Article Text

Abstract
Background Restoration of myocardial perfusion is the goal of percutaneous coronary intervention (PCI) in patients with ST elevation myocardial infarction. A major predictor of no-reflow is the increasing time to treatment (TTT). Thrombus aspiration (TA) is reported to improve myocardial reperfusion as compared with standard PCI (SP).
Objective To investigate the influence of TTT on TA efficacy.
Design Pooled analysis of individual patients' data of three prospective randomised trials comparing TA and SP.
Patients A total of 299 patients (150 in TA group and 149 in SP group) entered the study. The study population was divided into three subgroups according to the TTT: ≤3 h (short TTT subgroup), >3 h to ≤6 h (intermediate TTT subgroup), >6 h to ≤12 h (long TTT subgroup).
Main outcome measures The goal of the study was the comparison of optimal myocardial reperfusion, defined as the combination of myocardial blush grade 2 or 3 at post-PCI angiography and ST resolution more than 70% at post-PCI ECG, between SP and TA according to TTT.
Results In the SP group, increasing TTT was associated with a decreased rate of optimal reperfusion (27.4% vs 17.9% vs 10%, p for trend=0.06), whereas in the TA group the same trend was not seen (40.9% vs 33.8% vs 50%, p for trend=0.93). In a multivariate logistic regression model, a significant interaction (p=0.04) between time to treatment and thrombus aspiration was observed.
Conclusions TA limits the adverse effects of TTT prolongation on myocardial reperfusion.
- Acute myocardial infarction
- no-reflow
- thrombus aspiration
- myocardial perfusion
- STEM1
- coronary angioplasty (PCI)
Statistics from Altmetric.com
- Acute myocardial infarction
- no-reflow
- thrombus aspiration
- myocardial perfusion
- STEM1
- coronary angioplasty (PCI)
Background
No-reflow is a common adverse event affecting the long-term outcome of patients with acute myocardial infarction undergoing urgent percutaneous interventions (PCI).1–4 Atherothrombotic embolisation is considered to have an important role in the pathogenesis of this multifactorial phenomenon.4 The use of thrombus-aspiration devices is associated with a significant reduction of distal embolisation and of no-reflow during primary or rescue PCI5 and seems to favourably influence clinical outcome.6 7
Besides atherothrombotic embolisation, another important independent predictor of myocardial reperfusion and long-term clinical outcome in patients with ST elevation myocardial infarction (STEMI) undergoing mechanical reperfusion is time to treatment (TTT). Indeed, experimental studies have shown that the extent of myocardial and microvascular injury is strongly dependent on the duration of ischaemia, with reduced salvage of myocardium when reperfusion is accomplished after 3 h of coronary occlusion.8–10 Accordingly, prolonged ischaemic time is associated with lower rates of ST resolution (STR) and myocardial blush grade (MBG) 2–3, with larger infarct size and higher 1-year mortality in patients with STEMI.11 12
Few and conflicting data are available on the possible interaction between TTT and thrombus aspiration use in patients with STEMI undergoing mechanical reperfusion.13 14
We assessed this interaction by pooling the clinical and angiographic data from three randomised trials comparing manual thrombus aspiration (TA) and standard PCI (SP).
Methods
We pooled the single patients' baseline and post-PCI clinical and angiographic data from three randomised trials comparing TA with SP in patients with STEMI. The trials included were the REMEDIA trial,15 the PIHRATE trial16 and the Export study by Noel et al.17 The key protocol characteristics of the three randomised studies are summarised in table 1.
Key features of the three trials entered in the study
The whole study population was analysed according to the TTT (time from symptom onset to catheter laboratory), which was categorised as ≤3 h (short TTT subgroup), >3 h to ≤6 h (intermediate TTT subgroup) and >6 h to ≤12 h (long TTT subgroup).
Baseline and post-PCI measures of coronary flow, thrombus score and MBG were derived from the original studies and were obtained in all three trials according to the following standard methods:
Anterograde coronary flow according to the standard TIMI criteria18;
Thrombus score according to the TIMI study group19;
MBG according to van't Hof et al.20
STR was defined as ≥70% reduction in the sum of the ST-segment elevation score between ECGs obtained before PCI and immediately after the procedure in all the three randomised trials21 and the STR analysis derived from the original studies.
Patient-level data on the occurrence of death, new myocardial infarction and target vessel revascularisation (early major adverse coronary events (MACE)) during hospitalisation were also obtained from the original studies.
Goals of the study
The main goal of the study was to compare optimal myocardial reperfusion (defined as final MBG 2–3 plus STR ≥70%22 between patients randomised to TA or SP in the three TTT subgroups).
We also compared STR ≥70%, final TIMI 3 flow, final MBG 2–3 and in-hospital MACE between patients randomised to TA or SP in the three TTT subgroups.
Statistical analysis
Continuous variables (presented as mean±SD) were compared by t test and analysis of variance. Categorical variables (reported as raw numbers (%)) were compared with Fisher exact tests. Trends in proportions were assessed with a linear-by-linear association test.
