Article Text

Abstract
Background: Based on equivocal clinical data, intravenous antioxidant therapy has been used for the treatment of severe acute pancreatitis. To date there is no randomised comparison of this therapy in severe acute pancreatitis.
Methods: We conducted a randomised, double blind, placebo controlled trial of intravenous antioxidant (n-acetylcysteine, selenium, vitamin C) therapy in patients with predicted severe acute pancreatitis. Forty-three patients were enrolled from three hospitals in the Manchester (UK) area over the period June 2001 to November 2004. Randomisation stratified for APACHE-II score and hospital site, and delivered groups that were similar at baseline.
Results: Relative serum levels of antioxidants rose while markers of oxidative stress fell in the active treatment group during the course of the trial. However, at 7 days, there was no statistically significant difference in the primary end point, organ dysfunction (antioxidant vs placebo: 32% vs 17%, p = 0.33) or any secondary end point of organ dysfunction or patient outcome.
Conclusions: This study provides no evidence to justify continued use of n-acetylcysteine, selenium, vitamin C based antioxidant therapy in severe acute pancreatitis. In the context of any future trial design, careful consideration must be given to the risks raised by the greater trend towards adverse outcome in patients in the treatment arm of this study.
- CRFs, case report forms
- ERC, endoscopic retrograde cholangiography
- GSH, glutathione
- GSSG, glutathione disulphide
- HDU, high dependency unit
- HO-1, haem oxygenase
- IQR, interquartile range
- ITU, intensive care unit
- LODS, logistic organ dysfunction score
- MODS, Marshall organ dysfunction score
- MT-1, metallothionein
- pancreatitis
- antioxidants
- randomised controlled trial
Statistics from Altmetric.com
- CRFs, case report forms
- ERC, endoscopic retrograde cholangiography
- GSH, glutathione
- GSSG, glutathione disulphide
- HDU, high dependency unit
- HO-1, haem oxygenase
- IQR, interquartile range
- ITU, intensive care unit
- LODS, logistic organ dysfunction score
- MODS, Marshall organ dysfunction score
- MT-1, metallothionein
Oxidative stress caused by short lived intracellular oxygen-free radicals is one of the mediators of acinar injury in acute pancreatitis.1 Disruption of the balance between endogenous oxygen-free radical scavenger pathways and mechanisms for generation of these free radicals has been postulated to occur in acute pancreatitis.1 In experimental and in clinical acute pancreatitis there is evidence of depletion of circulating antioxidant levels2,3 with the degree of depletion corresponding to disease severity.4 There is corresponding accumulation of byproducts of oxidative stress pathways.4 In addition, there is corroborative evidence of increased expression of the oxidative stress response genes c-fos, haem oxygenase (HO-1) and metallothionein (MT-1) in experimental acute pancreatitis.5,6
Evidence that oxygen-free radical species are mediators of pancreatic injury was provided by Rau and colleagues in a rat model of taurocholate induced experimental acute pancreatitis.7 They demonstrated changes in pancreatic tissue concentrations of reduced glutathione, paralleled by raised levels of oxidised glutathione and malondialdehyde within 5 minutes of induction of acute pancreatitis. This study also demonstrated that although pretreatment with the free radical scavenger superoxide dismutase prevented the fall in glutathione and ameliorated pancreatic injury, intravenous infusion of xanthine oxidase as an oxidative stress generator failed to trigger acute pancreatitis despite reproducing the fall in pancreatic glutathione seen in experimental acute pancreatitis. These findings suggest that oxygen-free radical species are important mediators but not necessarily triggers of tissue damage in acute pancreatitis.
