Article Text

Abstract
Premature ovarian failure (POF) is the occurrence of amenorrhoea, elevated gonadotrophins and hypoestrogenism in women under 40 years of age. It has important physical and psychological consequences and is increasingly common due to improved survival following treatment for malignancy. Despite this, it remains a poorly understood condition. Here we review the presentation and investigation of POF, discuss recent advances in the management of affected women, and suggest how our knowledge of the condition could be improved.
Statistics from Altmetric.com
Introduction
Premature ovarian failure (POF) is a condition characterised by amenorrhoea, elevated gonadotrophins and sex steroid deficiency, occurring in women under 40 years of age. POF has widespread physical and psychological consequences due to the symptoms and long-term effects of sex steroid deficiency. Furthermore, for many young women the associated reduction in fertility is a devastating diagnosis. Despite this, many gaps remain in our knowledge of the condition. Its underlying aetiology and optimal treatment regimens remain poorly understood and controversy exists regarding its nomenclature. Use of the terms ‘premature ovarian dysfunction’ or ‘primary ovarian insufficiency’ have been suggested as better reflecting the unpredictable nature of ovarian function in this condition, and may be less emotive than the term ‘failure’.1 2
Epidemiology
Accurate estimates of the prevalence of POF are lacking. Spontaneous POF has been estimated to affect 1% of women under the age of 40 years.3 4 Of increasing concern is the rising incidence of iatrogenic POF, although specific data are lacking.5 Improved survival following malignant disease has led to increasing numbers of women experiencing the long-term effects of cancer treatments such as chemotherapy and radiotherapy. Analyses from the Childhood Cancer Survivor Study have found that 6.3% of patients who underwent treatment for cancer developed acute ovarian failure (defined as that occurring during or shortly after treatment).6 Additionally, a further 8% of the cohort went on to develop POF compared to 0.8% of controls.7 At the authors' unit, over one-third of cases of POF are as a result of treatment for cancer (Figure 1), most commonly the haematological malignancies.
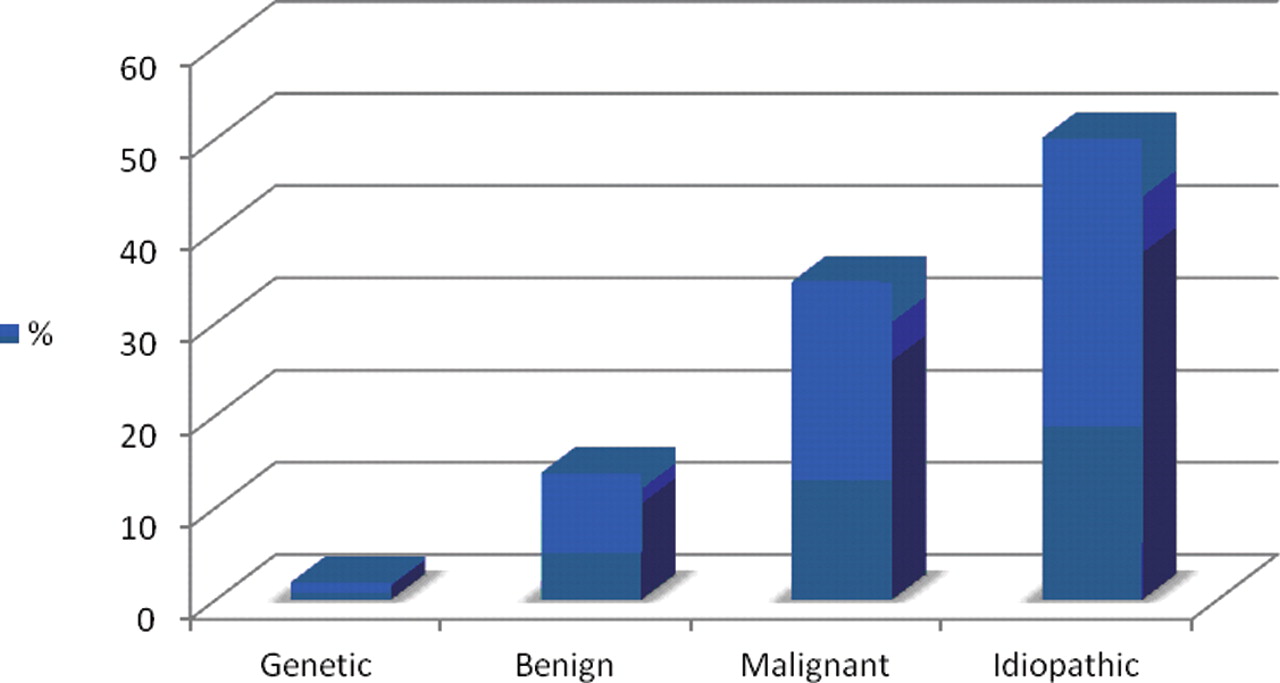
Aetiology of premature ovarian failure cases managed at the West London Menopause and PMS Centre, London, UK.
