Article Text

Abstract
Background The evolution of rheumatoid arthritis (RA) and axial spondyloarthritis (axSpA) is marked by flares, although their frequency is unclear. Flares may impact physical activity. Activity can be assessed objectively using activity trackers. The objective was to assess longitudinally the frequency of flares and the association between flares and objective physical activity.
Methods This prospective observational study (ActConnect) included patients with definite clinician-confirmed RA or axSpA, owning a smartphone. During 3 months, physical activity was assessed continuously by number of steps/day, using an activity tracker, and disease flares were self-assessed weekly using a specific flare question and, if relevant, the duration of the flare. The relationship between flares and physical activity for each week (time point) was assessed by linear mixed models.
Results In all, 170/178 patients (91 patients with RA and 79 patients with axSpA; 1553 time points) were analysed: mean age was 45.5±12.4 years, mean disease duration was 10.3±8.7 years, 60 (35.3%) were men and 90 (52.9%) received biologics. The disease was well-controlled (mean Disease Activity Score 28: 2.3±1.2; mean Bath Ankylosing Spondylitis Disease Activity Index score: 3.3±2.1). Patients self-reported flares in 28.2%±28.1% of the weekly assessments. Most flares (78.9%±31.4%) lasted ≤3 days. Persistent flares lasting more than 3 days were independently associated with less weekly physical activity (p=0.03), leading to a relative decrease of 12%–21% and an absolute decrease ranging from 836 to 1462 steps/day.
Conclusion Flares were frequent but usually of short duration in these stable patients with RA and axSpA. Persistent flares were related to a moderate decrease in physical activity, confirming objectively the functional impact of patient-reported flares.
- Physical activity
- rheumatoid arthritis
- axial spondyloarthritis
- disease activity
- flare
- patient-reported outcomes
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
- Physical activity
- rheumatoid arthritis
- axial spondyloarthritis
- disease activity
- flare
- patient-reported outcomes
Key messages
What is already known about this subject?
The evolution of rheumatoid arthritis (RA) and axial spondyloarthritis (axSpA) is marked by alternated periods of flares and stable disease activity.
What does this study add?
In this first study with weekly assessments over 3 months, patients with generally well-controlled RA or axSpA self-reported flares in 28% of assessments.
For the first time, the effect of patient-reported flares on physical activity (measured by activity trackers) was assessed.
Persistent flares (of more than 3 days) had an objective functional impact in RA and axSpA, leading to a relative decrease in physical activity of 12%–21%, that is, an absolute decrease of 836–1462 steps/day.
How might this impact on clinical practice?
This study confirms the objective consequences of patient-reported flares and indicates that connected activity trackers may give indirect information on disease activity.
Introduction
The evolution of rheumatoid arthritis (RA) and axial spondyloarthritis (axSpA) is marked by alternated periods of flares and stable disease activity.1 Flares are important for patients since they contribute to the unpredictability of the disease.2 3 Furthermore, due to the link between inflammation and structural degradation, flares are important to assess for disease management.4 There is growing interest in both RA and axSpA to characterise the reality behind the concept of patient-reported flares.5 6 This fluctuating disease activity can be assessed through patient-reported outcomes (PROs).7 8 Flares may be defined from the patient perspective by a simple question.6 9 10
Reports concerning the frequency of flares are heterogeneous.10–13 Most studies report data from retrospective patient assessments (eg, over 3 months), which are subject to memory bias.10 12 A frequent assessment of flares would be useful. The duration of flares should also be taken into account: very short flares are sometimes termed ‘bad days’14; longer flares may be more relevant both in terms of impact on daily life and of disease management.
The validation of the notion of flares has been explored in RA compared with physician assessments of disease activity,6 and in axSpA compared with physician-reported flares.10 Flares may lead to poor outcomes including low quality of life, poor function and work impairment.1 14 15 However the objective consequences of flares on daily life and in particular on physical activity have not been assessed. Previous studies in RA and axSpA have suggested that physical activity and disease activity were correlated16 17; however, all these studies were cross-sectional. Physical activity including everyday walking as well as aerobic exercise may be objectively and longitudinally assessed using connected activity trackers. These devices allow both an interactive feedback of physical activity and the visualisation of activity patterns, according to duration, intensity and frequency of physical activity.18 We hypothesised that flares may lead to effects on physical activity, which could be detected through the use of an activity tracker.
