Article Text

Abstract
The British Thoracic Society guideline for the investigation and management of pulmonary nodules is published as a supplement to this edition of the journal. It provides recommendations for the management of an individual with single or multiple pulmonary nodules and is a comprehensive reference text.
- Imaging/CT MRI etc
- Bronchoscopy
- Lung Cancer
- Thoracic Surgery
Statistics from Altmetric.com
Pulmonary nodules are a frequent finding on CT, and their management continues to occupy many hours of debate. Decisions can sometimes be based on preference of the clinician rather than on that of the patient following evidence-based advice and discussion. Until recently, there was a limited research base, with a profusion of review articles based on the same research. In 2005, guidelines were published by the Fleischner Society, which dealt with the difficult problem of the increasingly common detection of smaller nodules by CT.1 These guidelines have been largely adopted in the UK, resulting in many follow-up CTs for the commonly detected smaller nodules. More recently, the Fleischner Society published guidelines on sub-solid nodules,2 and there have been two guidelines from the American College of Chest Physicians, the latest update in 2013.3 The British Thoracic Society (BTS) guideline is published this month. One-third of the 359 references cited is from 2012 onwards, reflecting the considerable progress in the evidence base, which has resulted in significant changes in the recommendations compared with the aforementioned guidelines.
The BTS guideline suggests standardisation of the terminology applied to pulmonary nodules, classifying them by using the terms solid and sub-solid nodule (SSN), and further dividing the sub-solid category into part-solid nodule (PSN) and pure ground glass nodules (pGGN) (see figure 1). The terms non-solid, semisolid and pure ground glass opacity are more ambiguous, and should be avoided.
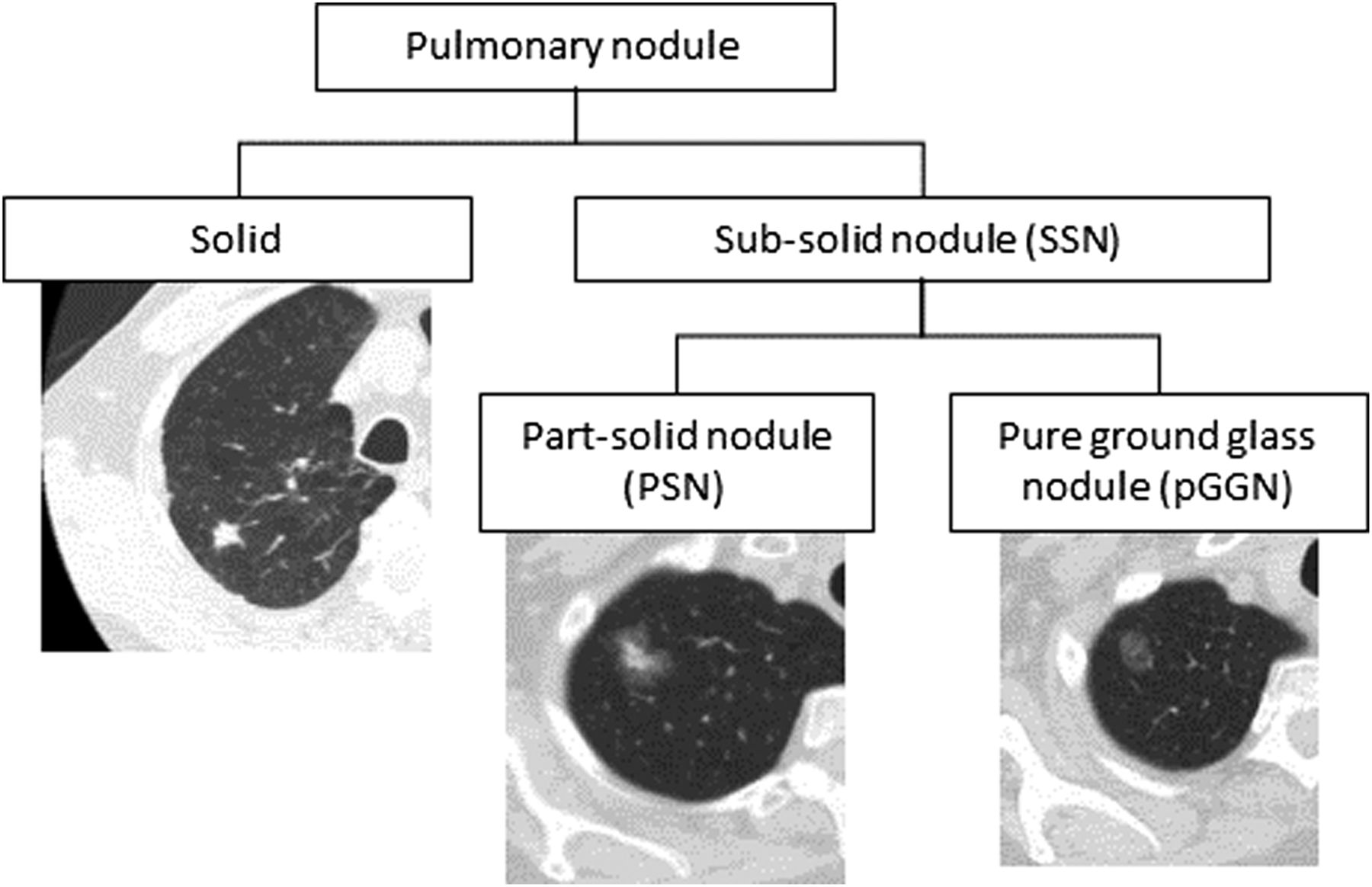
The classification and CT appearance of pulmonary nodules.
