Article Text

Abstract
Background Vitamin D plays a role in host defence against infection. Vitamin D deficiency has been associated with an increased risk of respiratory tract infections in children and adults. This study aimed to examine whether vitamin D supplementation is associated with a lower pneumonia risk in adults.
Methods Three independent case–control studies were performed including a total of 33 726 cases with pneumonia in different settings with respect to hospitalisation status and a total of 105 243 controls. Cases and controls were matched by year of birth, gender and index date. The major outcome measure was exposure to vitamin D supplementation at the time of pneumonia diagnosis. Conditional logistic regression was used to compute ORs for the association between vitamin D supplementation and occurrence of pneumonia.
Results Vitamin D supplementation was not associated with a lower risk of pneumonia. In studies 1 and 2, adjustment for confounding resulted in non-significant ORs of 1.814 (95% CI 0.865 to 3.803) and 1.007 (95% CI 0.888 to 1.142), respectively. In study 3, after adjustment for confounding, the risk of pneumonia remained significantly higher among vitamin D users (OR 1.496, 95% CI 1.208 to 1.853). Additional analyses showed significant modification of the association through co-use of corticosteroids and drugs that affect bone mineralisation. For patients using these drugs, ORs below one were found combined with higher ORs for patients not using these drugs.
Conclusions This study showed no preventive association between vitamin D supplementation and the risk of pneumonia in adults.
- Respiratory Infection
Statistics from Altmetric.com
Key messages
What is the key question?
-
Is vitamin D supplementation associated with a lower pneumonia risk in adults?
What is the bottom line?
-
Former studies, in children and adults, have investigated the effect of vitamin D supplementation on the incidence of respiratory tract infections but with conflicting findings.
Why read on?
-
This large project, including three independent case–control studies, shows no preventive association between vitamin D supplementation and the risk of pneumonia in adults.
Introduction
Despite advances in the treatment of pneumonia throughout the years, it is still a major healthcare problem, causing considerable morbidity and mortality, especially in older people.1 Vitamin D deficiency is also very common worldwide, particularly in risk groups such as older people and people living distant from the equator.2 ,3 An accumulating amount of data suggests that vitamin D deficiency is associated with an increased risk of respiratory tract infections in children and adults.4–9 A potential mechanism underlying this association might be the immunomodulatory actions of vitamin D.10 Next to its well known role in calcium and bone homeostasis, vitamin D is known to enhance innate immunity, in particular by increasing transcription of antimicrobial peptides. Vitamin D also plays a role in acquired immunity by its effect on dendritic cells, monocytes, T cells and B cells.10
The increased risk of pneumonia in patients with vitamin D deficiency and the interaction between vitamin D and the immune system lead to the question of whether vitamin D supplementation can lower the incidence of pneumonia. To date, several studies in children and adults have investigated the effect of vitamin D supplementation on the incidence of respiratory tract infections but with conflicting findings. In one placebo-controlled trial, daily vitamin D supplementation during the winter reduced the incidence of seasonal influenza A in schoolchildren in Japan.11 In another randomised controlled trial (RCT), a single high dose of vitamin D for children with pneumonia reduced the risk of repeat episodes of pneumonia.12 In contrast, three other well designed RCTs (two conducted in adults and one in a high-risk infant population) were not able to show a preventive effect of vitamin D supplementation on the incidence of respiratory tract infections.13–15 One of these studies even reported an increased risk of repeat episodes of pneumonia for children receiving vitamin D supplementation versus placebo.14 Considering all this, the preventive role of vitamin D supplementation in the development of respiratory infections remains uncertain. Therefore, in this project, we conducted three independent case–control studies in parallel to examine the association between vitamin D supplementation and risk of pneumonia. In contrast with former studies, including children or healthy adults, we examined the association in a relevant population at risk for pneumonia, namely older patients known to represent a considerable prevalence of vitamin D deficiency. Our a priori hypothesis was that vitamin D supplementation has a preventive effect on the development of pneumonia.
