Article Text

Abstract
Objectives To estimate the rate of paediatric attendance at emergency departments (EDs) in the Lombardy Region, Italy, and to determine the factors contributing to different patterns of use.
Methods By analysing healthcare administrative databases, ED attendance by 1.6 million youths <18 years old during 2012 in the Lombardy Region was assessed. The pattern of use was categorised based on the number of ED visits and level of emergency, defined by triage code and outcome of the visit. Logistic regression analyses were performed to identify the characteristics of access for non-urgent reasons and those of patients with frequent non-urgent access (≥4 accesses for non-urgent reasons only). A case–control study was carried out to compare healthcare resource use by children 1–5 years old who were ‘frequent non-urgent users’ with that of randomly selected controls, matched by age, gender, nationality and primary care physician.
Results During 2012, 440 284 (27%) of children and adolescents had at least one ED attendance, with trauma (26%) and respiratory tract infections (22%) as the most frequent diagnoses. In all, 533 037 (79%) accesses were for non-urgent reasons, and 12 533 (3% of the ED users) were frequent non-urgent users. Male gender (OR 1.12; 95% CI 1.08 to 1.17), preschool age (OR 3.14; 95% CI 2.98 to 3.31) and place of residence (OR 1.74; 95% CI 1.70 to 1.99) were associated with a higher risk of being a frequent non-urgent user. Moreover, a greater healthcare consumption was observed in this group.
Conclusions One out of four children and adolescents attended the ED at least once per year, 3% of whom were frequent non-urgent users, with a high overall healthcare resource consumption.
- epidemiology
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
What is already known on this topic?
An overuse of the emergency department (ED) by the paediatric population has been reported worldwide.
This phenomenon can be associated with different patterns of ED use: non-urgent visits, frequent attendance and return visits.
What this study hopes to add?
An evaluation of ED accesses by children and adolescents in a large regional population was performed in Italy.
More than 1 out of 4 youths accessed ED; 3% of ED attendees were frequent non-urgent users and accounted for 9% of visits.
A greater use of healthcare resources (prescriptions for drugs, diagnostic tests and visits) was found in frequent non-urgent users compared with controls.
Introduction
In recent years, a growing rate of emergency department (ED) access was reported in several countries, resulting in an overcrowding of these services. The US National Health Interview Survey in 2015, for example, found that 24% of children <5 years old and 14% of those 6–17 years old had at least one ED access.1 The consequences of this phenomenon are physician work overload, increase in costs, and increased risks of infections and length of stay that lead to dissatisfaction with the ED service.2
Some variables are associated with increased ED utilisation: age (≤5 years), male gender, foreign nationality, low socioeconomic status, low parental literacy level, proximity between ED and child’s house, residence in urban areas, access during cold seasons and out-of-hours and reasons for access (traumatic injuries, respiratory infectious diseases and gastrointestinal disorders).2–17
Moreover, some international studies have identified recurrent patterns of ED utilisation that can contribute to ED overcrowding. Non-urgent visits can account for 5%–90% of ED accesses; this wide range is mainly due to different criteria used for the definition of non-urgency generally based on triage code or diagnosis, treatment and management provided in the ED and outcome.18–20 In all, 2%–8% of the attendees can be considered ‘frequent users’ according to international studies,13 21 22 while 2%–24% of the attendees return to the ED shortly after the first visit (return visit).23–28
According to an Italian National Institute for Statistics survey, the prevalence of ED access in children <16 years old in the 3 months preceding the interview was 5.9% in 2012 and 6.8% in 2014.29
Available Italian studies report that non-urgent visits concern 27.6% of ED users and 58.2% of total paediatric attendance episodes,30 31 with a rate of return visits estimated at 1.4%.32
To the best of our knowledge, however, only one study estimated the prevalence of ED attendance by the paediatric population in Italy,33 and few evaluated the determinants of the different patterns of ED utilisation.30 31
Our study aimed to estimate the yearly prevalence of ED attendance in the Lombardy Region and to determine the factors contributing to the different patterns of use and to assess if frequent non-urgent (FNU) use, a proxy of inappropriate ED use, is associated with a higher healthcare resource consumption.
