Article Text

Abstract
Aim To determine the frequency of MED12 mutations in a series of 112 breast phyllodes tumours, and to correlate the findings with clinicopathological parameters and survival outcomes.
Methods Phyllodes tumours from the Department of Pathology, Singapore General Hospital, were classified into benign, borderline and malignant categories. Genomic DNA from formalin-fixed paraffin-embedded phyllodes tumours was extracted, purified and subjected to ultra-deep-targeted amplicon sequencing across exon 2 of the MED12 gene. Sequencing was performed on the Illumina MiSeq next-generation sequencing platform and bioinformatics analysis applied. Appropriate statistical analyses were carried out.
Results There were 66 benign, 32 borderline and 14 malignant tumours, with 43 (65.1%), 21 (65.6%) and 6 (42.8%) disclosing MED12 mutations (missense, splice site, indel), respectively. For 97 cases with available follow-up, there were 10 (10.3%) recurrences. Patients with phyllodes tumours that harboured MED12 mutations experienced improved disease-free survivals, with higher recurrence likelihood in those without MED12 mutations (HR 9.99, 95% CIs 1.55 to 64.42, p=0.015).
Conclusions Similar to fibroadenomas, phyllodes tumours show a high frequency of MED12 mutations, affirming the close biological relationship between these fibroepithelial neoplasms.
- BREAST
- CELL BIOLOGY
- GENETICS
Statistics from Altmetric.com
Introduction
Phyllodes tumours of the breast are unusual and infrequently encountered fibroepithelial neoplasms which bear clinicopathological resemblance to the common fibroadenoma.1 The relationship between phyllodes tumours and fibroadenomas has been a subject of long-standing discussion. Apart from microscopic similarities of the phyllodes tumour to the intracanalicular fibroadenoma, the finding of fibroadenoma juxtaposed to phyllodes tumour is a familiar experience of pathologists during routine diagnostic work. While the fibroadenoma is a benign and clinically innocuous lesion, the phyllodes tumour is regarded as a neoplasm that has a tendency to recur, with recurrence rates increasing from benign to borderline and malignant tumours.2
Published data on the biological link between these tumours are scant. There is a report of three cases of fibroadenomas progressing to phyllodes tumours, whereby patients with initial diagnoses of fibroadenoma later recurred as phyllodes tumours.3 In that report, clonality studies found the original fibroadenomas to be monoclonal, but whether they could have been undersampled phyllodes tumours was not addressed. Another group described clonality analysis of fibroadenomas, discovering one ‘simple’ fibroadenoma and one complex fibroadenoma with monoclonality of stroma. The monoclonal ‘simple’ fibroadenoma was histologically described to contain a phyllodes component, which also demonstrated stromal monoclonality.4 Kuijper et al5 found monoclonality in areas of apparent stromal expansion within fibroadenomas and suggested that there could be stromal progression of fibroadenoma to phyllodes tumour. Another study6 observed identical loss at the same microsatellite locus in a synchronous fibroadenoma and phyllodes tumour of the same breast, while allelic losses at TP53 and another microsatellite locus were detected in the phyllodes tumour but not in the synchronous fibroadenoma. The authors suggested that the latter could be implicated in progression of fibroadenoma to phyllodes tumour. In a study that included 36 malignant phyllodes tumours by a Japanese group,7 11 were associated with previous fibroadenomas, which could be interpreted as progression of fibroadenomas to phyllodes tumours. Interestingly, they concluded that there was a better clinical outcome in malignant phyllodes tumours preceded by fibroadenomas than in those diagnosed de novo.