The objective of this study was to evaluate the frequency of patient-reported flares in RA and axSpA based on repeated weekly assessments, and to assess longitudinally the relationship between flares and physical activity using a connected activity tracker.
Patients and methods
Study design
The ActConnect study was a prospective, multicentre, pragmatic, longitudinal observational study.19 Briefly, it took place in six participating centres (three tertiary care hospitals and three private practice physicians’ offices) in Paris, France.
Patients
Patients were included between January and April 2016 if they were over 18 years of age, had definite clinician-confirmed RA or axSpA according to the American College of Rheumatology/European League Against Rheumatism classification criteria20 or to the Assessment of SpondyloArthritis international Society21 classification criteria for RA and axSpA, respectively, and if they owned a smartphone or tablet which was compatible with the connected activity tracker and had an internet access. They were no inclusion criteria related to disease activity or to physical activity.
Data collection
Medical data
Patient characteristics collected at baseline included sex, age, weight, height, socioprofessional category, work status, type of rheumatic disease, disease duration, ongoing pharmacological treatment (including biologics) and comorbidities using the Functional Comorbidity Index, which ranges from 0 (0=no comorbidity; however the minimal score was 1 in the present study because of the rheumatic disease) to 18.22 Where available, in patients with RA, the status for rheumatoid factor (RF) and for anticyclic citrullinated peptide (anti-CCP), the presence of radiographic erosions and the Disease Activity Score 28 (DAS28) at inclusion were recorded23; in patients with axSpA, the Human Leukocyte Antigen (HLA) B27 status, history of peripheral and of extra-articular symptoms, and the presence of sacroiliitis according to the medical file, on X-rays and/or on MRI, were recorded. Disease activity was self-assessed at baseline by the Bath Ankylosing Spondylitis Disease Activity Index (BASDAI, ranging from 0 to 10) in patients with axSpA.24 25
Patient-reported outcomes
PRO questionnaires were completed from home each week during 3 months, following a text message reminder. All patient-reported data were collected online using the secured Sanoïa platform.24
Flares were assessed from the patient perspective by the question ‘has your disease flared up since the last assessment?’, with a categorical response according to no flare, flare lasting 1–3 days (short flare) or flare lasting more than 3 days (persistent flare). This question was adapted from the RA Flare questionnaire and translated to French.6
Patient global assessment (PGA) and pain were recorded using a 0–10 numeric scale at each assessment.26
Physical function was assessed by the modified Health Assessment Questionnaire at 3 months.27 At 3 months also, patients self-reported treatment changes for their rheumatic disease.
Physical activity data collection
Each participant received an activity tracker (the Withings Activité Pop watch28) and was instructed to wear it every day for 3 months. The Withings tracker records the number of steps per minute. Ninety consecutive days from the first Monday following activation of the device were collected. No instruction about physical activity was given to the participants; however, patients could visualise their physical activity on their smartphones.19
Physical activity was analysed as the number of steps per day, total activity duration (sum of minutes with at least 20 steps recorded per week) and activity duration in moderate to vigorous intensity (sum of minutes with at least 100 steps recorded per week).
Statistical analysis
Study population
Patients were analysed if they had at least one complete time point, which was defined by the completion of a questionnaire and the recording of physical activity at least 5 days over the 7 days preceding the questionnaire. All complete time points were entered in the analysis.