Patients and methods
Healthcare organisation in Lombardy
Lombardy is the region with the largest population in Italy (10 million inhabitants), covering 16% of the Italian paediatric population.
The Italian National Health Service (NHS) is organised into local health units (LHUs), subdivided into health districts. In 2012, Lombardy had 15 LHUs and 100 health districts, with nearly 110 EDs. The organisation of Lombardy’s healthcare was subsequently rearranged, but in this study, we will refer to the 2012 situation.
Every Italian resident is registered with a family paediatrician (FP) or a general practitioner (GP). Children are assigned to an FP until they are 6 years old; afterwards, the parents can choose to remain with that paediatrician until child is 14 years old or to register the child with a GP. All adolescents over 14 years are assigned to a GP.
Subjects needing emergency care can refer to an ED on any day or night of the week. Access is always free of charge for children younger than 14 years, while older children pay a fee for non-urgent visits.
Triage codes are assigned by triage nurses and consist of four categories, based on nationwide criteria: red (non-deferrable emergency, life-threatening condition), yellow (urgent, but not immediate life-threatening condition), green (low urgency and priority, deferrable care) and white code (non-urgent).34
Data source
The data sources were administrative healthcare databases of the Lombardy Region, routinely used for reimbursement reasons. In particular, four databases were analysed:
A demographic patient database containing information such as unique personal identification code, gender, date of birth, city and LHU of residence and the reference primary care physician (PCP).
An ED database, in which each visit record is associated with its date, time, triage code, ED structure, outcome and discharge diagnosis (International Statistical Classification of Diseases, Ninth Revision).
A drug prescription database containing prescriptions dispensed by retail pharmacies in the region and reimbursed by the NHS.
A specialist visit and diagnostic test prescription database.
Databases are linked by alphanumerical patient identification codes. All data were managed according to the current Italian law on privacy and were analysed using an anonymous subject code.
Population selection
The study population was composed of 1 640 713 subjects <18 years of age living in Lombardy on 31 December 2012.
Data from the Cremona LHU were excluded because of incomplete ED attendance recording.
Pattern of use and contributing factors
Three utilisation patterns were identified based on the criteria used in previous studies14 23 25 31:
Non-urgent access: defined by white or green triage codes and patient’s discharge as the outcome (including if the patient declined admission or left the ED before/during the medical examination).
Frequent users: youths with ≥4 accesses during 2012.
FNU users: children and adolescents who had ≥4 accesses, all ‘non-urgent’.
Return visits were defined as accesses that occurred within 72 hours of the first index visit. The following variables were evaluated to assess factors influencing the pattern of ED use: age, gender, nationality (Italian/other), residence (city and LHU), date and time span of attendance, type of referral, triage code, diagnosis, outcome (discharged/left the ED, hospital admission and other).
Visits occurring when the PCP is unavailable (ie, during the weekend or Monday–Friday from 20:00 to 08:00) were defined out-of-hours.
The average annual per capita income of the city of residence was derived from the Ministry of Economics’ website, and three classes were created using the distribution tertiles: low (<€18 200), average (€18 200–€20 261) and high (€20 622–€46 567).
The median number of paediatric patients cared for by one PCP was 905 for FPs and 71 for GPs.
Statistical analysis
Prevalence (number of youths with ≥1 access during the year divided by the total paediatric population) and number of accesses were estimated, and the distribution for the above variables was described.
Descriptive statistical analyses are reported as mean and SD or median and IQR. The area under the prevalence-time curve (AUC) from time 0 to 18 years (data plotted at the midtime interval) was calculated for males and females according to the linear trapezoidal rule.
To compare continuous variables, the t test and Kruskal Wallis tests were used, while χ2 test were performed to compare proportions.
Two multinomial logistic regression models with stepwise selection and level of significance α=0.05 were carried out. The first used non-urgent access as the dependent variable; age class (<1, 1–5, 6–11 and 12–17 years old), gender, nationality (Italian/other), LHU of residence, average income range of the city of residence (low/average/high) and ED structure of access, time of access (out-of-hours: yes/no), diagnosis (acute diseases, traumatic injuries, other) were used as the independent variables.
