Article Text

Abstract
Purpose Immunotherapy has shown activity in patients with brain metastases (BM) and leptomeningeal disease (LMD). We have evaluated LMD and intraparenchymal control rates for patients with resected BM receiving postoperative stereotactic radiosurgery (SRS) and immunotherapy or postoperative SRS alone. We hypothesize that postoperative SRS and immunotherapy will result in a lower rate of LMD with acceptable toxicity compared with postoperative SRS.
Patients and methods One hundred and twenty-nine patients with non-small-cell lung cancer (NSCLC) and melanoma BM who received postoperative fractionated SRS (fSRS; 3×9 Gy) in combination with immunotherapy or postoperative fSRS alone for completely resected BM were retrospectively evaluated. The primary endpoint of the study was the rate of LMD after treatments. The secondary endpoints were local failure, distant brain parenchymal failure (DBF), overall survival (OS), and treatment-related toxicity.
Results Sixty-three patients received postoperative SRS and immunotherapy, either nivolumab or pembrolizumab, and 66 patients received postoperative SRS alone to the resection cavity. With a median follow-up of 15 months, LMD occurred in 19 patients: fSRS group, 14; fSRS and immunotherapy, 5. The 12-month LMD cumulative rates were 22% (95% CI 14% to 37%) in the fSRS group and 6% (95% CI 2% to 17%) in the combined treatment group (p=0.007). Resection cavity control was similar between the groups, whereas DBF and OS were significantly different; the 1-year DBF rates were 31% (95% CI 20% to 46%) in the fSRS and immunotherapy group and 52% (95% CI 39% to 68%) in the fSRS group; respective OS rates were 78% (95% CI 67% to 88%) and 58.7% (95% CI 47% to 70%). Twenty-two patients undergoing postoperative fSRS and immunotherapy and nine subjected to postoperative fSRS experienced treatment-related imaging changes suggestive of radiation-induced brain necrosis (p=0.02).
Conclusions Postoperative fSRS in combination with immunotherapy decreases the incidence of LMD and DBF in patients with resected BM from NSCLC and melanoma as compared with fSRS alone, reducing the rate of neurological death and prolonging survival.
- radiotherapy
- immunotherapy
- central nervous system neoplasms
- brain neoplasms
Data availability statement
Data are available upon reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
Surgical resection is often performed in patients with larger brain metastases (BM) causing mass effect, with a reported 1-year local control of 50%–60%, which is significantly increased with the use of postoperative radiation.1–5 Historically, whole brain radiation therapy (WBRT) has been the cornerstone for treatment of resected BM, with a reduced risk of local recurrence from 46%–59% to 10%–28% and incidence of new lesions from 37%–42% to 14%–23%.1 Postoperative stereotactic radiosurgery (SRS) to the surgical bed has been increasingly employed as an alternative to WBRT with the aim of avoiding the risk of the detrimental neurocognitive effects associated with WBRT; several retrospective and prospective studies reported local control and overall survival (OS) rates of 70%–90% and of 50%–70%, respectively, at 1 year following SRS given in one or few fractions.2–14 Data from two randomized trials5 10 have demonstrated that postoperative SRS significantly improves local control compared with observation alone in patients with resected BM,3 while decreasing the risk of cognitive decline as compared with WBRT, without diminishing survival.10
The most feared adverse effects of combined surgery and SRS include the risk of developing leptomeningeal disease (LMD) and radiation-induced brain necrosis (RN).15 According to the recent guidelines of the European Association of Neuro-Oncology (EANO) and the European Association for Medical Oncology (ESMO),16 LMD is classified as linear, nodular, or both based on magnetic resonance image (MRI) patterns, and its development is presumably related to iatrogenic dissemination of tumor cells into the cerebrospinal fluid and meninges at the time of resection. Large retrospective series report a 1-year rate of LMD up to 31% after postoperative SRS of resected BM.5 12 14 17–19 A finding emerging from published studies is a peculiar pattern of nodular LMD in postoperative setting, characterized by new focal extra-axial enhancing lesions adherent to the dura or pia often adjacent to the surgical cavity, also referred as pachymeningeal enhancement.20–22 Another significant adverse effect of the treatment is the development of symptomatic RN after SRS, with an estimated risk for either resected or intact BM ranging from 3% to 22%.6–14
Immunotherapy with programmed cell death 1/programmed cell death-ligand 1 (PD-1/PD-L1) or cytotoxic T-lymphocyte antigen-4 checkpoint inhibitors, given alone or in combination, has shown intracranial activity in patients with BM from melanoma and non-small-cell lung cancer (NSCLC).23–25 In a randomized phase II study of 60 patients with melanoma BM receiving combined nivolumab and ipilimumab or nivolumab alone, Long et al24 showed 6-month intracranial progression-free survival (PFS) and OS rates of 35% and 68%, respectively, in patients receiving nivolumab, and 53% and 78%, respectively, in those receiving nivolumab and ipilimumab. Recent systematic reviews and meta-analyses have suggested that the combination of SRS with immunotherapy offers improved intracranial control and survival compared with SRS alone, although a higher risk of RN has been reported in some studies.26 27 Of note, a small prospective trial showed activity of pembrolizumab, 200 mg intravenously every 3 weeks, in patients with LMD from solid tumors. With a 3-month OS rate of at least 43% as the primary endpoint, Brastianos et al28 showed a 3-month survival rate of 60%.
These findings provide the rationale for exploring the potential impact of postoperative SRS to the resection cavity in combination with immunotherapy on the development of LMD. With this intent, we have retrospectively compared the clinical outcome of postoperative SRS with immunotherapy or SRS alone in a series of patients with resected BM from melanoma and NSCLC. The primary endpoint of the study was the rate of LMD following treatments. The secondary objectives were local failure (LF), distant brain failure (DBF), OS, cause of death, and risk of RN.
