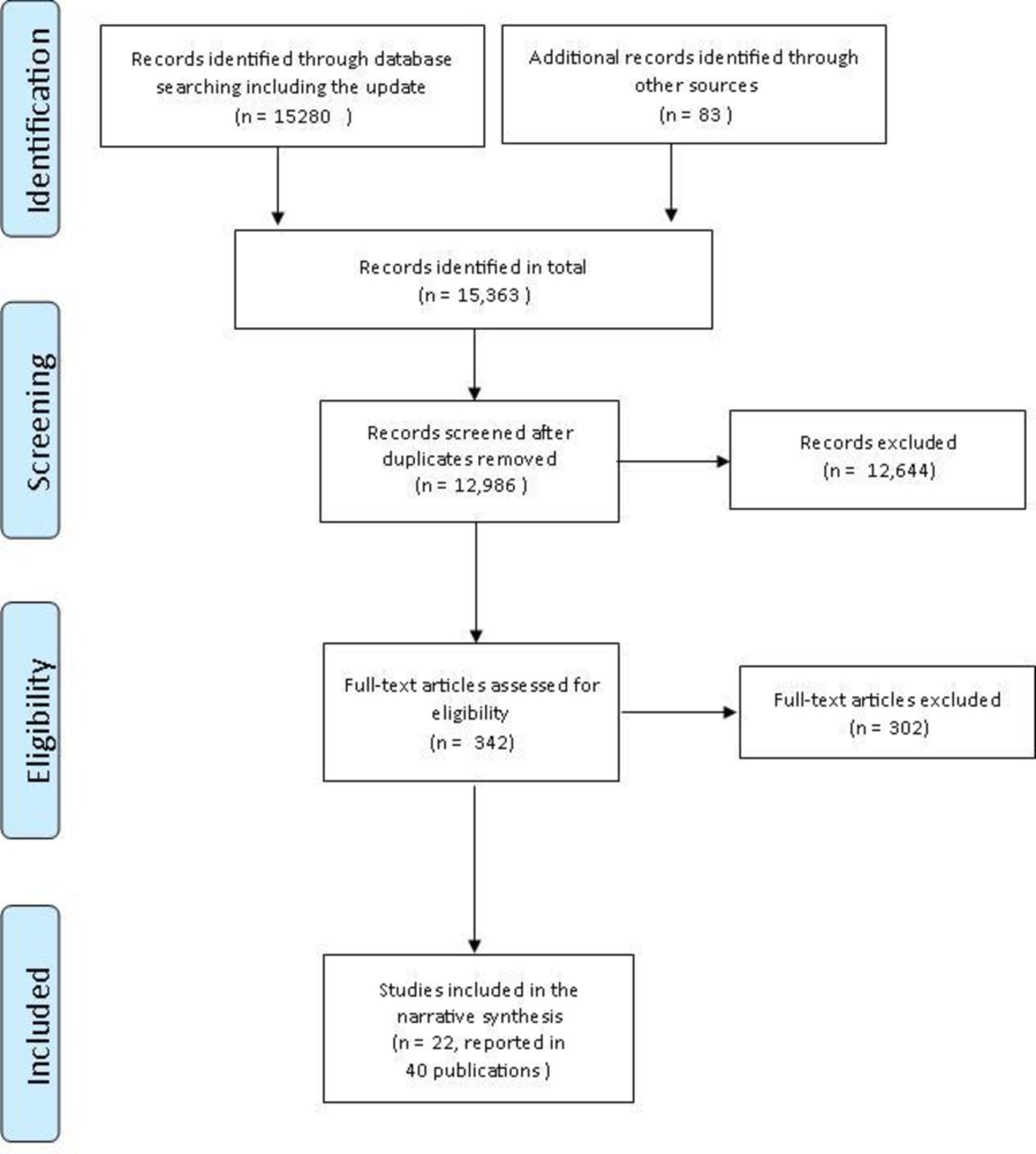
Fifteen thousand two hundred and eighty records were identified in the database searches (figure 1). Searches of relevant programme and organisation websites and eTOC searches yielded 83 additional records. Once all searches were combined and duplicates removed, 12 986 records remained. After title and abstract screening, 12 644 records that were outside the scope of the review were excluded (the vast majority of these because their intervention was targeted at families at high-risk of adverse outcomes or at children with identified conditions). Of the 342 records included in full-text review, there were 22 RCTs that fulfilled our inclusion criteria (reported in 40 publications23–62). We also identified three relevant ongoing trials.63–65 Reasons for exclusion are provided in figure 1.

