Article Text

Abstract
Objectives To report on the quality of advance care planning (ACP) documents in use in residential aged care facilities (RACF) in areas of Victoria Australia prior to a systematic intervention; to report on the development and performance of an aged care specific Advance Care Plan template used during the intervention.
Design An audit of the quality of pre-existing documentation used to record resident treatment preferences and end-of-life wishes at participating RACFs; development and pilot of an aged care specific Advance Care Plan template; an audit of the completeness and quality of Advance Care Plans completed on the new template during a systematic ACP intervention.
Participants and setting 19 selected RACFs (managed by 12 aged care organisations) in metropolitan and regional areas of Victoria.
Results Documentation in use at facilities prior to the ACP intervention most commonly recorded preferences regarding hospital transfer, life prolonging treatment and personal/cultural/religious wishes. However, 7 of 12 document sets failed to adequately and clearly specify the resident's preferences as regards life prolonging medical treatment. The newly developed aged care specific Advance Care Plan template was met with approval by participating RACFs. Of 203 Advance Care Plans completed on the template throughout the project period, 49% included the appointment of a Medical Enduring Power of Attorney. Requests concerning medical treatment were specified in almost all completed documents (97%), with 73% nominating the option of refusal of life-prolonging treatment. Over 90% of plans included information concerning residents’ values and beliefs, and future health situations that the resident would find to be unacceptable were specified in 78% of completed plans.
Conclusions Standardised procedures and documentation are needed to improve the quality of processes, documents and outcomes of ACP in the residential aged care sector.
- End-of-life
- Terminal Care
- Advance Care Planning
- Advance Directives
- Nursing Homes
- Aged Care
This is an open-access article distributed under the terms of the Creative Commons Attribution Non-commercial License, which permits use, distribution, and reproduction in any medium, provided the original work is properly cited, the use is non commercial and is otherwise in compliance with the license. See: http://creativecommons.org/licenses/by-nc/3.0/ and http://creativecommons.org/licenses/by-nc/3.0/legalcode
Statistics from Altmetric.com
It is well recognised that having a documented and accessible Advance Care Plan developed as part of a systematic approach to advance care planning (ACP) offers individuals some level of control over their end-of-life healthcare options, and can potentially provide improved quality of life during this final stage.1–6 However, ACP documentation in use across different healthcare settings and jurisdictions often varies in format and content, resulting in recommendations for national document standardisation.7–9 In addition, there are a range of barriers that can hamper the completion and availability of Advance Care Plans, thus limiting the likelihood that an individual's wishes will be followed at end-of-life.
These barriers can occur at any stage of the Advance Care Plan, from its development through to the moment that end-of-life medical treatment decisions are being made. Individuals and/or family members may be unwilling to discuss options for future treatment and receive no direction about the appropriateness and importance of such discussions from healthcare providers.10 ,11 In crucial periods, when an individual's deteriorating health may require life-prolonging treatments, medical practitioners may not have access to details of the individual's Advance Care Plan12 or may choose to make medical decisions based on their own views or on standard protocols.13 ,14 There are also various procedures that need to operate effectively to ensure that the individual's preferences are expressed accurately and clearly, are up-to-date, can be located easily and quickly, and are likely to be interpreted appropriately and consistently by key staff within and across the health spectrum.5 ,15–22
The importance of having Advance Care Plans that are easily accessible and interpretable by staff not involved in their original preparation is crucial whether in the hospital or in a residential aged care facility. These issues have received some attention in Australia and elsewhere.23 For example, some researchers have noted that medical practitioners and other health professionals outside the original setting may find the preferences or advance directives difficult to interpret.24 Documentation may be inconsistently worded and can be located in different sets of records, for example, patient medical records or separate ACP-specific forms stored with administrative files.7 ,25 ,26
In Victoria, Australia in 2009, under the umbrella of the federally funded Respecting Patient Choices (RPC) programme, a working party was established to develop an Advance Care Plan template for use in residential aged care facilities (RACFs) that were participating in the Making Health Choices (MHC) project. The goal of the MHC project was to develop, trial and evaluate a sustainable system for implementing effective ACP in RACFs throughout Australia. The preimplementation state of ACP in these trial sites has been described previously.27
This paper reports on the principles used to guide the development of the aged care specific Advance Care Plan template, the preimplementation quality of ACP documents and the performance of the newly developed Advance Care Plan template.