Flare analysis
The frequency of flares was assessed by the number of reported flares divided by the number of completed questionnaires for each patient. The percentage of time spent in flare was calculated for each patient by adding the duration of each reported flare (2 days for short flares, 5 days for non-consecutive persistent flares and 7 days for consecutive persistent flares), divided by the number of days assessed. Frequency of flares in patients with RA and axSpA was compared by Student’s test. The relationship between PGA or pain at each time point and flare assessment was analysed by mixed linear models, with a random intercept and slope for patients and with the flare as a fixed explanatory variable and sex and age as covariates (fixed effect), using the nlme R package.29
Longitudinal relationship between physical activity and disease activity
The relationship between physical activity and disease activity was assessed in univariate and multivariate analyses by linear mixed-effect models, also using the nlme package in R. The analyses were run for flare as a three-category variable (no flare, short flare, long flare) and as binary variable (yes/no), and for physical activity as the number of steps/day and as an activity duration/week. All models included fixed effect for time, disease activity and their interaction and intercept random effect for patients. Model assumptions of normality of the residuals and homoscedasticity were assessed by visual inspection of residual plots. When observed, heteroscedasticity was modelled using the power variance function. Covariates (as fixed effects) included rheumatic disease, sex, age, obesity, biologics and employment status. For illustrative purposes, the average physical activity level per patient was comparatively described according to the flare status, and the relative change of physical activity according to flare status was calculated. Given flare duration was only assessed as less or more than 3 days, ranges of decrease in physical activity were calculated: the difference in the number of steps between a week with no flare and a week with a flare was assumed to be ‘lost’ during the days of flares. For example, considering a patient who walked for a week with a short (1–3 days) flare 3000 steps less than for a week with no flare, the patient could have walked 3000 steps less per day of flare if the flare lasted 1 day, or 1000 steps less per day of flare if the flare lasted 3 days. Results are thus presented as ranges of steps reduction. Explanatory analyses to define specific reductions corresponding to a flare were inconclusive (data not shown).
All analyses were performed using R V.3.2.2 (R Development Core Team).30
Results
Among the 178 patients included in the study, 170 (91 patients with RA and 79 patients with axSpA) with a total of 1553 time points (mean±SD, 9.1±3.4 time points per patient) were analysed (table 1). The mean age was 45.5 (±12.4) years and the mean disease duration was 10.3 (±8.7) years; 60/170 (35.3%) were men. The majority of patients (129/170, 75.9%) were working. Patients with RA were more often female and were older than patients with axSpA (table 1). They had a mean DAS28 at baseline of 2.3 (±1.2); 51/91 (56.0%) had radiographic erosions, and 69/87 (79.3%) had positive RF and/or anti-CCP. Among patients with axSpA, 32/78 (41.0%) had experienced extra-articular symptoms, 44/75 (58.7%) had past or present peripheral symptoms, 53/71 (74.6%) carried HLA B27, and 57/69 (82.6%) had radiographic and/or MRI sacroiliitis. At baseline the mean BASDAI was 3.3 (±2.1). Overall, 90/170 (52.9%) patients were receiving biologics (table 1).
Characteristics of 91 patients with RA and 79 patients with axSpA
Treatments were globally stable: 30/170 (17.6%) patients reported a change over the 3 months in any treatment for their arthritis (in whom, 16 had increased their treatment and 9 had decreased it).
Flares frequency and duration
One hundred and twenty-seven (74.7%) patients reported at least one flare over the 3 months of follow-up. Respectively, 118 (69.4%) and 50 (29.4%) patients reported at least one short flare and one persistent flare. Patients reported having experienced a flare on average at 28.2% (±28.1%) of the questionnaires (table 2). Short flares were more frequent than persistent flares, with a mean frequency of, respectively, 21.3% (±23.8%) and 6.9% (±15.3%), that is, 78.9% (±31.4%) and 21.1% (±31.4%) of flares, respectively. These results correspond to 25.5 flares for 100 patient-weeks (respectively, 19.6 and 5.9 short and persistent flares per 100 patient-weeks).