Patients
Between June 2014 and October 2020, 154 consecutive patients ≥18 years old who received complete resection of at least one BM followed by adjuvant fractionated SRS (fSRS; 3×9 Gy) with or without immunotherapy were retrospectively evaluated. Radiographic, surgical, and pathological information was collected from a prospectively maintained database of patients with brain tumors treated at University of Pittsburgh Medical Center (UPMC) Hillman Cancer Center and Istituto di Ricovero e Cura a Carattere Scientifico (IRCCS) Neuromed. Twenty-five patients were excluded for the following reasons: insufficient clinical information at follow-up (n=3), prior WBRT (n=6), incomplete resection (n=5), previous use of anti-PD-1/PD-L1 (n=4), or different radiation schedules (n=7). Previous systemic therapies, including ipilimumab, BRAF/MEK (v-raf murine sarcoma viral oncogene homolog B1/mitogen-activated extracellular signal-regulated kinase) inhibitors, epidermal growth factor receptor tyrosine kinase inhibitors (EGFR TKI), and anaplastic lymphoma kinase (ALK) inhibitors, were allowed. A total of 129 patients with 135 BM were finally analyzed. According to the study design, immunotherapy consisted of the PD-1 inhibitors nivolumab and pembrolizumab; both drugs have been approved by the Italian Medicines Agency for treatment of metastatic melanoma and NSCLC during the period 2016–2017. Then, postoperative SRS alone was the prominent radiation treatment until 2017 (fSRS, 47; fSRS and immunotherapy, 27), while combined treatment was increasingly used over fSRS alone during the period 2017–2020 (fSRS, 19; fSRS and immunotherapy, 36). All patients provided written consent to the treatment.
Treatment
All lesions were treated with frameless linear accelerator-based SRS using a commercial stereotactic mask fixation system (Brainlab). Target volumes were contoured on postcontrast thin-slice (0.5–0.8 mm) gadolinium-enhanced T1-weighted axial MRI sequences fused to the treatment planning CT, with slices in thickness and spacing of 0.625 mm acquired throughout the entire cranium.
The gross tumor volume (GTV) was delineated as the edge of the resection cavity, with no inclusion of the surrounding areas of edema and the surgical resection corridor. To account for microscopic disease, the clinical target volume (CTV) was contoured by adding a margin of 1 mm around the resection cavity with an additional margin of 5 mm over the craniotomy bone flap adherent to the underlying dura for lesions presenting with preoperative dural contact. An additional margin of 1 mm was added around the CTV to generate the planning target volume (PTV). For patients presenting with multiple lesions, the PTV for intact lesions was generated by 1 mm expansion around the GTV.
All resection cavities were treated with a total dose of 27 Gy given in three fractions over 3 consecutive days. Doses were usually prescribed to the 80% isodose line to achieve a minimum 95% target coverage of the prescribed dose. The treatment was performed with a TrueBeam (Varian Medical Systems) or a Novalis TrueBeam STx (Brainlab and Varian Medical Systems) by using dynamic conformal arc or volumetric modulated arc therapy. Cone-beam CT and the ExacTrac image-guided systems were used for set-up verification before and during each fraction. For patients presenting with multiple BM, intact lesions were treated with single-fraction SRS, 18–22 Gy, or fSRS, 3×9 Gy. For patients undergoing fSRS, dexamethasone therapy was started by the first day of treatment at a maximum dose of 4 mg per day and maintained for 5–7 days after the end of treatment.
Concurrent immunotherapy started before or after a few days of receiving fSRS and consisted of intravenous nivolumab (3 mg/kg every 2 weeks) or pembrolizumab (200 mg every 3 weeks) until definitive progression, unacceptable toxicity, and patient or physician decision.
Post-treatment follow-up
Patients were examined clinically before treatment and then every 2 months. For clinical follow-up, a detailed neurological examination was performed, and the severity of complications was rated according to the Common Terminology Criteria for Adverse Events V.6.0.
LF was defined as the development of new nodular contrast enhancement within the resection cavity (infield recurrence within the 80% isodose line), and DBF by the presence of new parenchymal BM. According to the EANO-ESMO guidelines, LMD was defined by MRI as linear LMD (type IIA), nodular LMD (≥5 × 10 mm in orthogonal diameter; type IIB), or both (type IIC), typically involving the cerebral sulci, cerebellar folia, basal cisterns, spinal cord, cauda equina, and dural/pial surface, or neither (no imaging evidence). Examples of different types of LMD occurring in two patients with a resected BM are shown in figure 1. LMD was confirmed by a team consisting of two neurosurgeons (VE and SP), a neuroradiologist (AB), and a radiation oncologist (GM) who reviewed all neuroimages. Cytological confirmation of malignant cells in the cerebrospinal fluid was generally performed for patients without typical MRI findings. Pseudoprogression was defined as ≥25% increase in tumor contrast enhancement and edema occurring within 6 months from SRS which resolved or stabilized during the subsequent follow-up.29 For all patients who died, the cause of death (intracranial vs extracranial progression) was determined by clinical/neurological evaluation and brain/systemic radiological studies. Patients were considered to have died of neurological death if they had evidence of progressive intracranial disease consisting of expanding intracranial masses, central nervous system (CNS) hemorrhage, progressive neurological symptoms, and LMD.
