Article Text

Abstract
Objectives: To describe variations in fatigue over the course of 2 years in a sample of persons with multiple sclerosis (MS), and to investigate the predictive value of the following variables on variations in fatigue: sex, age, sense of coherence, living with a partner, living with children, work status, immunomodulatory treatment, mood, disease severity, disease course, time since diagnosis and time.
Methods: Every 6 months, 219 outpatients at an MS specialist clinic were assessed using the Fatigue Severity Scale (FSS). Predictive values were explored with Generalised Estimating Equation employing proportional odds models; FSS scores were categorised as non-fatigue, borderline fatigue or fatigue.
Results: FSS scores varied significantly (p = 0.02); 54% changed FSS category one or several times, 27% were persistently fatigued and 19% persistently non-fatigued. Independent predictors of increased fatigue were depressive symptoms, weak/moderate sense of coherence, living with a partner and not working. Furthermore, moderate disease severity predicted increase when combined with >10 years since diagnosis or a progressive course. Independent predictors of decreased fatigue were no depressive symptoms, strong sense of coherence, living alone and working. Moreover, mild and severe disease predicted a decrease when combined with >10 years since diagnosis, and mild severity combined with a progressive course.
Conclusion: Mood, sense of coherence and living with a partner were independent predictors of fatigue in persons with MS. In addition to monitoring disease related variables, health related services should apply a broad range of approaches and repeatedly assess fatigue in persons with MS, to provide preventive care and appropriate interventions.
Statistics from Altmetric.com
Fatigue in multiple sclerosis (MS) is a subjective lack of physical and/or mental energy, perceived by the individual or caregiver to interfere with usual and desired activities.1 The majority of persons with MS (PwMS) report fatigue.2 3 Studies have reported an association between fatigue and depressive symptoms,4–7 but results regarding associations with gender, age, disease severity, disease course and duration are inconsistent.2–4 8 Longitudinal studies on fatigue are scarce6 9; however, 48% of an outpatient sample were reported to have fatigue during an 18 month follow-up.9
Sense of coherence (SOC) gives an indication of an individual’s capacity to cope with stressful life events.10 11 While weak SOC was recently found to be associated with depressive symptoms in PwMS,12 its association with fatigue has not yet been explored.
Knowledge about how MS related fatigue varies over time and the role of contributing factors is limited. The aims of this study were:
to describe variations in fatigue in a sample of PwMS during a 2 year period;
to investigate the predictive value on variations in fatigue of sex, age, SOC, living with a partner, living with children, work status, immunomodulatory treatment, mood, disease severity, disease course, time since diagnosis and time.
METHODS
All persons with definite MS13 were eligible who, from 1 February to 12 June 2002, were scheduled for an outpatient appointment with senior neurologists at the MS Centre of Karolinska University Hospital, Huddinge, Stockholm, Sweden. The ethics committee of Karolinska Institutet approved the study. After informed consent, PwMS were included in the study. Data at baseline and at 6, 12, 18 and 24 months were collected in conjunction with regular visits to the neurologist, who determined disease severity and course. Remaining data were collected primarily by the same research physiotherapists at the same time of day for all time points.
Fatigue was assessed using the Fatigue Severity Scale (FSS).14 Items were rated according to the experience of PwMS over the past 6 months. The FSS score is the mean of nine items. Analyses used FSS scores and their categorisation into non-fatigue (FSS⩽4.0), borderline fatigue (4.0< FSS <5.0) or fatigue (FSS ⩾5.0).3 5 9
Table 1 presents methods regarding independent variables, categorisation criteria and sample characteristics.
Analysis
The χ2 test was used for univariate analyses and the Friedman test for changes in FSS scores. Probability values ⩽0.05 were considered significant.
Generalised Estimating Equation (GEE) models employing proportional odds were used to investigate the predictive value of the independent variables for increase and decrease in fatigue. In the models, the odds for increase, from non-fatigue to borderline fatigue or fatigue, are equal to the odds for a change from non-fatigue or borderline fatigue to fatigue, and the opposite for models of decrease. Using GEEs allowed the inclusion of participants with at least one FSS score and complete data for the independent variables. Model 1 contained all variables except work status. Model 2 contained all variables and PwMS <65 years of age. Interactions between time and the independent variables were controlled for, as were interaction between SOC and mood, and between disease severity, disease course and time since diagnosis. Stepwise backward selection was employed using probability values of ⩾0.05 for variable removal. Pairwise comparisons were adjusted for multiple comparisons with the Bonferroni correction. Separate GEEs were performed with the disease related variables removed. The predictive values are presented as odds ratios (OR) with 95% confidence intervals (CI) and probability values.