Inl-arginine induced experimental acute pancreatitis in a rat model, addition of intravenous antioxidants in the form of combined n-acetylcysteine, selenium and ascorbic acid, with the intervention given 12 hours after induction of pancreatitis resulted in amelioration in pancreatic and remote organ injury.8
In contrast to this work, there is no substantive clinical evidence that antioxidant supplementation is of benefit in human acute pancreatitis. Wollschlager and colleagues demonstrated that selenium supplementation in patients with acute pancreatitis was associated with lower serum levels of malondialdehyde.9 There were insufficient patients in this study to make more definitive conclusions. Kuklinski’s non-randomised series demonstrated a reduction in mortality from acute pancreatitis from 34% to 1.1% coincident with the introduction of selenium into the treatment protocol in his unit.10,11 These dramatic findings have never been reproduced. Based on these findings, Braganza and colleagues introduced a policy of treating severe acute pancreatitis with intravenous antioxidant therapy using a combination of n-acetylcysteine, selenium and ascorbic acid. Although we reported outcome in these patients using case-control methodology to calculate observed:expected (O:E) mortality ratios, considerable heterogeneity in data precluded any meaningful conclusion.12 Braganza and colleagues had earlier reported the results of their own randomised trial but a small study population (20 patients) included no patients with severe acute pancreatitis.13
Thus more than 25 years after the first reports of benefit from antioxidant therapy in clinical acute pancreatitis this treatment remains unvalidated in severe acute pancreatitis and the aim of this study was to conduct a randomised, double blind, placebo controlled trial of combination antioxidant therapy in severe acute pancreatitis using contemporary disease categorisation terminology and incorporating stratification for severity of organ dysfunction.
METHODS
Study design
We conducted a randomised double blind placebo controlled trial of intravenous antioxidant therapy in patients with predicted severe acute pancreatitis.
Study setting
The study was carried out at three university hospitals in north western England: the Manchester Royal Infirmary, Hope Hospital, Salford and Wythenshawe Hospital, Manchester.
Inclusion/exclusion criteria
Patients were included whose clinical and biochemical presentation was consistent with acute pancreatitis (specifically, a history of acute abdominal pain associated with a greater than threefold elevation of the serum amylase and/or computed tomographic evidence of acute pancreatitis); with predicted severe acute pancreatitis defined for the purposes of this study as an APACHE II score of 8 or more either at admission or within 48 hours of admission (an APACHE II score of 8 or more has an overall sensitivity of 63% and a specificity of 81% for the prediction of severe attacks when calculated on admission).14 Inclusion criteria stipulated that patients be enrolled within 72 hours of admission to hospital and that they be 16 years of age or over, not currently enrolled in another trial, without a history of allergy to intravenous antioxidant therapy and able to give written informed consent (consent from patients in a critical care unit setting was obtained from the next of kin). Patients were excluded if we were unable to obtain informed consent; more than 72 hours had elapsed since admission to hospital; they were under 16 years of age; or if they had previously enrolled in the trial with a previous episode of acute pancreatitis.
Power calculations and stopping rules
From audit records, organ dysfunction at 7 days was expected to be present in 75% of patients with severe acute pancreatitis. A study powered (at 80% power and alpha 5%) to detect a relative risk reduction of organ damage of 33%, or an absolute risk of 50% in the intervention group, required 67 patients in each arm when applying Fisher’s exact test.
Consistent with the need to ensure appropriate treatment and the safety of patients, early termination of the trial was prespecified on three grounds: failure of administration or conduct; new evidence about the care of this patient group making it unnecessary or unethical to continue; or a data dependent stopping condition being met. These stopping conditions included under-enrolment or treatment effect exceeding acceptable bounds for continuation (a two sided p value for the primary end point was estimated at each annual interim analysis and compared with the value generated by an alpha spending function algorithm).
Randomisation schedule
The pharmacy department of Central Manchester Healthcare (Manchester Royal Infirmary) was provided with a randomisation schedule utilising variable length even number blocks. Treatment allocation was stratified according to treating hospital and APACHE II score (low ⩽15; high >15). The pharmacy administered the randomisation and storage of therapeutics for all participating centres.