Recently, we discovered highly recurrent MED12 somatic mutations in 59% of fibroadenomas using exome sequencing.8 MED12 is a gene on the X chromosome that encodes the Mediator complex subunit 12, which is a multiprotein complex widely involved in transcriptional regulation of gene expression.9 Since our initial publication, there have been additional reports of MED12 mutations in fibroadenomas as well as phyllodes tumours,10–14 with some demonstrating a lower frequency of MED12 mutations in malignant than benign and borderline phyllodes tumours.11 ,13 In light of the intertwining link between fibroadenomas and phyllodes tumours, we therefore embarked on determining the frequency and spectrum of MED12 aberrations in a large series of breast phyllodes tumours, as well as to compare against those previously documented in fibroadenomas.
Materials and methods
Clinical specimens
Phyllodes tumours were diagnosed and subtyped according to histopathological examination of surgically excised tumours, using criteria recommended by the WHO classification of breast tumours.1 Briefly, a benign phyllodes tumour was diagnosed when a fibroepithelial neoplasm with exaggerated intracanalicular pattern and fronded architecture was accompanied by mild stromal cellularity with minimal to mild nuclear atypia, pushing borders and mitoses of four or less per 10 high power fields, without stromal overgrowth. The diagnosis of a malignant phyllodes tumour was rendered when there was marked stromal cellularity, marked atypia, stromal overgrowth, permeative margins and mitotic activity of 10 or more per 10 high power fields. Tumours with intermediate features were regarded as borderline.15 A total of 112 phyllodes tumours were included in this study, derived from archival formalin-fixed paraffin-embedded (FFPE) samples of excision specimens processed and handled by the Department of Pathology, Singapore General Hospital.
DNA extraction
Genomic DNA (gDNA) from FFPE tissue was extracted and purified using the Qiagen FFPE DNA kit according to the manufacturer's guidelines. gDNA yield and quality were determined using Picogreen fluorometric analysis as well as visual inspection of agarose gel electrophoresis images.
Ultra-deep-targeted amplicon sequencing of MED12 exon 2
For sensitive detection of low-frequency variants in MED12 exon 2, we used ultra-deep-targeted amplicon sequencing. Six PCR amplicons were designed and tiled across exon 2 of MED12. We then used Fluidigm's Access Array System to generate and pool the amplicons according to the manufacturer's instructions. For each sample, 50 ng of gDNA was used as template. Sequencing library preparation of the pooled amplicons was performed using the TruSeq HT DNA Sample Preparation Kit (Illumina) according to the manufacturer's instructions. Sequencing was performed on the Illumina MiSeq next-generation sequencing platform for 150 cycles using the MiSeq Reagent kit V.3.
Bioinformatics analysis of sequencing reads was performed. Briefly, undetermined (‘N’) base calls at the ends of reads were trimmed. Following this, the 5′ end of each read was trimmed by 25 bases to eliminate the possibility of primer inclusion. The Burrows–Wheeler Alignment16 tool (0.6.2) was used to align the resulting reads to the reference human genome (hg19). For more sensitive detection of insertions and deletions (indels), we also ran a separate alignment process using modified settings (o=2, e=30, d=30, O=0, E=0, L=0). Indels were identified through manual inspection, whereas automated detection of point mutations was performed using the samtools17 (0.1.18) mpileup tool. Variant calls were restricted to regions covered by amplicons. Variant allele frequencies were calculated for each position in the targeted region, and those that exceeded a threshold of 5% were considered candidate variants. In order to minimise the possibility of PCR-induced artifacts, variants were only considered valid if present in at least two amplicons. Candidate variants had at least 21 620 sequencing reads overlapping them, with an average coverage of 184 526 reads.
To ascertain the sensitivity of our assay, positive control samples containing spiked-in validated mutant MED12 at allele frequencies (15%, 10%, 5% and 3%) were generated via serial dilutions. We accurately detected variants in positive control samples at allele frequencies down to 3%. We also calculated alternate (non-reference) allele frequencies across all positions in our target region in order to estimate the likelihood of error from sequencing and alignment artifacts. The mean alternate allele frequency was 0.281% with a SD of 1.09%. Thus, our detection threshold of 5% exceeds four SDs from the estimated background error rate.