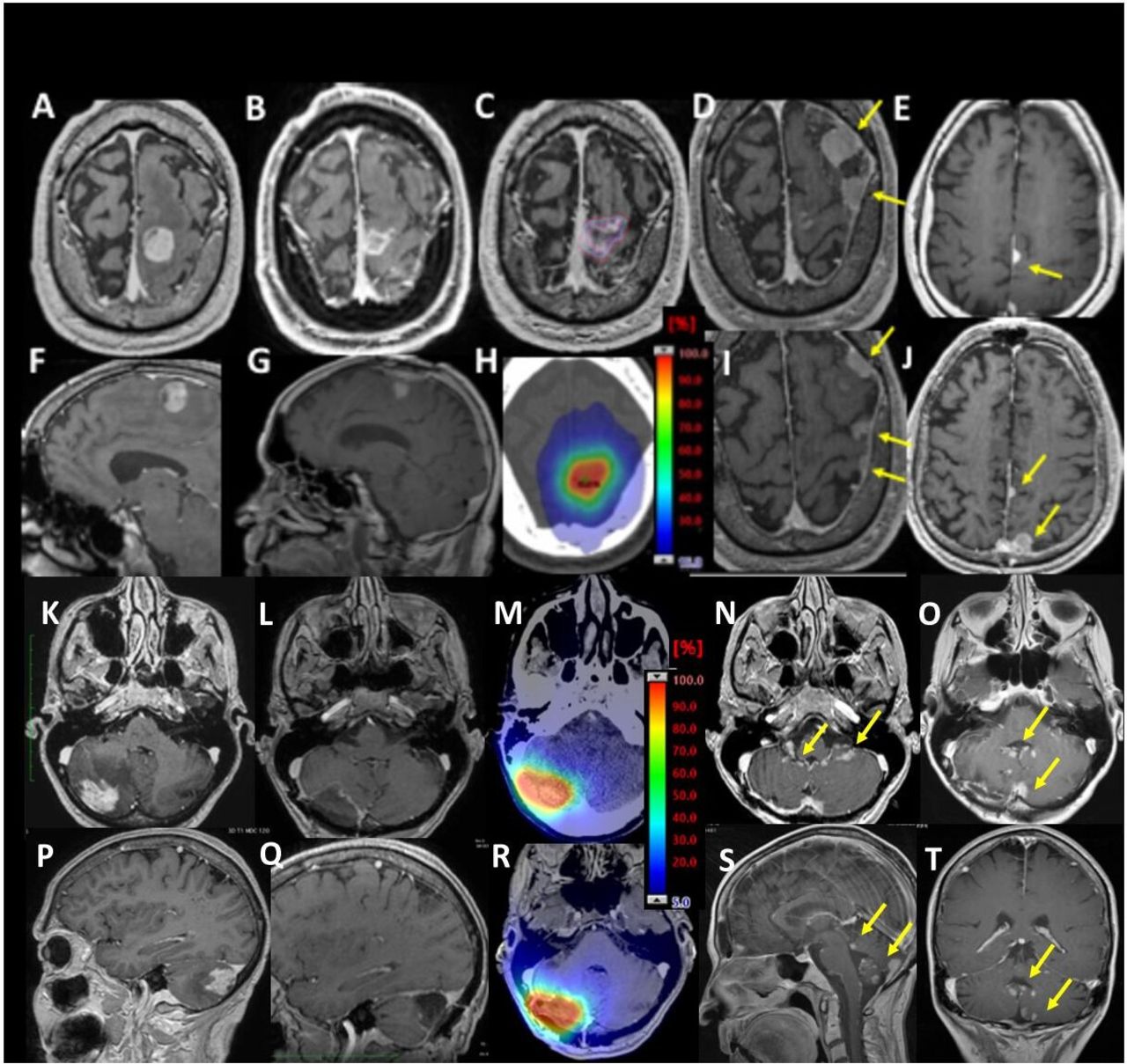
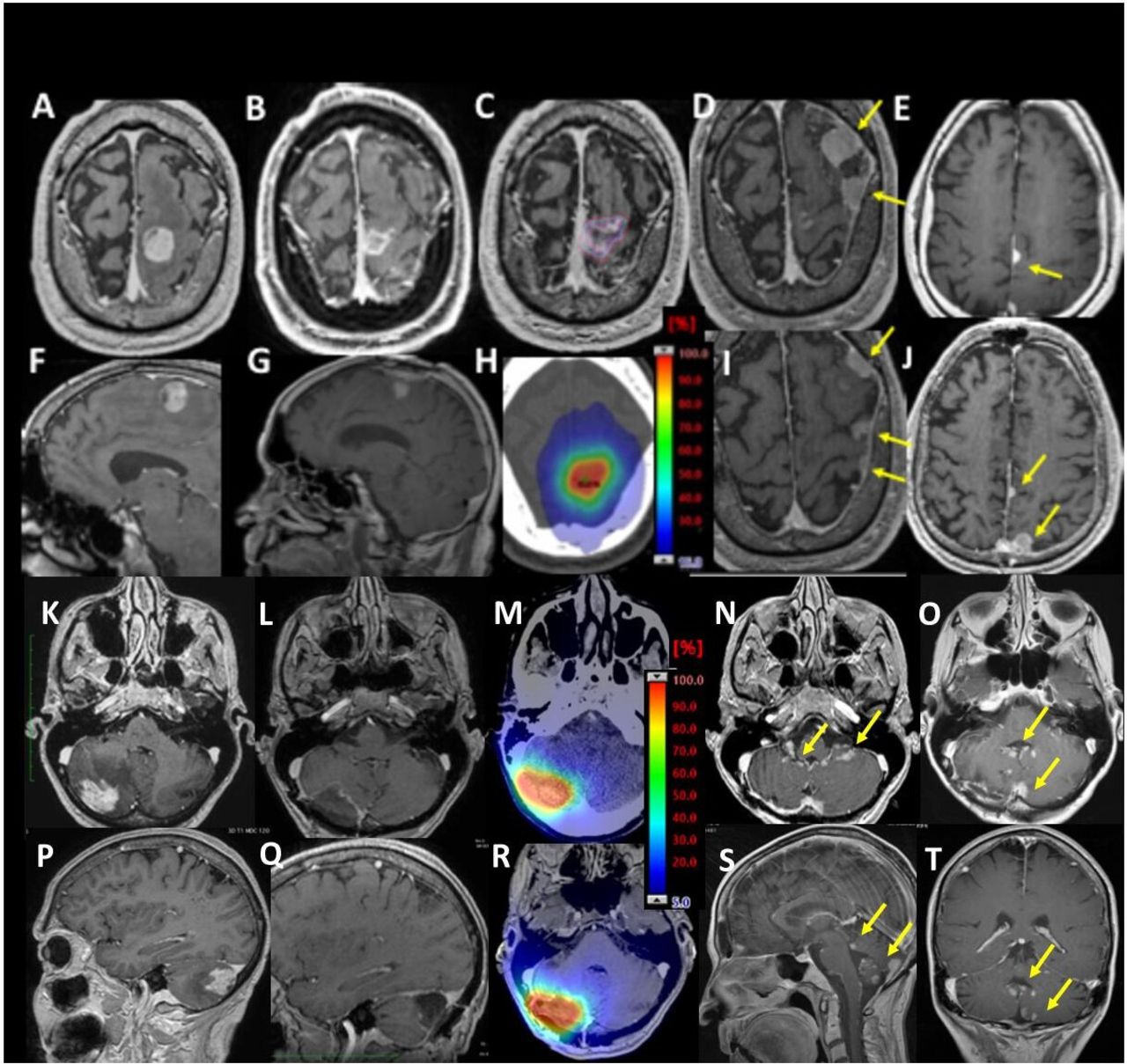
Two examples of LMD cases after postoperative stereotactic radiosurgery to the resection cavity. Patient 1: sagittal (upper panels) and axial (lower panels) T1-weighted gadolinium-enhanced MRI scans of a large melanoma brain metastasis before (A, F) and after (B, G) surgical resection. Four weeks after surgery, the patient received postoperative fSRS (3×9 Gy);panel C and H show details of target delineation and prescription isodose lines. Follow-up MRI scans show cavity control 9 months after treatment; however, the patient developed type IIB LMD, characterized by the presence of several nodules adherent to the dura near the site of the cavity (yellow arrows in D, E, I and J). Patient 2: sagittal (upper panels) and axial (lower panels) T1-weighted gadolinium-enhanced MRI of a large NSCLC cerebellar brain metastasis before (K, P) and after (L, Q) surgical resection. Details of selected prescription isodose lines are shown in M and R. Six months after postoperative fSRS to the surgical bed, follow-up MRI shows the presence of type IIC LMD, as defined by the presence of both linear and nodular leptomeningeal enhancement in the cerebellum (yellow arrows; axial view: N, O; sagittal view: S; coronal view: T). fSRS, fractionated stereotactic radiosurgery; LMD, leptomeningeal disease; NSCLC, non-small-cell lung cancer.
