Article Text

Abstract
Objectives To identify and prioritise important research questions for miscarriage.
Design A priority setting partnership using prospective surveys and consensus meetings following methods advocated by the James Lind Alliance.
Setting UK.
Participants Women and those affected by miscarriage working alongside healthcare professionals.
Results In the initial survey, 1093 participants (932 women who have experienced miscarriage, 8 partners, 17 family members, friends or colleagues, 104 healthcare professionals and eight charitable organisations) submitted 3279 questions. A review of existing literature identified a further 64. Non-questions were removed, and the remaining questions were categorised and summarised into 58 questions. In an interim electronic survey, 2122 respondents chose their top 10 priorities from the 58 summary questions. The 25 highest ranked in the survey were prioritised at a final face-to-face workshop. In summary, the top 10 priorities were ranked as follows: research into preventative treatment, emotional aspects in general, investigation, relevance of pre-existing medical conditions, emotional support as a treatment, importance of lifestyle factors, importance of genetic and chromosomal causes, preconception tests, investigation after different numbers of miscarriage and male causal factors.
Conclusions These results should be the focus of future miscarriage research. Presently, studies are being conducted to address the top priority; however, many other priorities, especially psychological and emotional support, are less well researched areas. We hope our results will encourage both researchers and funders to focus on these priorities.
- reproductive medicine
- qualitative research
- statistics & research methods
- ultrasound
- depression & mood disorders
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
- reproductive medicine
- qualitative research
- statistics & research methods
- ultrasound
- depression & mood disorders
Strengths and limitations of this study
This is the first time women and those affected by miscarriage have worked alongside healthcare professionals to prioritise research questions.
In total, 2122 participants prioritised these unanswered questions, and 21 key stakeholders agreed the top 10 research priorities for miscarriage during a final consensus meeting.
Demographic analysis showed similar priorities for different ethnicities and agreement between healthcare professionals and those affected by miscarriage.
Refined questions are broad and may be difficult for researchers to interpret.
It is hoped that this top 10 will lead to future research that will address issues of importance for the clinical management of miscarriage.
Introduction
Miscarriage is defined as pregnancy loss from conception to 24 weeks’ gestation. Approximately 15% of all clinically recognised pregnancies end this way.1 Most miscarriages occur in the first trimester, while only 1% occur after 12 weeks’ gestation.2 Recurrent miscarriage, defined as three or more consecutive pregnancy losses, affects about 1% of couples.3 About half of miscarriages are chromosomally abnormal,4 although this is lower in women with recurrent miscarriage.5 It is believed that a proportion of the remainder are of pregnancies carrying lethal recessive genes.6 Despite evidence that some women with recurrent miscarriage may have an autoimmune, thrombotic or endocrine cause; few immunologic, antithrombotic or hormone therapies have yet been shown to be effective. The exception is antiphospholipid syndrome (APS), the most important treatable cause of recurrent miscarriage, affecting 15-20% of women.3 A combination of heparin with aspirin may be helpful for women with this condition , however, the vast majority remain unexplained and most women receive no explanation for their miscarriage. Despite substantial evidence about the appropriate place for medical, surgical and conservative treatment for ongoing miscarriage, there remain gaps in our knowledge about how to minimise psychological sequelae.7 There is also uncertainty about the appropriate investigation for women who have had particular numbers of miscarriages.8 The best way to care for women experiencing miscarriage is uncertain, both when it occurs and in subsequent pregnancies.9 Which of these areas of research should be a priority? Traditionally, the research agenda has been set by the pharmaceutical industry and researchers themselves. A large proportion of miscarriage research has been funded by charitable trusts, but little consideration has been given to the priorities of women who have experienced miscarriage, their partners and the healthcare professionals (HCPs) who care for them. The James Lind Alliance (JLA), established in 2004, is a non-profit initiative with the aim of making healthcare research funders aware of these issues that matter most to patients and clinicians.10 The JLA, whose infrastructure is now funded by National Institute of Health Research (NIHR), achieves this through priority setting partnerships (PSPs), which bring together patients, carers and clinicians to identify and prioritise the top 10 uncertainties, or unanswered questions, about the effects of treatments.10 The first PSP focused on asthma,11 the NIHR have since funded a £1.2 million study into the benefit of breathing exercises.12 In women’s health, PSPs have been conducted in preterm birth, stillbirth and, most recently, endometrial cancer.13–15 We established the miscarriage PSP for women, those affected by miscarriage and HCPs to collaboratively identify and prioritise important questions for miscarriage research.