Statistical analysis
Statistical analyses were performed in R. The relationship between clinicopathological parameters and MED12 mutational status was tested using Fisher's exact tests as appropriate. Follow-up data were obtained from patient casenotes. Disease-free survival (DFS) was defined as time from diagnosis to recurrence or date of last follow-up. DFS was estimated with the Kaplan–Meier analysis and compared between groups using the log-rank statistics. Multivariate Cox regression was carried out to evaluate the effect of MED12 mutations on DFS. HRs together with 95% CIs were reported. A p value of <0.05 defined statistical significance.
Results
Phyllodes tumours were histologically subdivided into benign, borderline and malignant grades according to the WHO criteria (figure 1),1 with 66 benign, 32 borderline and 14 malignant tumours. Detailed clinicopathological features are shown in table 1. All 112 phyllodes tumours were subjected to amplicon sequencing analysis for the presence of MED12 exon 2 mutations (table 2). Overall, 70 (62.5%) of phyllodes tumours demonstrated MED12 mutations. Figures 2 and 3 show the distribution of somatic mutations among phyllodes tumours in this series, compared with those reported for our previous study on fibroadenomas.
Association between clinicopathological features of phyllodes tumours and MED12 mutations (N=112)
High frequency of MED12 exon 2 mutations in phyllodes tumours of breast
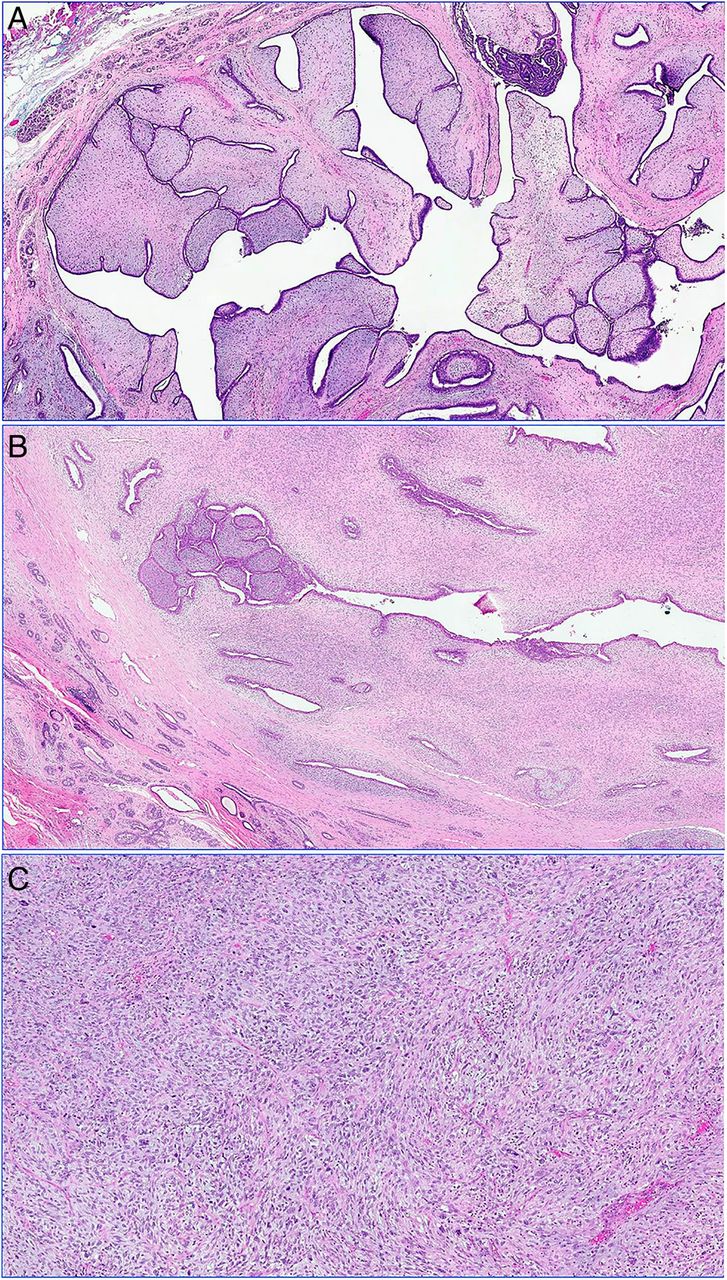
(A) Benign phyllodes tumour shows prominent leafy stromal fronds covered by benign epithelium, accompanied by patchy mild stromal hypercellularity, with pushing rounded borders. (B) Borderline phyllodes tumour demonstrates a greater degree of stromal hypercellularity and less well-defined borders. (C) Malignant phyllodes tumour discloses stromal overgrowth with marked stromal nuclear pleomorphism and brisk mitoses.