Diagnoses of tumor progression or RN were determined on the basis of histological findings (for patients who underwent surgical resection) or by imaging using magnetic resonance and F-DOPA (3,4-dihydroxy-6-(18)F-fluoro-l-phenylalanine) positron emission tomography (PET/CT), which resulted in a sensitivity and specificity of 90% and 92.3%, respectively, as previously reported.30
Statistics
OS was estimated using the Kaplan-Meier method calculated from the time of fSRS. The cumulative incidence of LMD rates was obtained with death as a competing risk. In addition, competing risk analysis was used to evaluate cavity LF, DBF, and risk of RN. Patients who did not experience an event were censored at the time of the last follow-up. Gray’s test was used to test for differences in the cumulative incidence of groups. Fisher’s exact test and non-parametric Mann-Whitney test were used to compare categorical characteristics of targets among different groups. Univariate and multivariate analyses were performed using the Cox proportional hazards regression model to assess the effects of clinical and treatment variables on outcomes. P<0.05 was considered statistically significant. Variables at significance levels of p<0.1 were included in the multivariate analysis. Statistical evaluation was performed using a commercial statistical software package (XLSTAT statistical software).
Results
Patient and treatment characteristics
Between March 2014 and September 2020, a total of 129 patients who met the inclusion criteria were analyzed. Patients and tumor characteristics are summarized in table 1. For their surgical cavities, 63 patients received fSRS and immunotherapy and 66 patients received fSRS alone. Among patients treated with fSRS and immunotherapy, 49 received nivolumab and 14 received pembrolizumab. Thirty-eight patients started immunotherapy after fSRS at a median interval of 7 days (range 2–28 days) and 25 patients before fSRS at a median interval of 5 days (range 2–10 days). Among patients receiving fSRS alone, subsequent systemic therapy included chemotherapy, BRAF/MEK inhibitors (n=3), ipilimumab (n=4), EGFR TKI (n=6), and ALK inhibitors (n=2). Baseline characteristics were similar between the two groups in terms of age, histology, Karnofsky performance status (KPS) scores, resection cavity volume, number of metastases, diagnosis-specific graded prognostic assessment score (DS-GPA),31 EGFR and BRAF mutations, and number of BM. The median pretreatment neutrophil lymphocyte ratio was 3.2 in the fSRS group and 2.8 in the combined group (p=0.18), being ≥5 in 21 (32%) and 15 (24%) patients (Fisher’s exact test, p=0.3). Seventy-eight patients received one or two lines of therapy prior to postoperative fSRS. All patients received the planned dose (3×9 Gy) to the resection cavity with the PTV that was covered by at least 95% of the prescription dose. The mean conformity index (volume covered by reference dose/PTV) was 1.41±0.2. The median time period from surgery to fSRS was 24 days, with 90% of patients receiving fSRS within 30 days of surgery. In 72 patients presenting with multiple BM, single-fraction SRS was used for 94 lesions and fSRS for 25 lesions. At the time of analysis, 31 patients were still alive (fSRS and immunotherapy, 19; fSRS, 12). Data were reported to June 2021.