A multivariate logistic regression model was fitted to examine interaction between TTT and TA. All the predictors of optimal reperfusion at univariate analysis with p<0.1 (diabetes, left anterior descending artery as infarct-related artery, thrombus score), plus background variables (age, sex, and a three-level variable representing the pooled studies), and TA, TTT and their interaction term, were included in the model.
Results
A total of 345 patients were enrolled in the three trials. Forty-six patients were excluded from the study as assessment of final MBG was not possible for technical reasons and/or early post-PCI ECG was lacking or non-interpretable. Thus, 299 patients entered the study: 150 patients randomised to TA and 149 patients randomised to SP. As shown in table 2, the baseline clinical and angiographic characteristics of patients randomised to TA or SP were similar.
Baseline clinical and angiographic features of the study population according to treatment
Overall, patients randomised to TA had significantly better rates of early STR ≥70% (p=0.01), final TIMI 3 flow (p=0.02), final MBG 2-3 (p=0.001) and optimal myocardial reperfusion (p<0.001) than patients randomised to SP, while in-hospital MACE rates were similar (p=0.21) (table 3).
ECG and angiographic results and MACE according to treatment
The study population was divided according to the TTT into three subgroups as follows:
short TTT subgroup: 128 patients (66 TA vs 62 SP)
intermediate TTT subgroup: 135 patients (68 TA vs 67 SP)
long TTT subgroup: 36 patients (16 TA vs 20 SP).
There were no significant differences in baseline clinical and angiographic characteristics between the three precoronary time subgroups (table 4). In particular, there were no differences in the rate of baseline TIMI flow 0-1 and in the rate of baseline thrombus score 3-5.
Baseline clinical and angiographic features according to time-to-treatment
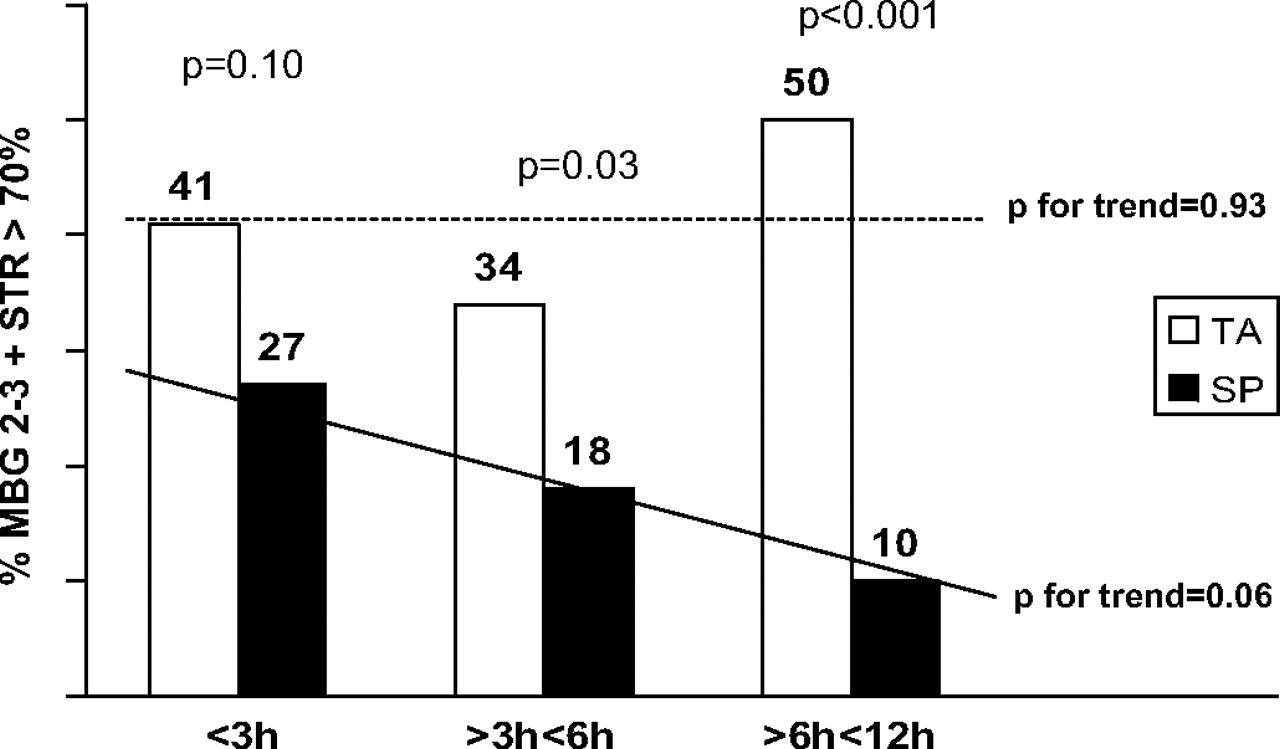
In the short TTT subgroup there was a trend in favour of TA for optimal reperfusion rate (27/66 (41%) TA versus 17/62 (27%) SP; p = 0.10), while a significant advantage in favour of TA was observed in the intermediate TTT subgroup (23/68 (34%) TA versus 12/67 (18%) SP; p=0.03) and in the long TTT subgroup (8/16 (50%) TA versus 2/20 (10%) SP; p<0.001) (figure 1).