SPSS version 13.0 was used for descriptive statistics and the Friedman test, and SAS System 9.1 (SAS Institute, Cary, North Carolina, USA) for GEEs.
RESULTS
Of 219 PwMS included, 200 completed the study; seven died and 12 withdrew. At the various time points, the FSS was completed by 98.5–100%. Two PwMS had no FSS score.
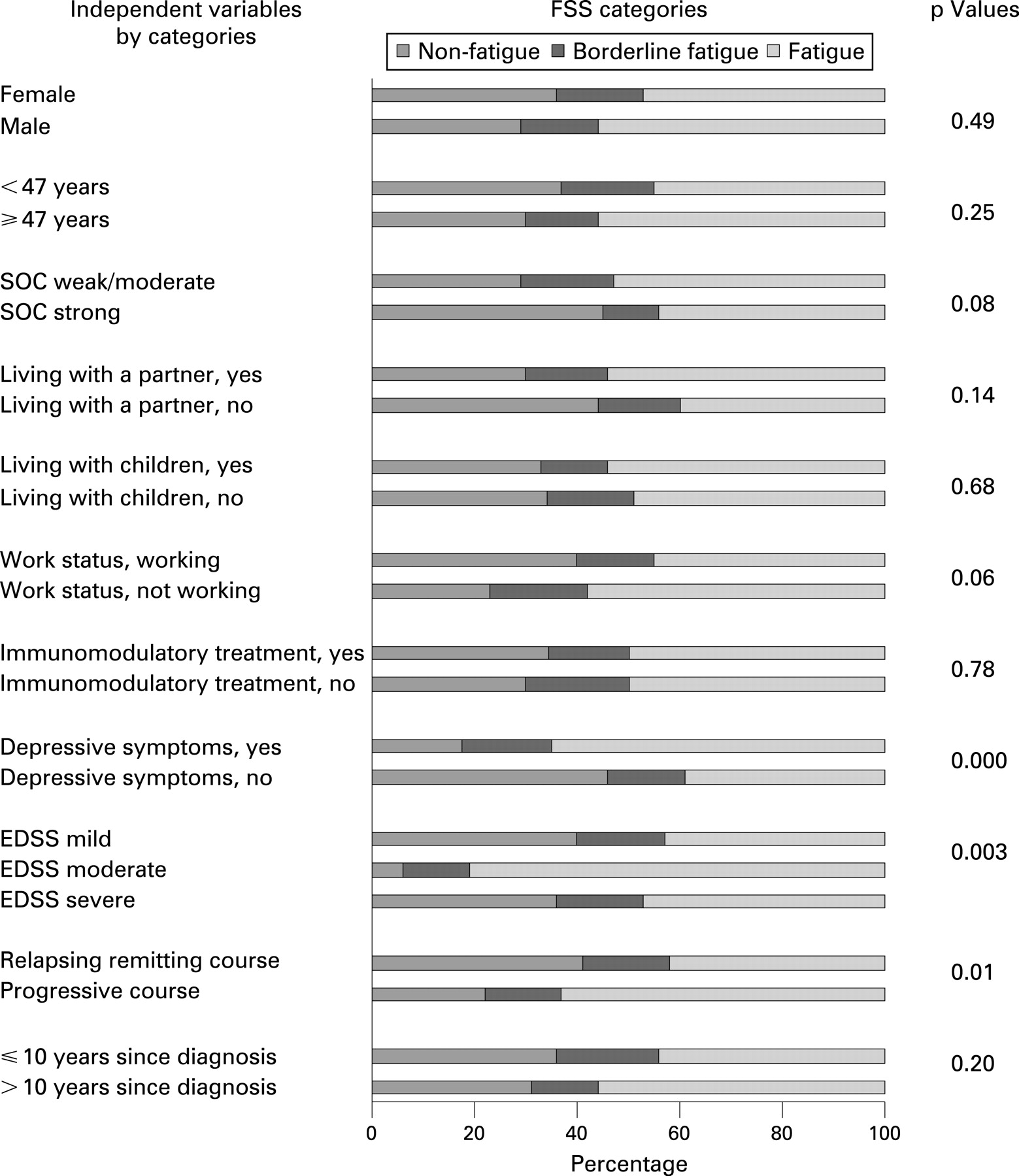
FSS scores varied significantly (p = 0.02) for PwMS with scores at all time points (n = 197). Proportions per FSS category varied from 32% to 39% for non-fatigue, from 14% to 18% for borderline fatigue and from 45% to 52% for fatigue. A total of 106 PwMS (54%) changed category 1–4 times while 91 (46%) remained in the same category during the study; 53 of the latter (27%) had fatigue and 38 (19%) non-fatigue. Figure 1 presents proportions per category of the independent variables by FSS category, and probability values of univariate analyses.