Preferred Reporting Items for Systematic Reviews and Meta-Analyses flow diagram. Reason for exclusion at full-text screening: ongoing study, n=3; quasiexperimental (control group but no randomisation), n=10; pre–post test comparison only, n=5; not a primary study (reviews, editorials, programme descriptions), n=67; not conducted in a high-income country, n=3; intervention delivered in childcare settings, n=14; targeted programme (child factors), n=37; targeted programme (adult or family risk factors), n=88; mean age of children at intervention >24 months, n=53; mean age of children at outcome >36 months, n=5; no child development outcomes, n=17.

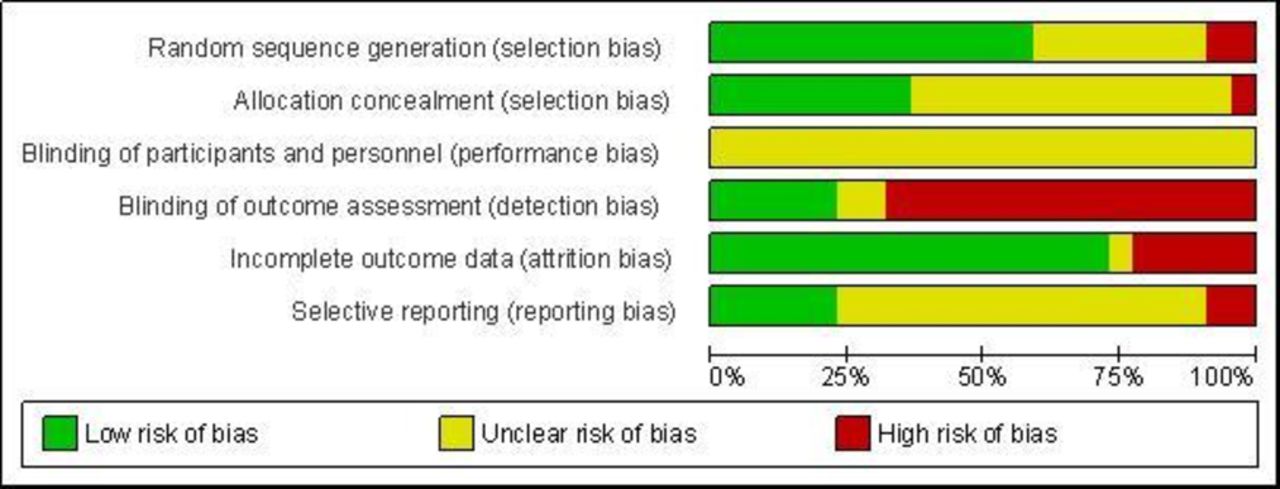
Risk of bias graph: review authors’ judgements about each risk of bias item presented as percentages across all included studies.

{kind=link}
{kind=link}
{kind=link}
Risk of bias summary: review authors’ judgements about each risk of bias item for each included study.
Trial characteristics
The 22 included trials are described in table 1. Three were cluster randomised (clinics25 46 or healthcare workers58), with the remainder randomising individual mothers, parents or mother–child dyads. Ten were conducted in the USA, three in the UK, two in Canada, two in Ireland, one in Australia, one in Chile, one in Japan and one was a multisite study conducted in four Southern European countries. Chang (2015) was conducted in Antigua, Jamaica and St Lucia and is included because Antigua is classified as a high-income country.
Characteristics of the included studies
Seventeen trials compared one intervention with usual care,25–28 36 37 41 44 46 50 51 54–56 58 59 61 although minor augmentations to usual care were made in six of these (eg, with some other information or services made available to parents who wished to access them).26 36 37 56 58 59 One of the trials compared two different interventions with usual care.61 In the remaining five trials, two interventions were compared with each other.24 30 47–49 The timing of intervention delivery varied, from the first month of life only24 to longer term interventions, with eight studies including interventions that continued beyond the child’s second birthday,27 30 36 41 47 50 51 55 and the maximum intervention length being 5 years.50 Studies ranged from 28 to 1593 participants: six included fewer than 100 participants; 12 included between 100 and 500; three included more than 500 participants; and one did not report the number of subjects recruited or analysed.58 In 17 of the 22 trials, outcome data were available for 75% or more of those randomised. All of the trials offered coverage of the intervention to all families in the general population or within a neighbourhood or defined population (eg, recruitment occurred in hospitals serving areas with high levels of social disadvantage or the intervention was made available to all individuals within specific postcodes).25 28 30 41 44 48 59 61 Three trials also included first time mothers only.