Patient characteristics and treatment parameters
Leptomeningeal disease
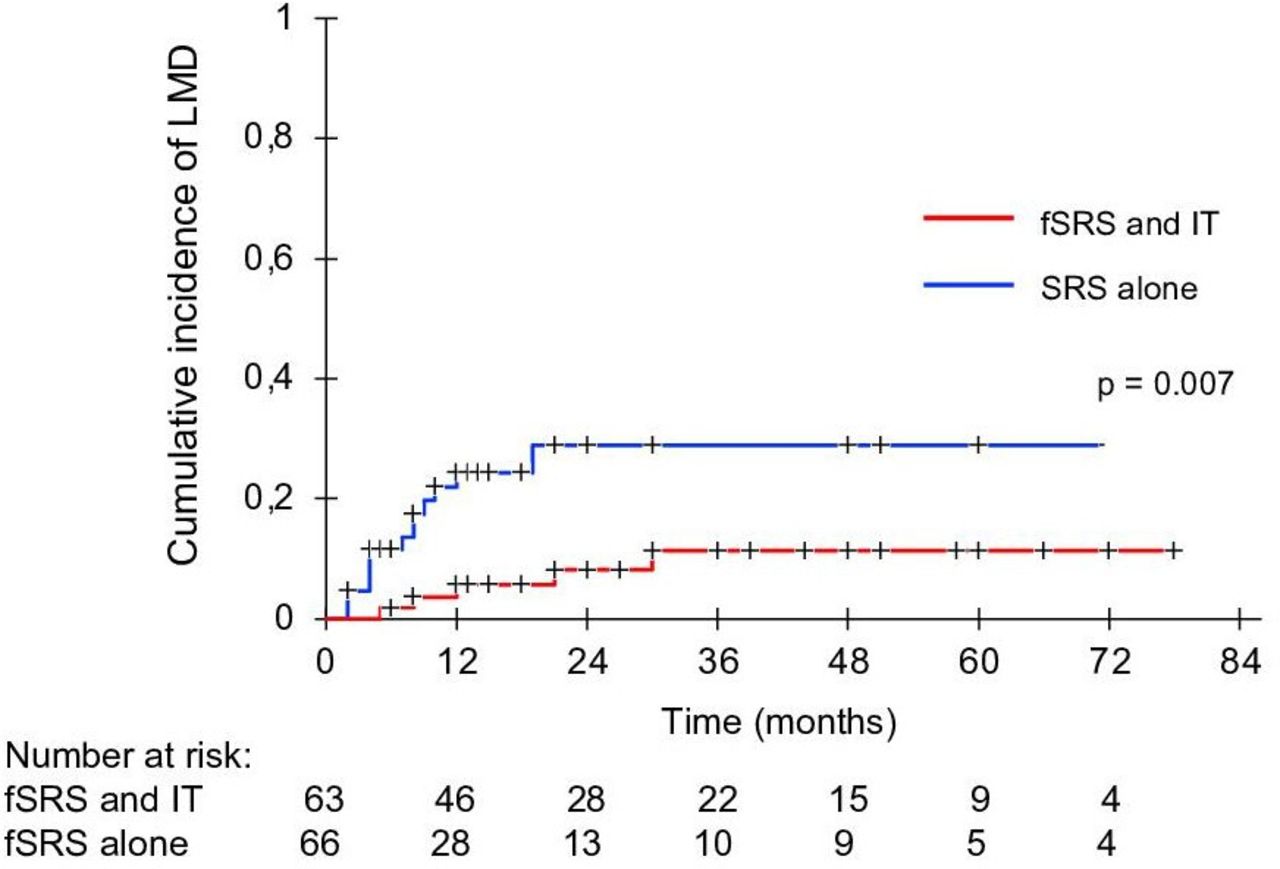
With a median follow-up of 15 months (37 months for alive patients), LMD occurred in 19 of 129 patients (14.7%) at a median time of 5 months (range 2–33 months) after surgical resection. Fourteen patients in the fSRS group and five patients in the fSRS and immunotherapy group developed LMD (Fisher’s exact test, p=0.04), as suggested by imaging (n=19), symptoms (n=13), and cerebrospinal fluid (CSF) cytology (n=4). The 1-year and 2-year LMD cumulative rates were 22% (95% CI 14% to 37%) and 30% (95% CI 18% to 49%), respectively, in the fSRS group, and 6% (95% CI 2% to 17%) in the fSRS and immunotherapy group (p=0.007) (figure 2). Based on MRI findings, the pattern of LMD was nodular in 11 patients, linear in 2 patients, and both in 6 patients. Diagnosis of LMD was confirmed by CSF analysis in 4 patients (type A, 1; type C, 3). Among patients with nodular pattern, LMD was seen as dura-arachnoid focal enhancing lesions adjacent to the resection cavity in 11 patients. Salvage treatments included WBRT (n=9), SRS (n=8), chemotherapy (n=4), targeted therapy (n=3), and immunotherapy (n=3), given alone or in combination. For the entire cohort, the median survival time from the time of diagnosis of LMD was 13 months (range 1–33 months).

Cumulative incidence of LMD in patients receiving postoperative fSRS alone or in combination with IT to resected brain metastases. Patients receiving fSRS and IT had a lower risk of developing new meningeal metastases after surgical resection. fSRS, fractionated stereotactic radiosurgery; IT, immunotherapy; LMD, leptomeningeal disease; SRS, stereotactic radiosurgery.
In the univariate analysis, no factors were associated with the development of LMD, including histology (NSCLC vs melanoma), size of lesion (≥3 cm vs <3 cm), type and timing of immunotherapy, number of BM, location (posterior fossa vs supratentorial location), proximity to the pial surface (<1 cm), and en bloc vs piecemeal resection; however, location in the posterior fossa (p=0.1) and en bloc resection (p=0.07) showed a trend toward reduced risk of LMD: the 1-year rates were 24% and 14%, respectively, for posterior fossa lesions versus other locations, and 26% and 13%, respectively, with piecemeal resection versus en bloc resection.