Methods
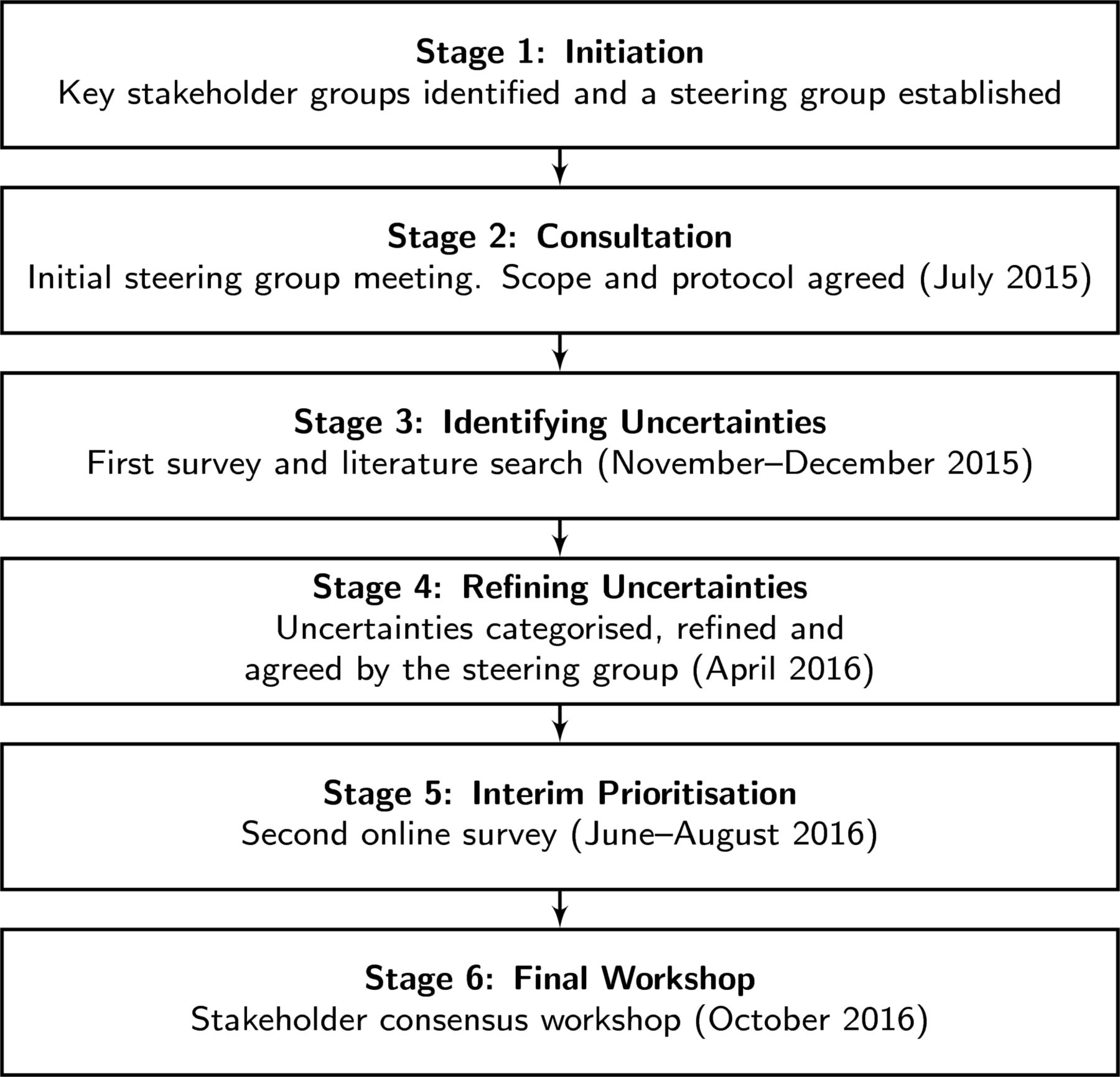
Oversight was provided by a steering group listed in online supplementary appendix 1 , independently chaired by a JLA facilitator (LM), consisting of women affected by miscarriage, charities representing them and HCPs. The six stages of the PSP are outlined in figure 1 and follow the PSP process described by the JLA.10 The protocol was agreed and published on the JLA website before the PSP began (http://www.jla.nihr.ac.uk/priority-setting-partnerships/miscarriage/). Previous JLA PSPs have been reviewed by research ethics committees and judged as service evaluations, and therefore as not requiring research ethics committee review. In view of this, in the present case, we followed the practice of many recent PSPs14 16–18 and made this decision ourselves without formally asking the research ethics committee.