Comparison of MED12 exon 2 mutations in fibroadenomas (FA) and phyllodes tumours (PT) shows a similar distribution in both tumours.
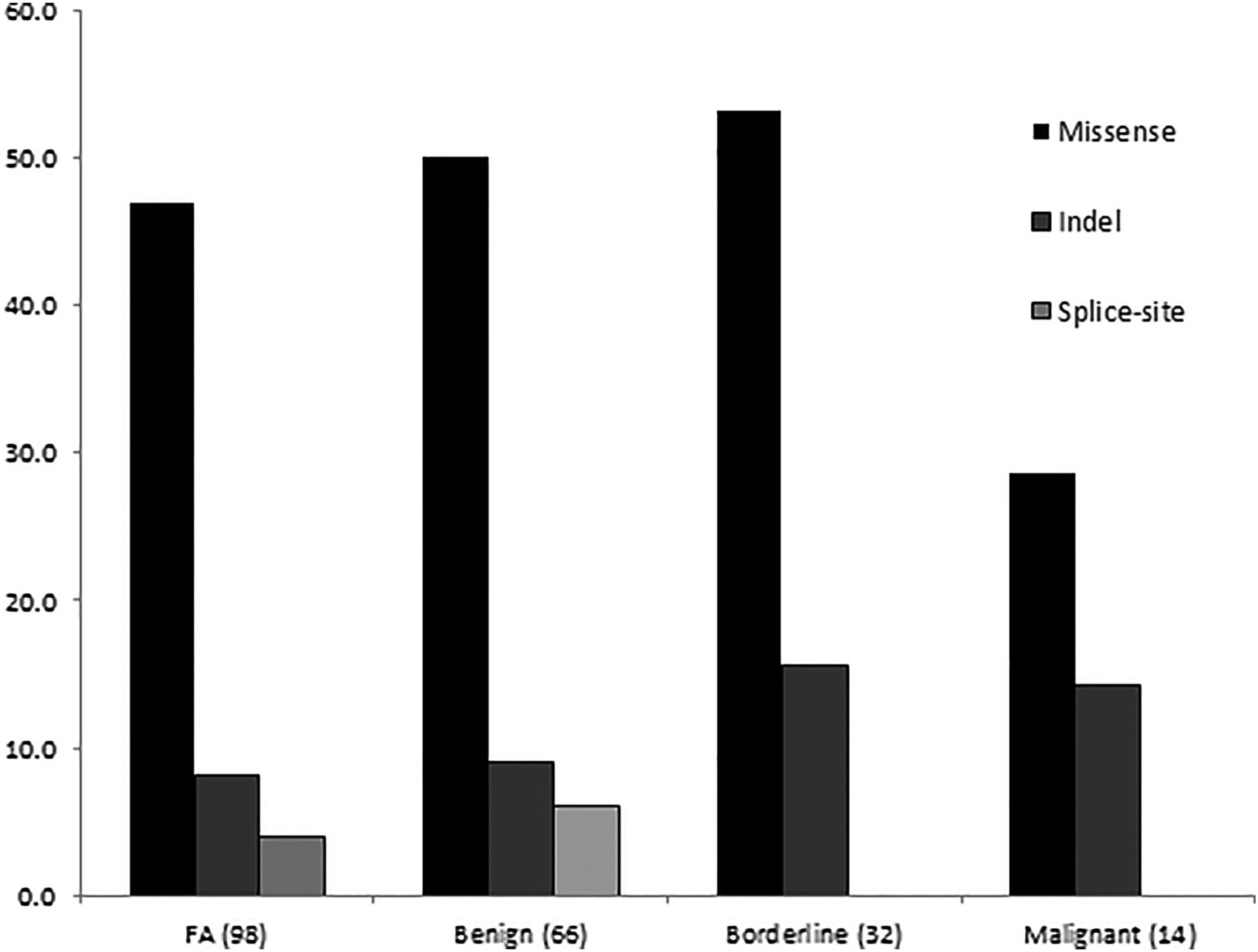
Frequency of MED12 somatic variants in fibroadenomas (FA) and phyllodes tumours (benign, borderline, malignant). Splice site mutations are observed only in FA and benign phyllodes tumours.
