Article Text

Abstract
Context To assess the global burden of late and/or poor management of severe neonatal jaundice (SNJ), a common problem worldwide, which may result in death or irreversible brain damage with disabilities in survivors. Population-based data establishing the global burden of SNJ has not been previously reported.
Objective Determine the burden of SNJ in all WHO regions, as defined by clinical jaundice associated with clinical outcomes including acute bilirubin encephalopathy/kernicterus and/or exchange transfusion (ET) and/or jaundice-related death.
Data sources PubMed, Scopus and other health databases were searched, without language restrictions, from 1990 to 2017 for studies reporting the incidence of SNJ.
Study selection/data extraction Stratification was performed for WHO regions and results were pooled using random effects model and meta-regression.
Results Of 416 articles including at least one marker of SNJ, only 21 reported estimates from population-based studies, with 76% (16/21) of them conducted in high-income countries. The African region has the highest incidence of SNJ per 10 000 live births at 667.8 (95% CI 603.4 to 738.5), followed by Southeast Asian, Eastern Mediterranean, Western Pacific, Americas and European regions at 251.3 (132.0 to 473.2), 165.7 (114.6 to 238.9), 9.4 (0.1 to 755.9), 4.4 (1.8 to 10.5) and 3.7 (1.7 to 8.0), respectively. The incidence of ET per 10 000 live births was significantly higher for Africa and Southeast Asian regions at 186.5 (153.2 to 226.8) and 107.1 (102.0 to 112.5) and lower in Eastern Mediterranean (17.8 (5.7 to 54.9)), Americas (0.38 (0.21 to 0.67)), European (0.35 (0.20 to 0.60)) and Western Pacific regions (0.19 (0.12 to 0.31). Only 2 studies provided estimates of clear jaundice-related deaths in infants with significant jaundice [UK (2.8%) and India (30.8%).
Conclusions Limited but compelling evidence demonstrates that SNJ is associated with a significant health burden especially in low-income and middle-income countries.
- neonatology
- jaundice
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
What is already known on this topic?
Acute bilirubin encephalopathy (ABE), exchange transfusions and death are frequent and costly outcomes of severe neonatal jaundice (SNJ) especially in low-income and middle-income countries.
Long-term disabilities including cerebral palsy and deafness can occur following ABE.
The actual burden of SNJ is not well documented.
What this study hopes to add?
A review of population-based literature to assess the global impact of severe neonatal jaundice (SNJ) highlighting the importance of this disease as defined by its clinical presentations.
Objective evidence that the burden of SNJ is not evenly distributed and that a heavier burden of disease is born by low-income and middle-income countries.
The limited amount of population-based data currently available and the need to capture this information globally.
Introduction
Newborn jaundice occurs in up to 85% of all live births.1–3 In the absence of haemolysis, sepsis, birth trauma or prematurity, it usually resolves within 3–5 days without significant complications.1 However, epidemiological evidence suggests that severe neonatal jaundice (SNJ) results in substantial morbidity and mortality.4 SNJ has been recognised as a significant cause of long-term neurocognitive and other sequelae, cerebral palsy, non-syndromic auditory neuropathy, deafness and learning difficulties.5 6 The burden is unacceptably high in low-income and middle-income countries (LMICs) and has prompted calls for intense scrutiny and attention.4 Under the millennium development goals, the potential impact of adverse perinatal conditions such as preterm birth complications and birth asphyxia on thriving and well-being beyond survival rarely received attention.7 With the current focus on inclusiveness for persons with disability under the sustainable development goals (SDGs), it is essential that we tackle SNJ as one key component of optimising neurodevelopmental outcome.7 8
A recent report by Bhutani et al 4 noted that at least 481 000 term/near-term neonates are affected by SNJ/hyperbilirubinaemia each year, with 114 000 dying and an additional 63 000 surviving with kernicterus. However, these alarming estimates were based on limited data determined by mathematical modelling as true population-based data are limited and difficult to find. Therefore, the incidence of SNJ and thus its contribution to global neonatal morbidity and mortality presently remain unclear and possibly significantly underestimated.
Jaundice is usually recognised around a total serum bilirubin (TSB) of 5 mg/dL in neonates.3 SNJ is unlikely to happen before a TSB of at least 20–25 mg/dL in term neonates presenting early.4 TSB is unfortunately often either not available or delayed in many LMICs.9 Therefore, for the purposes of this article, severe SNJ is defined as jaundice associated with acute bilirubin encephalopathy (ABE)/kernicterus and/or exchange transfusions (ET) and/or jaundice-related death.