In the second model, being an FNU user (yes/no) was the dependent variable, and age class, gender, nationality, LHU of residence and average income were the independent variables.
Poisson regression was performed to evaluate the association between the above variables and the number of non-urgent accesses per subject.
Statistical analysis was performed using SAS V.9.4 software, and ARCMAP V.10.5 was used to create maps of prevalence on the basis of LHU of residence.
FNU users’ healthcare resource utilisation
A case–control study was also carried out to ascertain whether FNU attendees made a greater use of other healthcare resources as well.
Cases were defined according to the following criteria:
FNU use.
Age 1–5 years.
All accesses during 2012 occurred for diseases that could be managed almost exclusively by the FP. We therefore excluded cases of children attending the ED at least once for the following conditions that may justify an ED access: poisoning and injuries, abdominal pain, acute lymphadenitis, asthma, seizures, rotavirus gastroenteritis, influenza, laryngitis, nephritis and pneumonia. These criteria, adopted only for the case–control study, were applied with the aim to identify children with the highest likelihood of inappropriate ED use.
For each case, one child was randomly selected, matched by FP, age, gender and nationality (Italian/other). For both cases and controls, prevalence (percentage of children with at least one prescription/total number of cases or controls) and number of drug prescriptions, specialist visits, diagnostic tests and drug boxes were estimated.
Prevalence in cases and controls was compared by χ2 test, while the number of prescriptions was evaluated using the Wilcoxon test.
Results
ED utilisation of the paediatric population in Lombardy in 2012
During 2012, 440 284 children and adolescents <18 years (prevalence: 26.8%) had at least one ED attendance, for a total of 678 322 accesses. In all, 294 561 users (67%) attended ED once during the year.
The highest prevalence was observed in children aged 10–24 months, with a peak (46.7%) for 1-year-old children. Prevalence then decreased, with a statistically significant trend (p<0.001), reaching 22% in children and adolescents aged 7–17 years (figure 1A).

Prevalence of emergency department attendance in the paediatric population of the Lombardy Region by gender and age (A) and prevalence of frequent non-urgent use by age and gender (B).
The attendance rate was higher in boys than in girls for all ages, with an AUC0–18 male/female ratio of 1.2 and was higher in Italian, compared with foreign, children (relative risk (RR)=1.34; 95% CI 1.33 to 1.36), with similar trends by age and gender.
Slight differences in prevalence of access were observed among LHUs, ranging from 24.1% to 28.8%, as well as small differences by average income of city of residence (p=0.02).
Peak attendance occurred in winter and spring (each season accounted for 27% of total attendance), while summer had the lowest rate (20%). Moreover, 367 356 visits (54%) occurred out-of-hours.
Only 10 905 (2%) children were referred to the ED by a PCP, while 607 766 (89%) arrived following parental decision.
The triage code was green in 79.7% of the cases, white in 14.6%, yellow in 5.5% and red in 0.1%.
The most frequent diagnoses were traumatic injuries (26%), respiratory infections (22%) and gastrointestinal disorders (8%). Children >6 years old (33% of the cases) and adolescents (47%) attended the ED most frequently for traumatic injuries, infants (29%) and children aged 1–5 years (33%) for respiratory infections.
In all, 40 390 attendees (6%) were hospitalised after the ED visit. A total of 39 447 children and adolescents, 10% of those discharged after the index visit, had at least one return visit, 5736 (14%) of whom were admitted after it. The overall rate of hospital admission after ED attendance was 7% after pooling index and return visits.
A total of 533 037 (79%) accesses were ‘non-urgent’ and represented 84% of the attendees (368 156/440 284).
Only nationality was not associated (p=0.90) with non-urgent attendance in the multivariable analysis, while the most important independent determinants were: LHU of residence, attendance for an acute disease/symptom that could have been managed by PCPs (eg, upper respiratory tract infections, fever, nausea and vomiting) and age (table 1).