{kind=link}
Rates of optimal myocardial reperfusion in the standard PCI (SP) and thrombus aspiration (TA) groups according to time to treatment. p Value for comparison derived from χ2 test. Trend in proportions assessed with linear-by-linear association test. Continuous line for SP; dotted line for TA. MBG, myocardial blush grade; STR, ST resolution.
Moreover, in the SP group increasing TTT was associated with a decreasing rate of optimal reperfusion (27.4% vs 17.9% vs 10%, p for trend=0.06), whereas in the TA group no trend was observed (40.9% vs 33.8% vs 50%, p for trend=0.93) (figure 1).
The remaining angiographic, electrocardiographic and clinical finding according to treatment modality and TTT are shown in table 5.
ECG and angiographic results and in-hospital MACE according to treatment modality and to time to treatment
The clinical and angiographic predictors of optimal myocardial reperfusion in the whole population were identified by univariate analysis (table 6) and included (with background variables and the interaction term between TA and TTT) in the multivariate analysis, for which results are depicted in the table 7. Moreover, at multivariate analysis, a significant interaction between thrombus aspiration and time to treatment was found (p=0.04).
Clinical and angiographic predictors of optimal myocardial reperfusion in the whole population
Estimated associations in the final logistic regression model
Discussion
The results of this pooled analysis of three trials indicate that TA may counterbalance the adverse effects of increasing ischaemic time on myocardial reperfusion.
The failure to achieve myocardial tissue reperfusion is the main complication limiting the early and long-term clinical benefit of mechanical reperfusion in patients with STEMI.4 No-reflow phenomenon is multifactorial and can be caused by the variable combination of different pathogenetic components like distal atherothrombotic embolisation and ischaemic injury.4 Ischaemic injury is known to be strongly related to the ischaemic time: after prolonged ischaemia, morphological changes in endothelial cells, in myocardial cells and in the interstitial space can cause microvascular obstruction 23–25 and a longer time to reperfusion is associated with a higher prevalence and extension of no-reflow.9
Among the different strategies to reduce distal embolisation, the use of TA is promising.7 26 Whether or not the efficacy of TA depends on the ischaemic time is unknown.
According to our results the beneficial effect on optimal myocardial reperfusion of TA seems to be more pronounced in the subgroups with a time to treatment >3 h. In particular, in the TA group the rates of optimal myocardial reperfusion were constant in the three subgroups of TTT while in the SP group increasing TTT (as expected) was associated with decreasing rates of optimal reperfusion. Such original observation is consistent with the recent results of the VAMPIRE trial, which showed a greater reperfusion and clinical benefit by thrombectomy in the subgroup of late-presenting (6–24 h) patients.13 Interestingly, the recently published update of the American College of Cardiology guidelines on STEMI treatment considers thrombus aspiration as a class IIa indication for PCI in STEMI, suggesting that it is reasonable to use it in patients with high thrombus burden and short ischaemic time.27 This study showing greater absolute efficacy of TA with longer ischaemic time argues against this suggestion, leading to the need for further investigation on this crucial issue.
The most likely explanation of the increasing benefit of TA over time is that the contribution of distal embolisation to microvascular obstruction becomes more relevant with the passage of time. Unfortunately, this hypothesis cannot be tested in current experimental models,8–10 as in these models myocardial infarction is caused by coronary ligation and not by thrombotic occlusion.
The results of this pooled analysis of three randomised trials suggest that TA may reduce the adverse effect of the TTT prolongation on myocardial reperfusion in patients with STEMI.
Study limitations
The main limitation of our study is the difference in the inclusion criteria used in the three trials which entered the single-patient data analysis. This heterogeneity, leading to an overall lower rate of the primary end point in the PIHRATE trial, may be caused by the selection in this study of a higher-risk population, with baseline TIMI flow 0 or 1, and the exclusion of lower-risk patients with largely patent culprit artery (TIMI flow 2 or 3) at presentation (table 1). However, in our study, we accounted for between-study differences in the statistical modelling and found no evidence of treatment effect heterogeneity (p value for interaction term between ‘study variable’ and ‘thrombus aspiration variable’=0.2).
Another possible limitation is the use of two different TA devices in the included studies (Export catheter in the Noel study and Diver CE in the REMEDIA and PIHRATE trials; table 1), although no large difference in the effect size was previously observed between the two devices.28
The results may also have been influenced by the quality of each original trial. Indeed, no single-patient data were available on thienopyridine, or on the issue of direct stenting versus predilatation, or on drug-eluting stents use.
References
Footnotes
Competing interests None.
Patient consent Obtained.
Ethics approval This study was conducted with the approval of the ethics committee of the Catholic University of Sacred Heart, Rome, Italy.
Provenance and peer review Not commissioned; externally peer reviewed.