Phototherapy and ET are widely used therapeutic modalities for jaundice.2 However, due to constrained resources, devices for measuring bilirubin10 11 and effective phototherapy are often lacking in LMICs.12 This, together with higher prevalence of glucose-6-phosphate dehydrogenase (G6PD) deficiency, blood group incompatibilities, late referrals and delayed recognition of excessive bilirubin levels in LMICs, has necessitated excessive use of ETs.13
We systematically reviewed the available evidence pertaining to the global burden of SNJ to inform child health policy regarding its prevention and management especially in LMICs.
Methods
Search criteria
Although most SNJ occurs at TSB at 20 mg/dL (343 µmol/L), there is no standard worldwide definition of SNJ or clinically significant TSB necessitating medical intervention. There is a wide range of definitions of significant jaundice. In studies reviewed in this article, TSB levels considered significant, when results were available, generally ranged from 15 to 30 mg/dL.14–27 Even though beginning in 2004, the American Academy of Pediatrics recommended ABE be used for acute manifestations of SNJ in the first weeks of life and kernicterus for chronic manifestations of SNJ/ABE,28 many still use the terms interchangeably. Because of limited availability of TSBs and our attempt to quantify the burden of clinical disease, we defined SNJ clinically using ABE, ET and jaundice-related death.
We systematically reviewed published papers following PRISMA guidelines (online supplementary appendix 1).13 Databases searched included Ovid Medline, PubMed, CINAHL, Global Health, Scopus, Popline, Africa Journal Online and Bioline databases for published articles on SNJ. We used both controlled subject headings and free-text terms for neonatal jaundice (NNJ), jaundice, bilirubin/blood levels, haemolytic anaemia, G6PD deficiency in various forms and in combination with terms for ET, ABE, kernicterus, death, mortality and phototherapy. Other inclusion criteria were jaundice in first month of life; availability of data on incidence of ABE/kernicterus; provision of information on incidence of ETs for SNJ or jaundice-related death which we defined as SNJ. We also reviewed references of selected retrieved articles and review papers, and contacted authors of relevant articles for missing dates. No language restrictions were used. To be included in the meta-analysis, a study must have reported estimates of incidence from a retrospective or prospective population-based study, increasing likelihood that estimates could be generalised to the geographical location where the study was conducted. The search results were limited to publication dates of 1990 to June 2017. See online supplementary appendix 2 for complete Ovid Medline search strategy.
Data extraction
Two authors examined studies using a predetermined checklist (online supplementary appendix 3) devised by three authors for selecting articles that met inclusion criteria after one author screened titles and abstracts. Two authors independently confirmed eligibility of all full-text articles. Discrepancies were resolved by discussion and when needed by a third author. The following data were extracted from each article: publication year, study design, country, WHO region, sample size, SNJ definition and outcomes (ET, ABE, mortality). Articles were excluded if neonates were enrolled before 1990; study published after June 2017; sample size <10; ET unrelated to SNJ, results limited to only metabolic or primary liver diseases, studies with defined enrolment period, failure to define neonates as having ABE, ET or jaundice-related death and for the meta-analysis if they included only premature neonates.
Quality assessment
We explored several quality assessment tools reported in the literature for observational studies including the Newcastle-Ottawa Scale,29 and found none directly applicable for evaluating diagnostic studies on NNJ /hyperbilirubinaemia. We therefore chose to adopt the tool validated by Wong et al 30 with all the critical components for assessing the risk of bias across studies. Two authors examined four important components of quality/risk of bias assessment: selection of subjects (representativeness), case definition for SNJ (exposure ascertainment), diagnostic criteria for jaundice and outcome measurement. Study quality was judged based on number of criteria that were met: all 4 (high), 2–3 (medium) or 1 (low). Finally, two authors determined which studies were population-based. We defined population-based studies as studies that addressed the incidence of SNJ for a defined population with every individual in the population having the same probability of being in the study and the results of the study having the ability to be generalisable to the whole population from which study participants were sampled and not necessarily the individuals included in the study.31 Disagreements were resolved through consensus after joint reassessment.
