Article Text

Abstract
Background Since 1988, Brazil's Unified Health System has sought to provide universal and equal access to immunisations. Inequalities in immunisation may be examined by contrasting vaccination coverage among children in the highest versus the lowest socioeconomic strata. The authors examined coverage with routine infant immunisations from a survey of Brazilian children according to socioeconomic stratum of residence census tract.
Methods The authors conducted a household cluster survey in census tracts systematically selected from five socioeconomic strata, according to average household income and head of household education, in 26 Brazilian capitals and the federal district. The authors calculated coverage with recommended vaccinations among children until 18 months of age, according to socioeconomic quintile of residence census tract, and examined factors associated with incomplete vaccination.
Results Among 17 295 children with immunisation cards, 14 538 (82.6%) had received all recommended vaccinations by 18 months of age. Among children residing in census tracts in the highest socioeconomic stratum, 77.2% were completely immunised by 18 months of age versus 81.2%–86.2% of children residing in the four census tract quintiles with lower socioeconomic indicators (p<0.01). Census tracts in the highest socioeconomic quintile had significantly lower coverage for bacille Calmette-Guérin, oral polio and hepatitis B vaccines than those with lower socioeconomic indicators. In multivariable analysis, higher birth order and residing in the highest socioeconomic quintile were associated with incomplete vaccination. After adjusting for interaction between socioeconomic strata of residence census tract and household wealth index, only birth order remained significant.
Conclusions Evidence from Brazilian capitals shows success in achieving high immunisation coverage among poorer children. Strategies are needed to reach children in wealthier areas.
- Epidemiology
- ethnicity
- health status
- health policy
- surveillance
This is an open-access article distributed under the terms of the Creative Commons Attribution Non-commercial License, which permits use, distribution, and reproduction in any medium, provided the original work is properly cited, the use is non commercial and is otherwise in compliance with the license. See: http://creativecommons.org/licenses/by-nc/2.0/ and http://creativecommons.org/licenses/by-nc/2.0/legalcode.
Statistics from Altmetric.com
Introduction
Brazil's national immunisation programme was created in 1973 to provide universal access to a number of vaccines to control infectious diseases and reduce the post-neonatal component of childhood mortality.1 Health was declared a universal right in the 1988 Brazilian Constitution, and the immunisation programme became part of the Unified Health System (Sistema Unico de Saúde or SUS) with the aim of providing universal and equal access to services for health promotion.2 Vaccination is voluntary; the Brazilian government provides vaccines to guarantee universal access to childhood vaccination but does not use coercive strategies. In addition to routine vaccination at health facilities, supplemental immunisation activities during national immunisation days provide opportunities to receive missed vaccinations. Despite the guarantee of universal access, heterogeneous vaccination coverage suggests that some population groups remain underserved.3
In 2006, the Brazilian Ministry of Health commissioned a population-based vaccine coverage survey to provide estimates of the proportion of children receiving recommended immunisations by 18 months of age. The survey was conducted in all 26 state capitals and the federal district. In this study, we examine coverage with universally recommended and other vaccines by socioeconomic characteristics of children's census tracts of residence and evaluate risk factors for incomplete vaccination.
Methods
Recommended childhood immunisations in Brazil
In 2005, the recommended childhood immunisation schedule included bacille Calmette-Guérin at birth, oral polio vaccine (OPV), diphtheria–tetanus–whole cell pertussis (DTP) and Haemophilus influenzae type b (Hib) vaccine at 2, 4 and 6 months, and hepatitis B (HepB) vaccine at 1, 2 and 6 months.4 DTP and Hib are given as a combined quadravalent vaccine (Bio-Manguinhos, Rio de Janeiro, Brazil); HepB is given as a monovalent vaccine (produced by Butantan Institute, São Paulo, Brazil). Measles–mumps–rubella vaccine is recommended at 12 months of age. Children who received all vaccines included in the recommended infant immunisation schedule by 18 months of age were considered completely vaccinated. Children were considered incompletely vaccinated if they were missing one or more recommended vaccines and unvaccinated if they had not received any of the recommended vaccines. Dropout was defined as receipt of the first dose of DTP–Hib without completing the three-dose series by 18 months of age. Yellow fever vaccine and oral rotavirus vaccine were not included in this analysis. Yellow fever vaccine is recommended only in yellow fever endemic areas.4 Oral rotavirus vaccine was introduced into Brazil's national immunisation programme in April 2006 without catch-up vaccination for older children.