Intervention group patients received maximal conventional therapy plus intravenous antioxidant therapy for 7 days. Placebo group patients received maximal conventional therapy plus intravenous placebo for 7 days. If patients in either group required intravenous fluids for less than 7 days, then active or placebo treatment was stopped upon cessation of intravenous fluid replacement.
Blinding
Treatment (active or visually identical placebo) packs were provided by the pharmacy on receipt of valid documentation from enrolling clinicians. The pharmacy was responsible for ensuring concealment of allocation and maintaining blinding of physicians and patients to active therapy. On request, the pharmacy passed to the remote site statistician (JM) the randomisation schedule which identified enrolled patients by their unique patient number. On request, the lead investigator (who remained blind to treatment allocation until after recruitment and analysis had been completed) passed enrolled patient data in electronic form, identifiable only by patient number. The statistician conducted interim and final analyses using these anonymised patient data.
End points
The principal end point was presence of organ dysfunction at day 7 using last observation carried forward (that is, if the day 7 datum was missing, the last previous value was carried forward). Presence of organ dysfunction was determined as a score of one or more using the Marshall organ dysfunction score (MODS).15 Secondary clinical end points included APACHE-II, MODS, logistic organ dysfunction score (LODS),16 laboratory markers of antioxidant depletion and oxidative stress (serum ascorbic acid, serum selenium, the ratio of reduced glutathione (GSH) to glutathione disulphide (GSSG)—GSH/GSSG ratio and serum C reactive protein), death (assessed at end of day 7 and at 3 months), days in intensive care, high dependency care and general wards.
Standards of clinical care for severe acute pancreatitis
Maximal conventional therapy was as defined according to the British Society of Gastroenterology guidelines,17 which represented UK standard of care during the period of recruitment and comprised fluid resuscitation, supplemental oxygen therapy, monitoring of vital signs (level of invasiveness and use of critical care facilities at the discretion of individual clinician or unit) and early endoscopic retrograde cholangiography (ERC) for severe acute biliary pancreatitis (selection criteria at individual clinician’s discretion). Prophylactic antibiotics were used at the discretion of the treating clinician. Patients were followed up until discharge from hospital (or death). In order to detect clinical events occurring after discharge from hospital, patients were sent a questionnaire at 6 weeks from time of disease onset to ascertain re-admission and ongoing disease related problems. All disease descriptors were compliant with the terminology of the 1992 Atlanta consensus conference.18
Drug composition and delivery schedules
Antioxidant therapy or placebo was administered via an infusion device. The active regimen is shown in table 1. The active drugs or placebo were made up under sterile conditions in syringes labelled “antioxidant trial” and identified by enrolment number. N-acetylcysteine, selenium and ascorbic acid were made up in separate syringes and administered by infusion driver. Drug or placebo was administered either via peripheral intravenous infusion or via central line at the discretion of the patient’s attending clinician.
Intravenous antioxidant regimen: protocol for use of selenium, ascorbic acid and n-acetycysteine
Measurement of antioxidant levels
Serum antioxidant levels were routinely monitored in an appropriately accredited hospital laboratory: if levels exceeded the upper limit of currently validated ranges during the course of infusion, therapy was stopped. Such patients were not excluded from the analysis.
Data record and statistical analyses
Data were recorded prospectively using case report forms (CRFs) for all patients participating in the trial, including patient demographics, disease course, treatment, outcome and adverse effects. All analysis was conducted by intention to treat. Comparison of binary end points was by Fisher’s exact test; continuous interval data were by unmatched two sample Student t test; and organ dysfunction scores was by the Mann-Whitney U test. Post hoc subgroup and regression analyses were conducted to explore determinants of organ dysfunction for the purposes of hypothesis generation.
Ethics committee approval
The full study protocol was approved by the Central Manchester local research ethics committee (approval number 02/CM/377) and also by the research and development department of the Manchester Royal Infirmary.