Results of multinomial logistic regression for non-urgent accesses and of Poisson regression analysis
FNU users
In all, 21 072 children were frequent users (5% of the ED attendees), 12 533 (59%) of whom accessed the ED for non-urgent reasons only. These subjects represented 0.8% of the paediatric population and 3% of the ED users and were responsible for 59 184 accesses (9% of total).
The increase in prevalence of FNU use starts at 7 months, and children aged 16–24 months have the highest prevalence (2.7%) (figure 1B). The access rate drops to 0.3%–0.4% for youths ≥6 years-old, with a statistically significant trend (p<0.001).
The prevalence of FNU use was higher in boys than in girls, with an AUC0–18 male/female ratio of 1.3, and was higher in Italian compared with foreign children (RR=1.87, 95% CI 1.71 to 2.06).
Differences in prevalence were observed among LHUs (range: 0.5%–1%), and children living in cities with an average/high income had a slightly higher prevalence of FNU use than children living in low income cities (0.8% vs 0.6%, p<0.001).
In all, 33 749 (57%) accesses attributable to FNU users occurred out-of-hours, and no statistically significant differences were found in the rate of FNU use based on the median number of children cared for by the PCP (p=0.17).
Respiratory infections were the most common diagnoses in FNU attendees (31.9%), in particular in children 1–5 years old (39.8% of accesses). Traumatic injuries were the second cause of attendance (15.6%) and accounted for 24.2% of visits in children 6–11 years old and 39.6% of adolescents’ accesses.
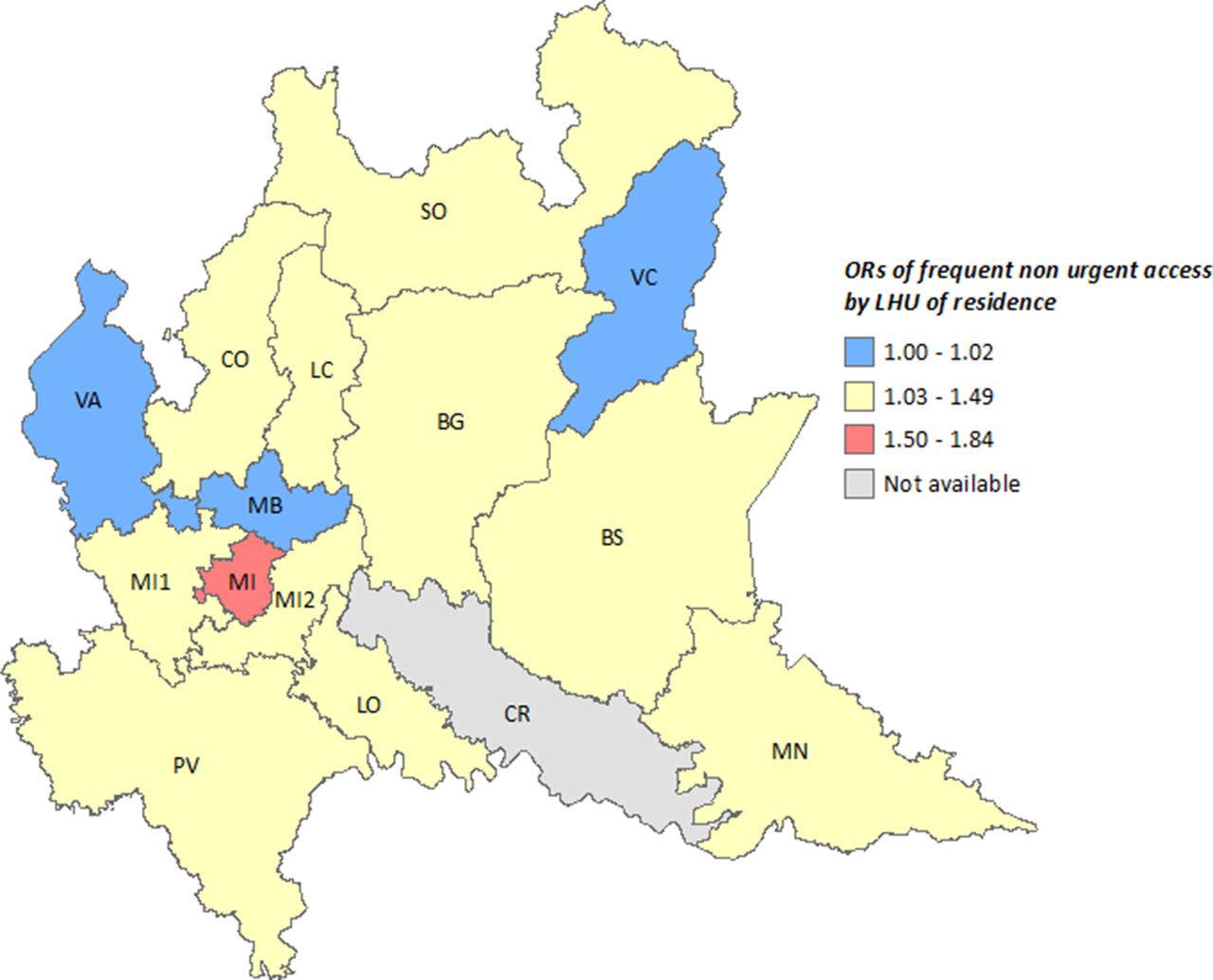