Methods
Study design and data origin
Three independent case–control studies were conducted comprising cases and controls from different settings with respect to hospitalisation status. Study 1 included hospitalised patients with community-acquired pneumonia who participated in two clinical trials in the Netherlands (ANTONIUS cases) and controls drawn from the PHARMO Record Linkage System database (PHARMO controls).16 ,17 The PHARMO Institute (Utrecht, the Netherlands) is an independent scientific research organisation studying drug use and outcomes. The PHARMO database includes detailed information on patient demographics, drug use and hospital admissions from about 3 million community-dwelling inhabitants of 48 geodemographic areas in the Netherlands (http://www.pharmo.nl). In study 2, cases and controls were retrieved from the PHARMO Record Linkage System database (PHARMO cases and PHARMO controls). Study 3 included primary care cases and controls obtained from the Netherlands Primary Care Research Network (NPCRD) database (NPCRD cases and NPCRD controls). This nationwide database is coordinated by NIVEL, the Netherlands institute for health services research. The database is collected by a network of general practitioners (GP) across the Netherlands and includes longitudinal data on clinical diagnoses, drug prescriptions and referrals from about 700 000 individuals representative of the Dutch population (http://www.nivel.nl/representativiteit-van-linh).18
Case–control study 1 (ANTONIUS-PHARMO)
ANTONIUS cases were patients hospitalised with radiographically confirmed community-acquired pneumonia who participated in two clinical studies.16 ,17 Patients were admitted through the emergency department of the St Antonius Hospital in Nieuwegein or the Gelderse Vallei Hospital in Ede (teaching hospitals in the Netherlands) between October 2004 and August 2006, and between November 2007 and September 2010. Pneumonia was defined as the presence of a new pulmonary infiltrate on a chest radiograph, in combination with at least two of the following criteria: cough, sputum production, temperature above 38°C or below 35°C, auscultatory findings consistent with pneumonia, C-reactive protein concentration >15 mg/L, white blood cell count >10×109 cells/L or <4×109 cells/L, or >10% of rods in leukocyte differentiation. On the day of hospital admission, pneumonia severity index and CURB-65 scores were calculated for all patients.
Population-based PHARMO controls were individually matched to the ANTONIUS cases by year of birth, gender and index date, in a 4:1 ratio. The index date was the date of pneumonia diagnosis of the corresponding case. Controls were considered ineligible if they were diagnosed with pneumonia in the 6 months before the index date (identified by the International Classification of Diseases, nineth revision, Clinical Modification (ICD-9-CM) codes 481–487).
Case–control study 2 (PHARMO-PHARMO)
PHARMO cases were patients hospitalised with pneumonia (community acquired and hospital acquired) between 2004 and 2010. Cases were identified based on hospital discharge records coded according to the ICD-9-CM codes 481–487. Population-based PHARMO controls were individually matched to the PHARMO cases by year of birth, gender and index date, in a 2:1 ratio. Controls were excluded from the study if they were diagnosed with pneumonia in the 6 months before the index date (identified by ICD codes).
Case–control study 3 (NPCRD-NPCRD)
NPCRD cases were primary care patients diagnosed with pneumonia by a GP between 2004 and 2010. Diagnosis was based on clinical criteria, mainly without radiological confirmation. Cases were identified based on GP morbidity records coded by using the International Classification of Primary Care (ICPC) scheme. The ICPC code used for this purpose was R81 (‘pneumonia’).
Population-based NPCRD controls were individually matched to the NPCRD cases by year of birth, gender and index date, in a 5:1 ratio. Controls were excluded from the study if they were diagnosed with pneumonia in the 6 months before the index date (identified by ICPC codes).
Exposure definition
For the ANTONIUS cases, community pharmacies were approached to identify all dispensed prescription drugs issued in the 6 months before the diagnosis of pneumonia. The PHARMO database supplied drug-dispensing records for related cases and controls. The NPCRD database provided drug prescription data for related cases and controls. Exposure definitions were identical for all cases and controls in all three case–control studies. We identified all prescriptions for vitamin D monotherapy and combination supplements by recording the following Anatomical Therapeutic and Chemical (ATC) codes: A11CC (vitamin D and analogues), H05BX02 (paricalcitol), A12AX (calciumcarbonate/colecalciferol), M05BB03 (alendronic acid and colecalciferol), M05BB04 (risedronic acid, calcium and colecalciferol, sequential) and M05BB05 (alendronic acid, calcium and colecalciferol, sequential).