RESULTS
Patients were enrolled between June 2001 and November 2004, at which point the trial was terminated after interim analysis revealed that all deaths were in the treatment group. Although deaths were not clearly attributable to intervention and the difference was not statistically significant, the risk of demonstrating harm precluded further recruitment. A CONSORT flow chart recording progression through the trial is shown in figure 1 and a completed CONSORT checklist is provided in the appendix (see Gut website, www.gut.bmj.com/supplemental). Groups were comparable at baseline at conventional levels of statistical significance (table 2). There was a trend towards placebo patients being older although the importance of this is unclear. One outlying patient (aged 20) enrolled to intravenous antioxidant accounts for about half of the baseline difference in age. Comparing groups the amount of intravenous treatment received was similar.
Trial participant characteristics and intravenous treatment received
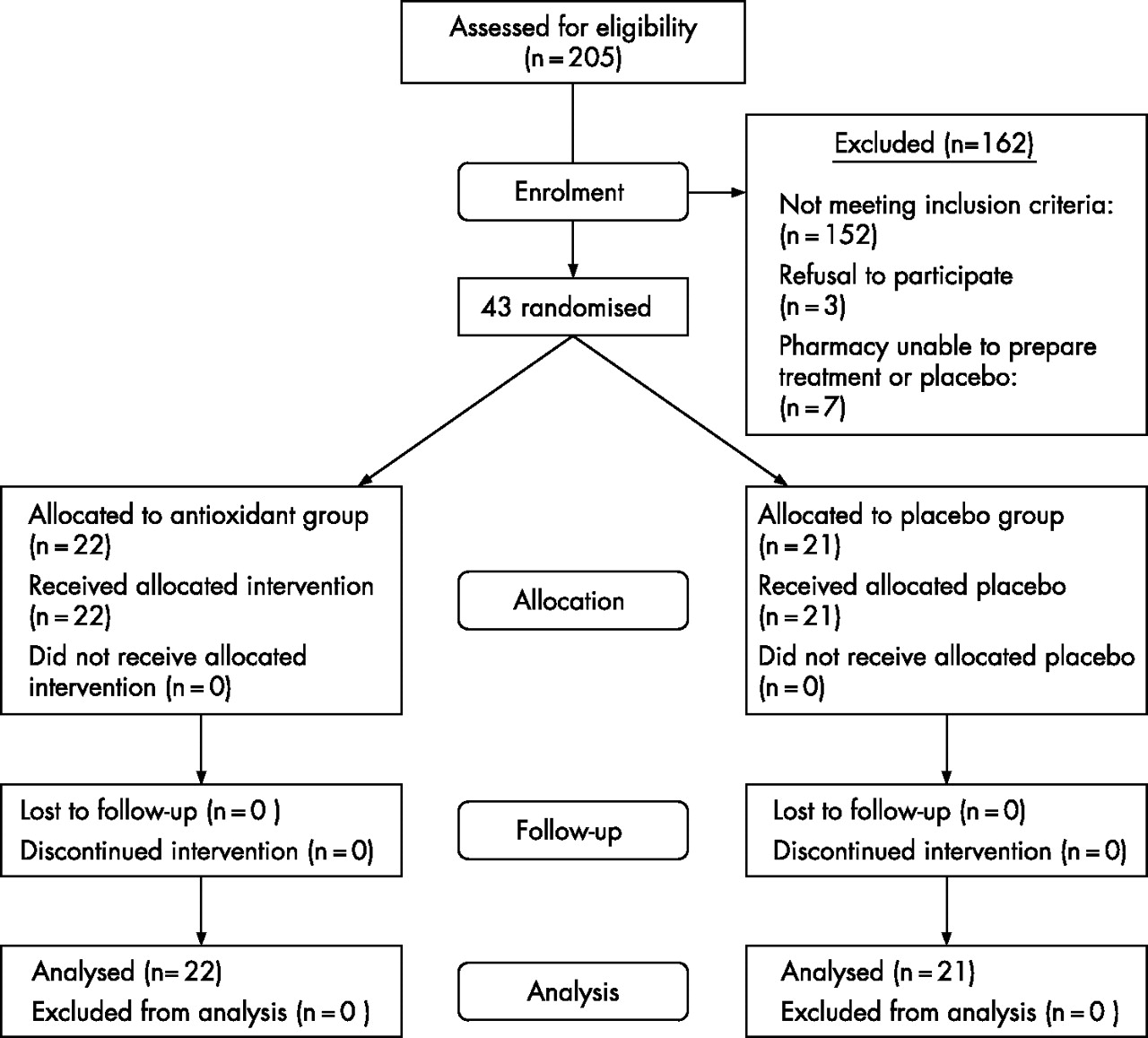
CONSORT flow chart of progression through trial.