The federal government purchases vaccines, which are distributed to state and local immunisation programmes. Government-purchased vaccines are offered at no cost throughout the country at >30 000 public facilities, 108 private clinics and 36 public referral centres for populations with specific indications. During national immunisation days, vaccines have been provided at >130 000 vaccination posts. Licensed vaccines not included in the immunisation schedule are available for purchase at private clinics and are provided for free to children with specific risk factors at public referral centres.
Survey design
We conducted a household cluster survey based on WHO's EPI cluster survey methodology for estimating immunisation coverage,5 in 27 Brazilian capital cities (including 26 state capitals and the federal district), which together account for 23.7% of Brazil's population. The target population for the survey was children born in 2005, who were between 20 and 40 months of age at the time of household surveys conducted between August 2007 and May 2008. According to the national birth registry (SINASC), there were 713 510 children born in these 27 capital cities in 2005. The survey was approved by the Research Ethics Committee of Santa Casa Hospital in São Paulo, Brazil.
Census tracts were systematically selected using a stratified cluster design in each of the 27 capitals (figure 1). For each capital, we obtained a complete listing of census tracts and their populations in the 2000 census from the Brazilian Institute of Geography and Statistics.6 Census tracts in each capital were ranked in decreasing order of mean head of household income, per cent of heads of household earning >20 times the minimum wage and per cent of heads of household with ≥17 years of education, according to 2000 census data.6 Ties were assigned equal rank. The sum of the three ranks was used to create quintiles (labelled A, B, C, D and E) within each capital, in which census tracts with the highest combined income and education measures were in the highest socioeconomic quintile (stratum A) and those with the lowest combined income and education measures were in the lowest socioeconomic quintile (stratum E; web appendix 1). Ranking of census tracts within each capital takes into account marked differences in household income (web appendix 1). Census tracts with small populations in a given socioeconomic stratum were combined to obtain a minimum number of children younger than 5 years.

Study design for immunisation coverage survey in Brazilian capital cities.
In all 27 capital cities, an equal number of census tracts were randomly selected from each socioeconomic quintile to obtain a total of 60–150 clusters based on total population size (web appendix 2). In total, 2910 clusters, which included 4009 census tracts, were sampled. In each cluster, the first household was randomly selected as follows: census tract maps were subdivided into polygons formed by intersecting streets, each polygon was numbered, one polygon was randomly selected and within that polygon, one intersection was randomly selected. Interviewers began at the first household at the selected intersection and followed a predetermined direction inside the polygon before moving to the next polygon until all polygons in the cluster had been surveyed. In each cluster, the first seven eligible children were included in the survey. No replacement was sought for children whose parent or guardian refused to participate.
Trained interviewers in each capital recorded the child's gender, race and birth order on standard forms, as well as responses to standardised questions about household possessions, presence of child's grandparents, number of inhabitants per room, years of mother's education, mother's employment and whether household was headed by a single parent. As an index of household wealth, we used the Brazilian Economic Classification Criteria, a composite score based on possession of durable goods and years of education of female head of household.6 Dates for each vaccine and dose received were recorded from the child's vaccination card. Interviewers asked if the child participated in the most recent national immunisation day against poliomyelitis and the reason for non-participation for those children who did not participate.
Statistical analysis
We calculated the incidence of completely vaccinated children by 18 months of age. Children without vaccination cards were excluded from this analysis. Sample weights for each child included in the survey were calculated based on the probability of selection and adjusted for non-response and the design effect. Weighted estimates of coverage and 95% CIs for each vaccine and complete vaccination schedule were calculated in Csample EpiInfo 2000 (V.3.4.3, US Centers for Disease Control and Prevention) to account for complex sample design. Statistical significance was defined as p<0.05.