Vitamin D use was defined as two or more prescriptions in the 6 months (182 days) before the index date. Defined daily doses were calculated based on strength and prescribed dosing regimen of the most recent prescription prior to the index date.19
Potential confounders
Comorbidities predisposing people to pneumonia were identified by drug proxies (as indicator for disease).20 The following comorbidities were considered potential confounders: diabetes mellitus (identified by use of antidiabetics), chronic obstructive pulmonary disease (COPD) or asthma (identified by use of inhalation medication), osteoporosis (identified by use of bisphosphonates and/or calcium), advanced renal disease (identified by use of erythropoietin and/or phosphate binders) and congestive heart failure (identified by use of digoxin plus diuretics). Oral corticosteroids and enzyme-inducing anticonvulsants were also considered potential confounders because of their interaction with vitamin D metabolism.21–23 For all drugs, except for erythropoietin and phosphate binders, drug use was defined as two or more prescriptions in the 6 months before the index date. Erythropoietin and phosphate binder use was defined as one or more prescriptions in the 6 months before the index date.
Statistical analysis
Patient characteristics were compared using the independent samples t test, the χ2 test or the Fisher's exact test, if appropriate. Conditional logistic regression was performed to study the association between vitamin D supplementation and risk of pneumonia. Unadjusted ORs and 95% CIs were estimated. Confounders were selected for the multivariate model stepwise by direct estimation of the degree of confounding produced by each factor (relative change of the regression coefficient for pneumonia associated with vitamin D supplementation). Factors that modified the regression coefficient by >10% were included in the final model to obtain adjusted ORs and 95% CIs. Additionally, we evaluated the same factors (from univariate analysis or previously mentioned in literature) as potential effect modifiers. We considered factors as an effect modifier when their interaction term (factor×vitamin D use) was statistically significant in a conditional logistic regression model with the factor and vitamin D use included.
All statistical analyses were performed using SPSS V.18.0 (Chicago, Illinois, USA). In all analyses, a p value <0.05 was considered statistically significant.
Results
Patient characteristics
A total of 33 726 pneumonia cases and 105 243 matched controls were included in this project, subdivided over three independent case–control studies. Case–control study 1 comprised 504 pneumonia cases and 2016 matched controls, case–control study 2 comprised 20 824 pneumonia cases and 41 268 matched controls, and case–control study 3 consisted of 12 398 pneumonia cases and 61 959 matched controls. Patient characteristics of cases and controls for all study cohorts are shown in table 1. Overall, cases were more likely to have comorbid illnesses such as diabetes mellitus, congestive heart failure, osteoporosis, COPD or asthma, and more often used vitamin D supplementation and oral corticosteroids.