Key message points
▶ Premature ovarian failure (POF) requires multidisciplinary management to address its complex physical and psychological consequences.
▶ Many factors may influence the presentation of POF. A greater understanding of these may allow a targeted approach to treatment and in turn help improve patient satisfaction.
▶ In the absence of large-scale, prospective randomised controlled trials we must rely on observational data such as patient registries. Long-term follow-up of such registries will facilitate development of evidence-based treatment guidelines.
The risk of POF varies by ethnicity. A cross-sectional survey of 11 652 women in the USA4 found that Caucasian (p=0.02), African-American (p=0.004) and Hispanic (p=0.004) women had significantly increased risk of POF compared to Japanese women. Other factors that influence the risk of POF or early menopause have been identified in a cross-sectional study by Chang et al.8 Cigarette smoking was associated with an increased risk of idiopathic POF [odds ratio (OR) 1.82, 95% CI 1.03–3.23] and certain factors related to ovulation, such as later menarche, irregular menstruation and longer breastfeeding, significantly reduced the risk of POF.8
Aetiology
Ovarian failure can occur by a variety of different mechanisms. There may be reduced peak follicle number, increased atresia of follicles through apoptosis, or failure of follicle maturation. POF can be considered as primary (spontaneous) or secondary (iatrogenic). In the majority of spontaneous cases (90%) no cause is found. However, many factors predisposing to POF have been identified.
Chromosomal
Chromosomal abnormalities are found in around 50% of patients with POF who present with primary amenorrhoea,9 but are much less common in those presenting with secondary amenorrhoea. X chromosome abnormalities are also found more frequently in those patients with a family history of POF. While identifying these abnormalities may have little impact on management, their presence or absence may help family planning decisions in other family members.
Deletions and translocations within the X chromosome have been associated with POF. These usually occur within the Xq13-26 region, which is thought to play a crucial role in ovarian development and function. X monosomy (Turner syndrome) is associated with rapid degeneration of follicles occurring from birth, resulting in POF, often preceding the age of menarche.
Genetic
Around 10–15% of women with spontaneous POF will have a first-degree family relative who is also affected. Obtaining a detailed family history is therefore a crucial part of the initial assessment.
Some 13–26% of women with the FMR1 gene premutation will develop POF and an increasing number of CGG repeats is associated with younger age at menopause.10 The FMR1 gene is the gene responsible for Fragile X syndrome, the most common cause of familial mental retardation. Women with a family history of POF have a higher incidence of the FMR1 premutation (14%) than those with sporadic POF (2%). Screening for the FMR1 premutation is therefore important to identify patients or their siblings who may be at risk of having offspring with the Fragile X syndrome. Other important genetic mutations include those coding for enzymes crucial to reproduction [e.g. 17α-hydroxylase deficiency, follicle-stimulating hormone (FSH) and luteinising hormone (LH) receptor mutations] and others such as gut-associated lymphoid tissue (GALT), eukaryotic translation initiation factor 2B (EIF2B) and forkhead box protein L2 (FOXL2).
Autoimmunity
POF is often found in association with autoimmune disorders, most commonly hypothyroidism (25%), Addison's disease (3%) and diabetes mellitus (2.5%).11 It has also been found in association with the autoimmune polyendocrine syndromes (APS types 1 and 2), systemic lupus erythematosus, pernicious anaemia, rheumatoid arthritis and vitiligo among others.