We analysed risk factors for incomplete vaccination using logistic regression in the SPSS software package (V.17) and present adjusted OR and 95% CI from logistic regression models. We used a hierarchical modelling strategy,7 in which the dependent variable, vaccination status by 18 months of age, was dichotomised as completely vaccinated (referent group) or incompletely vaccinated. Children who had received none of the recommended immunisations were excluded from the multivariable analysis.
Independent variables were grouped in four hierarchical blocks (from more contextual to more individual characteristics): neighbourhood characteristics (census tract socioeconomic quintile), household characteristics (household socioeconomic index according to the Brazilian Economic Classification Criteria, number of inhabitants per room, presence of child's grandmother), maternal characteristics (years of education, single parent and employment) and child characteristics (gender, birth order and race). Child's race was defined based on census categories as Caucasian, African–American, Asian, indigenous or mixed race. Within each block, variables were added using forward stepwise selection, with a significance value of p<0.05 for retaining each additional variable. Results are presented for the final hierarchical model that included retained variables from all four blocks.
To access heterogeneity of effects of completely vaccinated children among strata of census tract socioeconomic quintile and household wealth index, we conducted a stratified analysis and calculated attributable risk, defined as the difference between the incidence of children completely vaccinated by 18 months of age in the specified stratum versus the reference stratum (children in households with lowest wealth index in census tracts in the lowest socioeconomic quintile).
Results
Interviews were conducted for 17 749 (87.1%) of the 20 370 target children. Parent or guardian refusal to participate accounted for 2.1% of attempted interviews, unavailability of parent or legal guardian on three separate attempts to interview accounted for 2.7% and inability to find seven eligible children in selected census tract clusters for 8.2%. In households with eligible children, those in the highest socioeconomic quintile had the highest refusal percentage (6.8% in stratum A, vs 2.4%, 1.4%, 1.0% and 0.6% in strata B–E, respectively, χ2 test for trend, p<0.001), accounting for 54.2% of all refusals.
Vaccination cards were available for 17 295 (96.8%) of 17 749 children surveyed in 27 Brazilian capital cities. The proportion of children without vaccination cards was similar by socioeconomic quintile of census tract of residence (stratum A, 3.3% (95% CI 2.5% to 4.2%); stratum E, 2.7% (95% CI 1.9% to 3.6%)). Among 17 295 children with vaccination cards, 14 538 (82.6%) had received all recommended vaccinations, 2634 (18.2%) were missing one or more vaccinations and 123 (0.7%) had received none of the recommended childhood vaccinations by 18 months of age. Descriptive statistics of children according to vaccination status are shown in web appendix table 3.
Children residing in census tracts in the highest socioeconomic stratum had the lowest percentage of complete immunisations by 18 months of age (77.2%, 95% CI 75.3% to 79.7%, p<0.01), while children residing in other socioeconomic quintiles were statistically equivalent (81.2%–86.2%; figure 2). The percentage of children who were completely vaccinated by 18 months of age varied substantially by capital (table 1). In 10 capitals, children residing in census tracts in the highest socioeconomic quintile had the lowest percentage of complete vaccination by 18 months of age. In three capitals, children residing in census tracts in the lowest socioeconomic stratum had the lowest vaccination coverage (table 1).