Patient characteristics for the three independent case–control studies
Association between vitamin D supplementation and pneumonia
Case–control study 1
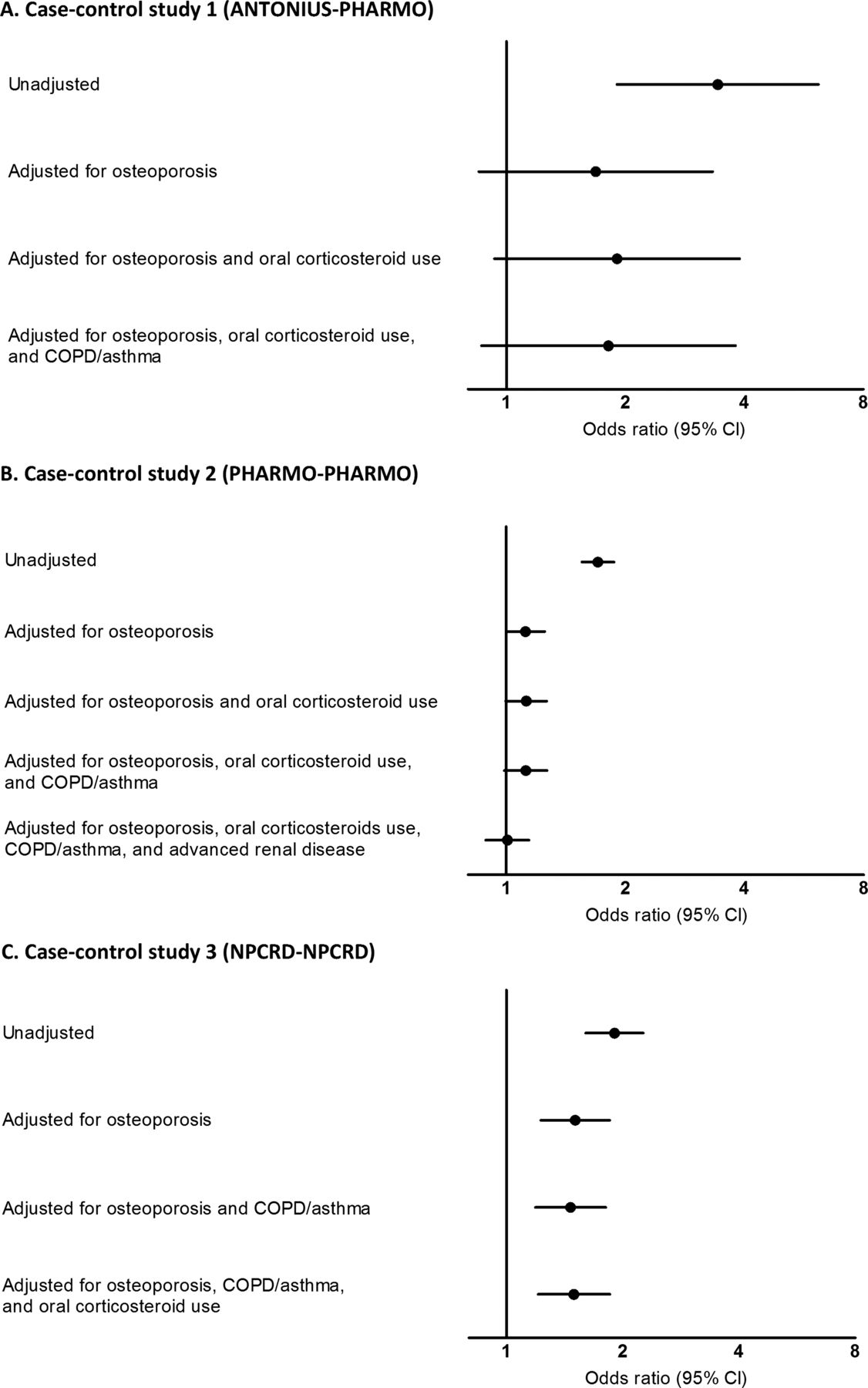
In the crude analysis in the ANTONIUS-PHARMO cohort, vitamin D supplementation was associated with a higher risk of pneumonia (OR 3.428, 95% CI 1.906 to 6.165). The following confounders were identified: osteoporosis (58% modification of the regression coefficient), oral corticosteroids (16%) and COPD/asthma (12%). Adjustment for these confounders resulted in a non-significant risk of pneumonia among vitamin D users compared with non-users (OR 1.814, 95% CI 0.865 to 3.803).
Case–control study 2
In the crude analysis in the PHARMO-PHARMO cohort, vitamin D supplementation was associated with a higher risk of pneumonia (OR 1.708, 95% CI 1.556 to 1.874). In this cohort, osteoporosis (79% modification of the regression coefficient), oral corticosteroids (32%), COPD/asthma (24%) and advanced renal disease (17%) were identified as confounders. Adjustment for these confounders resulted in a non-significant risk of pneumonia among vitamin D users compared with non-users (OR 1.007, 95% CI 0.888 to 1.142). No dose–effect relation was found in the association between vitamin D supplementation and pneumonia risk (data not shown).