The logistic regression analysis (table 2) showed that nationality and average income of city of residence have no statistically significant relationship with being an FNU user, while independent risk factors were: age (1–5 years old: OR=3.14, 95% CI 2.98 to 3.31), male gender (OR=1.12, 95% CI 1.08 to 1.17) and LHU of residence, with Milan having the highest risk (OR 1.84, 95% CI 1.71 to 1.99) (figure 2). Similar findings were obtained when performing the Poisson regression model: preschool age (1–5 years old; incidence rate ratio (IRR) 1.21, 95% CI 1.21 to 1.22), LHU of residence (Milan, IRR 1.19, 95% CI 1.17 to 1.20) and male gender (IRR 1.01, 95% CI 1.01 to 1.02) resulted the variables associated with an increased IRR (table 1).
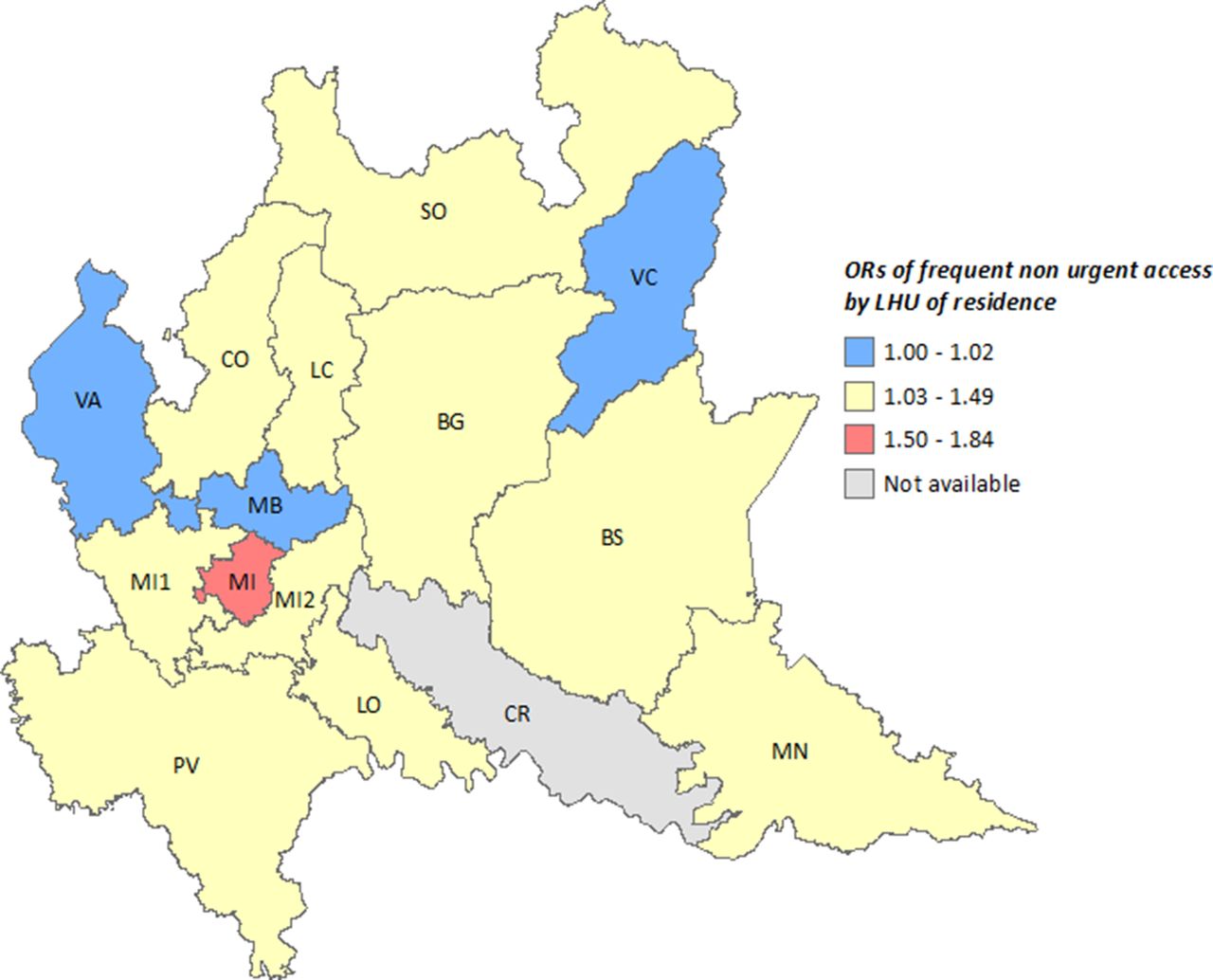
Distribution of ORs of frequent non-urgent access by local health unit (LHU) of residence. BG, Bergamo; BS, Brescia; CO, Como; CR, Cremona; LC, Lecco; LO, Lodi; MN, Mantova; MI, Milano; MI1, Milan 1; MI2, Milan-2; MB, Monza Brianza; SO, Sondrio; PV, Pavia; VA, Varese; VC, Vallecamonica.
Results of multinomial logistic regression for patients with frequent non-urgent accesses
Evaluation of healthcare resource utilisation by FNU users
A total of 3515 cases were identified, representing 2% of ED users and 0.7% of the population aged 1–5 years. Characteristics of this sample are summarised in table 3.
Healthcare resource consumption in cases and controls
The prevalence of prescriptions was significantly higher in cases compared with controls (figure 3), and the same was true for median number of drugs, specialist visits, diagnostic test prescriptions and drug boxes (table 3).

{kind=link}
{kind=link}
{kind=link}
Prevalence of healthcare resource prescriptions in cases and controls.