Methods
Membership of the Working Party comprised industry experts in aged and palliative care, academics and RPC staff involved in the MHC project. An important outcome of this working party's deliberations was a set of guiding principles for conducting ACP in the aged care setting (see table 1).
Principles for Advance Care Planning
Details of the MHC project and the RACFs involved in this project have been described.27 A total of 19 RACFs, representing 12 aged care organisations, participated in the project. This number included facilities based in rural or metropolitan locations with bed numbers ranging from under 50 to over 100, all of which provided high-level care (care for residents who may have complex healthcare needs and/or who may require increased support for activities of daily living and/or behavioural management), either as the majority of care provided (high-care only facilities), in a separate unit alongside a low care unit (low and high care) or as part of an aging-in-place facility (high care provided in situ as residents’ needs increase).27
Preimplementation ACP documentation
Participating RACFs provided copies of existing documentation used to record resident treatment preferences and end-of-life wishes prior to the MHC project. This documentation was then assessed by two raters for the presence and quality of information according to the nine key domains referred to in table 1, item 17. Since the small sample size precluded statistical examination of inter-rater reliability, differences between raters in their assessments of these documents were resolved by reviewing items against these criteria until concordance was reached.
Development of recommended aged care specific Advance Care Plan template
The recommended template was developed by the working party based on the guidelines (table 1) and piloted at two RACFs that were not participating in the MHC project. Those testing the form (lifestyle coordinators, registered nurses and relatives, and one general practitioner) answered six questions regarding the clarity and usability of the form (see online supplementary table S1 for questions and responses).
Audit of Advance Care Plans completed on the recommended template
After commencement of the MHC programme, participating RACFs were also asked to provide de-identified actual examples of Advance Care Plans they had completed at their facility using the recommended template. These plans were completed by participating staff during ACP discussions with RACF residents and/or their family members (if the resident was not competent) over the course of the MHC project. ACP discussions would assist the resident to consider their current health state, their current goals, values and beliefs and their future preferences regarding health care if they should become seriously unwell. The staff would assist the resident/family to complete the plan in their own words. It would then be signed by the competent resident or the nominated family member of the resident who had lost capacity, and witnessed by the staff member, the general practitioner or a family member. If appropriate, the staff member would also assist the resident to appoint a substitute decision maker. The completeness and quality of all sections of submitted Advance Care Plans was assessed by a single rater. The reliability of ratings was assessed by applying κ statistics to assessments made on 30 cases by an independent second rater. Inter-rater agreement was acceptable for all relevant items, ranging from κ 0.73–0.79.
Results
Pre-existing ACP documentation
All 12 aged care organisations provided preimplementation documents (representing documents in use at all 19 participating RACFs), with the use of 14 different titles. Some RACFs used two separate documents, however, the purpose of each document was not always clear from the title given (see table 2). Table 3 provides details of the number of organisations with documentation adequately covering each of the nine key domains identified in table 1, item 17. None of the organisations used document sets that covered all of these key domains. Only a third of the organisations had developed documentation that clearly provided details of an individual who had been given Medical Enduring Power of Attorney (MEPOA), and specification of the resident's competency status was included in only a quarter of the document sets. Documentation most commonly recorded preferences regarding hospital transfer, life prolonging treatment and personal/cultural/religious wishes. However, the recording of preferences around life-prolonging treatment was judged inadequate in the majority of document sets. Reasons for a rating of inadequate included: (1) cases where documents referred to CPR preferences only (four documentation sets); (2) where documents did not ask for specific treatment preferences but had questions that were phrased in a way that may elicit non-specific responses for example, ‘do you or your family have any concerns regarding the prolonging of life by artificial means?’ (two document sets); (3) where documents asked for confirmation that resuscitation and palliative care issues had been ‘explained to the resident/family’, and do not elicit specific treatment preferences (one document set). In the case of preferences around hospital transfer, one set was rated inadequate because residents were only asked to indicate a yes/no response to the statement ‘only to be transferred to hospital if absolutely necessary’ (the term ‘absolutely necessary’ gives no practical guidance to the nurse who must make the decision about what to do). Items recording information regarding personal/cultural/religious wishes were assessed as inadequate in three of the documentation sets for the following reasons: (1) Residents were only asked if they would like a minister to be contacted; (2) Residents were only asked if they had any cultural wishes relating to death and if they would require the notification of a religious minister in specified situations; (3) Residents were only asked if they had any religious/spiritual wishes.