Antiovarian antibodies are found in around 50% of patients with POF. However the clinical significance of this is unclear due to their high prevalence (31%) in women without POF.12
Infection
POF has also been associated with infections such as mumps, tuberculosis, malaria, varicella, shigella, cytomegalovirus and herpes simplex. Ovarian failure has been shown to occur in 2–8% of women with mumps oophoritis, although it is usually transient.13
Iatrogenic
Of increasing importance are the many women who develop POF after medical treatments. This occurs most commonly following chemotherapy, pelvic irradiation or surgery for malignancy. Risk factors for ovarian failure include older age at treatment, a diagnosis of Hodgkin's lymphoma, exposure to abdominal, pelvic or spinal radiotherapy and certain chemotherapeutic drugs, especially alkylating agents.6 14 A small proportion of cases will be due to surgical treatment of benign gynaecological disorders such as endometriosis or premenstrual syndrome.
Diagnosis and evaluation
Women with POF may present in a variety of ways. Most commonly it is with secondary amenorrhoea or menstrual irregularity and this may or may not be associated with the common symptoms of estrogen deficiency such as hot flushes. A small percentage will present with primary amenorrhoea, in which case an underlying chromosomal cause is more likely. Many factors may influence how women present. Data from the authors' unit has shown that women with a surgical menopause or those with a menopause due to treatment for malignancy are much more likely to be symptomatic. In contrast, women diagnosed before the age of 20 are significantly less likely to experience symptoms of hot flushes and sweats, low mood and vaginal dryness (Figure 2).15
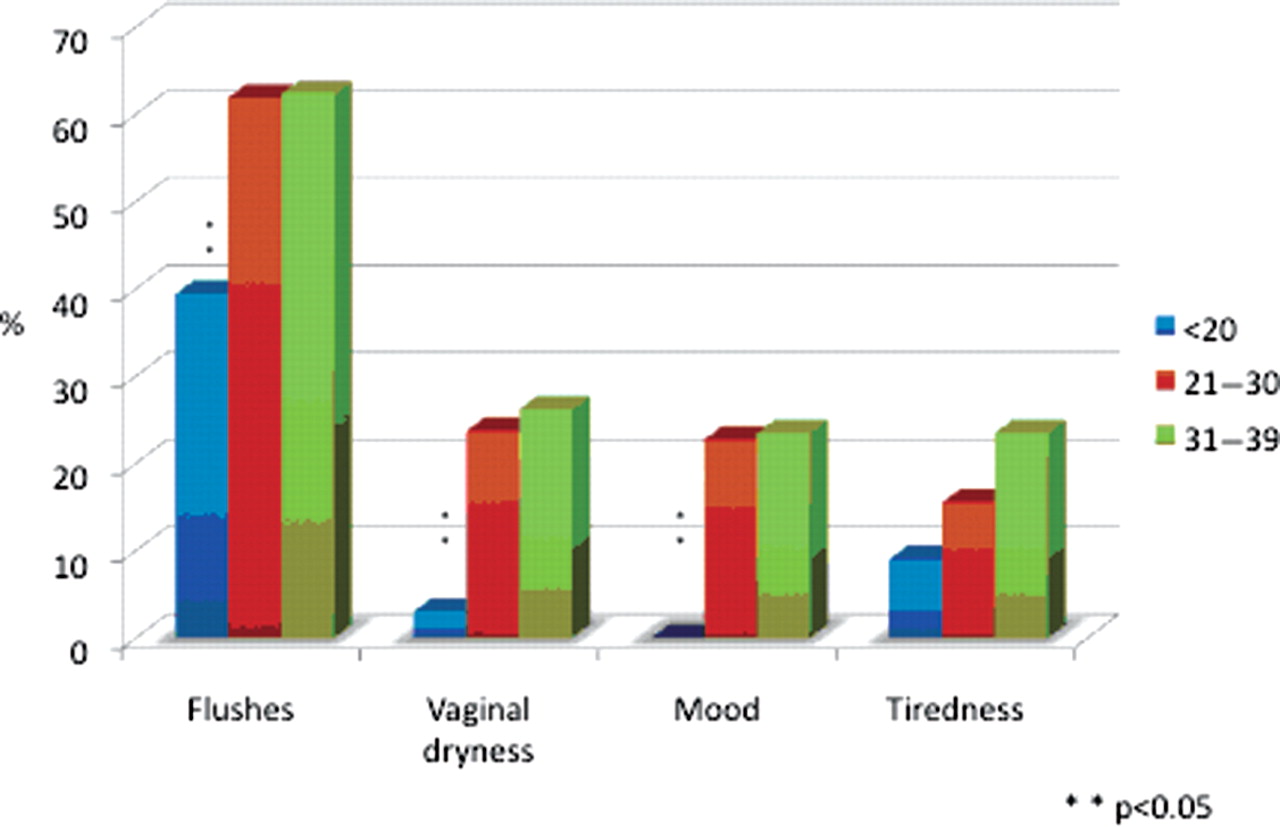
Symptom variation by age for premature ovarian failure cases managed at the West London Menopause and PMS Centre, London, UK.