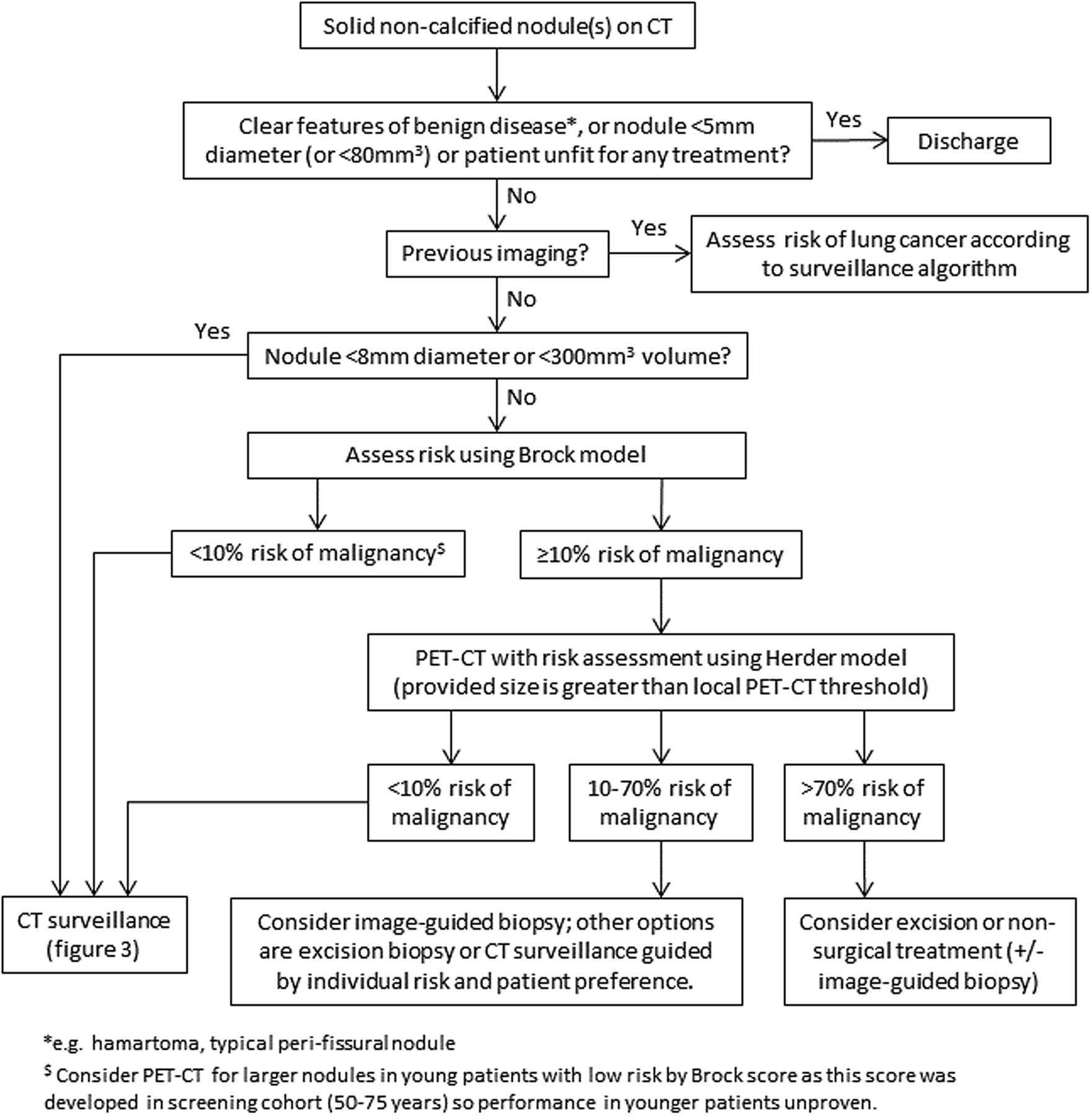
Figure 2 shows the first of the four algorithms that appear in the full guideline, illustrating the evidence-based approach to the initial assessment of solid nodules. This shows that nodules measuring <5 mm in diameter or those with a volume of <80 mm3 do not require further follow-up. This recommendation is based on a large body of evidence from screening trials showing that these nodules have a very low chance of being malignant, and in one large trial, the risk of developing cancer was no greater than in subjects with no nodule detected.4 This will reduce the need for follow-up imaging for many people. Inevitably, very occasional cancers <5 mm in diameter will be missed, but the frequency of this occurrence will be low, and the yield of ongoing surveillance in these patients appears to relate to their background risk of cancer rather than to the nodule itself.

Initial approach to solid pulmonary nodules.
The algorithm also shows that for nodules ≥8 mm in diameter (or ≥300 mm3 volume), initial assessment of risk of malignancy should use the Brock University tool5 (table 1). This model shows the highest accuracy for predicting malignancy, and has also recently been validated in a UK population where the area under the receiver operating characteristic curve (AUC) was 0.90.6 For nodules where the probability of malignancy is <10% (and for those nodules ≥5 to <8 mm in diameter/ ≥80 to <300 mm3 volume), ongoing CT surveillance is recommended. Where the probability of malignancy equals or exceeds 10%, positron emission tomography (PET)-CT is recommended, with the findings used to further assess the risk using the tool described by Herder et al7 (table 1). The latter tool was derived from the Mayo Clinic model,8 but with the findings of PET added; it had the highest accuracy in the UK population (AUC 0.92).6 Management is then guided by risk.
The Brock and Herder risk-prediction models