Supplementary file 1

The six-stage process of the miscarriage priority setting partnership.
Initiation
Key stakeholder groups were identified through a process of peer knowledge and consultation. First, the PSP approached all organisations we knew that represented the following groups: women who have experienced miscarriage; partners, family members, friends or colleagues of women who have had a miscarriage; and doctors, nurses and professionals allied to medicine with clinical experience of treating miscarriage. Organisations approached at this stage were the Miscarriage Association, Tommy’s, Royal College of Obstetricians and Gynaecologists (RCOG) Womens Network, Scottish Care & Information on Miscarriage, Fertility Network UK, Hughes Syndrome Foundation, Ectopic Pregnancy Trust, Birthrights, Mumsnet, Netmums, Babyloss, the Association of Early Pregnancy Units, the Royal College of Nursing, the British Fertility Society and the Royal College of General Practitioners. These organisations were consulted about the PSP, invited to participate and identify groups who had been excluded, so we could invite them also. Partner organisations identified interested individuals to form a steering group. The steering group reviewed the partner organisations to ensure a broad spectrum of participants and to verify that all key stakeholders had been invited to be involved. Non-clinical researchers and representatives of the pharmaceutical industry were excluded. Steering group members completed a declaration of interest form. The declaration included declaring: competing interests that could be seen to influence participation in the miscarriage PSP; any publicly declared strong opinions about miscarriage; receipt of any funding that may influence your contribution; and involvement in any other activities or initiatives that may be seen to influence conduct.
Consultation
The steering group was a balanced composition of women who had experience of miscarriage, charities that represented them and clinicians. Some members representing charities or HCPs also had personal experience of pregnancy loss. We identified at least four conflicting definitions for miscarriage. Most miscarriages occur before 12 weeks’ gestation, but the definition of early miscarriage varies between organisations. The European Society of Human Reproduction and Embryology uses ‘spontaneous pregnancy demise before 10 weeks of gestational age’; the RCOG ‘before 10 completed weeks’; and the National Institute for Healthcare and Clinical Excellence (NICE) ‘before 13 completed weeks’. In the UK, the legal definition is spontaneous pregnancy loss ‘before 24 weeks’ gestation’. Patient representatives highlighted that many women would not consider a second trimester pregnancy loss to be a miscarriage. Since two previous PSPs had ranked research priorities for stillbirth and preterm birth, the steering group decided that it was unlikely that another PSP would be formed to include late miscarriage. Therefore, we chose to define miscarriage as anything from a positive pregnancy test to pregnancy loss before fetal survival was possible. Threatened miscarriage was also included. All aspects of miscarriage including conservative, medical and surgical management, psychological sequelae, treatments for recurrent miscarriage, complementary therapies, nutrition and service design were included within the scope of the priority setting process. Other early pregnancy complications, ectopic pregnancy, gestational trophoblastic disease and termination of pregnancy were excluded.
Identifying questions
An online pilot survey was created consisting of an explanation of what we would like participants to do, guidance and example questions. To avoid bias, example questions were taken from submissions to other PSPs unrelated to women’s health. Participants were simply asked: what unanswered questions about miscarriage would you like to see answered by research? Each participant could complete up to three free text responses. The survey tool was peer reviewed by the steering group and piloted by eight women and five HCPs. Content validity was ensured by this peer review and piloting process. Given the range of different constructs measured, internal consistency calculations were not undertaken. The feedback received was used to rephrase medical language in the description and refine the accompanying text for clarity. The refined survey was hosted at www.miscarriagepsp.org and distributed by partner organisations using their own networks; promotion in newsletters and conferences; printed flyers in clinics; online forums and social media. Participants could answer the initial survey anonymously. In addition to the public survey, we also performed a literature search of DARE, the Cochrane Library, RCOG Green Top-Guidelines, NICE Guidelines and the HTA Database for previously published research questions falling within the scope of the PSP.