There is currently a lack of standardised diagnostic criteria for POF, which can often result in diagnostic confusion. One study demonstrated that over 50% of patients with POF had seen at least three clinicians before the diagnosis was made and in 25% the diagnosis took more than 5 years.16 Delayed diagnosis has been cited as one reason why women with POF appear to have low bone density at the time of diagnosis, due to the significant period of oestrogen deficiency that may have occurred.17
It is commonly accepted that estimation of gonadotrophin levels should be performed after 3–4 months of amenorrhoea or menstrual irregularity. If these are within the menopausal range they should be repeated after 4 weeks along with estradiol to confirm hypogonadism. Assessment of thyroid function and prolactin is also recommended to exclude alternative pathology. Pelvic ultrasonography should be considered, as the antral follicle count is severely reduced in POF. We also recommend a baseline assessment of bone density to identify those at greatest risk of osteoporosis.
A further diagnostic tool that is gaining increasing interest is anti-Mullerian hormone (AMH). AMH, produced by developing antral follicles, is currently thought to be the most reliable measure of reduced ovarian reserve and may play a role in predicting age at menopause,18 although further data are required to confirm this. Sowers et al. have shown that the decline of AMH levels to undetectable is highly associated with a time point 5 years prior to the final menstrual period (FMP) (p<0.0001) and that subjects' initial AMH was associated with age at FMP (p<0.035).19 AMH has the advantage that it is not cycle-dependant and can therefore be estimated at any time in the menstrual cycle.
Once the diagnosis has been confirmed, targeted investigations to look for an underlying cause should be considered (Box 1). Karyotyping and screening for the FMR1 gene premutation are especially important in younger patients, or those with a family history of POF or learning difficulties, to exclude an underlying genetic cause. The implications for future pregnancies of any abnormalities such as the Fragile X mutation should be discussed if identified. Auto-antibody screening, for antiadrenal, antiovarian and antithyroid antibodies, is also recommended. This may identify an underlying cause or highlight those patients at increased risk of autoimmune disorders in the future. In those with adrenal auto-antibodies, yearly assessment of adrenal function should be considered as adrenal antibodies confer a 50% risk of developing adrenal insufficiency – a potentially fatal condition.