Statistical analysis
For the meta-analysis, when multiple reports were obtained from the same population with overlapping study years, the one providing sufficient data (ie, numerator and denominator data) to derive estimates of disease burden was selected. To facilitate meta-analytical techniques, estimates of incidence were logit transformed to enable them to correspond to probabilities under the standard normal and permit use of the normal distribution for significance testing. Pooled estimates were calculated using DerSimonian and Laird’s random effects method, weighting individual study estimates by the inverse of the variance of their transformed proportion as study weight, with their 95% (CI) determined using Clopper-Pearson exact binomial method.32 For presentation, pooled transformed estimates were back transformed. Statistical heterogeneity among studies was investigated using Cochran’s Q test and I2 with a conservative p value less than 0.1 chosen as the level of significance. Forest plots were then used to examine the overall effects. Exploration of potential sources of heterogeneity was undertaken using meta-regression. Whether it is an interventional or an observational study, small studies are more likely to show more extreme values given wider CIs compared with larger studies. Since more extreme findings may be more newsworthy and hence more likely to be published, potential for publication bias was assessed by visual inspection of the funnel plot as well as by formal means using Begg’s adjusted rank correlation and Egger’s regression asymmetry tests.33 All analyses were conducted using R Statistical Software.34
Results
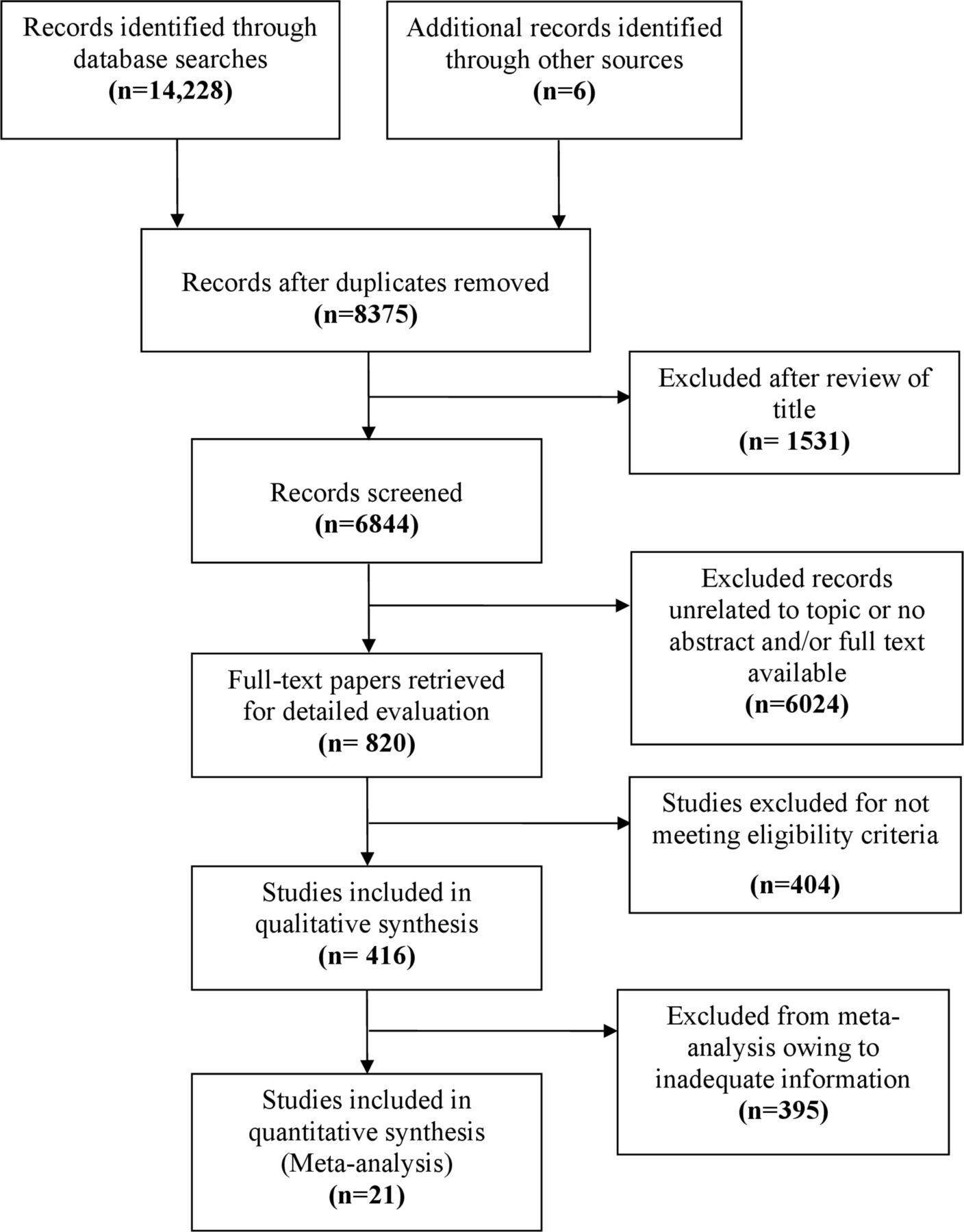
Search of electronic databases identified 6844 articles (figure 1). Eight hundred and twenty papers were reviewed. After excluding studies not meeting inclusion criteria, 416 studies were selected for further review. Multiple languages (Chinese, English, Farsi, French, German, Hebrew, Italian, Norwegian, Polish, Portuguese, Serbian and Spanish) were represented, with translation of relevant sections, but only 26/416 were non-English, none of which were population based. Of these, 416 papers included at least one marker of SNJ, but only 21 provided population-based data on 4 975 406 neonates (table 1).

Flow chart of study selection for the meta‐analysis.