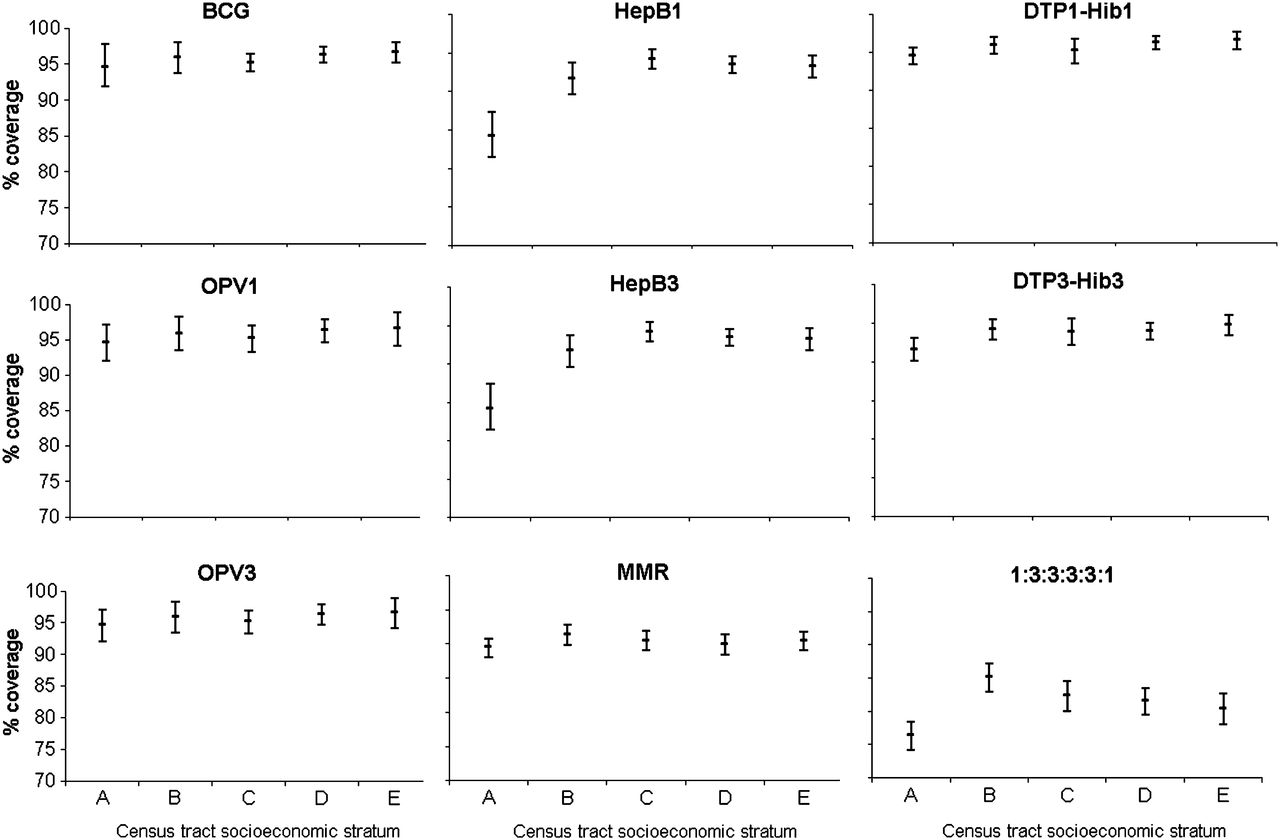
Per cent of children surveyed who by 18 months of age had received childhood immunisations included in the national immunisation programme, according to socioeconomic quintile of residence census tract (A=wealthiest, E=poorest) in 27 Brazilian capitals. BCG, bacille Calmette-Guérin; DTP, diphtheria–tetanus–whole cell pertussis; HepB, hepatitis B; Hib, Haemophilus influenzae type b; MMR, measles–mumps–rubella; OPV, oral polio vaccine.
Variation between Brazilian capitals in estimated coverage with complete vaccination schedule by 18 months of age, by socioeconomic stratum, 2007–2008*
In univariate analyses, living in single-parent households was associated with having received none of the recommended vaccines by 18 months of age (OR 1.5, 95% CI 1.0 to 2.3), while having mothers who worked outside the home was protective (OR 0.5, 95% CI 0.3 to 0.7). Associations were not significant after adjusting for socioeconomic variables. Receiving none of the recommended vaccinations was not significantly associated with residing in census tracts in the highest socioeconomic stratum (OR 1.6, 95% CI 0.9 to 2.8) or in households with higher wealth indices (OR 1.2, 95% CI 0.7 to 2.0).