Refining questions
The aim of this stage was to review the questions gathered in the identification stage and create a list of summary questions. First, we removed non-questions (statements or comments) and questions not related to miscarriage deemed being out of scope. The remaining questions were assigned categories by a single researcher (MP) who qualitatively developed a taxonomy based on the focus of each uncertainty in turn. For example, ‘Are there any ways to protect against miscarriage?’ was assigned to a ‘prevention’ category. In total, there were 20 categories shown in online supplementary appendix 2. Where a respondent included more than one uncertainty in the same question, we duplicated the response and assigned it to each category. Each category was collaboratively reviewed by at least one HCP and one patient representative from the steering group. At this stage, duplicates were excluded and questions were combined and rephrased to create summary questions, which we refined into a standard format.10 The full list of summary questions was checked and agreed by the steering group. The Cochrane Library, MEDLINE, Embase and CINAHL were searched from the inception of each until May 2016 for systematic reviews of interventions for the management of miscarriage. All summary questions were checked against the evidence base to determine if they were true questions or if the survey respondent was unaware there was already evidence to answer their question. If evidence was available, a link was passed onto the survey respondent so they could access it themselves.
Interim prioritisation
The aim of the interim stage was to rank the summary questions into those considered important by women and those affected by miscarriage and those considered important by HCPs. To do this, the refined set of questions were put into a new online survey and displayed in a randomised sequence each time it was accessed. This second survey was hosted at www.miscarriagepsp.org and participants invited by partner organisations and advertised using newsletters, online and social media. Participants were asked to read the list of questions and identify their 10 priorities. Questions were ranked based on the frequency they had been chosen. Participants could answer this survey anonymously. Analysis of the top priorities for patients and HCPs and women from different ethnic origins was performed to ensure the overall rankings represented all groups. The top 25 questions were taken to the final workshop.
Final workshop
Participants were invited to the workshop, representing women and partners affected by miscarriage, including representatives from charities and HCPs. Prior to the meeting, participants completed a declaration of interest form and individually prioritised the top 25 questions presented in random order labelled A–Y. This allowed them to attend the workshop with an idea of their own top 10. The workshop was chaired by an independent JLA facilitator (KC) with no previous experience of miscarriage. Ground rules were agreed at the start of the meeting to ensure confidentiality of individual’s responses and respecting others views and compromise. This process intended to prevent the domination of the discussions by a single member, encourage quieter members of the group to speak and highlight that consensus meant people were unlikely to leave the meeting with all their views being represented in the final top 10. Participants were divided into three groups of mixed representation of women and those affected by miscarriage and HCPs. Each group, chaired by a JLA facilitator, was asked to prioritise all 25 questions, which were printed on A4 cards. Each card had the interim prioritisation for each group (women and those affected by miscarriage and professionals) written on the back, to assist with decision making. The three sets of rankings were combined into one list. Participants were then divided into three different groups, again with mixed representation. In the second round, the groups were presented with the combined prioritisation from round one. Participants were asked to focus on whether the correct questions were in the top 10 and had the right prioritisation. In the final round, all three groups’ priorities were combined and presented to the entire group. The focus was on the top 10. When disagreement arose, consensus was reached by raised-hands voting. The top 10 research priorities in miscarriage were agreed.
Findings
The findings of the miscarriage PSP were reported to funding and research agenda setting organisations including NIHR Evaluation, Trials and Studies Coordinating Centre, which include the HTA Programme, and the Medical Research Council. The findings were also reported to Wellbeing of Women and Tommy’s as major research funding charities in this field.