Studies that met the inclusion criteria to be included in the meta-analysis
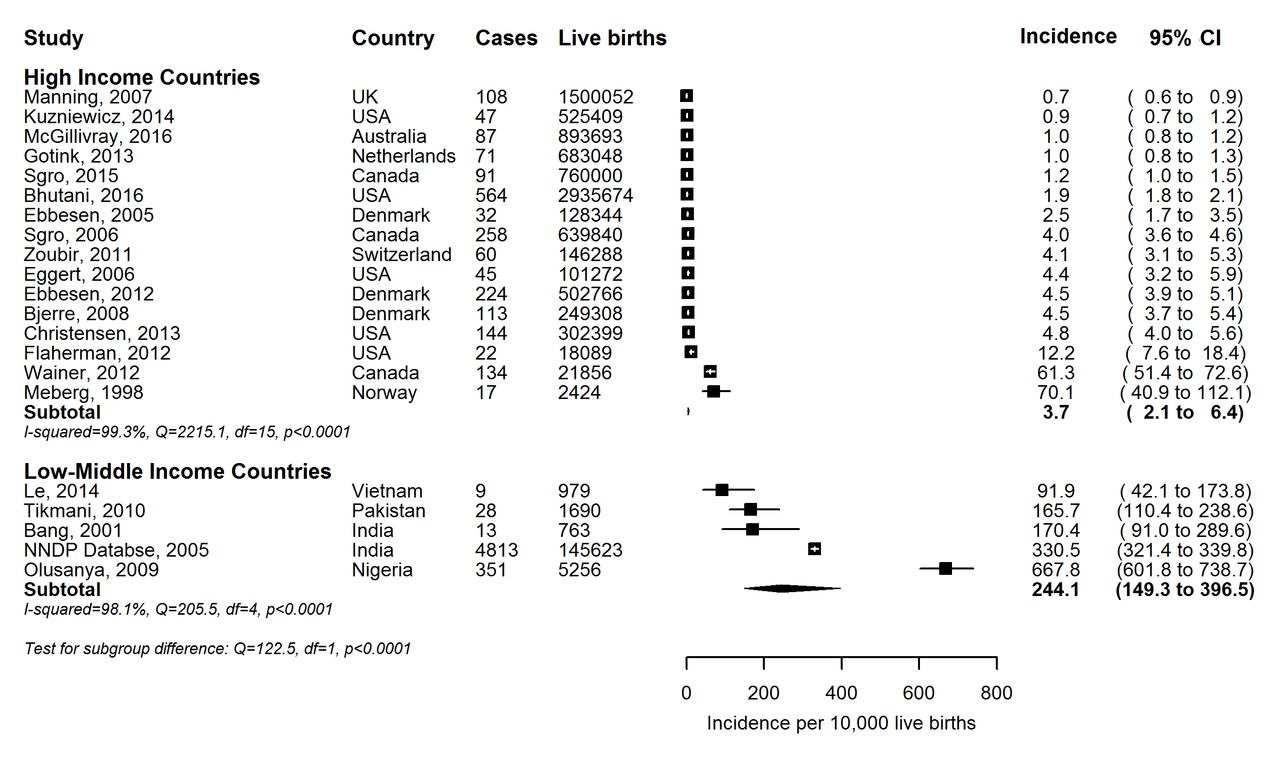
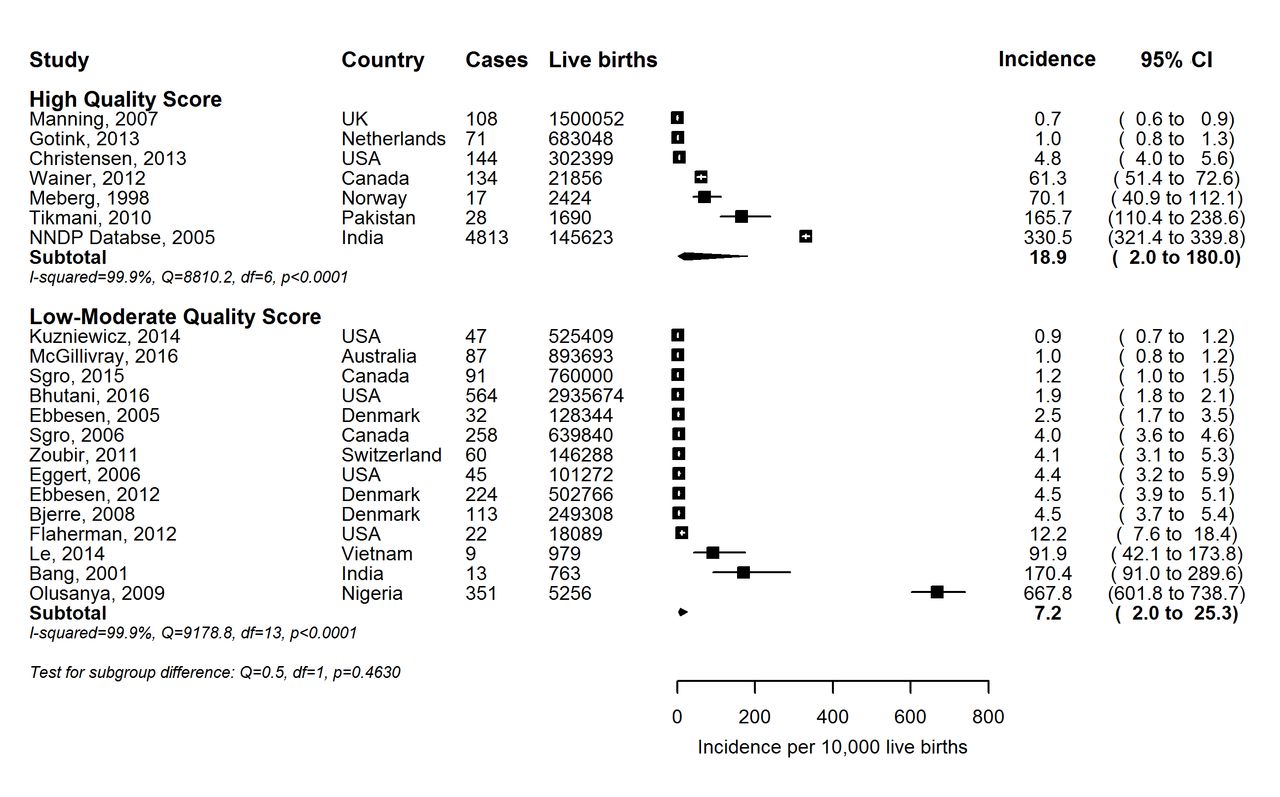
Sixteen (76%) were from high-income countries and 13 (62%) used a prospective study design. High-quality studies tended to report lower incidence compared with low-quality to moderate-quality studies (figure 2). High-quality studies tended to come from high-income countries with less disease while low-quality studies tend to come from LMICs. Overall, incidence estimates of SNJ from high-income