LF, distant parenchymal failure, and OS
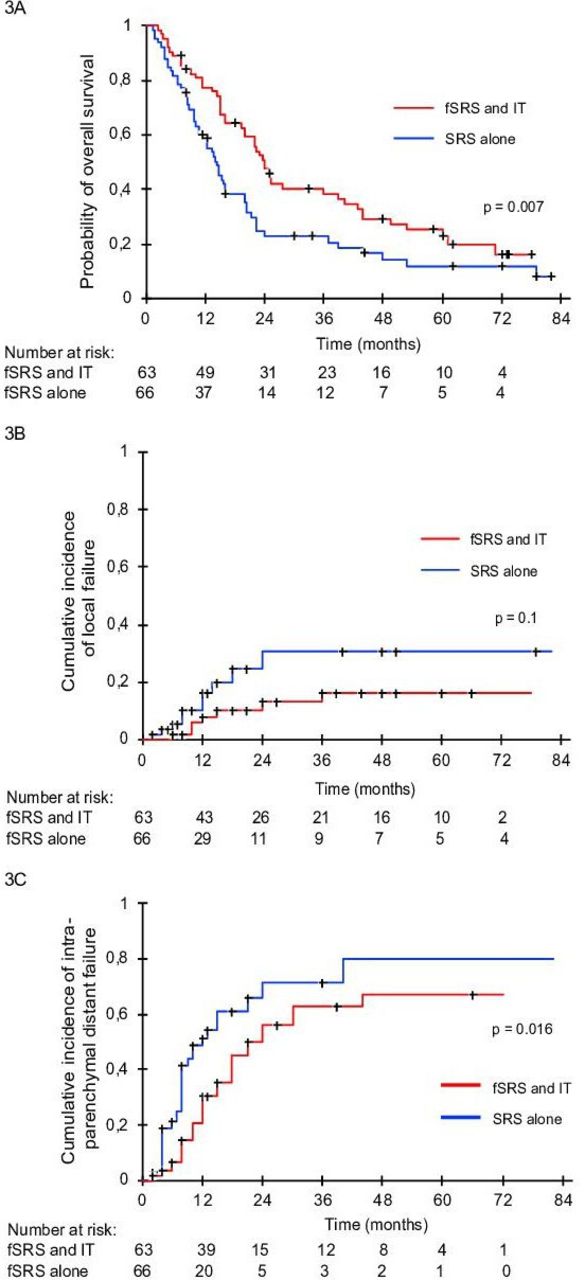
LF analysis demonstrated no significant differences between the groups. The 1-year and 2-year LF rates were 8% (95% CI 3% to 18%) and 13% (95% CI 7% to 24%), respectively, in the fSRS and immunotherapy group, and 16% (95% CI 8% to 31%) and 30% (95% CI 16% to 43%), respectively, in the hypofractionated stereotactic radiotherapy (HSRT) group (p=0.15) (figure 3A). Failure within the resection cavity was seen in 7 patients receiving combination treatment and in 10 patients receiving fSRS alone, with a median time to LF of 12 months (range 2–24 months) and 8 months (range 6–36 months), respectively.
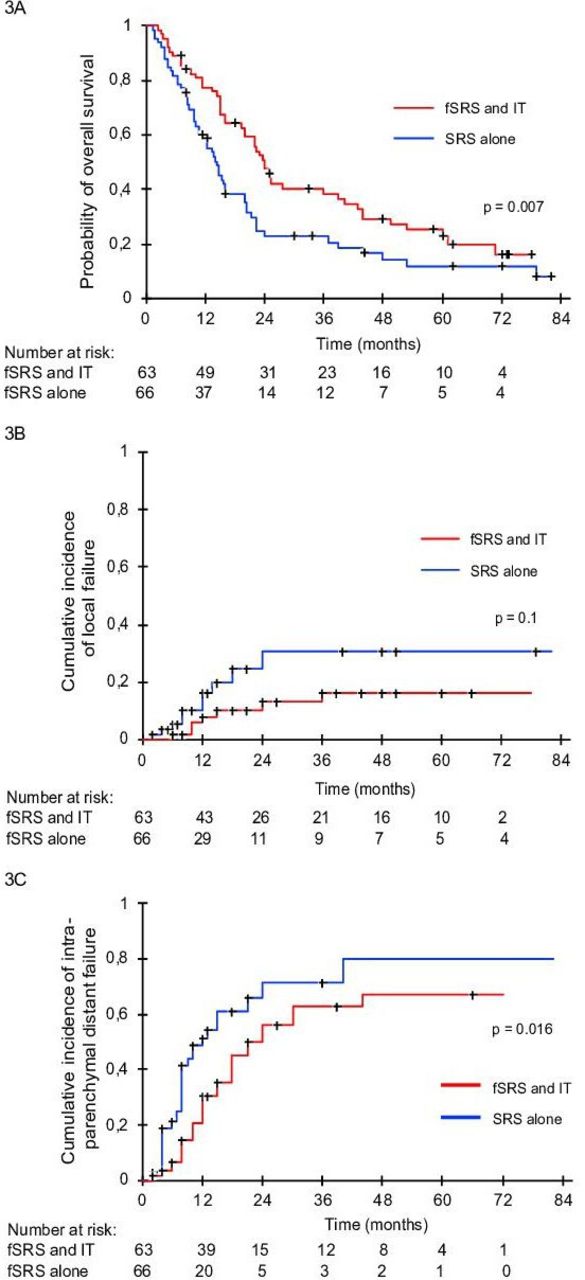
Cumulative incidence of local failure (A), distant brain failure (B), and Kaplan-Meier analysis of overall survival (C) after postoperative fSRS alone or in combination with IT for patients with resected brain metastases. Overall survival and distant brain control were significantly better in the fSRS and IT group. fSRS, fractionated stereotactic radiosurgery; IT, immunotherapy; SRS, stereotactic radiosurgery.
DBF and OS rates were significantly different between the groups. The median time to distant progression was 21 months in the fSRS and immunotherapy group and 10 months in the fSRS group (figure 3B). Twenty-four (38%) patients receiving fSRS and immunotherapy and 32 (48%) patients receiving fSRS had a distant event; respective 1-year and 2-year DBF rates were 31% (95% CI 20% to 46%) and 56% (95% CI 43% to 74%), and 52% (95% CI 39% to 68%) and 72% (95% CI 57% to 90%) (p=0.016). Overall, differences in cumulative incidence of LMD and DBF between groups resulted in a significantly decreased risk of intracranial failure of 32% for patients receiving fSRS and immunotherapy. The median OS was 24.8 months in the combination treatment group and 14.7 months in the fSRS group (p=0.007) (figure 3C); the 1-year and 2-year survival probabilities were 78% (95% CI 67% to 88%) and 50% (95% CI 38% to 63%), respectively, in the fSRS and immunotherapy group, and 58.7% (95% CI 47% to 70%) and 22.8% (95% CI 12% to 34%), respectively, in the fSRS group. Thirty-four patients succumbed to their intracranial disease (fSRS and immunotherapy, 11; fSRS alone, 23; p=0.03) and 64 patients died of progressive extracranial disease (fSRS and immunotherapy, 31; fSRS alone, 33; p=0.6).
The 1-year and 2-year extracranial PFS rates were 59% and 39%, respectively, in the fSRS and immunotherapy group, and 43% and 19%, respectively, in the fSRS group (p=0.02). The majority of patients had concurrent intracranial and extracranial progression; intracranial progression alone occurred in 6 patients receiving fSRS and immunotherapy and 15 patients undergoing fSRS alone.