Names of advance care planning related document sets reported by aged care organisations
Completeness and quality of existing documentation sets used by participant aged care organisations to record resident treatment preferences/wishes for end of life care
Testing of the draft recommended Advance Care Plan template
Staff who trialled the draft recommended Advance Care Plan template provided positive responses to all six assessment questions, noting that it was much simpler to use than their existing documentation, and suitable for use with competent and non-competent residents. Furthermore, testers noted that the template provided a clear guide during ACP discussions. As a result of the positive feedback, the draft template format was used for the MHC project.
Completed Advance Care Plans using the recommended template
A total of 244 completed care plans were provided by 16 separate facilities (representing 10/12 participating aged care organisations) with a total of 1074 beds. Forty-one of these plans were excluded from the audit because they were provided by facilities that were part of the same umbrella organisation that chose to continue to use their preimplementation ACP documentation (reports from this organisation indicated that recent Board ratification of existing documentation precluded the use of the newly developed Advance Care Plan template in these facilities). This left 203 Advance Care Plans completed on the recommended template that were provided by 13 different RACFs to be included in this audit.
Of 203 plans, 49% included the appointment of a MEPOA with completed contact details, while 40% of plans indicated that no MEPOA had been appointed for the resident in question. Overall requests concerning medical treatment were specified in almost all completed documents (97%), with 73% nominating the option of refusal of life-prolonging treatment. Twelve per cent preferred the doctors to make medical treatment decisions in keeping with the resident's expressed preferences, while only 6% selected transfer to hospital for treatment and assessment as their preferred choice.
Nearly all plans (99%i) also had information listed in the ‘wanted/not wanted treatments’ section of the form. Treatments listed as wanted and those listed as not wanted were judged to be consistent in 96% of submitted plans where this rating was possible. Of the seven plans receiving an inconsistency rating for this item; five made inconsistent requests around CPR for example, ‘wanted-CPR, not wanted—ventilation’; and two made inconsistent requests relating to surgery for example, ‘wanted—surgery to clear bowel obstruction, not wanted—IVs’. The information in this section was assessed to be consistent with selections made in the overall medical treatment request section of the form in 98% of cases. All four plans that received an inconsistency rating indicated tick box 1 (refusal of life prolonging treatment selected) and yet requested CPR in the wanted treatment list (in two cases the request for CPR was specifically in the context of a witnessed arrest only).
Examples of values and belief statements given in completed Aged Care Plans
▸ My children, grandchildren and great-grandchildren
▸ Strong family ties, independence is highly important
▸ Maintain independence and social interactions. No specific religion
▸ Family and friends. Soft music playing during the day. Sitting in the garden on nice warm days. Church (catholic) communion, blessing of the sick
▸ Family. Independence, going visiting places, being among people
▸ Family, religious beliefs, independence and privacy. Favourite football club
▸ Family, reading, knitting, keeping her mind active. Has her own spiritual beliefs and does not wish to be visited by clerics. Independence important but is seriously decreasing
▸ Family very important. To be treated with dignity by being kept clean and comfortable. Also having adequate pain management. Music especially opera CDs
▸ Likes limited company, likes own space. Family
▸ Strong family affiliation. Practising Roman Catholic. Enjoys bingo, pokies, magazines, jigsaws and pets, particularly the family dog
▸ Independence.
Over 90% of plans included information concerning residents’ values and beliefs (see box 1). Major themes drawn from these values included: family, independence, faith and spiritual beliefs. Future health situations that the resident would find to be unacceptable were specified in 78% of completed plans, examples of which are given in box 2. The resident's current health status was completed in 93% of plans although the information provided frequently appeared to be the staff's knowledge of the resident's health status (71%) rather than residents’ or families interpretation of their current health. Finally, 93% of plans had been signed by a competent resident or on behalf of a non-competent resident with 86% of these plans assessed as having all sections signed and witnessed correctly.