Description of frequency and duration of patient-reported flares assessed weekly over 3 months
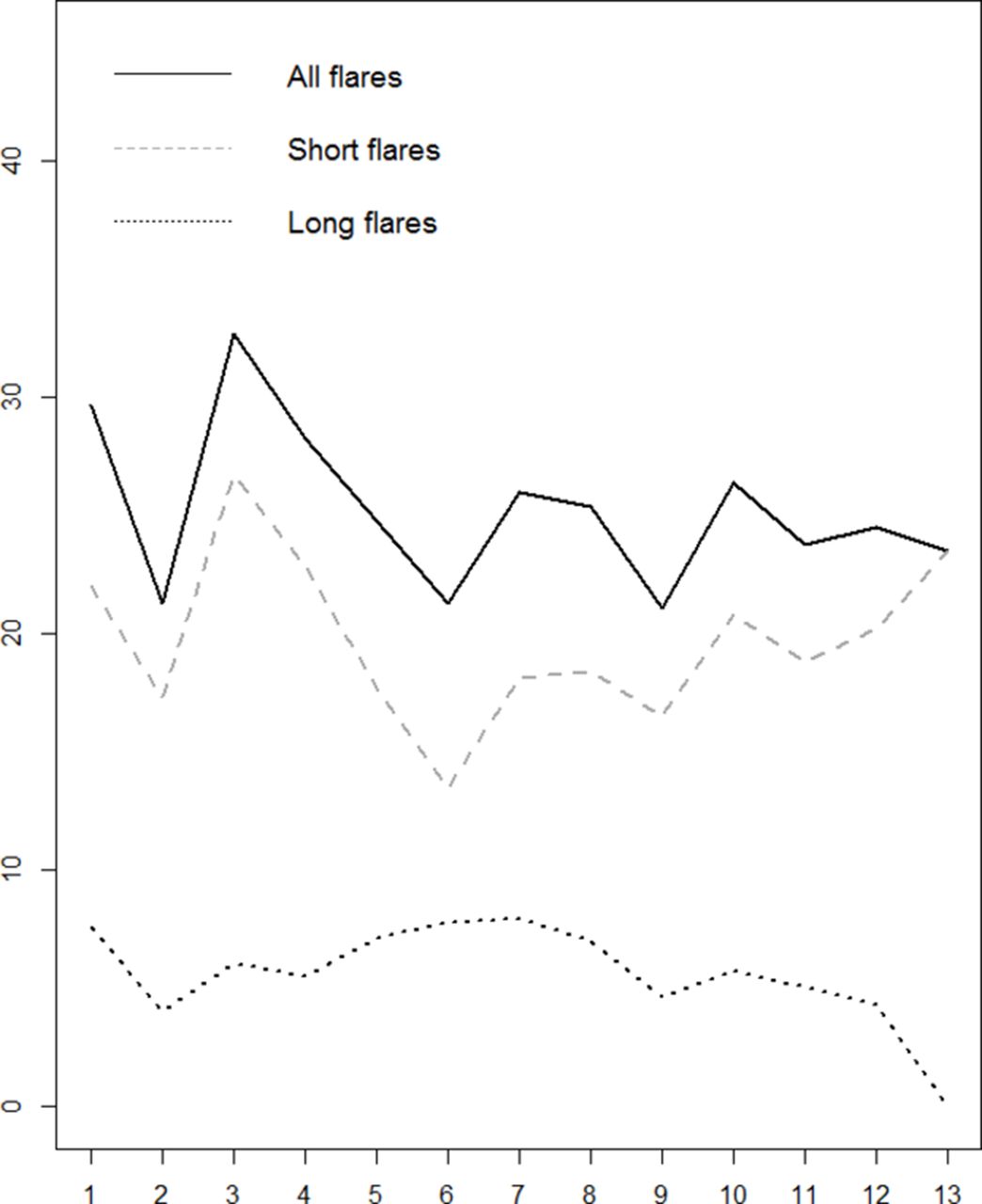
Patients spent on average 11.6 (±14.8)% of days in flare over the 3 months. Flares frequency and time spent in flare were similar in RA and in axSpA (data not shown). At any time point, 21.1%–33.3% of patients reported being in flare and this was globally stable over 3 months (figure 1).