countries tended to be lower compared with LMICs (figure 3). Studies which enrolled all neonates regardless of gestational age had a higher incidence of SNJ compared with studies enrolling only term/near-term (table 2).
Pooled incidence (per 10 000) of severe neonatal jaundice among all neonates aged 24 months or less according to study quality.
{kind=link}
{kind=link}
{kind=link}
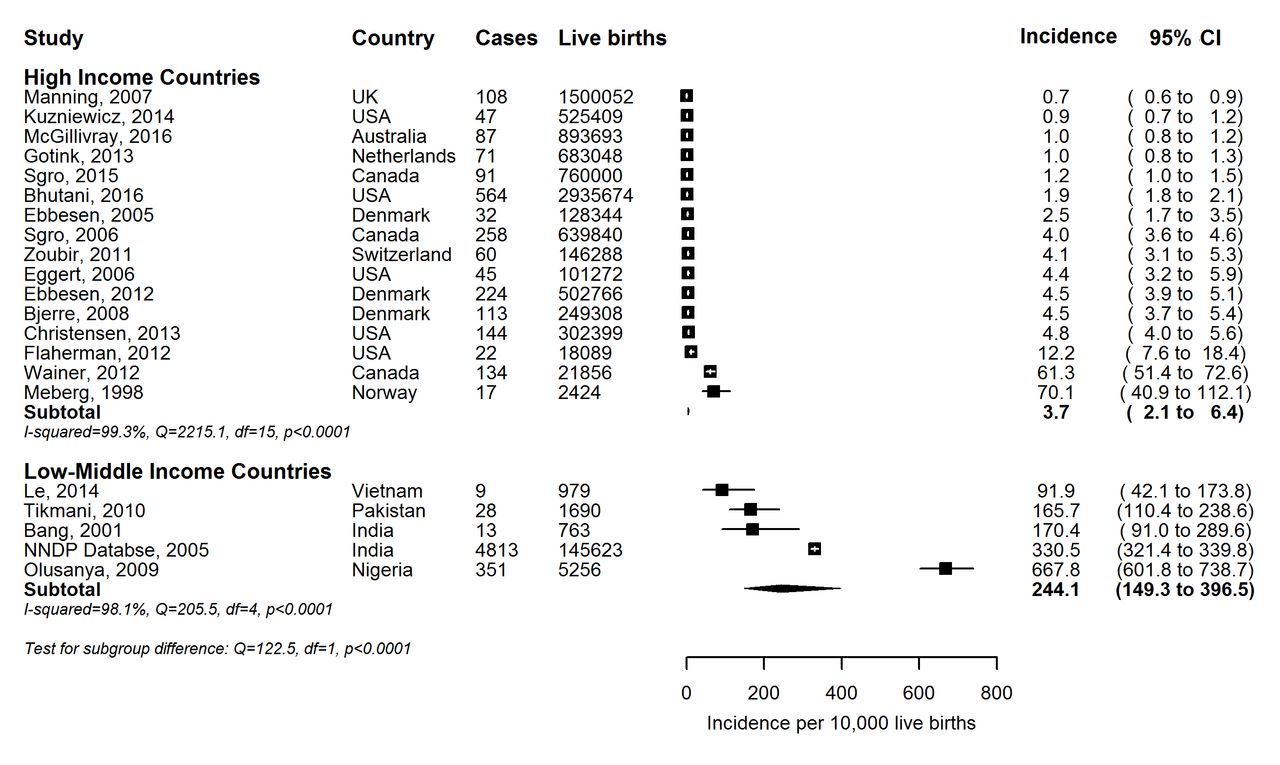
Pooled incidence (per 10 000) of severe neonatal jaundice among all neonates aged 24 months or less according to income.