For the whole population, multivariate analysis showed that combination treatment (p=0.001), controlled extracranial disease (p=0.01), and KPS >70 (p=0.02) were significant indices of prolonged OS. According to DS-GPA score, the median OS times were 5.5, 11, and 25.2 months for patients with scores of 0–1, 1–2.5, and 3–4 (p<0.001), respectively. Combination treatment and one BM were predictors of longer distant intraparenchymal control. Among patients receiving fSRS and immunotherapy, subanalysis showed that patients with melanoma had better OS and distant intraparenchymal control compared with those with NSCLC; the 2-year OS and DBF were 58% and 45%, respectively, for patients with melanoma, and 44% and 29%, respectively, for those with NSCLC (p=0.03). No factors emerged as a predictor of resection cavity control.
Toxicity
Adverse events were recorded in 35 (55%) patients receiving fSRS and immunotherapy and 18 (27%) receiving fSRS alone, with grade 3 events observed in 16 (25.4%) and 8 (12%) patients (p=0.07), respectively. Immunotherapy-related grade 3 events affecting the CNS were represented by headache (n=3), seizure (n=3), and increased brain edema (n=1). Intracranial hemorrhage was seen in two patients. Nivolumab was discontinued in six patients and pembrolizumab in two patients. The most common extracranial grade 3 events were fatigue (n=4), diarrhea (n=4), increased serum aspartate aminotransferase (n=3), and rash (n=2).
Twenty-two patients undergoing fSRS and immunotherapy and nine subjected to postoperative fSRS experienced treatment-related imaging changes suggestive of RN (p=0.02). Diagnosis of RN was made by MRI/PET imaging in all patients and confirmed by histology in nine patients (fSRS, 3; fSRS and immunotherapy, 6) who underwent surgery. The cumulative 1-year incidence of RN was 35.5% in patients receiving fSRS and immunotherapy and 14.7% in those receiving fSRS (p=0.03) (figure 4). Symptomatic grade 2 (n=9) or grade 3 (n=4) RN occurred in 13 patients (fSRS, 5; fSRS and immunotherapy, 8), requiring medical treatment or surgery; the estimated cumulative 1-year incidence was 13% for the combination treatment group and 8% for the fSRS group (p=0.09). Neurological deficits associated with RN included seizure (n=4), motor deficits (n=6), sensory deficits (n=3), cognitive deficits (n=3), dizziness (n=3), and speech deficits (n=3).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
TCumulative incidence of treatment-related imaging changes suggestive of radionecrosis in patients undergoing concurrent fSRS alone or fSRS and IT to postoperative resection cavity. Treatment with postoperative fSRS and IT was associated with a significantly increased risk of radiation necrosis within the treatment field. fSRS, fractionated stereotactic radiosurgery; IT, immunotherapy.
Early treatment-related imaging changes of irradiated cavities after fSRS were recorded in 10 patients (11 lesions) at a median time of 8 weeks (range 4–20 weeks). Grade 2 and grade 3 neurological deficits developed in three and two patients, respectively, requiring medical therapy. On subsequent imaging, tumor volumes decreased or disappeared in eight patients, confirming the diagnosis of pseudoprogression, and continued to enlarge in one patient who underwent surgery, with histology that confirmed tumor recurrence. In the subsequent follow-up, imaging findings suggestive of RN were observed in 22 cavities (fSRS and immunotherapy, 14; fSRS, 8), requiring surgery or long-term medical treatment. In seven patients who underwent surgery, diagnosis of RN was confirmed by histology. Overall, grade 2 and 3 neurotoxicity, including motor deficits (n=5), dizziness (n=2), neurocognitive deficits (n=3), seizure (n=2), and speech deficits (n=2), occurred in six and two patients, respectively.
In the univariate analysis, fSRS and immunotherapy (p=0.037) and larger PTV (p=0.04) were associated with an increased risk of RN; no other factors were predictors of RN, including preoperative tumor size, tumor histology, tumor location, type of immunotherapy, and number of metastases. In the multivariate analysis, only combination treatment was found to be a significant independent predictor of RN (HR 1.1; 95% CI 1.04 to 1.16; p=0.044).
Salvage therapy
Seventy-eight patients had intracranial progression, defined as the presence of either leptomeningeal or parenchymal BM, with a median time to progression of 10 months (range 2–36 months). Salvage treatments included surgery (n=6), repeated SRS (n=46), WBRT (n=14), and systemic therapies (chemotherapy, 32; targeted therapy, 15; immunotherapy, 24). Among patients treated with fSRS and immunotherapy, 10 received chemotherapy, 6 molecular targeted agents, and 16 continued on immunotherapy. Among patients treated with fSRS alone, 22 received chemotherapy, 8 were given immunotherapy, and 9 molecular targeted agents.
Discussion
Our study, where 129 patients with melanoma and NSCLC BM received postoperative fSRS to the resection cavity with or without concomitant immunotherapy, shows that combination treatment offers a significantly reduced risk of LMD compared with irradiation alone. The crude incidence of LMD was 22% in patients receiving fSRS and 7.5% in those receiving fSRS and immunotherapy, with cumulative rates of 22.5% and 5.8%, respectively, at 1 year.
The reported risk of developing LMD in the fSRS group is consistent with those seen in several large series showing 1-year rates ranging from 16% to 31% after surgical resection and postoperative SRS of BM.3 12 14 17–19 In a randomized trial comparing adjuvant SRS with observation for 128 patients who underwent gross total resection for one to three BM between 2009 and 2016 at The University of Texas MD Anderson, Mahajan et al3 observed a 28% rate of LMD. In contrast, in the North Central Cancer Treatment Group (NCCTG) N107C/CEC.3 prospective randomized trial of 194 patients with one resected BM who were assigned to either SRS or WBRT, Brown et al10 found a rate of LMD of 7% at 1 year, and a similar low rate has been observed in other few series.15 The variable range reported may, at least in part, be explained by differences in tumor histology, location of lesions, and type of surgical resection. Moreover, differences in imaging follow-up and under-reporting of nodular LMD,22 which is generally seen as focal nodules adherent to the dura or pia near the site of cavity in contrast to the classic LMD, may account for variability in assessment. Overall, our results confirm the relatively high rate of LMD after surgical resection and SRS and strongly support the concurrent use of immunotherapy and SRS to reduce the risk in patients with surgically resected BM.