Six trials were classified as being at low risk of bias (all compared interventions with usual care), one was at high risk, and 15 had an unclear risk (figures 2 and 3).
Intervention characteristics
Twenty eight interventions were examined in total (see table 2A for studies that included one intervention and table 2B for studies that compared two interventions). Most papers described the body of literature on which the intervention development had been based, but provided less detail on the proposed mechanisms of action of the intervention. Seven were of low intensity: short films followed by group discussions shown in health centre waiting rooms (Chang, see table 2A); sets of building blocks and activity handouts sent to parents by post (Christakis, table 2A); ‘literacy promoting anticipatory guidance’ by paediatricians (High, table 2A); a brief parenting course (Hiscock, table 2A); access to community groups (Wiggins, intervention 2, table 2A) and two different methods for giving feedback to mothers on a neonatal behavioural assessment (Beeghly, table 2B). Ten were of moderate intensity. These included one-to-one home visits (between five (Cheng, table 2A) and twelve visits (Wiggins, table 2A) in total), group sessions (up to eight in total (Feinberg, Niccols 2008, Niccols 2009, all table 2A)), training for primary healthcare workers in interview techniques that encouraged consideration of child development (Tsiantis, table 2A), training for parents in daily activities to promote motor development (Lobo, table 2B) or a combination of different components (Santelices table 2A, Doyle table 2B). Eleven interventions were of high intensity. They were classified as such because they included multiple components (up to a maximum of eight) and regular contact with parents over a sustained period of time or intensive contact for a shorter period of time. In the five studies that included two interventions, the interventions were of the same intensity in all but one (Doyle, which compared a medium intensity intervention with one of high intensity). The aim of these studies was to compare different models of care with each other.
Description of intervention components and intensity
The mode of delivery of the intervention varied between trials. The intervention was delivered by health professionals in seven trials,24–26 44 46 47 58 by other professionals (including ‘parent educators’, ‘family visitors’ or researchers) in eight trials,30 36 48 50 54–56 59 by a mixture of health and other professionals in three trials37 41 51 and by peer mentors in one trial.28 One trial examined one intervention delivered by health professionals and another delivered by community support groups.61 In the remaining trials, one included materials delivered to parents by post27 and one examined training for parents by a physiotherapist to deliver a handling and positioning intervention.49
A full narrative summary of the results, including the tools used to assess the outcome in each trial and the estimates of intervention effects, is given in online supplementary web appendix C. Many of the trials reported several measures of the same outcome and/or measured outcomes at different time points, resulting in multiple comparisons for each outcome. The findings are summarised by outcome in table 3 and are described below. Effect estimates are given in the text below only for the studies found to be at low risk of bias. An effect direction plot66 provides a visual display of the results across all outcome domains, ordered by risk of bias and the intensity of the intervention (table 4).
Summary of findings
Effect direction plot, ordered by risk of bias and intensity of intervention (key given in footnote)
Motor development outcomes
Six studies, including a total of 37 comparisons in 1276 participants, reported motor development outcomes using validated tools. The quality of the evidence was moderate. Three studies comparing one intervention with usual care showed no effect (972 participants, three comparisons), and three studies in which two interventions were compared (304 participants) showed no effect in 25 of 34 comparisons. The positive effects were all from one study of 28 infants who received a daily 15-minute handling and positioning intervention or a social interaction intervention for three weeks.49 In addition to its small sample size, this study had an unclear risk of bias. Only one study at low risk of bias examined motor development outcomes.28 This study found no difference in the mean scores for the psychomotor scores of the Bayley Scale of Infant Development between the intervention and control groups (mean difference 1.64, 95% CI -0.94 to 4.21, p=0.21).