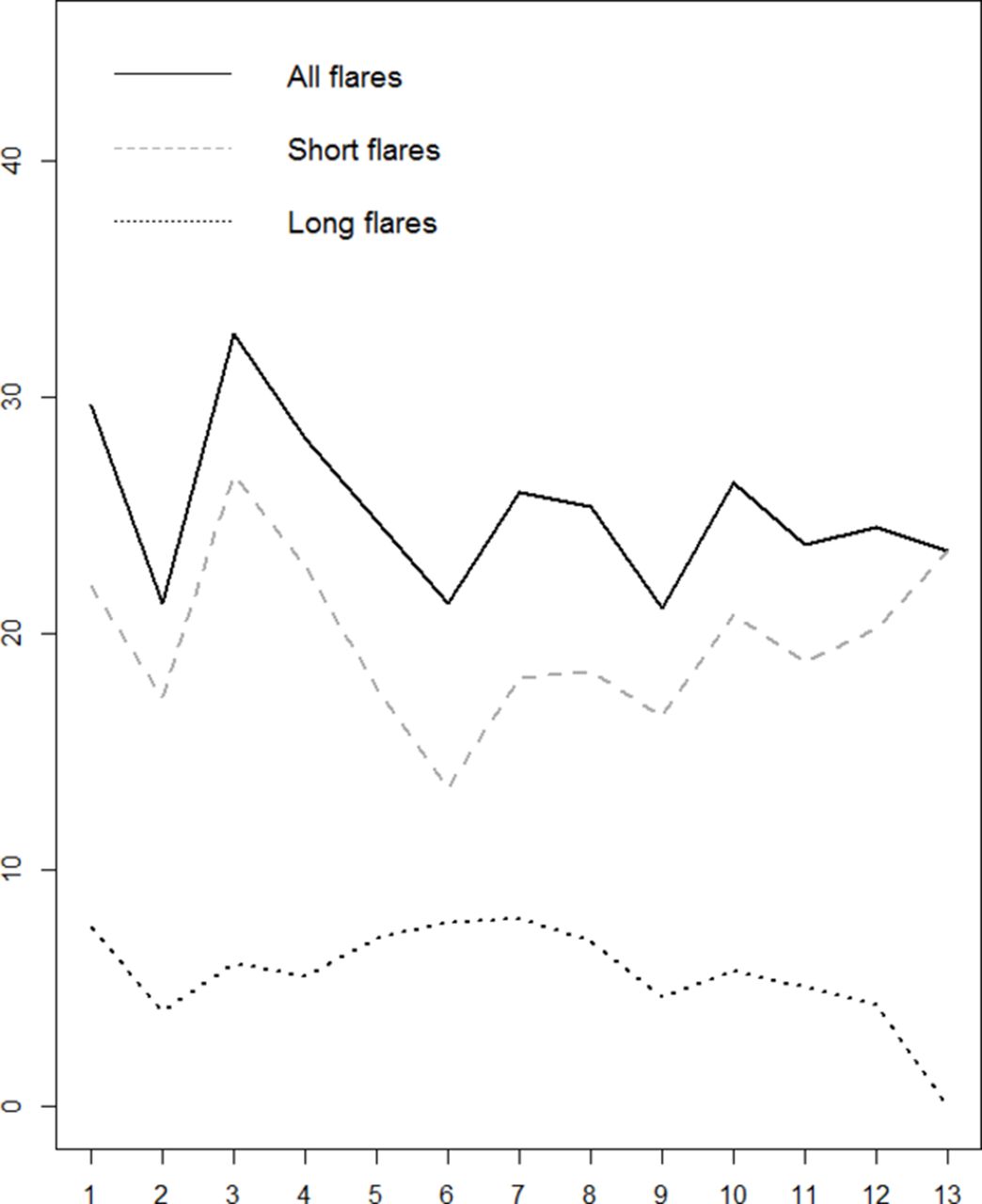
Frequency of patients in flare at each time point over 3 months. x-Axis, questionnaire number since the beginning of the study; y-axis, proportion of patients in flare (%).
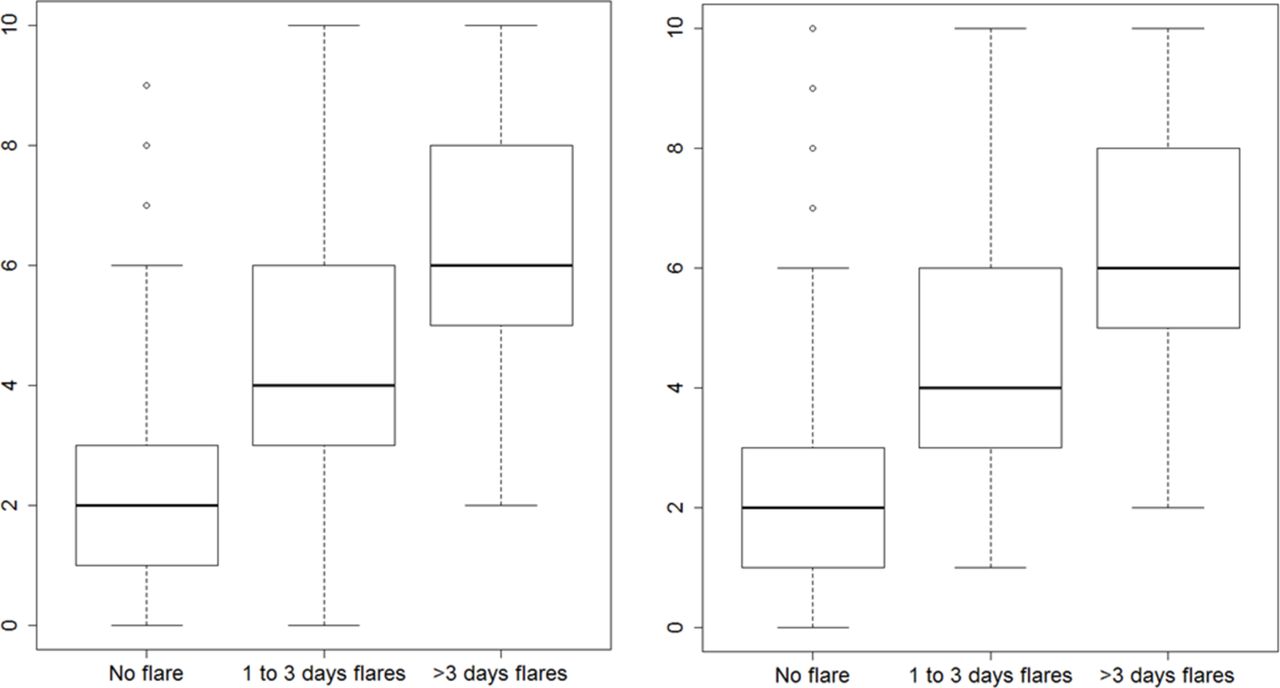
Pain and PGA significantly increased when patients self-reported flares (figure 2).

{kind=link}
{kind=link}
Mean pain and PGA across 1553 time points according to self-reported flare status in 170 patients with RA and axSpA: (A) Pain, (B) PGA. p<0.001 between the three categories for both pain and PGA; 1157 assessments with no flare; 304 assessments with 1–3 days flares; 92 assessments with >3 days flares. axSpA, axial spondyloarthritis; PGA, patient global assessment; RA, rheumatoid arthritis.
Longitudinal relationship between disease activity and physical activity
Over all assessments, the mean number of steps was 7067 (±2770) steps/day, corresponding to 715 (±282) min/week of physical activity, of which 105 (±89) min/week were in moderate to vigorous intensity (table 3).19
Physical activity according to flare status in 170 patients with RA and axSpA
When assessed longitudinally, reported flares were independently associated to a decrease in the mean number of steps (p=0.03) and in the total activity duration (p=0.02) (table 3). These results were confirmed when considering separately persistent flares, but not short flares. For descriptive purposes, the decrease in activity was computed. Patients were walking a mean of 7197 (±2810) steps/day, when not in flare. Physical activity levels were lower when patients reported a flare, and especially a persistent flare. The decrease in steps/day ranged from 836 to 1462 steps per day, corresponding to a relative decrease of 12.2%–21.3% when compared with assessments with no flare (table 3). Of note, the decrease in physical activity was not significant regarding moderate to vigorous physical activity.
Discussion