Incidence (per 10 000 live births) of severe neonatal jaundice among all neonates aged 24 months or less by gestation and study design
The incidence of SNJ per 10 000 live births was highest in the African region at 667.8, followed by Southeast Asian at 251.3, Eastern Mediterranean with 165.7 and Western Pacific region with 9.4. The Americas and European regions each had substantially lower incidence of 4.4 and 3.2, respectively (table 3).
Incidence of severe neonatal jaundice per 10 000 live births, among all neonates aged 24 months or less
The incidence of ET per 10 000 live births was significantly higher for the African (186.5) and Southeast Asian (107.1) regions and lower in Eastern Mediterranean, Americas, European and Western Pacific regions reporting estimates of 17.8, 0.38, 0.35 and 0.19, respectively (table 4).
Incidence of exchange transfusions, per 10 000 live births, among all neonates aged 24 months or less
Visual inspection of funnel plot in which incidences of SNJ were plotted against their standard errors showed asymmetry. This was confirmed by formal tests of publication bias (Begg-Mazumdar test: p=0.016, Egger: bias, p=0.002). The observed heterogeneity between studies may explain the asymmetric funnel plots. In random effects meta-regression analyses, the overall observed between-study heterogeneity explained by covariates which were selected a priori (study design and duration, income classification of country and gestational age) was 66.23%; p<0.001. However, only income classification of country was statistically significant determinant of the incidence of SNJ (table 5). Only two studies provided information on jaundice-related deaths with estimates of 2.8, 30.8 and 50.0 for UK (European),22 and India (Southeastern)35 While one study fromPakistan3 (Eastern Mediterranean), mentions death in 30% of infants with jaundice but stated they did not feel the deaths could be directly attributed to jaundice.
Meta-regression analysis potential factors* influencing the heterogeneity of incidence of severe neonatal jaundice
Discussion
Although data are limited despite our extensive literature review, this systematic review and meta-analysis suggests that the incidence of SNJ is high, with regions that include predominantly LMICs bearing the greatest burden of disease. In the systematic review, mentioned earlier by Bhutani et al 4 18% of 134 million live births had SNJ with the greatest burden of disease in LMICs, and therefore supporting this hypothesis. But as previously pointed out, these estimates were generated by mathematical modelling due to lack of accurate incidence data available. Both Bhutani’s data as well as this review, highlight the glaring paucity of studies particularly in LMICs. Although all WHO regions are represented, only 4/136 (2.9%) LMICs countries were represented with most having only one study (India (Southeast) n=2,25 35 Nigeria (African) n=136 and Pakistan (Eastern Mediterranean) n=1,3 Vietnam (Western Pacific) n=1).37 In contrast representation among high-income countries, while low was better with 8/79 (10.1%) high-income countries having population-based data (Australia (Western Pacific) n=1,23 Canada (Americas) n=3,26 38 Denmark (European) n=3,15 17 39 Norway (European) n=1,24 Netherlands (European) n=1,20 Switzerland (European) n=1,27 USA (Americas) n=5,16 18 19 40 UK and Ireland (European) n=1).22 This general lack of population-based studies worldwide emphasises the need for more accurate data to determine the actual burden of disease.
Jaundice was the primary diagnosis in 17% of neonates ≤1 week in a hospital-based study in Kenya,41 and several other African-based studies demonstrate that SNJ commonly leads to hospital admissions.42–44 This pattern is also observed in Asia, including the Middle East.41 45–49
Although not readily generalisable, all regions do have numerous hospital-based studies among the 416 articles with at least one clinical indicator of SNJ, highlighting the prevalence of SNJ among admissions. For some countries, such as the USA and many European nations where hospital birth is the norm, this data would more accurately reflect true population-based data. However, in LMICs where ‘60 million women give birth outside a facility’ (2012)50 and recorded data population data spares, hospital data cannot be assumed to reflect true population data. The higher incidence of home births correlates well with the much higher incidence of SNJ noted in the studies from the African, Southeast Asian and Eastern Mediterranean regions compared with substantially lower incidence noted in the regions of the Americas and Europe.