Language development outcomes
Ten studies including a total of 43 comparisons examined this outcome, with nine using validated tools. The total number of participants for this outcome is unknown as one study did not report numbers,58 but was in excess of 3000. The quality of the evidence was low. Seven studies comparing 1 intervention with usual care showed no effect in 10 comparisons, a positive effect in 4 comparisons and a negative effect (poorer language development in the intervention group) in 2 comparisons. Three studies which compared 2 interventions (632 participants) found no difference between the interventions in 23 comparisons and a positive effect in 4 comparisons. Only one study at low risk of bias examined language development outcomes.61 This study compared two different interventions with usual care (supportive health visiting (SHV; moderate intensity) and community groups (CGS; low intensity)). This study found that fewer mothers in the SHV group expressed a worry about their child’s speech than in the control group (risk ratio 0.46, 95% CI 0.23 to 0.93), and no difference in the number of number of mothers expressing worries about speech between CGS and control (risk ratio 1.22, 95% CI 0.78 to 1.92).
Cognitive development outcomes
Eight studies, including a total of 40 comparisons in 2245 participants, examined cognitive development outcomes. All used validated tools, except for one where videotaped interactions were coded for ‘independent goal-directed play’.48 The quality of the evidence was low. In 5 studies (1729 participants) comparing 1 intervention with usual care, there was no effect in 18 of 20 comparisons, and a positive effect in 2 comparisons. Three studies which compared two interventions (516 participants) found no difference between the interventions in 16 of 20 comparisons and a positive effect in four comparisons. Two studies at low risk of bias examined cognitive development outcomes. One study28 found no difference in the mean scores in the intervention and control group for the mental development scores of the Bayley Scale of Infant Development (mean difference −0.81, 95% CI −2.81 to 1.16, p=0.42). The other50 found no difference in mean scores between intervention and control on cognitive development using the British Ability Scale (mean score in intervention group -0.05 (SD 1.01) and in control group 0.03 (SD 0.99), Hedges g effect size −0.63, 95% CI −0.28 to 0.15, p=0.56).
Social and emotional well-being outcomes
These outcomes were examined in 156 comparisons in 18 trials (total participant numbers unknown as 1 study did not report participant numbers58 but was in excess of 5000). Many different outcomes were examined (see online table C4 in the supplementary web appendices for details), with most assessed using validated tools (such as the Child Behaviour Checklist, the Infant Behaviour Questionnaire, the Parent–Infant Relationship Global Assessment, the Q-Sort Measure of the Security of Attachment and social and emotional well-being scores from the Ages and Stages Questionnaire). Most focused on behavioural outcomes.
The quality of the evidence was low. In 15 studies comparing 1 intervention with usual care, there was no effect in 60 of 69 comparisons. In the 3 studies which compared 2 interventions (630 participants), there was no difference between the interventions in 82 of 87 comparisons, a positive effect in four comparisons and a negative effect in one comparison. Six studies at low risk of bias examined social and emotional well-being outcomes, and none found a difference between intervention and control groups. The largest of these46 found no difference in mean scores between intervention and control for externalising or internalising behaviours measured using the Child Behaviour Checklist at 3, 9 or 21 months postintervention. For example, the adjusted mean difference for externalising behaviours at 3 months was 0.16 (95% CI −1.01 to 1.33, p=0.79), at 9 months was −0.79 (95% CI −2.27 to 0.69, p=0.30) and at 21 months was −0.80 (95% CI −2.2 to 0.6, p=0.26).
Overall child development outcomes
Four studies including a total of 12 comparisons in 1565 participants examined global estimates of child development. The quality of the evidence was moderate. Three studies (1414 participants) comparing one intervention with usual care found no effect in seven of eight comparisons based on validated measures of global child development (Griffith Mental Development Scale25 and mean score from the Schedule of Growing Skills II41). Two studies at low risk of bias examined this outcome. In one study,61 there was no difference between SHV and control (risk ratio 0.88, 95% CI 0.39 to 1.99) or CGS and control (risk ratio 0.57, 95% CI 0.22 to 1.52) in the mother’s perception of whether her child’s development was normal. However, mothers in the SHV group had fewer mean number of worries about their child’s development than in the control group (mean difference −0.23, 95% CI −0.42 to −0.01), but there was no difference in the mean number of worries about their child’s development between CGS and control (mean difference 0.13, 95% CI −0.10 to 0.36). The other study, comparing 2 interventions (151 participants), found no difference between the interventions in 4 comparisons (using the mean development score from the Ages and Stages Questionnaire).30
Subgroup effects reported within studies
Subgroup comparisons presented within the individual studies included examining whether the effects were different in families of different incomes or in children with different characteristics (eg, low birthweight infants vs normal birthweight infants, see tables 3 and 4). Some positive effects were seen, but the reporting of these analyses was generally incomplete, with an emphasis on positive intervention effects. No conclusions can therefore be drawn on subgroups in this review.