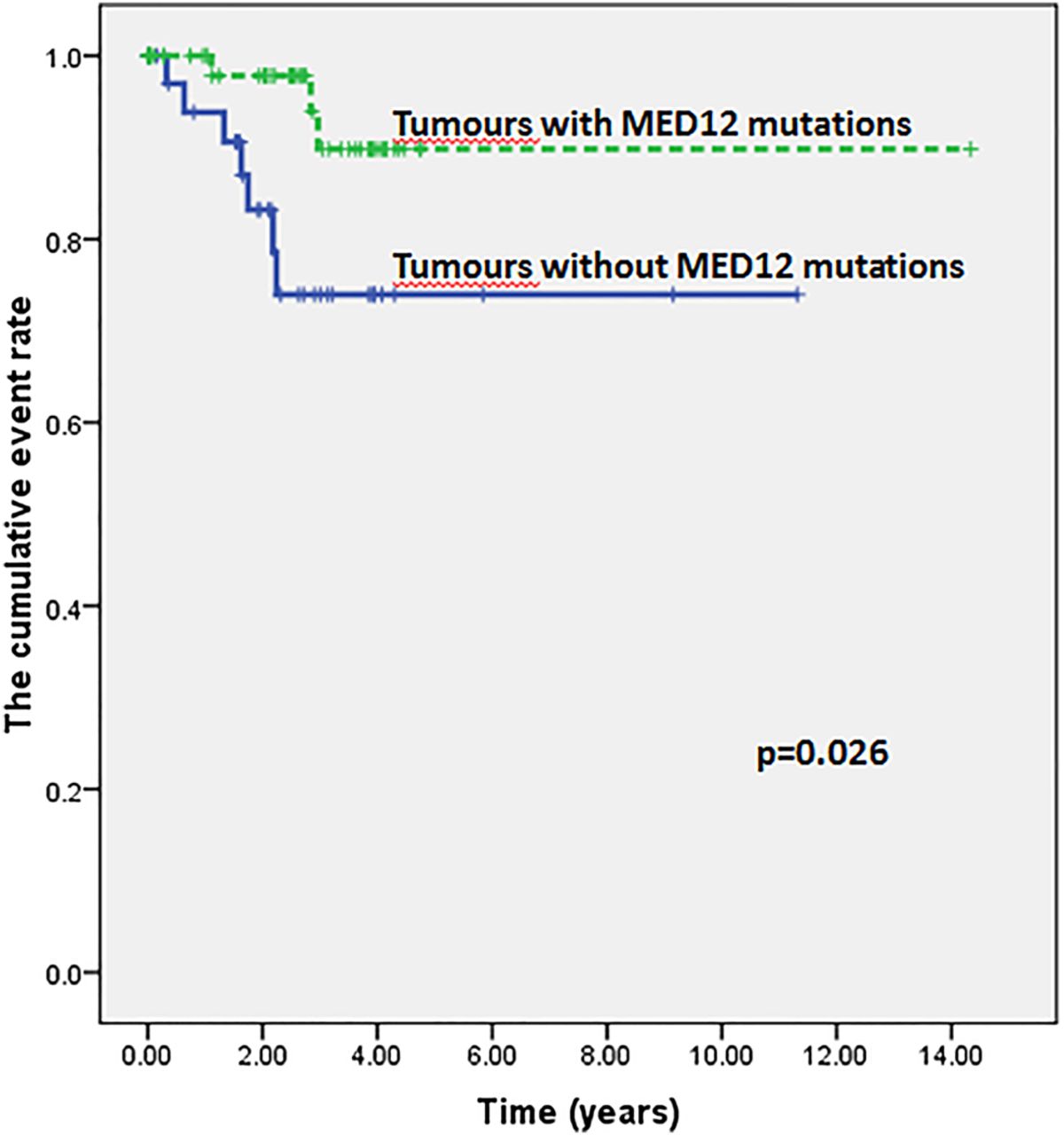
Follow-up information was available for 97 cases, with mean and median durations of 32 and 30 months, respectively (IQR, 1.24–3.70 years). There were 10 (10.3%) recurrences, constituted by three (5.3%) of 57 benign, five (17.2%) of 29 borderline and two (18.2%) of 11 malignant tumours. Patients with phyllodes tumours that harboured MED12 mutations experienced improved DFS than those without mutations (figure 4). On univariate analysis, the only parameter that correlated with recurrence was MED12 status (table 3). Multivariate Cox regression analysis, with adjustment for age, grade, tumour size and ethnicity showed a HR of 9.99 (95% CIs 1.55 to 64.42, p=0.015) for tumours without MED12 mutations.
Univariate analysis of clinicopathological parameters with disease-free survival

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Kaplan–Meier survival analysis showed an improved disease-free survival for patients whose tumours disclosed MED12 mutations.
Discussion
The MED12 gene is located on the long arm of the X chromosome. The protein that it encodes, mediator complex subunit 12, forms a part of the mediator complex that comprises 25 proteins working together in concert to regulate gene activity.18 The MED12 protein is involved in early neuronal development as well as cellular signalling that governs cell growth, migration and differentiation. Germline mutations in the MED12 gene are linked to several syndromes,19 ,20 while somatic mutations are described in a variety of tumours including uterine smooth muscle tumours, prostatic and colonic adenocarcinomas18 ,21–23 and more recently, fibroadenomas and phyllodes tumours of the breast.8 ,10
In this series of breast phyllodes tumours, the overall rate of MED12 mutations of 62.5% is similar to the 59% frequency in fibroadenomas,8 affirming the close molecular relationship between these neoplasms. In addition, the majority of MED12 mutations (52 of 70; 74%) involved codon 44, comparable again with the 71% MED12 codon 44 aberrations documented in our previously described fibroadenomas.8 When phyllodes tumours were separated into benign, borderline and malignant varieties, 65.1%, 65.6% and 42.8% showed MED12 mutations, respectively.
The histological distinction of fibroadenoma, particularly the cellular variety, from phyllodes tumour is a constant challenge, even among pathologists who specialise in breast pathology.24 Occurrence of MED12 mutations in phyllodes tumours in a similar frequency to that in fibroadenomas provides the biological basis to this likeness, despite the divergence in recurrence rates and clinical progression.