Case–control study 3
In the crude analysis in the NPCRD-NPCRD cohort, vitamin D use was associated with a higher risk of pneumonia (OR 1.905, 95% CI 1.604 to 2.262). In this cohort, osteoporosis (36% modification of the regression coefficient), COPD/asthma (21%) and oral corticosteroids (20%) were identified as confounders. Adjustment for these confounders gave a lower, but still elevated, risk of pneumonia among vitamin D users compared with non-users (OR 1.496, 95% CI 1.208 to 1.853).
For all three case–control studies, table 2 lists the unadjusted and adjusted ORs for the association between vitamin D supplementation and pneumonia risk. Figure 1 shows the change of the OR for vitamin D supplementation and pneumonia risk by adding each confounder stepwise.
Unadjusted and adjusted ORs for the association between vitamin D supplementation and pneumonia risk for the three independent case–control studies
{kind=link}
ORs on a log scale in the association between vitamin D use and pneumonia with progressive multivariate adjustment for confounders in three independent case-control studies.
Identification of effect modifiers
In addition to the overall analyses, the possibility of effect modification was ascertained in all three case–control studies. ‘Osteoporosis’ was a significant effect modifier in case–control studies 1 and 2 (p=0.018 and p=0.000, respectively), and borderline significant in case–control study 3 (p=0.072). ‘Oral corticosteroids’ was a significant effect modifier in case–control studies 2 (p=0.024) and 3 (p=0.006), but not in case–control study 1 (p=0.121). Adjusted ORs of these effect modifiers can be found in table 3.
Effect modification of adjusted ORs for the risk on pneumonia with vitamin D supplementation in all three case–control studies
Discussion
In three independent case–control studies in adults, vitamin D supplementation was not associated with a lower risk of developing pneumonia. Interestingly, the use of drugs that affect bone mineralisation (bisphosphonates and/or calcium) or oral corticosteroids significantly modified the association.
The absence of a preventive association between vitamin D supplementation and pneumonia was contrary to our expectations. This finding, however, is in accordance with the most recent placebo-controlled studies on vitamin D and respiratory tract infections. In 3000 infants in Afghanistan a quarterly dose of 100 000 IU vitamin D3 or placebo during 18 months did not affect the incidence of pneumonia. Interestingly, they even showed a significant higher incidence rate of repeat episodes of pneumonia in vitamin D treated children.14 The recent placebo-controlled study by Murdoch et al15 also showed no reduction in the incidence or severity of upper respiratory tract infections in 322 healthy adults in New Zealand who randomly received oral vitamin D3 (an initial dose of 200 000 IU followed by 200 000 IU after 1 month, and then 100 000 IU monthly for 18 months), or placebo. The most recent study by Li-Ng et al13 conducted in 162 adult volunteers from Long Island, New York, who were randomised to either 2000 IU vitamin D3 daily for 12 weeks or placebo during the winter, also reported no benefit of vitamin D supplementation in decreasing the incidence of upper respiratory tract infections. In our study, including more than 130 000 mostly older people (comprising 4432 people who took vitamin D), no association between vitamin D supplementation and risk of acquiring pneumonia was observed. This suggests that any preventive effects, if present, do not extend to older people, in whom there is considerable prevalence of vitamin D deficiency.24 So far, studies in which a preventive effect of vitamin D supplementation on respiratory tract infections was found were conducted in children.11 ,12 Maybe, future study, including genetic data, will be able to identify small subgroups that might benefit from vitamin D supplementation.25
The modification of the association between vitamin D supplementation and pneumonia by drugs that affect bone mineralisation (‘osteoporosis’) and oral corticosteroids may have different explanations. First, there might be a pharmacological interaction between vitamin D and these drugs. An interaction between vitamin D and calcium has been suggested in a recent individual patient data meta-analysis that showed a reduced overall mortality in older patients using vitamin D and calcium together, whereas sole use of vitamin D supplementation did not affect the mortality rate.26 ,27 This could mean that co-use of calcium is necessary for vitamin D to become beneficial. Second, it might also be that in patients with osteoporosis vitamin D will most likely be prescribed for its effect on calcium metabolism and not because of confirmed vitamin D deficiency. It is not inconceivable that the vitamin D dosages observed in our study are insufficient to overcome true vitamin D deficiency and thus explain why vitamin D supplementation in patients not using osteoporosis drugs is associated with an increased pneumonia risk. Linked to the latter, it is also possible that in patients not using drugs that affect bone mineralisation, vitamin D is prescribed for indications that predispose people to pneumonia but that those indications were not available for assessment as confounders in the present study. The percentage of people who took vitamin D and also used bone mineralisation affecting drugs varied between 72% and 80% across the three datasets. In study 3, after adjustment for confounding, there remained an overall significant increased risk of pneumonia in patients receiving vitamin D supplementation. Nevertheless, the effect modification was similar in all three datasets, indicating no preventive effects of vitamin D supplementation on pneumonia risk in patients using vitamin D alongside drugs that affect bone mineralisation.