Examples of resident/family statements regarding unacceptable future health situations
▸ Can't walk, can't talk, can't eat
▸ Feeding/breathing tubes, needing assistance to go to the toilet, loss of any more independence
▸ Poor quality of life, unable to get around, unable to communicate
▸ Current health status is unacceptable
▸ Unable to communicate, would find pain that was not managed unacceptable
▸ Having to live a poor quality of life, not able to eat/drink, loss of dignity
▸ Unable to communicate, feed myself, comprehend surroundings
▸ Being kept alive when there is no hope of recovery
▸ Bed bound, unable to move or communicate or lead any sort of meaningful existence
▸ Prolonging my life no matter what, machines keeping me alive
▸ If I can't swallow on my own, to receive percutaneous endoscopic gastronomy feeding
▸ Current condition unacceptable
▸ Unable to tell my family that I love them all
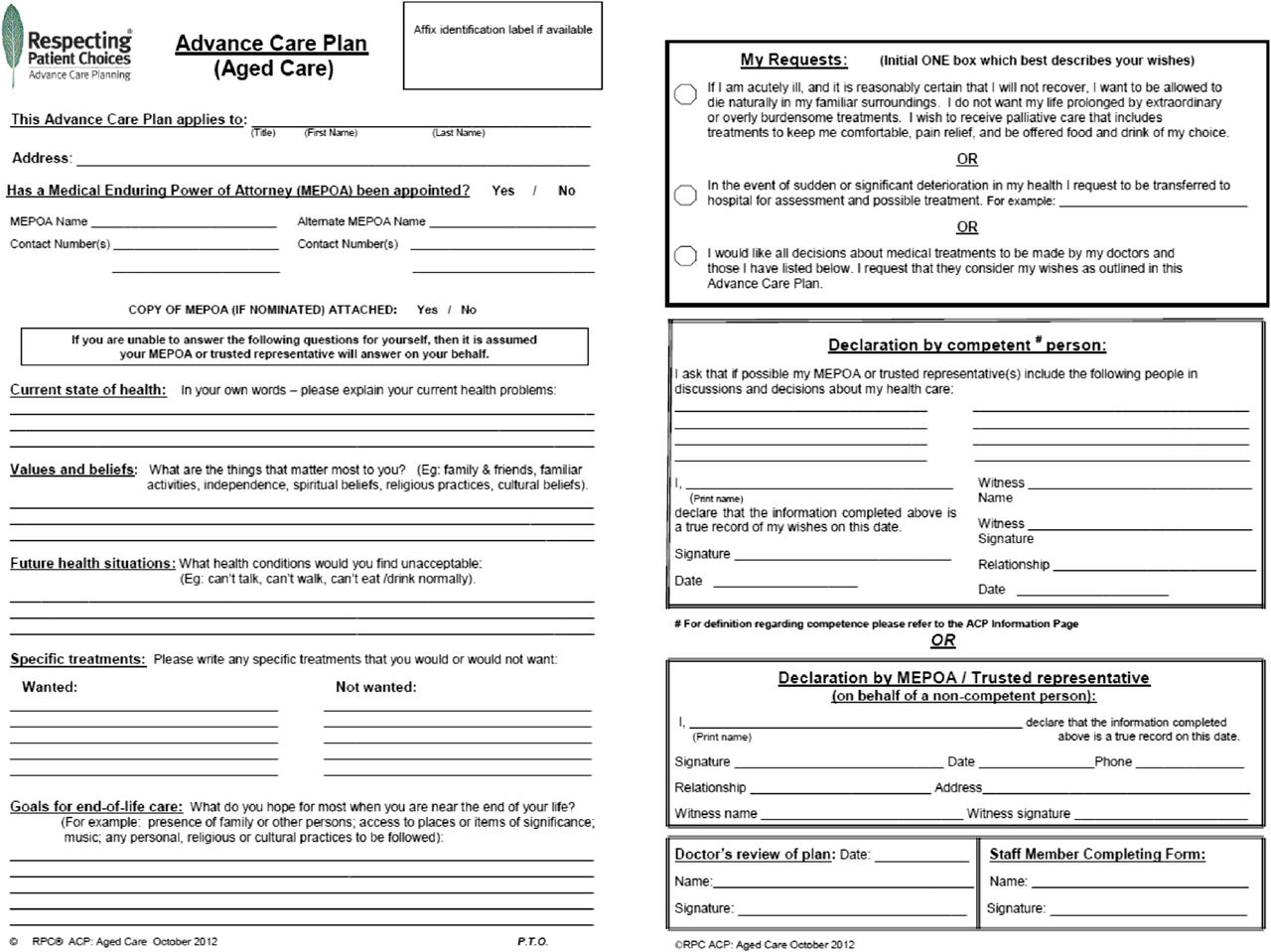
Following further feedback from participants using the template during the project period, a final version of the RPC Advance Care Plan template was developed. This template is provided in figure 1.
{kind=link}
Aged care specific Advance Care Plan.