Box 1 Initial assessment and investigations for premature ovarian failure
▶ Detailed history
Especially for family history of early menopause
▶ Hormone profile
Follicle-stimulating hormone (FSH) and luteinising hormone (LH) levels elevated >30 on two occasions >4–6 weeks apart with estradiol
Thyroid function and prolactin
▶ Autoimmune screen
Antithyroid, antiadrenal and antiovarian antibodies
▶ Karyotyping and genetic analysis
Especially in <30 years or family history
▶ Ultrasound scan
To assess antral follicle count
▶ Dual-energy X-ray absorptiometry (DXA) scan
Estimation of baseline bone mineral density
▶ Anti-Mullerian hormone (AMH) or Inhibin B
Consider for assessment of ovarian reserve
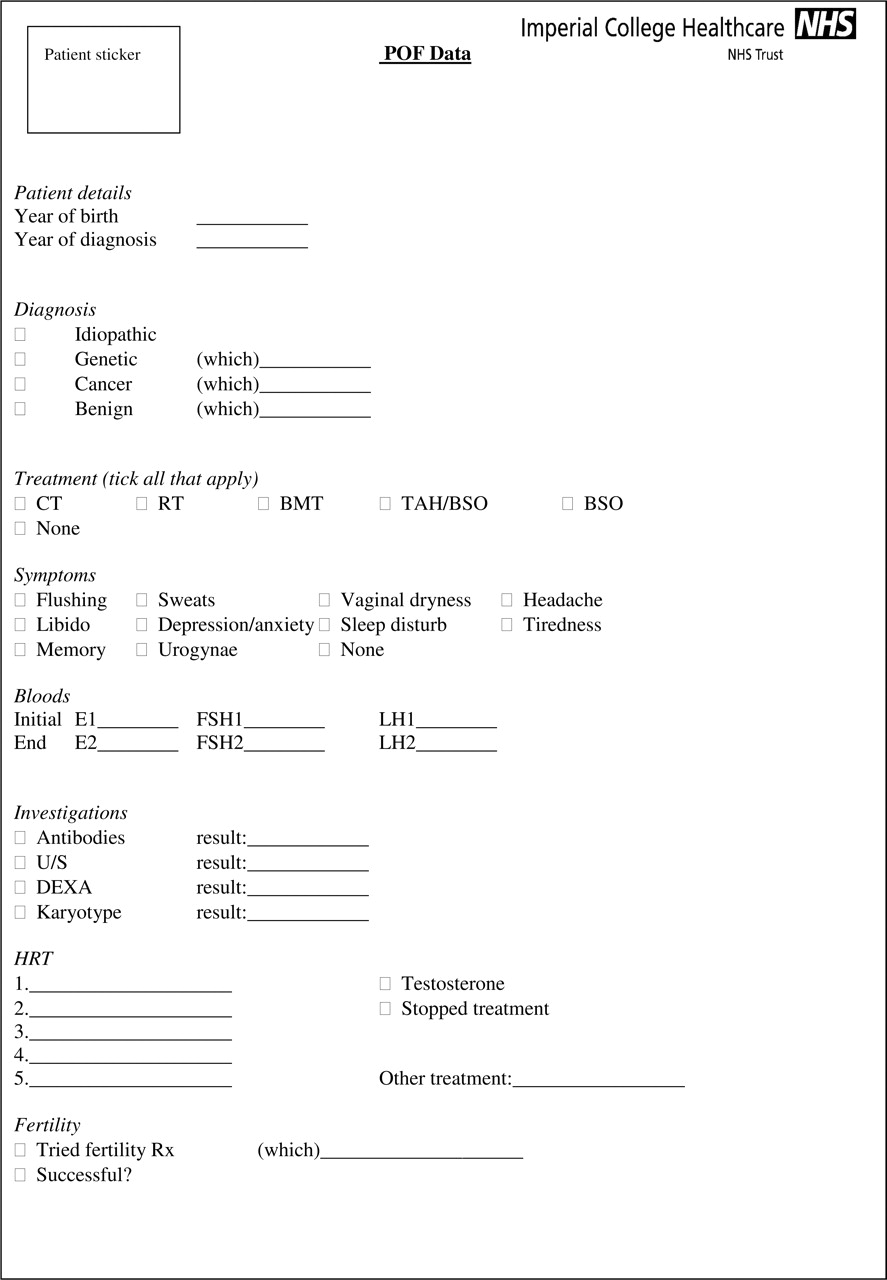
At the West London Menopause and PMS Centre we have developed a proforma that is used to ensure that the correct assessments are performed for all new referrals (Figure 3). This information is then collated into a database, which currently includes details of 330 patients. The database can be used for audit and qualitative research purposes, and we hope to provide much needed long-term follow-up data.
{kind=link}
{kind=link}
{kind=link}
Data proforma used at the West London Menopause and PMS Centre, London, UK for cases of premature ovarian failure (POF).
Management
Women with POF should ideally be managed within specialist multidisciplinary teams to address their complex physical and psychological needs (Box 2).