The median number of drug prescriptions and boxes remained higher in cases compared with controls, even after excluding prescriptions dispensed during the 7 days that followed an ED access (table 3).
Discussion
Our study showed that the overutilisation of the ED is a problem that affects the Lombardy Region and that is associated with a general overuse of healthcare resources in a small, but well-defined, group of ED users.
About one-fourth of the resident children and adolescents attended the ED at least once, a rate similar to that reported by Del Torso et al,33 and higher than the one reported in the USA,1 while the percentage of children with at least one return visit was five times higher than that previously reported in Italy.32 Moreover, the percentages of non-urgent visits and non-urgent users were higher than those observed in five LHUs in Veneto Region and in one ED in Crotone area, in the south of Italy,30 31 but similar to those reported in a multicentre study involving 10 Italian hospitals in eight different regions.35 Our study evaluated for the first time in Italy the prevalence of frequent users; the observed rate (1 out of 20 ED attendees) is consistent with findings from other countries.
The role of some contributing factors was confirmed: being male and being a preschooler is associated with a more frequent and more inappropriate ED use. This may be related to the high frequency of infections due to kindergarten attendance, and difficulties experienced by young children in communicating their symptoms may justify the mothers’ anxiety for non-urgent conditions such as fever (fever phobia).36
Infants, on the contrary, are at highest risk of urgent access, although it is difficult to distinguish if it is due to disease severity or to a more cautionary approach during the triage.