The major strengths of this project are the very large numbers of patients, extensive adjustment for confounding, and the fact that we studied the same association in three cohorts in different settings with respect to pneumonia diagnosis and hospitalisation status. The fact that comparable results were observed adds to the robustness of the findings. Furthermore, the three studies were conducted in the same country and time period, limiting the possibility of differences in medical guidelines, insurance policy or socioeconomic situation as sources of heterogeneity.
There are limitations to our project that need to be addressed. First, the absence of an association might be caused by residual confounding as a result of missing information on medical diagnoses. Proxies, varying in robustness, were used as indicators for comorbidity and therefore only patients treated with medication were recognised as having a comorbid illness. This could also be an explanation for the unexpected ORs above 1 in study 3, in which, in contrast to studies 1 and 2, only drug prescription data and not dispensing data were available. This could have led to a lower prevalence of medications prescribed by specialists and hence a lower rate of comorbidities.
Second, data about over-the-counter vitamin D use were not available, something which might have led to an underestimation of the true effects of vitamin D supplementation on pneumonia risk. However, we think that such information bias is unlikely to lead to a protective association being missed because controls would have to use twice as much over-the-counter vitamin D compared with the cases and prevent the doctor from prescribing.
Third, it was not possible to adjust for baseline vitamin D status because 25-hydroxyvitamin D levels in blood were not available. Possibly, vitamin D was not supplemented adequately enough to correct vitamin D status to normal. It cannot be ruled out that for prevention of pneumonia, larger amounts of vitamin D are needed to acquire an effect. The small number of patients receiving high-dose vitamin D supplements in the present study precluded a thorough analysis of dose dependency. However, this project also did not show a trend towards any dose dependency. Finally, we were not able to verify pneumonia diagnosis in all studies. In study 1 all pneumonia diagnoses were radiographically confirmed, but in studies 2 and 3 patients were selected from administrative databases. However, the patient characteristics of study 2 are very similar to those of study 1 and several studies have shown high positive values for pneumonia coding in administrative databases.28 ,29
In conclusion, three large independent case–control studies showed no preventive association between vitamin D supplementation and pneumonia. In patients using vitamin D supplementation without drugs that affect bone mineralisation or oral corticosteroids, the risk of pneumonia was increased. This might indicate unmeasured confounding, insufficient supplementation or a true risk. Further research is necessary to explore the interaction between vitamin D supplementation and concurrent drugs on the risk of developing pneumonia.
Acknowledgments
The authors thank the staff of NIVEL/the NPCRD for their help in data collection and data extraction.
References
Footnotes
-
Contributors HHFR and SMCS performed the data analysis and interpretation, and drafted the manuscript. JJO and WJWB were involved in data interpretation and revised the manuscript critically for important intellectual content. MCHdG and EMWvdG designed the study, were involved in data analysis and interpretation, and revised the manuscript critically for important intellectual content. All authors had full access to the data and can take responsibility for the integrity of the data and the accuracy of the data analysis. All authors approved the final version of the manuscript. MCHdG is the guarantor. MCHdG and EMWvdG shared senior authorship.
-
Competing interests None.
-
Ethics approval For ANTONIUS cases, the original studies were approved by the local Medical Ethics Committee and all patients gave written informed consent. For PHARMO / NPCRD cases and controls, this was not applicable.
-
Provenance and peer review Not commissioned; externally peer reviewed.
Linked Articles
- Airwaves