Risk factors for incomplete vaccination in univariate analyses included higher birth order, less maternal education and residing in census tracts in the highest socioeconomic stratum (table 2). However, the observed association between incomplete vaccination and census tract socioeconomic measure was modified by household wealth index (see web appendix 4) and was no longer significant when all interaction terms were added to the multivariate model (table 2).
Incomplete vaccination by 18 months of age and factors associated for children surveyed in 27 Brazilian capital cities, 2007–2008
With the exception of households in census tracts with the highest socioeconomic indicators, higher percentages of children were completely vaccinated in the wealthiest households than in those with the lowest wealth index. However, in census tracts with the highest socioeconomic indicators, the lowest percentage of completely vaccinated children was observed in the wealthiest households (figure 3). The attributable risk of living in the wealthiest households in census tract with the highest indicators was a 5.5% reduction in the frequency of completely vaccinated children compared with the lowest economic stratum (poorest households in census tract with the lowest socioeconomic indicators). On the other hand, frequency of completely vaccinated children was 5.5% higher among children living in the wealthiest households compare with the poorest households in the lowest census tract quintile and were equivalent in the highest and lowest census tract quintiles among children living in households with the lowest wealth indices.

Per cent of children completely vaccinated by 18 months of age by socioeconomic stratum of residence census tract and household wealth index for all 27 Brazilian capital cities, 2007–2008.
When individual vaccines in the recommended immunisation schedule were analysed across all 27 capitals, the same trends were observed towards lower incidence of vaccinated children residing in census tracts in the highest socioeconomic stratum (figure 2). Among 2680 children with incomplete immunisations at 18 months of age, 67.0% were missing only one vaccination, 12.4% were missing two vaccinations and 8.7% had only received one of the vaccines in the recommended schedule. The vaccinations most commonly needed were HepB (42%) and measles–mumps–rubella (38%).
Among recommended vaccines in the primary immunisation series, the combined DTP–Hib vaccine was received by the greatest percentage of children; 93.9% (95% CI 93.2% to 94.5%) had completed the three-dose series by 18 months of age. In four socioeconomic strata (A, B, D and E), we observed significantly lower coverage with the third dose of DTP–Hib vaccine compared with the first DTP–Hib dose. The dropout percentage for DTP–Hib was 3% among children in stratum A versus 1% among children residing in census tracts in lower socioeconomic strata (p<0.01).
Among children surveyed, 91.9% (95% CI 91.3% to 92.6%) had received OPV during the most recent national immunisation day against poliomyelitis. The lowest percentage (84.2%, 95% CI 81.5% to 87.4%) was observed in stratum A; percentages in the other socioeconomic strata were similar. A total of 15.6% of all children received one or more vaccines other than OPV during national immunisation days.
Children who received vaccinations exclusively from public immunisation providers were more likely to be completely vaccinated by 18 months of age than those who received from private providers (OR 1.45, 95% CI 1.22 to 1.72). This association between exclusive use of public services and completing the recommended immunisation schedule by 18 months of age was observed whether children received all vaccinations from the same provider (OR 1.61, 95% CI 1.25 to 2.08) or from more than one provider (OR 1.33, 95% CI 1.03 to 1.72). Overall, 16.0% of children received vaccinations from private providers, with highest percentages in strata A and B (45.7% and 23.2%, respectively) and low percentages in strata C, D and E (13.1%, 6.6% and 4.0%, respectively). The percentage of children surveyed who had received any one of four commercially available vaccines not included in the public immunisation programme was strongly correlated with socioeconomic stratum of residence (figure 4).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Per cent of children who by 18 months of age had received vaccines not included in the national immunisation programme, by socioeconomic quintile of residence census tract (A=wealthiest, E=poorest) in 27 Brazilian capitals. Note: Vaccines not included in the national immunisation calendar were purchased from private immunisation clinics or provided at public referral centres for children with specific medical indications.