In our study, Italian children had a higher prevalence of ED access than foreigners, but nationality did not result as an independent risk factor for non-urgent attendance or FNU use. This finding is in contrast with international studies,14 37 while in Italy, the role of migrant status on ED use is not clear.35 38 39
The influence of socioeconomic status is controversial in international studies; it has been poorly analysed in Italy in the past and does not seem to be significant in our study.
Consistently with other studies,13 14 40 we observed a higher rate of FNU use in a metropolitan area, represented by Milan in the case of Lombardy Region, which is likely due to the high density of EDs. It is likely that parents of FNU users prefer to bypass the PCP. This can be deducted by the fact that (A) this pattern is not statistically associated with a higher number of children cared for by the FP/GP (a proxy of physician’s office overcrowding), (B) FNU users have an out-of-hours percentage of access not very different from the overall one and (C) the most frequent cause of FNU use is represented by respiratory tract infections, which also represent the most common reasons for PCP visits. Our study also demonstrates that the inappropriate use of the ED is associated with an increased consumption of other healthcare resources (drug prescriptions, specialist visits and diagnostic tests). The fact that differences in number of drug prescriptions in cases versus controls remained significant even after excluding those potentially attributable to the ED physicians (ie, occurring in the 7 days after the attendance) may indicate that the greater resource utilisation is not fully induced by ED. It is therefore likely that parental attitude can have a pivotal role.
Different types of strategies have been proposed to reduce the overburden of EDs: to introduce a fee for non-urgent visits not followed by admission, to homogeneously distribute PCPs’ offices, to extend their opening times, to intensify group or association paediatric practice models of work, to provide enhanced access, to plan educational interventions in order to help parents in recognising urgent conditions and to strengthen the relationship between the PCP and parents, but the evidence of effectiveness of these strategies appears scant and generally of low quality.9 20 40–44
Our findings support the hypothesis that the overuse of ED by the paediatric population may be due to a parental attitude towards a general overuse of healthcare resources. According to the results of our study, priority should therefore be given to educational interventions for parents aimed to increase the appropriateness of healthcare resource utilisation.
Strengths and limitations
This is the first Italian study that has been able to evaluate the rate and characteristics of ED access by the paediatric population living in an Italian region during an entire year. Furthermore, to the best of our knowledge, we have described, for the first time, a group of children with an inappropriate utilisation of the ED and a high consumption of other healthcare resources.
However, some limitations should be considered. We are not confident that our results can be generalised to the other regions, since Lombardy is characterised by low drug consumption, and regional differences exist in the drug prescription profiles and in ED organisation.45 46
Additionally, due to the limitations of administrative databases, we could not evaluate the role of some factors considered in previous studies, for example, family’s structure and socioeconomic status, mother’s marital status and literacy level, distance between the child’s house and the ED or the PCP’s office and the PCP of the child’s model of work (individual, network, group or associated paediatric practice).
In this regard, we tried to estimate the socioeconomic status using the data on the city of residence, but we are aware that our estimate may not be accurate.
Conclusions
Our study shows that there is an ED overuse in Lombardy: more than one out of four children and adolescents accessed ED during a 1-year period, and 1 out of 10 accesses were due to youths who were visited several times for non-urgent reasons only. Frequent use of the ED is partially associated with an inappropriate use of other healthcare resources. It is therefore necessary to adopt strategies to improve the appropriate use of health service resources in order to provide quality health solutions to real health needs.
References
Footnotes
Contributors All the authors contributed equally to the design of the study. BR was involved in planning the data analysis and wrote the first draft of the manuscript. AC contributed in planning the data analysis and in writing the manuscript. MC undertook the statistical analysis. AngB, IF and LM were involved in data collection and management. AC, AndB and MB supervised the study. All authors contributed to and have approved the final manuscript.
Funding The study was funded by the Lombardy Region (EPIFARM Project).
Competing interests None declared.
Patient consent Not required.
Provenance and peer review Not commissioned; externally peer reviewed.