Stratification of results across studies by risk of bias and intensity of interventions
Table 4 gives the effect direction plot, summarising the results for each outcome, ordered by risk of bias and the intensity of the intervention. In the studies at low risk of bias, there was no intervention effect when either low or high-intensity interventions were studied. Some positive effects were seen in the two trials of moderate intensity interventions, although in one, this was limited to subgroups only (children with ‘disturbed’ attachment at baseline),26 and in the other, positive effects were not consistently seen.61
One study was classified as being at high risk of bias, and this examined a low intensity intervention.44 Inconsistent positive intervention effects were seen in this study, with most of these in one subgroup only. The remaining studies were classified as being at unclear risk of bias, and there is no clear pattern the effects seen in these studies. Programme intensity does not appear to be associated with effectiveness in these studies, in that there is no evidence that higher intensity interventions are associated with more intervention effects.
Table 4 also summarises the uptake and adherence to intervention components. These factors were variable across studies and inconsistently reported. For example, for low-intensity interventions, this ranged from only 19% of the women accessing the intervention at all (community support groups61) to 83% accessing every session.25 Patterns of adherence to the moderate and high-intensity interventions also varied.
No clear pattern in the results were seen when stratification by the other prespecified variables was conducted (see online supplementary web appendix D).
Discussion
The need for interventions to promote child development outcomes in all families has been clearly articulated. Using a broad systematic search of the extensive literature in this field, we found 22 RCTs examining the effect of interventions that enhance health service contacts from the antenatal period to 24 months postpartum. The interventions varied greatly in their content and intensity, and uptake, adherence and fidelity were not consistently reported. The quality of evidence for motor development and overall child development was moderate, and the majority of comparisons showed no intervention effect. The quality of evidence for language development, cognitive development and social and emotional well-being was low. The majority of the comparisons for these outcomes showed no effect, and where positive impacts were observed, within-study effects were inconsistent. Studies that compared one intervention with usual care did not demonstrate more positive intervention effects than studies comparing two interventions. We conclude that there is insufficient evidence to suggest that the interventions reviewed here are effective at improving child development outcomes. The low-to-moderate quality of evidence overall suggests that there is a need for high-quality robust trials to inform current health service delivery in this area.
The strength of our review was the broad search strategy, which encompassed many sources of information other than database searching. We are confident that we have identified most relevant studies (including three trials not yet published in peer-reviewed journals). Although it was not possible to conduct a meta-analysis due to the variation in the types of interventions and methods used to measure outcomes, the narrative review—supplemented with the effect direction plot—provides a comprehensive picture of the limited evidence-base in this field.
To our knowledge, this is the first systematic review of interventions which aim to enhance health service contacts to improve child development outcomes, including social and emotional well-being outcomes in the very early years. Our conclusion is consistent with other reviews of early years interventions. For example, the Allen review9 found that none of the interventions designed for universal use in the early years (defined as conception to school) had ‘best’ quality evidence available to support them. A recent rapid review to update the evidence for components of the Healthy Child Programme in England also found few studies of interventions aiming to promote child development outcomes in all families with children in the 0–5 age range.10 We reviewed a larger number of primary studies than either of these previous publications. Previous studies have also examined the effects of programmes such as these on parental knowledge, attitudes or practices. We did not systematically review parental outcomes here, so cannot comment on whether parents benefited from these interventions. However, we can conclude that—in these studies—any effects on the parents did not, in turn, lead to consistent improvements in child development outcomes.