Apart from breast fibroepithelial neoplasms, MED12 mutations have been detected in uterine leiomyomas.18 ,23 The uterine leiomyoma is a benign tumour which occurs in an organ that is hormonally responsive, similar to the breast. While MED12 aberrations are common in the leiomyoma, they are rare in its malignant counterpart—the leiomyosarcoma.22 If the role of MED12 in both fibroadenomas and leiomyomas is related to oestrogen regulation as postulated,8 the lower rate of mutations in malignant phyllodes tumours may implicate a loss of dependence on the oestrogen regulation pathway in the development of this subset, a consideration that can be partially and indirectly supported by a study that found decreasing epithelial hormonal expression with increasing malignancy in phyllodes tumours.25 It is likely that other genetic aberrations contribute to the development of malignant phyllodes tumours or are harnessed in the progression of benign phyllodes tumours to the malignant variety.
Cani et al10 described frequent MED12 mutations (67%) across all three histological grades of 15 breast phyllodes tumours, with individual subset mutational rates of 80%, 80% and 40% in benign, borderline and malignant tumours, respectively. Loss of function mutations in p53 and deleterious mutations in Rb1 and NF1 were exclusively detected only in the malignant grade.10 These additional mutational events in tumour suppressor genes are likely responsible for acquisition of malignant characteristics and aggressive biological behaviour in phyllodes tumours.
There were no statistically significant correlations between clinicopathological characteristics of our series of phyllodes tumours and MED12 mutations, suggesting that MED12 may not be specifically linked to, or be responsible for, histological alterations used in the grading of these tumours. Nevertheless, the presence of MED12 mutations augured a better prognosis for women with phyllodes tumours, with those cases lacking MED12 aberrations demonstrating close to tenfold increased likelihood of recurrence. The underlying reason for this improved clinical behaviour of phyllodes tumours harbouring MED12 mutations is uncertain and may be related to the suggestion of hormonal dependence of neoplasms bearing MED12 aberrations.
Limitations of this study include the relatively few number of malignant phyllodes tumours which may affect the dependability of the reported MED12 mutation rates in the subset. While no laser capture microdissection was performed in this study of paraffinised tumour samples to verify that MED12 mutations were indeed confined to the stromal component, our previous work on fibroadenomas8 as well as phyllodes tumours unpublished (unpublished) had verified the stromal origin of MED12 mutations through laser microdissected material. In addition, the few recurrences resulted in relatively wide CIs, reducing statistical robustness.
In summary, our study of 112 phyllodes tumours shows a similar rate of MED12 mutations as previously reported in breast fibroadenomas, underscoring their close biological relationship. Malignant phyllodes tumours were less frequently associated with MED12 mutations (42.8%) although this was not a statistically significant finding. No correlations were found with other clinicopathological features. Tumours with MED12 mutations demonstrated an improved DFS which may provide insights into its biological role. More work to elucidate accompanying genomic abnormalities that drive aggressive behaviour in borderline and malignant phyllodes tumours is needed to expand the current understanding of this group of fascinating neoplasms.
Take home messages
The MED12 gene, found on the X chromosome, encodes the Mediator complex subunit 12, a multiprotein complex widely involved in transcriptional regulation of gene expression.
MED12 is frequently mutated in breast fibroadenomas (59%) and phyllodes tumours (62.5%), underscoring their close biological relationship, and suggests a role in initiation of these neoplasms.
MED12 mutations have a slightly lower frequency in malignant phyllodes tumours (42.8%), though this finding is not statistically significant.
The improved disease-free survival of patients whose phyllodes tumours harboured MED12 mutations may reflect its effect on biological behaviour.
References
Footnotes
Handling editor Cheok Soon Lee
Contributors CCYN, JT, CKO, WKL, VR performed the experiments and analysed the bioinformatics data. NDMN and JCTL carried out the histotechnical aspects. AAT, SAS, JI, IB and APYC reviewed the cases. BTT and PHT initiated and supervised the study, reviewed and wrote the manuscript.
Funding This work was supported in part by funding from the Singapore National Medical Research Council (NMRC/STAR/0006/2009) and the Singapore National Cancer Centre Research Fund.
Competing interests None declared.
Ethics approval SingHealth Centralised Institutional Review Board (2005/002/F).
Provenance and peer review Not commissioned; externally peer reviewed.