Results
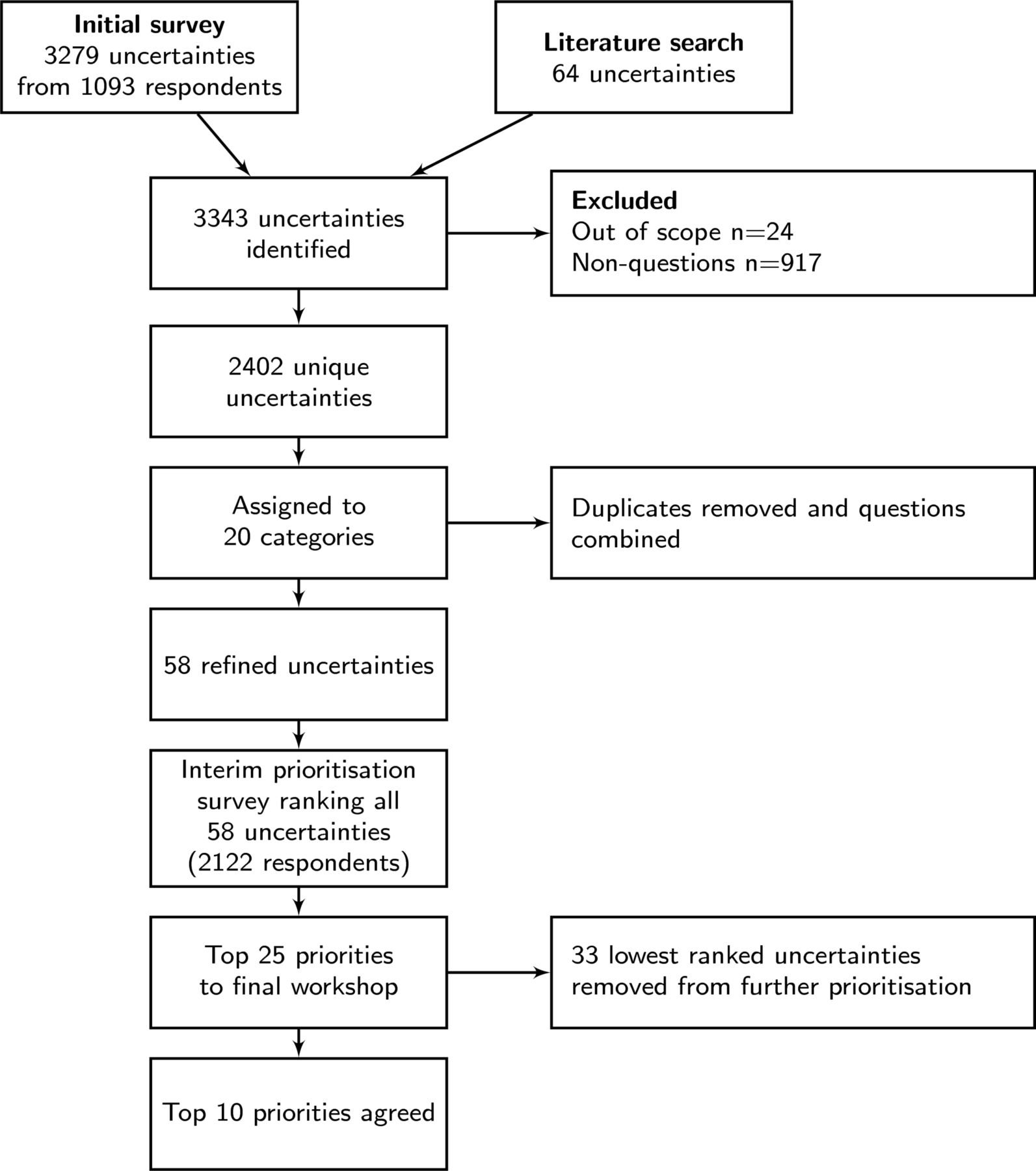
A flow diagram of the process and results are shown in figure 2.

{kind=link}
{kind=link}
Flow diagram of process.
Consultation and identifying questions stages
The initial survey was open from 2 November 2015 to 31 December 2015. Overall, 1093 participants submitted 3279 questions via the survey and 64 were identified by a literature search. Survey respondents included 932 women who have experienced miscarriage, 8 partners, 17 family members, friends or colleagues, 104 HCPs and 8 charitable organisations. Participants were distributed according geographical regions as follows: East Midlands: 84 (8%), East of England: 55 (5%), London: 93 (9%), North East: 74 (7%), North West: 126 (12%), Northern Ireland: 17 (2%), Scotland: 96 (9%), South East: 147 (13%), South West: 88 (8%), Wales: 23 (2%), West Midlands: 128 (12%), Yorkshire and Humber: 72 (7%), outside the UK: 32 (3%) or did not answer: 58 (5%). Nine respondents (1%) had threatened, 598 (68%) one or two miscarriages, and 274 (31%) had recurrent miscarriage. Demographic data for survey respondents are shown in online supplementary appendix 3.
Refining questions
Submissions that were either non-questions or not related to miscarriage were removed and 2402 questions remained. Qualitative sorting generated a taxonomy of 20 categories shown in online supplementary appendix 2. Each category was assigned to at least one patient representative and one clinician from steering group. Duplicates were excluded, and submissions were refined to 58 summary questions. Referring to the existing literature, no questions could be resolved at this stage. All refined uncertainties are shown in online supplementary appendix 4.