Understanding how health service contacts can be enhanced to provide support for parents to achieve the best possible developmental outcomes for their children is necessary but challenging. Maternal and child health services consist of many components, many of these untested. Parents also access a wide variety of other forms of support, and the effects of these are poorly understood. Although the evidence base examined in this review is limited, it does allow us to conclude that there is no convincing evidence that the interventions studied provide an additional benefit to the care currently provided in the settings included in these trials. There was also no evidence that interventions of high intensity confer more benefit than those of lower intensity as no dose–response relationship was evident: programmes of greater intensity (in terms of length, number or type of components) did not show more positive intervention effects than programmes of lower intensity. This is consistent with recent evidence for targeted interventions (such as the recent trial of the Family Nurse Partnership programme in the UK67) and has implications for commissioners of early years health services.
Many interventions currently incorporated into health services have not been adequately evaluated, and we recommend further research to generate this evidence. The methodological quality of many of the studies—or the reporting of their methods—was poor (as shown in figure 2 and 3). Eight of 22 trials provided no detail on how their randomisation sequence was generated, and one reported using an inappropriate method. Thirteen provided no detail of allocation concealment, and one reported using an inappropriate method. Ten relied on parental reporting of outcomes only, and a further five used a mix of parental reporting and observations. Although blinding of outcome assessment can be a challenge in studies that rely on parental reporting of their child’s development, validated measures of assessing children’s development without using parental report (eg, coding of videotaped interactions as used in 26 54 55 58) exist and we would encourage their use in research of this kind. We had also hoped that this review would advance our knowledge on the types of social and emotional well-being outcomes that can be influenced by interventions of this kind. However, this was not possible given that the outcomes included were not well defined or consistent and mainly measured behaviour. Future studies that aim to measure effects on social and emotional well-being in young children need better articulation of their conceptual definitions of the social-emotional domains targeted68 and the proposed mechanisms of action of the intervention. Finally, 15 studies did not publish a protocol or provide evidence of trial registration, and 2 did not report on all outcomes described in the Methods section of the paper. Improvements in trial registration and a priori specification of analysis plans are needed in trials in this field.
We also note that adherence was poor across studies and inconsistently reported. Future research should carefully report uptake, adherence and fidelity (particularly whether parents have received the intervention in sufficient dose) to further develop our understanding of the mechanism of action of these programmes and how to engage and retain families.69 70 Involvement of parents from the design stage onwards is essential to improve engagement of families within these important research studies.71 Recent work has shown that monetary incentives can also increase participant retention in RCTs.72 Research is also needed on whether new delivery platforms (such as technology-assisted interventions73) may provide a more engaging, feasible and cost-effective mechanism for providing support to parents.
There have been calls for new public health models of interventions to enhance early child development within existing healthcare systems.74 As shown in our review, however, the current evidence base for interventions delivered to all families is lacking. It is unclear from the literature reviewed why programmes had limited impact on child developmental outcomes. However, many of the interventions relied on parents to change their behaviours and action in relation to their children and were educational in tone but did not have a theoretical framework or a sound basis in behaviour change mechanisms.75 Additionally, authors did not always report on a clear formative research phase or logic model. Future studies should follow guidance on the development and evaluation of complex interventions (such as the Medical Research Council’s guidance).76 The results of all phases of intervention development also need to be published alongside trial results, as current studies alone do not allow us to fully understand why interventions have not produced expected effects.
Currently, there is insufficient evidence that, where health services are available to all families with very young children, additional elements or enhancements to these improve child development outcomes. Early intervention to improve child development is a public health priority, but funding is scarce. There is an urgent need for more robust evaluation of existing interventions and to develop and evaluate novel intervention packages to enhance the offer to all families.
References
Footnotes
Contributors LH, SP, PL, DW, JW and RL conceived and designed the study. MM designed the search strategy (in consultation with other review authors) and performed the database searches. LH and LJG searched the websites and journal table of contents. LH and LJG selected and reviewed eligible reports. LH, LJG, SG, SP and TP extracted data. LH drafted the paper. All authors commented on and revised the paper, and approved the final version. LH is the guarantor for the paper.
Funding This work was funded by Public Health Wales. The Director of Policy, Research and Development at Public Health Wales (Professor MAB) provided expert technical advice during discussions on the study design, the interpretation of the results and the drafting of the paper, and is an author on the paper.
Competing interests None declared.
Patient consent Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement This paper reports on a systematic review. No original study data was obtained from the authors of the trials included in the review. Extra data (such as the results of the review stratified by characteristics other than those included in the report) is available by emailing Lisa Hurt.