Box 2 Suggested composition of the multidisciplinary team for the management of premature ovarian failure
General lifestyle and dietary measures should be recommended to all patients, to reduce the risks of development of cardiovascular disease and osteoporosis. The current recommended daily intake of calcium is 1000 mg and of vitamin D is 800 IU and supplementation should be considered, particularly in those with reduced bone density. In addition, regular weight-bearing exercise, minimising smoking and reduction of alcohol and caffeine intake will have beneficial effects. Referral to a dietician should be considered to help patients optimise their dietary intake.
Hormone replacement therapy
It is widely accepted that estrogen replacement should be offered to women with POF to help alleviate the symptoms of estrogen deficiency and to minimise the risks of development of osteoporosis and cardiovascular disease.20 In adolescents, hormone replacement may be required to help induce secondary sexual characteristics. At present, very little evidence exists regarding the optimum method of hormone replacement and options include both the combined oral contraceptive pill (COCP) and hormone replacement therapy (HRT).
Women with POF will typically require higher doses of estrogen than older postmenopausal women. Administration of 100 µg 17β-estradiol by transdermal patch achieves serum estradiol levels equivalent to premenopausal mid-follicular estradiol levels (300–400 pg/ml). Data are lacking regarding the optimal estradiol levels for prevention of the long-term sequelae of POF and therefore these target estradiol levels are based on first principles.
The transdermal route avoids first-pass hepatic metabolism and subsequent effects on clotting factors and triglycerides. However, at present, no evidence exists to support a particular route of administration or treatment regimen and patient choice therefore plays a crucial role. Patients should be made aware that there is no evidence that the results of the Women's Health Initiative (WHI) studies21regarding an increased breast cancer risk with HRT apply to its use in these much younger age groups, where the aim is to provide the hormones that should be present naturally.
In non-hysterectomised women, estrogen therapy must be given in combination with a progestogen to provide endometrial protection. This is usually achieved by administering a progestogen or progesterone in a sequential manner (e.g. micronised progesterone 200 mg daily for 12 days per month). Alternatively, if the patient has been amenorrhoeic for over a year, a continuous combined regimen may be preferred. Data are sparse regarding particular regimens and, as with estrogen administration, patient preference should guide treatment choice.
Women with POF have been shown to have lower androgen levels compared to control groups.22 Consideration therefore should also be given to androgen replacement, especially in those suffering from symptoms of testosterone deficiency, such as reduced libido or lethargy. In the authors' unit, transdermal testosterone patches (Intrinsa®, Warner Chilcott UK Ltd) or subcutaneous implants are used. Transdermal gels may also be used but are currently unlicensed. Serum testosterone levels should be kept within the physiological range to minimise the risks of side effects such as unwanted hair growth and acne.
Close liaison with oncology teams is vital for women who require HRT after malignancy, especially after treatment of hormone-sensitive tumours. There is little evidence regarding the long-term outcomes of HRT use after malignancy and therefore each case should be treated individually. In those with hormone-sensitive tumours, a delay of at least 6–12 months before commencement of HRT may help reduce the risk of recurrence, but further data are needed.
For some women, the COCP will be a more acceptable method of hormone replacement. COCPs deliver synthetic hormones in supra-physiological doses, but women often see the COCP as a simpler and more peer-friendly regimen than HRT. Concerns have been raised about symptom resurgence during the pill-free week. The recent availability of the first 17β-estradiol containing COCP (Qlaira®, Bayer-Schering Pharma) with a reduced hormone-free interval may prove a useful development for the treatment of POF, although clinical trials are needed. Initial studies suggest that the use of 17β-estradiol may have favourable effects on lipid profiles and less impact on haemostasis when compared to ethinylestradiol.23
A randomised controlled trial (RCT) assessing the effects of the COCP and HRT in POF is currently in progress24 and it is hoped that this will provide greater insight into the differences between these methods of hormone replacement.