Discussion
Socioeconomic inequalities in vaccination coverage have been evaluated by comparing vaccination coverage in the lowest economic quintile with coverage in the highest economic quintile.8 ,9 The 1996 Demographic and Health Survey in Brazil reported the lowest coverage with recommended vaccines among children living in households in the lowest socioeconomic quintile, based on an index of household possessions.10 However, the wealth index used in the Demographic and Health Survey may not be a good proxy for socioeconomic position.11 In the current survey, vaccination coverage was contrasted using area-based socioeconomic measures of socioeconomic status, which had the advantage of providing a representative sample of census tracts according to five socioeconomic strata in each Brazilian capital. We found that census tracts with the best socioeconomic indicators had lower incidence of completely vaccinated children than those with less favourable socioeconomic measures.
While important differences in vaccination coverage were observed when comparing capital cities, results of this survey suggest that Brazil's immunisation programme has been successful in achieving high vaccination coverage among poorer children in urban areas.3 Distribution of wealth in Brazil is extremely unequal. Based on its Gini coefficient, a measure of income inequality, Brazil ranked 11th highest out of 126 countries in 2006.12 On health and quality of life indicators summarised by the Human Development Index, Brazil ranked 70th out of 177 countries. Vaccination coverage for individual vaccines and for complete immunisation series in Brazilian capitals was similar to estimates for the USA,13 with many of the same challenges including geographic heterogeneity, delayed vaccinations and high drop-out rates.14–16 In Italy, the use of combined vaccines and compulsory vaccination strategies has reportedly achieved higher coverage.17 ,18 In the USA, a lower percentage of children living in poverty complete recommended immunisation series than those living at or above the US federal poverty index.13 In many states of India, wide gaps exist between immunisation coverage among the highest and lowest economic quintiles.19 In this survey, we found that Brazilian children living in the poorest census tracts and in households with the fewest number of household possessions had vaccination rates that were equal to or better than those living in better economic conditions.
The complex relationship identified in this survey between area-level socioeconomic indicators and household characteristics calls for further investigation. Children living in the wealthiest households in census tracts with the highest socioeconomic indicators had among the lowest vaccination coverage identified in the survey. However, in census tracts with lower socioeconomic indicators, vaccination coverage was highest among children living in the wealthiest households. These findings are cause for concern.
Consistent with previous studies conducted in São Paulo and other Brazilian cities,3 children in the highest socioeconomic stratum had the lowest incidence of complete vaccination, lowest coverage for several individual vaccines and lowest participation in the most recent national immunisation day. Reductions over the past 30 years in the incidence of vaccine-preventable diseases may be leading to complacency among Brazil's wealthier and more educated population. Higher drop-out rates and lower coverage with three doses of HepB vaccine among children in the highest socioeconomic stratum suggest failure to keep children up-to-date on recommended immunisations, rather than resistance to vaccination.20 However, with reductions in disease incidence and the elimination of childhood diseases such as poliomyelitis and measles, parents may perceive the risk of adverse events associated with vaccination to be greater than the risk of disease. Unfounded claims associating vaccines with autism, multiple sclerosis and a host of other illnesses may have changed Brazilian parents' perceptions of vaccine safety, as has been reported in several more developed countries.21–23 Private providers may also have a conflict of interest in selling vaccines such as inactivated poliovirus and advise parents concerned about the safety of OPV not to take their children to vaccination posts on national immunisation days. Children who do not participate in national immunisation days may miss opportunities to receive vaccines besides OPV offered on these days.24 Paradoxically, parents in Brazilian capitals with the economic means to provide their children with vaccines not included in the national immunisation programme may feel that their children receive too many injections already or that exposure to too many antigens at once may weaken the immune system, attitudes that have been reported from the USA.21
Higher birth order and less maternal education have been associated with not receiving recommended immunisations in other countries.15 ,23 ,25–28 In contrast, factors such as child's race15 living in a single-parent household, mother's employment outside the home15 ,27 and less maternal education23 ,27 were not associated with incomplete vaccination in this study after controlling for other factors. In the USA, use of public health services15 and not having private health insurance16 ,29 have been associated with incomplete vaccination. Among children living in Brazilian capitals, race was not associated with incomplete vaccination and children who received all immunisations from public services were more likely to be up-to-date by 18 months than those who received some or all vaccinations from private providers. This suggests that Brazil's universal vaccination policy has contributed to improved immunisation coverage among poor children.