Discussion
This paper describes the process of developing, piloting and wider testing of an effective Advance Care Plan template for use in RACFs. It details the limitations with documentation used in participating RACFs prior to implementation. It identifies key principles for ACP, major domains of information that should be covered in an effective Advance Care Plan and reports on the results of 203 Advance Care Plans completed using the recommended template in 13 separate facilities.
In line with previous research in this area,7 the existing document sets used by the participating organisations had a number of serious limitations, beginning with the variability in their titles and structures. Given the mobility of the aged care workforce,28 it would be important to have consistency in the naming and layout of these ACP documents to ensure new staff can identify and work with them easily. It is also notable that a majority of document sets used by these organisations failed to include key components of a workable Advance Care Plan. These included: MEPOA status and details; whether the resident was competent at the time of completion; and information concerning the resident's end-of-life values and important wishes. Without this information it is difficult to see how the resident's wishes could be effectively enacted. Seven of the 12 documents also failed to adequately and clearly specify the resident's preferences as regards life-prolonging medical treatment. It was also disappointing how frequently the most common questions in the pre-existing documents were regarding funeral arrangements and the resident's desire to be transferred to hospital.
The development of the guiding principles for ACP by the expert working group served to ensure that the new Advance Care Plan template contained all the essential elements and guided the objective assessment of old and new documents. The new document template was met with broad approval and its ease-of-use was confirmed by the high standard of completion. Completion of Advance Care Plans, by RACF staff using the recommended template as part of the MHC project, was clearer and more thorough with the inclusion of fields such as personal values and unacceptable future health situations. It is notable that fewer than half of these completed Advance Care Plans specified a MEPOA including complete contact details. Many residents, however, may have lacked the capacity to appoint a MEPOA by the time ACP was conducted. The addition of information on residents’ values and priorities, and unacceptable health situations is in line with recent studies regarding effective ACP29 ,30 and makes it more likely that attention, care and resources that are given to residents in their last stage of life will be comforting and acceptable.
The main limitation of this study is the relatively small number of RACFs from which this data was gathered. This limitation is offset by the consistency of the findings regarding the inadequacy of preimplementation documents and the high performance of the Advance Care Plan template.
A major conclusion to draw from this assessment is that standardisation of ACP processes and documentation is likely to improve the quality and ultimately the outcomes of ACP in the residential aged care sector. The guiding principles for ACP in aged care and the use of the template presented in this paper, should assist RACFs and their staff to increase the frequency and quality of completion of Advance Care Plans in the residential aged care setting. Completion and revision of clear comprehensive ACP documents are essential components of this process.
Acknowledgments
We would like to thank all participating aged care organisations and associated residential aged care facilities and staff.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online table
Footnotes
-
Licence for publication The Corresponding Author has the right to grant on behalf of all authors and does grant on behalf of all authors, an exclusive licence (or non exclusive for government employees) on a worldwide basis to the BMJ Publishing Group Ltd to permit this article (if accepted) to be published in BMJ Supportive and Palliative Care and any other BMJPGL products and sublicences such use and exploit all subsidiary rights, as set out in our licence (http://group.bmj.com/products/journals/instructions-for-authors/licence-forms).
-
Contributors WS: Study lead, study design, contribution to the first draft and subsequent manuscript revisions, and final approval of the version to be published. RAP: Data analysis, formulated the first draft of the manuscript, final approval of the version to be published. VJL: Study design, contribution to the first draft and subsequent manuscript revisions, and final approval of the version to be published. RSF: Data collection, data analysis, contribution to the first draft and subsequent manuscript revisions, and final approval of the version to be published. RS: Study design, data collection, contribution to manuscript revisions and final approval of the version to be published. LJ: Study design, data collection, contribution to manuscript revisions and final approval of the version to be published. VW: Study design, data collection, contribution to manuscript revisions and final approval of the version to be published. RH: Study design, contribution to manuscript revisions and final approval of the version to be published.
-
Correction notice This article has been corrected since it was published Online First. The e-mail address in the ‘Correspondence to’ section has been changed from ‘rachael.fullam@austin.org.au’ to ‘william.SILVESTER@austin.org.au’.
-
Funding Australian Government Department of Health and Ageing.
-
Competing interests None.
-
Ethics approval La Trobe University Human Research Ethics Committee.
-
Provenance and peer review Not commissioned; externally peer reviewed.
-
Open Access This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 3.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/3.0/
-
↵i Percentage calculated excluding plans (n=4) where a rating was not possible due to incomplete copies of the plan.