{kind=link}
The probability of belonging to a certain FSS category did not change over time; time did not interact with the other independent variables, nor did SOC with mood. Disease severity interacted with time since diagnosis and disease course. In model 1 (n = 193), the variables independently predicting increased fatigue were depressive symptoms (odds ratio (OR) 2.73, confidence interval (CI) 1.65 to 4.51; p<0.001), weak/moderate SOC (OR 1.90, CI 1.12 to 3.20; p = 0.017) and living with a partner (OR 1.92, CI 1.09 to 3.39; p = 0.025). Expanded Disability Status Scale (EDSS) moderate, predicted increased fatigue in conjunction with: (a) >10 years since diagnosis compared with EDSS mild (OR 13.39, CI 2.03 to 88.47; p = 0.001) and EDSS severe (OR 19.49, CI 1.27 to 303.03; p = 0.023) and (b) a progressive course, compared with EDSS mild (OR 37.83, CI 3.12 to 459.00; p = 0.001). In model 2 (n = 177), these predictors displayed similar predictive values; in addition, not working was an independent predictor (OR 1.78, CI 1.01 to 3.15; p = 0.047). Reciprocal categories of the same variables predicted decreased fatigue and displayed similar predictive values: no depressive symptoms, strong SOC, living alone, working, >10 years since diagnosis combined with EDSS mild or EDSS severe compared with EDSS moderate, and progressive course and EDSS mild compared with EDSS moderate. In GEEs with disease related variables removed, depressive symptoms, weak/moderate SOC and living with a partner predicted increased fatigue (similar predictive values) as well as age ⩾47 years (OR 1.75, CI 1.10 to 2.79; p = 0.0184); reciprocal categories predicted a decrease.
DISCUSSION
This is the first study that has described longitudinal variations in MS related fatigue while exploring predictors for variations in fatigue. FSS scores varied and the majority changed FSS category. Depressive symptoms, weak/moderate SOC, living with a partner and not working were independent predictors for increased fatigue. PwMS with EDSS moderate appeared at particular risk.
Of PwMS with FSS scores at all time points, 46% remained in the same category. Tellez et al reported 65% as stable when assessed twice over 18 months.9 It is likely that the more frequent data collection of our study allowed better detection of variations.
This study demonstrates that several variables predict MS related fatigue, irrespective of the presence of disease related variables. Depressive symptoms and increased fatigue were longitudinally associated, in agreement with a report in which depression predicted physical fatigue over 1 year.6 However, studies are needed to explore associations between depressive symptoms and different dimensions of fatigue. Weak/moderate SOC independently predicted increased fatigue, in line with findings where MS fatigue was associated with low sense of environmental mastery.20 In our study, no interactions were found between depressive symptoms and SOC, but both predicted fatigue. SOC has been reported to contribute to fatigue variability in people with other diagnoses.21 Living with a partner has not previously been found to be associated with MS fatigue and needs further exploration. The associations of fatigue with several variables found in this study emphasise the need for health related services to monitor other than disease related variables.
Our results should be interpreted keeping in mind that a large proportion of the sample received immunomodulatory treatment, although such treatment did not predict fatigue. In our models, selected variables were studied regarding their predictive value on fatigue. Future studies should explore other variables (eg, sleep and cognition) and, conversely, the predictive value of fatigue on the studied variables.
In conclusion, fatigue varied in the majority of PwMS when followed over 2 years. Depressive symptoms, weak/moderate SOC, living with a partner and not working independently predicted increased fatigue. PwMS with EDSS moderate appeared at particular risk. In light of the variation in fatigue and the impact of mood and psychosocial variables, health related services targeting PwMS should not only monitor disease related variables but should apply a broad range of approaches and systematically assess fatigue, aiming to provide preventive care and appropriate interventions.
Acknowledgments
The authors express their gratitude to the PwMS participating and the staff of the MS Centre, Karolinska University Hospital, Huddinge; to Professor Hans Link; and to Thomas Masterman and statistician Jakob Bergström of Karolinska Institutet.
REFERENCES
Footnotes
Funding: An unrestricted grant from Biogen Idec supported data collection. The study was funded by grants from the Centre for Health Care Sciences, the Health Care Sciences Postgraduate School, Karolinska Institutet; the Swedish Association of Persons with Neurological Disabilities; and the Swedish Research Council.
Competing interests: None.
Ethics approval: The ethics committee of Karolinska Institutet approved the study.