The study has several limitations. The survey was only conducted in Brazilian capital cities. Data are not generalisable to other urban areas in Brazil or to the approximately 20% of children younger than 5 years living in rural areas. Furthermore, the survey design did not include verification of health centre copies of vaccination records for children included in the survey. The analysis was limited in its ability to separate area-level effects from those of household or family characteristics; multilevel analyses may be needed in future surveys.
Finally, although refusals were uncommon, selected census tracts in the highest socioeconomic stratum had the highest non-completion rate due to parent refusals or inability to find seven eligible children. Vaccination practices in included households may differ from those in households that were not included.
A strength of the survey was that health cards were available for 97% of children surveyed. However, vaccination cards may be incomplete. Multiple sources of data may provide more accurate vaccination histories.30 An advantage of the retrospective cohort design is that it provided information about vaccination coverage among children born in 2005 when they reached 18 months of age.
Despite the high immunisation coverage documented by this survey, there is room for improvement. Maintaining high coverage among children from all groups is important to prevent accumulation of susceptible children. Children in wealthier families may be more likely to travel internationally, thus increasing the risk for exposure to diseases such as measles and poliomyelitis that have been eliminated in Brazil. In a public health system that has been focused on reducing missed opportunities and barriers to access, strategies will be needed to improve acceptance of immunisations in a highly educated and influential segment of the Brazilian population. Engaging private healthcare providers will be critical.
What is already known on this subject
Immunisation coverage among poorer children often lags behind that of wealthier children. While area-level socioeconomic measures have been linked to disease outcomes, few surveys have investigated differences in immunisation coverage among children according to socioeconomic characteristics of census tracts in which they reside.
What this study adds
We present evidence from 27 major cities in Brazil that vaccination coverage among children residing in census tracts with poorest socioeconomic indicators was similar to coverage among children in wealthier census tracts, while coverage lagged among children in the wealthiest 20% of census tracts. This suggests that Brazil has been successful in achieving high levels of immunisation coverage among poor urban children. Strategies are needed to reach children in wealthier areas.
Appendix
Vaccine Coverage Survey 2007 Group
Maria A Veras, Paulo C Castro, Ione A Guibu, Maria J Penon-Rujula, Oziris Simões, Santa Casa Medical School, São Paulo, Brazil; Expedito Luna, Institute of Tropical Medicine, University of São Paulo, São Paulo, Brazil; Deise CC Afonso, Maria CJW Cortes, Elizabeth B Franca, Federal University of Minas Gerais—UFMG, Belo Horizonte, Brazil; Susan M Pereira, Raimunda MC Santos, Public Health Institute, Federal University of Bahia—UFBA, Salvador, Brazil; Silvana GN Gama, Maria C Leal, National School of Public Health, Oswaldo Cruz Foundation—FIOCRUZ, Rio de Janeiro, Brazil; Maria BC Antunes, Pernambuco State University—UPE, Recife, Brazil; Sotero S Mengue, Federal University of Rio Grande do Sul—UFRGS, Porto Alegre, Brazil; Helena A Barbosa, Maria LR Mello, São Paulo State Health Department, São Paulo, Brazil.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Download Supplementary Data (PDF) - Manuscript file of format pdf
Footnotes
↵* Vaccine Coverage Survey 2007 Group are listed in appendix 1.
Funding The vaccination coverage survey was wholly financed by the Brazilian Ministry of Health. The Brazilian national immunisation programme commissioned the survey but played no role in its design, data analysis or preparation of the final report. Results of the survey were presented to the Brazilian Ministry of Health. In several capitals, field staff were recruited from local immunisation programmes and trained as interviewers to conduct fieldwork.
Competing interests None declared.
Ethics approval Research Ethics Committee of Santa Casa Hospital in São Paulo, Brazil.
Provenance and peer review Not commissioned; externally peer reviewed.