Principal end points
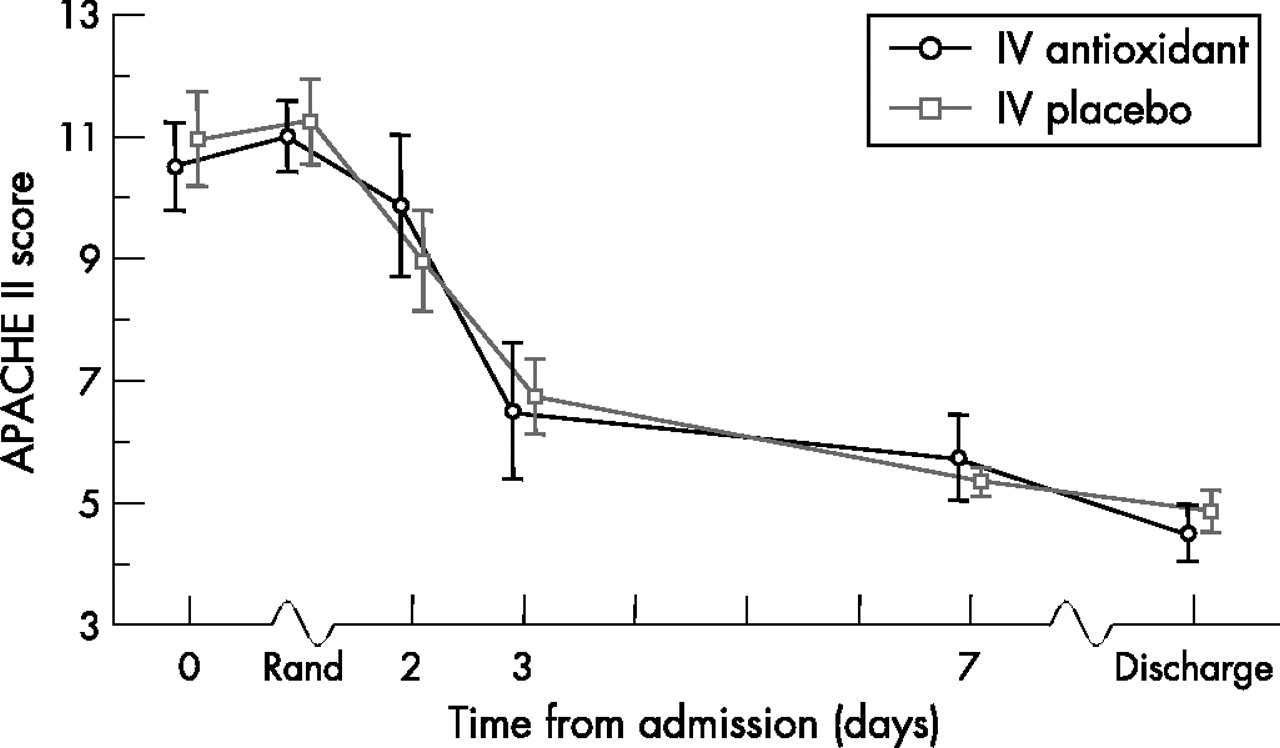
The primary end point, presence of organ dysfunction at 7 days, was statistically similar comparing antioxidant and placebo groups (32% vs 19%, difference 13%, 95% CI: −13% to 39%, p = 0.33) (table 3). Analysis of MODS at day 7 revealed a trend towards more multiple organ dysfunction in patients on active treatment than on placebo (difference at 7 days, p = 0.093 (fig 2). This difference was not apparent at baseline and it is unclear whether it is a chance finding or attributable to the antioxidant therapy itself. Analysis of APACHE-II scores revealed no difference between active and placebo therapy over the first 7 days of treatment (fig 3).