This study brings original information on both the frequency of flares and their objective consequences on physical activity in RA and axSpA. Flares were frequent in weekly assessments of patients with RA and axSpA over 3 months: they were self-reported in 28% of questionnaires. However, 79% of flares lasted less than 3 days. Although persistent flares were less frequent, they were noted in a mean of 7% of assessments in this population, with well-established and stable disease often receiving biologics. Flares, and especially persistent flares, significantly impacted physical activity, with a decrease of around 1000 steps for each day spent in flare compared with a day with no flare. These results confirm objectively the functional impact of patient-reported flares and indicate connected activity trackers may give indirect information on disease activity.
This study has strengths and weaknesses. Although the inclusion criteria did not specify any levels of disease activity, most patients had well-controlled and stable disease activity. This possible selection bias should have led to a low proportion of flares (which is not the case). There were 1553 time points to analyse, making this one of the largest studies on patient-reported flares, with also remarkably little missing data, when compared with other ‘regular assessment’ studies.31 Given the current lack of validated question applicable in both diseases, flares were assessed from the patient perspective by a single question, which has not been fully validated. However, a similar question has been previously used.6 9 10 The links between the flare question and well-validated outcomes (pain, PGA) strengthen the validity of the present results. To avoid memory bias, flares were assessed weekly. However, the precise days of flares were not recorded; the use of averages over a week may have decreased the strength of the relationship between flares and physical activity. Although a decrease in physical activity was noted in case of flares, it was difficult to quantify precisely this reduction and only indicative ranges could be presented, according to the possible flare duration.