Contraception
Unpredictable return of ovarian function may occur and spontaneous pregnancies have been observed in 5–10% of women with POF.25 Furthermore, there is evidence that estrogen and progestogen HRT does not prevent ovulation and pregnancy in POF.26 Women using HRT rather than the COCP must therefore be advised to use additional methods of contraception if pregnancy is undesirable. The levonorgestrel intrauterine system (Mirena®) may be used to provide both contraception and endometrial protection in association with estrogen in a continuous-combined HRT regimen, although supporting data for this approach are sparse.
Non-hormonal treatments
In certain circumstances estrogen replacement may be contraindicated or undesirable. Patients with hormone-sensitive malignancies (such as estrogen receptor-positive breast cancer or endometrial cancer) or those at high thromboembolic risk may choose to use non-hormonal treatment options. In these patients, the risks and benefits must be weighed up carefully and an informed decision made. At present there is very little evidence regarding the efficacy of non-hormonal options such as complementary therapies, selective serotonin re-uptake inhibitors (SSRIs), venlafaxine or gabapentin. These may provide some symptomatic relief but will not to act to reduce the long-term effects of estrogen deficiency.
Psychological and psychosexual support
Women with POF have been shown to have increased anxiety, depression and somatisation, with reduced self-esteem and overall life satisfaction compared to control groups.22 27 28 In a cross-sectional descriptive study, 50% of patients with POF requested psychological support, predominantly due to low self-esteem.29 Psychological support therefore forms a vital aspect of the management of these patients. Groups such as The Daisy Network (www.daisynetwork.org.uk) and Women's Health Concern (www.womens-health-concern.org) can help provide valuable support and information, which women can access in their own time.
Another common problem in POF is sexual dysfunction, with reduced sexual well-being, reduced arousal, reduced frequency of sexual encounters and increased pain.22 The development of complex psychological impairment is associated with a younger age at diagnosis.30 Sexual dysfunction should be managed with psychosexual counselling in addition to estrogen and potentially androgen replacement.
Ongoing management
The ongoing management of women with POF includes regular assessment of bone density (usually every 3–5 years) and monitoring of thyroid or adrenal function if antibodies have been identified. Treatment should generally be continued until the average age of the menopause (52 years), with annual review.
Long-term consequences
The mean life expectancy of women with POF has been shown to be 2 years less than that of those reaching the menopause at over 55 years of age,31 and several studies have shown increased mortality among women with POF compared to those with a menopause after the age of 50 years.32 33
Osteoporosis
Women with POF have significantly lower bone density compared to controls,34 35 and this is associated with a significantly higher overall fracture risk.36 There is evidence that the use of HRT for at least 3 years may help reduce subsequent fracture risk.37 No evidence exists for the use of other medications such as bisphosphonates or strontium for preventing osteoporosis in women with POF. Furthermore, there are concerns regarding the use of these agents in POF due to unknown effects on fetal development should spontaneous pregnancy occur.
Analysis of patients from the authors' unit has shown that at the time of diagnosis 27.7% of patients have osteopenia and 3.8% have osteoporosis.15 Reduced bone density was significantly more frequent in those with idiopathic and malignant aetiologies compared to benign aetiologies such as surgical management of menorrhagia, endometriosis or premenstrual syndrome. Further analysis is required but this may be a reflection of the differences in time to diagnosis and subsequent duration of hypoestrogenism. Additionally, it may be that a larger proportion of idiopathic and malignant aetiologies are in young women who may not have achieved their peak bone density by the time of development of POF.
Cardiovascular disease
A significantly increased risk of cardiovascular disease has been demonstrated in women with POF, with an estimated 80% increased risk of mortality from ischaemic heart disease in those with a menopause under the age of 40 years compared to those with menopause at 49–55 years.38 This risk of ischaemic heart disease was more pronounced in those who had never used estrogens.
POF has been associated with several risk factors for the development of cardiovascular disease including impaired endothelial function,39 adverse effects on the lipid profile,40 reduced insulin sensitivity41 and the metabolic syndrome.42 The observation that reduced ovarian reserve, as reflected by elevated serum FSH on Day 3 of the menstrual cycle, is associated with increased cholesterol and low-density lipoprotein (LDL) cholesterol,43 suggests that factors other than estrogen deficiency may alter cardiovascular risk in POF.