Although only one study each from Africa and Eastern Mediterranean met the definition of population based, these two studies underscore the burden of ETs in LMIC’s with 186.5 and 107.1 ET’s per 10 000 live births in stark contrast to the American and European regions with only 0.38 and 0.35 per 10 000 live births, respectively.
ET for SNJ
While many paediatricians and even neonatologists in high-income countries never perform an ET, physicians in LMICs continue to perform ETs on a regular basis.13 Although population-based data were available in only a few LMICs studies, other hospital-based studies support their findings. Of note again is the high prevalence of ETs, reported in studies from many LMIC (22%–86%), particularly Nigeria,36 51 52 India53 54 and Bolivia.55
Access to ET, a proxy indicator of the magnitude of SNJ, is often limited in resource poor countries.13 56 57 Multiple studies have demonstrated early intervention including phototherapy and appropriate ET can prevent kernicterus.56 58 59 Despite benefits of ET, there are associated complications13 making it important to provide effective phototherapy before ET is needed.60
SNJ is significant due to the associated mortality, but some would argue even more so because of associated long-term morbidity especially in LMICs ill-equipped to handle these disabilities. Farouk et al reported abnormal neurological findings in almost 90% of infants returning for follow-up after ABE in their nursery.61 Olusanya and Somefun,62 reported ET as a risk factor for sensorineural hearing loss in their community-based study in Nigeria, as did da Silva et al in Brazil.63
Contribution of SNJ to neonatal mortality
While only two studies in this review,22 35 64 provided information on clear jaundice-related deaths, other studies have shown striking numbers of jaundice-related deaths where it reportedly accounted for 34% of neonatal deaths in Port Harcourt Nigeria,52 15% in Ile-Ife, Nigeria,65 14% in Kilifi District Kenya,66 6.7% in Cairo Egypt67 and 5.5% in Lagos Nigeria.68
Multiple factors contributing to kernicterus in LMICs and the need for solutions addressing these factors has been spelled out in articles by Olusanya et al 69 and Slusher et al 2 including the need for national guidelines,9 60 effective phototherapy, rapid reliable diagnostic tools, maternal and healthcare provider education.70
Contribution of SNJ to long-term disability
Current evidence indicates SNJ continues to contribute significantly to the burden of cerebral palsy, deafness and other auditory processing disorders.4 In India, Mukhopadhyay et al 71 found an abnormal MRI or brainstem auditory evoked response in 61% and 76%, respectively, of children who underwent ET. In Nigeria, Ayanniyi and Abdulsalam72 reported NNJ as the leading cause of cerebral palsy (39.9%) trumping birth asphyxia (26.8%), while Ogunlesi et al 73 also from Nigeria, reported cerebral palsy, seizure disorders and deafness as leading sequelae of ABE, occurring in 86.4%, 40.9% and 36.4%, respectively. Oztürk et al from Turkey,74 observed a history of prolonged jaundice commonly in children affected with cerebral palsy. Summing up available estimates, a recent Lancet article by Lawn et al 75 indicts pathological hyperbilirubinaemia/jaundice in >114 000 deaths and states that there are >63 000 damaged survivors.
The increased global awareness of SNJ has led to improvement in some locations. One notable example of this is Myanmar where a package of services including a photoradiometer, education and intensive phototherapy decreased ET by 69%.76 Another example is the development, ongoing testing and refinement of filtered sunlight phototherapy in areas without access to continuous electricity or intensive phototherapy.77 Several studies have shown that maternal and health worker education, screening programmes14 18 28 38 and national guidelines78 can and do improve outcomes and decrease the observed clinical sequelae of SNJ.14 38 78 Many programmes supported by groups such as WHO79 and Essential Care for Every Baby80 now strongly support screening for jaundice and highlight it as a danger sign needing urgent care. This increased focus and awareness on SNJ is beginning to lead to decreases of this problem even in LMICs where recent studies though not always population based are beginning to show decreases in severe sequela.76
Some limitations of this comprehensive review should be noted, besides those inherent in meta-analysis.81 Only 12/195 sovereign nations82 are represented in the quantitative data. While highlighting one of the greatest problems in determining the actual burden of disease from SNJ, absence of data from other countries despite searching multiple databases limits generalisability of our findings. Another significant limitation is the marked variability in the actual focus of the articles. The populations studied, availability of a TSB, recommendations and methods of screening, differences in TSBs and many other variables of included articles span an extremely wide range. Finally, the initial search excluding articles by title was done by only one author and the auditory evoked brainstem response, which is rarely available in LMICs, where not included in the criteria for SNJ.