In the present study, 75% of patients experienced flares during the 3 months’ follow-up, although they had a long-standing disease and were often treated with biologics. This frequency was higher than previously reported.9–12 The tight monitoring and the assessment of all flares, including short ones, may explain these results. Overall, 79% of flares lasted less than 3 days. The higher frequency of short flares versus persistent flares was in agreement with previous studies.1 12 It is questionable whether flares lasting less than 3 days should be called ‘flares’ or whether they are in fact ‘bad days’.14 Indeed, flares have been previously described in RA as a worsening in disease activity of sufficient intensity and duration to consider a change in therapy,12 32 whereas bad days may correspond to small disease fluctuations. The absence of statistical link between short flares and physical activity may argue in favour of this notion of ‘bad days’, although there may be here an issue of lack of power. The patient-perceived impact of flares (even short ones) should be further explored. As regards flares lasting more than 3 days, the frequency of 7% can be seen as high when considering this well-controlled and well-treated population. It may also simply reflect the fluctuating nature of RA and axSpA.33
The present study was the first study to explore longitudinally and objectively the relationship between disease activity and physical activity. Most of the previous cross-sectional studies confirmed that an increase in disease activity was related to a decrease in physical activity.16 17 34–37 The originality of the present study was to explore disease activity from the patient perspective regularly, once a week, and to cross-tabulate this information with objective measurements of physical activity. Most previous studies have compared patient-reported flares either with other PROs6 9–11 15 or with physician assessment in both RA and axSpA.6 10 The present results indicate the reality of the impact of flares using an objective measure of daily life and functioning: the number of steps and activity duration assessed through a connected device. Of note, some activities without steps, such as cycling, were not assessed here. Previous studies in the field of rheumatic diseases have often used questionnaires to measure physical activity.17 38 Connected activity trackers may bring more objective information.39
In the present study, a significant decrease in physical activity was noted concomitantly to patient-reported flares. This decrease was present even though there were no secondary benefits for the patient (such as sick leave) to overdeclare flares nor to change their physical activity since the data were not analysed in real time and were not relayed to their physician. Furthermore, as patients reported flares retrospectively for the past week, a possible influence of this report on their physical activity seems implausible. The patients had access to their physical activity reports on their smartphone, which may have rather played a motivational role.40 The decrease was moderate, corresponding to 836–1462 steps per day or 12%–21% of relative decrease, which indicates the present patients did not stay bedridden when in flare. Of note, in the present study, most patients were in general good health, had few comorbidities and had a professional activity. They probably developed coping mechanisms to deal with flares while continuing their daily activities.41 On the other hand, a decrease of 12%–21% of physical activity may correspond to concrete changes in daily life, for example to take the car instead of walking to work, resting when at home, avoiding stairs and so on. However, we did not observe a reduction in moderate to vigorous physical activity during flares, possibly due to lack of power since the present patients performed very little aerobic activity.19
In conclusion, flares in patients with RA and axSpA were frequent but usually of short duration. Flares, and especially persistent flares, were related to a moderate decrease in the level of physical activity, which confirms and objectivises the functional impact of patient-reported flares. These results open perspectives to integrate in the future connected devices in the monitoring of patients with chronic arthritis, in clinical research as well as in clinical practice.
Acknowledgments
We thank the following physicians who included patients in the study: F Bailly, S Dadoun and L Morardet, all in rheumatology department, Pitié Salpêtrière Hospital, Paris, and S Rozenberg and B Banneville, in rheumatology private practice, Paris. The study was conducted under the umbrella of the Société Française de Rhumatologie, Section e-Santé.
References
Footnotes
Contributors LG, CJ and HS drafted the study design. CJ and LG drafted the manuscript with contributions from all authors. CJ, LG and BG analysed and interpreted the data. CJ, AM, JS, VF, FG, CH, SM, BF and LG participated in the patient inclusion and data collection. HS participated in the data acquisition. All authors approved the final manuscript.
Funding The study was funded by unrestricted academic grants from Lilly France, BMS France and Pfizer France.
Competing interests None declared.
Patient consent All patients returned an agreement form, written for this specific study.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement Data are available from CJ at jacquemin.charlotte@gmail.com.