Trial findings

Distribution of MODS (Marshall organ dysfunction score) values. LOCF, last observation carried forward.

{kind=link}
{kind=link}
{kind=link}
APACHE II score from admission to discharge.
There was a trend towards higher use intensive and high dependency care in the active treatment group correlated with greater organ dysfunction in individual patients (table 3). This finding was mirrored in the higher number of deaths in the antioxidant group (4 vs 0)
Laboratory markers
Relative to the placebo group, active group antioxidant levels rose while markers of oxidative stress fell (table 3).
Adverse effects
There were no adverse effects directly attributable to antioxidant therapy. Detailed focus on the four deaths in patients in the antioxidant group revealed that all were admitted primarily to the hepatobiliary service of the Manchester Royal Infirmary (there were no tertiary referral patients in the trial), they were 64, 73, 67 and 75 years of age, respectively. These individuals had APACHE II scores at 48 hours of 24, 16, 22 and 15, respectively. Duration of disease from admission to death was 3, 15, 10 and 41 days, respectively, and cause of death was certified as multiple organ failure secondary to severe acute pancreatitis in all of them.
Post hoc analysis
We undertook post hoc secondary analyses to further understand our findings. In a binomial regression with the primary end point (organ dysfunction at day 7) as the predicted variable, only baseline MODS score and age were predictive. Consequently the primary end point was reanalysed according to MODS score (table 4) comparing treatment and control groups for patients enrolled with MODS scores of 0 or 1. The poorer outcomes at higher enrolment MODS values are reflected in all cause mortality (table 4).
Subgroup (post hoc) analyses
DISCUSSION
This study reports the findings of the largest placebo controlled trial of multiple compound antioxidant therapy in acute pancreatitis and to the best of our knowledge the only study to date to examine the effect of this intervention in patients with severe disease.
The backdrop to this study was provided by our report in l-arginine induced experimental acute pancreatitis in a rat model.8 This study demonstrated that combination antioxidant intervention using selenium, ascorbate and n-acetylcysteine given up to 12 hours after induction of acute pancreatitis was associated with a reduction in pancreatic and remote organ injury. Other experimental and clinical reports of favourable outcome in acute pancreatitis after antioxidant therapy had led this unit to introduce antioxidant therapy as a treatment for severe acute pancreatitis in the mid 1990s.19,20 We reported data on outcome in this cohort of patients receiving antioxidant therapy using case-control methodology.12 Observed mortality rates calculated for each individual based on their admission logistic organ dysfunction score were higher than expected.
These potentially contradictory data together with continuing sporadic reports on antioxidant therapy21 in acute pancreatitis led to this study. It was agreed that antioxidant therapy would only be used in these units in the context of this placebo controlled randomised trial. The combination of n-acetylcysteine, selenium and ascorbic acid that was then in use in critical care patients and which when modified by backwards extrapolation had provided the concentrations used in our rat model was selected for use in this trial. A pragmatic reason for this selection was that in the preceding decade there had been no reports of serious adverse outcome from these drugs when used in our unit in the dosage schedule in table 1.