Interim prioritisation
The interim prioritisation survey was open between 6 June 2016 and 1 August 2016 and completed by 2122 respondents. Respondents were distributed by geographical regions as follows: East Midlands: 162 (8%), East of England: 125 (6%), London: 180 (8%), North East: 124 (6%), North West: 216 (10%), Northern Ireland: 54 (3%), Scotland: 218 (10%), South East: 341 (16%), South West: 169 (8%), Wales: 65 (3%), West Midlands: 163 (8%), Yorkshire and Humber: 159 (7%), outside the UK: 101 (5%), or did not answer: 45 (2%).
Overall, 1797 women who have experienced miscarriage, 22 partners, 68 family members, friends or colleagues, 185 HCPs and 31 people whose experience of miscarriage was unclear completed the survey. Thirteen women with experience of miscarriage (1%) had threatened, 1213 (67%) one or two miscarriages, and 597 (33%) had recurrent miscarriage. The steering group recognised the imbalance between those who had experienced miscarriage and HCPs. There was also an ethnic imbalance (1942 white British/Irish (95%) and 79 black, Asian and minority ethnic (3.9%) and 18 prefer not to say). Considering this, the overall rankings were compared with those of each subgroup, lay, HCP, white and ethnic minority. The highest 25 overall ranked questions included the following number of questions from each groups top 25: lay: 24, HCP: 18, white: 25 and ethnic minority: 21. No uncertainty in the top 8, for HCPs or the top 18 for ethnic minorities were excluded from the final workshop. This analysis is demonstrated in online supplementary appendix 5. Given this analysis, the steering group agreed to take the 25 highest overall ranked questions to the final workshop.
Final workshop and top 10 priorities
The 1-day workshop took place in October 2016. There were 21 participants including 11 women who had experienced miscarriage, 2 male partners of women affected by miscarriage and 8 HCPs shown in online supplementary appendix 7. The top 10 to research priorities for miscarriage were agreed and shown in table 1.
Top 10 ranked research questions for miscarriage
Publicity
Findings were disseminated to funders of miscarriage research and shared by partner organisations through their own networks. The JLA disseminated the findings and publicised descriptive reports of the process itself. Finally, the steering group published this academic paper.
Discussion
This PSP has established the top 10 research questions for miscarriage.
Strengths and limitations
To our knowledge, this is the first time where women who have experienced and those affected by miscarriage have worked together with HCPs to prioritise research questions. The response to both surveys was comparable with other PSPs shown in online supplementary appendix 6. Nonetheless, as the survey was distributed widely in a variety of different media formats, including social media, we are unable to assess response rate. Care was taken to account for demographic differences between respondents, especially ethnicity and HCPs compared with those who had experienced miscarriage. However, no data were collected for social status, income and level of education that may bias results. Furthermore, this miscarriage PSP was predominantly UK based, with only 5% of respondents from overseas, making results primarily relevant to UK funders and researchers, with relevance to other countries uncertain. Collaborative priority setting between patients and HCPs is seen as a positive progress in research prioritisation, but the optimum proportion of respondents for each category of participants is not known.
The main output of a JLA PSP has traditionally been a top 10 list of questions that focus on treatment.10 To consider a treatment uncertainty to be answered requires an up-to-date systematic review. Recent PSPs, including this one, have considered questions broader than treatment questions. This includes questions which, by definition, cannot be answered by a systematic review of treatments, such as what is the probability of a further miscarriage after one, two, three or more previous miscarriage(s)? Therefore, none of the 58 summary questions could be answered by existing literature. Priorities may be skewed towards common conditions. Rarer conditions may be diluted due to wide public consultation.
Comparison with previous research
Guidelines published by Cochrane, NICE and the RCOG have highlighted research gaps. For example, ‘are there any lifestyle or personal interventions that can prevent miscarriage?’; ‘what types of care are effective in preventing mental health problems for mothers and fathers during and immediately after a miscarriage?’; and ‘does surgery reduce miscarriage in women with uterine anomalies?’. Our PSP process has confirmed them as being important to women and HCPs. Miscarriage can be considered part of the spectrum of poor reproductive outcome ranging from subfertility, miscarriage, preterm birth, stillbirth and neonatal death. Indeed, some of the potential causes and treatments are the same. Comparing our priorities with those of the preterm birth13 and stillbirth 14 demonstrated some overlap show in table 2. What are the effective interventions to prevent miscarriage and preterm birth were the top priorities and the eighth priority for stillbirth. There was desire to see further research into how best to provide emotional support to women experiencing all three conditions and both the miscarriage and stillbirth partnerships prioritised lifestyle factors sixth and third, respectively. To complete this spectrum of prioritisation, a fertility PSP is required, but we anticipate there will be considerable agreement with the priorities of related PSPs.