Imaging review confirmed the peculiar pattern of nodular leptomeningeal enhancement in the postoperative setting20 21 32; type IIB pattern occurred in 58% and type IIA or IIC LMD in 42%. In a multi-institutional analysis of 147 patients from seven centers who received postoperative single-fraction or fractionated SRS to the surgical bed, Prabhu et al21 reported a similar risk of developing LMD. At a median time of 5.6 months, nodular LMD occurred in 57% of patients and classic LMD in 43% of patients. Recognizing this pattern of meningeal spread is of importance because it may be associated with better outcome compared with the classic LMD.20 32 In our series, survival was 16 months for nodular LMD and 6 months for classic LMD, consistent with published studies. Of note, a median survival of 14 months was seen in six patients who received pembrolizumab at the time of diagnosis of LMD, supporting its activity in patients with leptomeningeal BM from solid tumors.33
Further endpoints of our study included LF, DBF, OS, and treatment-related toxicity. Cumulative incidence curves showed no significant differences in resection cavity control between the groups, confirming that SRS alone offers excellent local control also in radioresistant tumors.15 In contrast, combination treatment was associated with significantly better distant intracranial control and OS, consistent with previous published series.34–38 Differences in cumulative incidence of LMD and DBF between groups resulted in a significantly decreased risk of intracranial failure (32% at 1 year) and neurological death for patients receiving fSRS and immunotherapy, with 50% and 26% of patients expected to be alive at 2 and 5 years.
Although our study indicates that postoperative fSRS and immunotherapy may represent an effective treatment in selected patients with resected BM, the small number of patients and the study design (not a randomized study) do not allow us to draw definite conclusions about the superiority of our approach over other treatment modalities, such as immunotherapy given alone or in combination with different radiation schedules. In this regard, prospective studies have shown significant intracranial response up to 65% for patients with melanoma and NSCLC BM receiving checkpoint inhibitors, especially when given in combination.23–25 In a recent update of the ABC randomized trial, Long et al39 reported 5-year intracranial PFS rates of 46% for patients receiving nivolumab plus ipilimumab vs 15% for those receiving nivolumab alone, with respective 5-year OS rates of 51% and 34%. Currently, a phase II, open-label, randomized controlled trial (ABC-X trial; ClinicalTrials.gov, NCT03340129) is enrolling asymptomatic treatment-naïve patients with melanoma BM assigned to receive either nivolumab plus ipilimumab in combination with SRS or nivolumab plus ipilimumab alone.
Treatments were generally well tolerated, with less than 10% of patients discontinuing immunotherapy. Imaging changes suggestive of RN were significantly increased in patients receiving combination treatment over fSRS alone; however, grade 3 toxicity was observed in less than 15% of patients. In a significant subset of patients, an early enlargement of treated lesions associated with increased perilesional edema occurred within 4 months after treatment. In the majority of patients these imaging findings resolved in 6–8 weeks without interruption of systemic therapy and were recorded as pseudoprogression. Overall, the rate of symptomatic RN observed in the current study is consistent with those observed in several retrospective series and systematic reviews of SRS in combination with immunotherapy for intact BM26 27 34–38 and SRS alone to postoperative resection cavity,15 providing some reassurance about the feasibility of using this approach in patients with resected BM.
We used a 3×9 Gy schedule based on the evidence of a lower risk of RN after fSRS over single-fraction SRS.40 41 Moreover, preclinical studies have suggested that hypofractionated radiotherapy may enhance the antitumor immune response of checkpoint inhibitors.42 43 In a previous study of 80 patients who received SRS and concurrent ipilimumab or nivolumab for multiple BM, we found better intracranial and extracranial PFS when checkpoint inhibitors, either nivolumab or ipilimumab, were administered in combination with fSRS compared with single-fraction SRS.38 Current ongoing trials are evaluating the efficacy of checkpoint inhibition alone or in combination with radiation in different tumors.44 45
The current study has several limitations, owing to its retrospective nature. The presence of unmeasured baseline characteristics, including levels of PD-1/PD-L1 expression in resected BM, previous systemic treatments, use of corticosteroids, and different salvage therapies at progression, is likely to introduce selection bias and may contribute to the observed differences in clinical outcomes between groups. Nevertheless, our results indicate that postoperative fSRS in combination with immunotherapy can offer significant reduction of either new leptomeningeal or parenchymal metastases in patients with resected BM.
In conclusion, our study shows that combining fSRS with immunotherapy is associated with better intracranial control and OS compared with fSRS alone in patients with resected BM. Combination treatments were able to decrease the rates of LMD and DBF with acceptable toxicity. Prospective trials are needed to explore the efficacy and safety of different radiation schedules in combination with immunotherapy over other therapeutic strategies in patients with resected BM.
Data availability statement
Data are available upon reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants and was approved by IRCCS Neuromed (2020/R0033) and Ospedale San Pietro (Study number 12/2020; ethical approval for retrospective study for both UPMC Hillman Cancer Centers). IRCCS Don Calabria approved this study as a retrospective clinical research. All our patients, at admission, provided a general consent form on the use of their data in anonymized form for research, including scans that are collected prospectively in an institutional database as their specimen (in case of surgery or biopsy).
Acknowledgments
The authors would like to thank the patients presented in this study.
References
Footnotes
Contributors GM is responsible for the conception and design of the study, participated in the analysis and interpretation of data and was responsible for statistical analysis, and drafted and finally revised the article. GM is also responsible for the overall content as guarantor. GL, LC, and IR participated in the study and data analysis. MG, LM, and VE participated in the study and article preparation. FC participated in the study, analysis and interpretation of data. AB participated in the analysis and interpretation of data and in article preparation and revision. FA and SP participated in the study, article preparation and revision. LN participated in the study, analysis of data and article preparation. GF participated in the collection and analysis of data. FB and TT participated in the study and interpretation of data. PCG participated in article preparation and revision. All authors read and approved the final manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.