Trial design focused on the need to recruit patients with severe disease and also to enter patients early in the disease course. The final agreed inclusion criterion of “within 72 hours of admission to hospital” represented a practical compromise between early inclusion and the need to allow patients time to discuss enrolment followed by preparation of antioxidant and/or placebo and represents a potential weakness of study design: it is possible that different outcomes may have been observed in patients given antioxidant therapy earlier in the disease course and also the range of inclusion period from 0 to 72 hours may have contributed to a broader spectrum of disease evolution than would be preferred.
One further point of emphasis in trial design was the prediction that 75% would have evidence of organ dysfunction at day 7: this is probably an overestimate. It was derived from internal audit data which showed that 75% of patients in the critical care unit with severe acute pancreatitis at 7 days would have evidence of organ dysfunction but even with contemporary disease descriptors based on the 1992 Atlanta consensus conference, a lower cut-off set at an APACHE II score of 8 will include individuals with less severe disease.
Recruitment to this study was predicted to be difficult and proved to be so. The need for three separate syringe drivers led to regular difficulties: additional intravenous access was required in a population of patients already needing multiple intravenous access for fluids, analgesia, antibiotics and monitoring. In addition, the restriction of entry criteria to APACHE 8 or more and also within 72 hours of admission to hospital led to sustained difficulties in recruitment (fig 1). The trial was terminated after the year 3 interim analysis. Despite the small number of patients in the final report the data are thought to represent a valid cross section of severe acute pancreatitis as the overall mortality rate in the group was 10% and thus reasonably representative of outcomes seen in contemporary management of this disease.
The key finding is that although antioxidant supplementation avoided the fall in antioxidant levels seen in the placebo group there is no evidence to support the use of intravenous antioxidants in patients with severe acute pancreatitis in terms of organ dysfunction, patient outcomes or reduced length of stay. Further, our data suggest that intravenous antioxidants might be harmful in patients with baseline organ dysfunction at two or more organ sites: however this is most probably interpreted as a chance finding. Deaths in patients with acute pancreatitis in this study occurred in individuals with more severe disease, with multiple organ failure. The study is underpowered and thus we acknowledge that there is a risk of type II error (inferring no difference between antioxidant therapy and placebo when a difference really exists).
In practical terms, these findings are in major contrast to the results of earlier studies by Kuklinski et al10,11 and this contradiction is not readily accounted for. We would argue that as the patient population in the present study is better characterised and also more representative of contemporary severe acute pancreatitis, our findings are more likely to be representative. It is accepted that a larger study may reveal benefits from antioxidant therapy in severe acute pancreatitis that are not identified here. None the less, the present data are important and unique in that they provide the first pragmatic evidence of lack of benefit from randomised evaluation of antioxidant therapy in severe acute pancreatitis. Considering the trend towards worse outcome (although not demonstrably treatment related) these data question the risk of exposing patients to future n-acetylcysteine, selenium and vitamin C based antioxidant trials in severe acute pancreatitis.
Acknowledgments
We acknowledge the support of our consultant surgical colleagues Ian Maclennan, Robert Pearson, James Hill, Rory McCloy and Basil Ammori. We are also indebted to David Schofield and Pauline Kay of the pancreatic laboratory for their technical assistance and to Dr Ioannis Virlos for his input at the trial design stage. We also acknowledge the efforts made by the staffs of the critical care units at all three hospitals and in particular Dr Jane Eddleston for her support and Dr Michael Parker for his protocol critiques. We are also indebted to the pharmacy departments at all three hospitals. Finally, we acknowledge our debt to the nursing staff of the surgical unit of the Manchester Royal Infirmary (wards 11 and 12) and in particular the lead nurse of the HPB service, Sister Shelagh Aldred.
REFERENCES
Supplementary materials
Files in this Data Supplement:
Footnotes
-
Published Online First 3 March 2007
-
Financial support: This study was supported by a grant from the Pancreatitis Patients’ Support Group at Manchester Royal Infirmary and the costs of antioxidants and placebo were met by Pharmanord UK.
-
Conflicts of interest: none.
Linked Articles
- Commentary