There is no clear evidence as to whether HRT in women with POF reverses this risk of cardiovascular disease. The vascular endothelium plays a crucial role in regulating vascular tone, thrombogenesis and fibrinolysis, and endothelial dysfunction is often considered as a precursor to atherosclerosis. Kalantaridou et al.39 demonstrated that women with POF have impaired endothelial function and that this impairment was reversed by estrogen replacement. Whether this translates into long-term reduction of cardiovascular mortality remains unknown.
Cognitive impairment
It has been suggested that patients with POF may be at increased risk of dementia or reduced cognitive function. The Mayo Clinic Cohort Study of Oophorectomy and Aging investigated the risk of cognitive impairment and Parkinsonism in women undergoing premenopausal oophorectomy. They demonstrated that women who underwent either unilateral or bilateral oophorectomy before the onset of the menopause had an increased risk of cognitive impairment or dementia44 and Parkinsonism45 compared to controls and that this risk increased with younger age at oophorectomy. They also demonstrated a protective role for oestrogen replacement in women with bilateral oophorectomy when taken until at least 50 years of age. Further data are needed, specifically in POF patients with non-surgical aetiology, to quantify these risks of cognitive impairment more accurately.
Fertility
Ovarian function can return intermittently in up to 50% of patients with POF and this can occasionally lead to ovulation and pregnancy. For most women wishing to conceive, in vitro fertilisation (IVF) with donor oocytes confers the highest chance of successful pregnancy, with success rates of 40–50% per cycle. A significant problem, however, is the availability of donor eggs, primarily because of restrictions on paying donors in the UK.
In patients with some remaining ovarian reserve at the time of diagnosis, ovulation induction with timed intercourse or intrauterine insemination may be an option. There is evidence to suggest that the success rate of ovulation induction with exogenous gonadotrophins may be improved by pre-treatment with estrogen, by lowering FSH levels.46 There have also been recent case reports about the use of 5-dehydroepiandrosterone (DHEA) leading to ovulation and spontaneous pregnancies in POF.47
For women who require treatment for malignancy or have a strong family history of POF, other options may exist. Some of these methods currently have little evidence base although they provide promise for the future of fertility treatment in POF.
Preservation of ovarian function may be achieved via ovarian transposition prior to radiotherapy. This is usually done laparoscopically and can greatly reduce radiation exposure of ovarian tissue.
Cryopreservation techniques have received much interest in recent decades as they provide a potential means of preserving fertility in patients requiring chemotherapy. Of these, embryo cryopreservation is probably the most successful approach and pregnancy rates of about 20–30% per transfer of two or three embryos have been reported, depending on the age of the patient.48 However for some patients, the requirement for ovarian stimulation may result in an unacceptable delay of 2–3 weeks before treatment of their malignancy can commence.
Oocyte cryopreservation is a potential option for women without a partner or who do not wish to use donor sperm. Technical advances in oocyte preservation such as vitrification have improved live birth rates following freezing of mature eggs.49 Concerns exist over the fragility of the oocytes, and although success rates are improving they remain low.50
Cryopreservation of ovarian tissue and later transplantation is still largely experimental, although spontaneous pregnancies resulting in live births have been reported.51 52 The rationale for this approach is that primordial follicles in excised ovarian tissue may be more resistant to freezing and thawing than mature oocytes and the tissue may therefore be collected and preserved without imposing a delay in treatment.
Conclusions and future goals
POF remains a poorly understood condition with complex physical and psychological morbidity. Its management requires an ongoing multidisciplinary approach as different problems may manifest at different stages in a woman's life. Despite recent advances in terms of available hormonal and fertility treatments, many questions remain unanswered.
Further research is urgently needed to aid the development of evidence-based treatment guidelines and to determine the optimum regimens to reduce the long-term consequences. The inherent difficulties with large-scale studies in this population have led to calls for an international patient registry,53 which would play a vital role in providing large-scale follow-up of these women. In the authors' unit a database of all POF patients is kept, which provides a useful tool for retrospective research and audit. In the absence of large-scale RCTs, we hope that national and international collaboration of data will contribute to meaningful research.
References
Footnotes
-
Competing interests None.
-
Provenance and peer review Commissioned; externally peer reviewed.