Despite these limitations, this review still fills critical holes in our knowledge about the true burden of disease from this devastating but preventable tragedy. To our knowledge, this is the first attempt to report the global burden of SNJ derived from population-based studies. While providing strong evidence for the burden of disease, it highlights the notable lack of population-based data from most countries, especially LMICs where the disease is more prevalent and most devastating. The burden of SNJ and its acute and chronic ramifications establish a strong case for appropriate health education, routine screening, early diagnosis and effective treatment. The spectrum of disease crosses ethnic and socioeconomic boundaries, impacting children everywhere, and is a commonly encountered hospital diagnosis worldwide. SNJ may represent the most common unrecognised and/or under-reported neonatal cause of preventable brain damage.83 More research with capacity building especially in LMICs and other areas where data are limited are needed to truly quantify the impact of this disease and to better understand how to integrate screening and therapy to eliminate this disease in the future.
Conclusion
Compelling but limited evidence from the literature demonstrates that SNJ is associated with a significant acute and chronic health burden, especially in LMICs. There is an urgent need to address this preventable disease in these regions, consistent with the inclusiveness advocated for erstwhile disadvantaged populations under the current SDGs dispensation.
Acknowledgments
We thank Dr Vinod Bhutani, Ms. Judith Hall RNC-NIC, and Dr Mark Ralston for their edits to an earlier version of the manuscript. We also thank Dr Philip Fischer, MD, Dr Reza Khodaverdian, Dr Janielle Nordell, Ms Ann Olthoff, RN, Dr Clydette Powell, Dr Hoda Pourhassan, Dr Maryam Sharifi-Sanjani, Ms Olja Šušilović, Dr Deborah Walker, Ms Allia Vaez and Ms Agnieszka Villanti, RN, for their help in the translation of foreign language literature used in this review. We also thank Ms Ayo Bode-Thomas, Dr Katie Durrwachter Erno, Mr Jeffrey Flores, Ms Judith Hall, RNC-NIC, Mr Jonathan Koffel, Ms Toni Okuyemi, Dr Mark Ralston, Mr Del Reed, Mr Paul Reid, Dr Yvonne Vaucher, Ms Mabel Wafula, Ms Katherine Warner, Dr Olga Steffens for their help in editing the article/tables including retrieving articles, verifying numbers, and managing Endnote.
References
- 1.↵
- 2.↵
- 3.↵
- 4.↵
- 5.↵
- 6.↵
- 7.↵
- 8.↵
- 9.↵
- 10.↵
- 11.↵
- 12.↵
- 13.↵
- 14.↵
- 15.↵
- 16.↵
- 17.↵
- 18.↵
- 19.↵
- 20.↵
- 21.↵
- 22.↵
- 23.↵
- 24.↵
- 25.↵
- 26.↵
- 27.↵
- 28.↵
- 29.↵
- 30.↵
- 31.↵
- 32.↵
- 33.↵
- 34.↵
- 35.↵
- 36.↵
- 37.↵
- 38.↵
- 39.↵
- 40.↵
- 41.↵
- 42.↵
- 43.↵
- 44.↵
- 45.↵
- 46.↵
- 47.↵
- 48.↵
- 49.↵
- 50.↵
- 51.↵
- 52.↵
- 53.↵
- 54.↵
- 55.↵
- 56.↵
- 57.↵
- 58.↵
- 59.↵
- 60.↵
- 61.↵
- 62.↵
- 63.↵
- 64.↵
- 65.↵
- 66.↵
- 67.↵
- 68.↵
- 69.↵
- 70.↵
- 71.↵
- 72.↵
- 73.↵
- 74.↵
- 75.↵
- 76.↵
- 77.↵
- 78.↵
- 79.↵
- 80.↵
- 81.↵
- 82.↵
- 83.↵
Footnotes
Contributors TS and BOO conceptualised and designed the study, acquired data, analysed and interpreted data, supervised the study, drafted the manuscript and conducted a critical revision of the manuscript for intellectual content and approved the manuscript as submitted. TGZ conceptualised and designed the study, and assisted with acquiring data and approved the manuscript as submitted. AMS assisted in acquiring data and approved the manuscript as submitted. EMK and JUS were responsible for acquisition of data as well as providing administrative, technical and material support and approved the manuscript as submitted. SBR was responsible for acquisition of data, analysing and interpreting data and provided administrative, technical and material support and approved the manuscript as submitted. DA, MAS and BWL analysed and interpreted the data, conducted the statistical analysis, and conducted a critical revision of the manuscript for important intellectual content and approved the manuscript as submitted. All authors had full access to all data, take responsibility for the accuracy and integrity of the data and approved the manuscript as submitted.
Funding Support for the quantitative analysis was provided in part by The Programme for Global Paediatric ReSouth-East Asianrch, Centre for Global Child Health, The Hospital for Sick Children, Toronto, Canada.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.