Comparison with preterm birth and stillbirth PSPs.
Clinical implications
Clinicians need to be cognisant of the uncertainty in the treatment of miscarriage when counselling women. Two priorities in the top 10 are on the emotional well-being of women and their partners. There has been very little good quality research on improving physical and emotional health for couples with pregnancy loss.19
Research implications
It is reassuring ongoing studies are closely aligned with these priorities. Both the NIHR-funded PRISM and C-Stitch trials intend to help answer the top priority, investigating progesterone and cervical cerclage to prevent miscarriage, respectively. Nonetheless, many other priorities especially psychological and emotional support are less well researched areas. We hope our results will encourage both researchers and funders to focus on these priorities. Some questions cover broad topics, overlap with other questions or do not translate easily into questions research studies can be designed to answer. We intend to work closely with NIHR to refine these priorities into research questions with involvement from patients and professionals. Nonetheless, future research must be high quality as simply adding more poorly quality studies will not provide answers to these important questions. Study design must be appropriate to the research question and follow EQUATOR guidelines for publication.
Acknowledgments
We would like to thank members of the Miscarriage PSP steering group (appendix 1) and partner organisations who have publicised the PSP. These include The James Lind Alliance, The University of Nottingham, Nurture Fertility, The Miscarriage Association, Mumsnet, Tommys, Royal College of Obstetricians and Gynaecologists, Royal College of Obstetricians and Gynaecologists Women’s Voices Involvement Panel, The Hughes Syndrome Foundation, The British Society for Gynaecological Imaging, The British Fertility Society, Association of Early Pregnancy Units, Wellbeing of Women, Fertility Network UK, The Ectopic Pregnancy Trust, Birthrights, Netmums, The Royal College of Nursing, Fertility Fairness, College of Emergency Medicine, Miscarriage Support Scotland, Muslim Bereavement Support Service, The Royal College of General Practitioners and ISUOG. We would also like to thank the delegates who attended the final workshop (appendix 7). Finally, we would like to thank women who have experienced miscarriage, those affected by miscarriage and healthcare professionals who participated by submitting their questions and prioritising them.
References
Footnotes
Contributors MP made the initial application to the JLA for a Miscarriage PSP, organised Steering Group meetings and teleconferences, contacted and enrolled partner organisations, designed the surveys, liaised with partner organisations throughout the PSP, conducted the literature reviews, wrote regular website updates and wrote the majority of the final manuscript. LM (JLA chair) chaired all meetings and teleconferences and organised the final workshop, which was led by Katherine Cowan, JLA facilitator. LM ensured compliance with JLA methodology throughout. MP, CB, JB and LR organised dates, venues and facilities for meetings and teleconferences, including the final workshop. MP drafted and circulated minutes of every meeting and teleconference. All authors classified the suggestions received from the first survey, and subsequently compiled the shortlist of 58 summary questions, with guidance from LM. All authors collectively drafted and approved the PSP protocol and terms or reference. All authors attended a majority of teleconferences. MP, JB, AC, BH-J, EO, JS and JT attended the final workshop; all authors collectively signed off on steering group decisions (as guided by LM). All authors actively promoted and disseminated both surveys to their respective partner organisations and to other stakeholder groups where relevant; JO designed the PSP logo and poster advertising for first survey. All authors made comments and suggestions for the final manuscript and approved it before submission.
Funding This study was funded by the University of Nottingham. It was also supported by the Royal College of Obstetricians and Gynaecologists, Royal College of Nursing, Tommy’s, The Miscarriage Association and Imperial College Healthcare NHS Trust who kindly provided venues for meetings free of charge.
Competing interests JB is chief executive of Tommy’s baby charity, which funds research to prevent and treat miscarriage. RS is chair of the Association of Early Pregnancy Units. BH-J is vice chair of the Miscarriage Association and represented them in the PSP. She works for Roche pharmaceuticals in clinical research, but Roche do not have any products or conduct research for miscarriage. LR is president of the Royal College of Obstetricians and Gynaecologists. AC is director of Tommy’s National Centre for Miscarriage Research at the University of Birmingham.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement No additional data are available.