The merits of biopsy of indeterminate lesions were examined. As with any diagnostic test, the post-test probability of malignancy (following a non-malignant CT biopsy) will depend on the pre-test probability. Negative likelihood ratios were calculated from the 10 studies of transthoracic needle biopsy, with a total number of 1568 cases. The negative likelihood ratio was shown to be 0.10, (95% CI 0.08 to 0.12). When a biopsy is negative (ie, non-malignant), there is still approximately a 50% chance of malignancy where the pre-test probability is 90%. These calculations were recently confirmed in the largest retrospective series where there was a 90% prevalence of malignancy.9 The authors emphasised the importance of considering repeat biopsies as they also showed that these usually confirmed the diagnosis of malignancy. The utility of biopsy is greatest for nodules of intermediate malignancy risk (10%–70% pre-test probability), and is the preferred option for this group, although as with all other aspects of decision-making, this must be guided by an informed discussion with the patient.
Surveillance recommendations have also changed (figure 3). Semiautomated volumetry is now the preferred method of assessment of nodule size and volume doubling time (VDT). This method has shown improved accuracy compared with manual calliper measurement of nodule diameter. Volumetry is able to detect nodule growth at a rate consistent with malignancy at an earlier time point during surveillance thereby allowing more prompt intervention, at a 3-month interval scan. By using volumetry, it is also possible to more confidently demonstrate stability at 1-year follow-up, thus allowing earlier discharge of people with nodules compared with current practice. The guideline recommends immediate further assessment for nodules that show a VDT of ≤400 days and either biopsy or further observation for nodules with VDTs of between 400 and 600 days (see figure 3). People with nodules that have a VDT >600 days (measured by volumetry) have a very low risk of malignancy, and can be offered the option of discharge. In situations where volumetric analysis is either not possible or not available, surveillance for 2 years is recommended, as is the current practice.

Solid pulmonary nodule surveillance algorithm. VDT, volume doubling time.
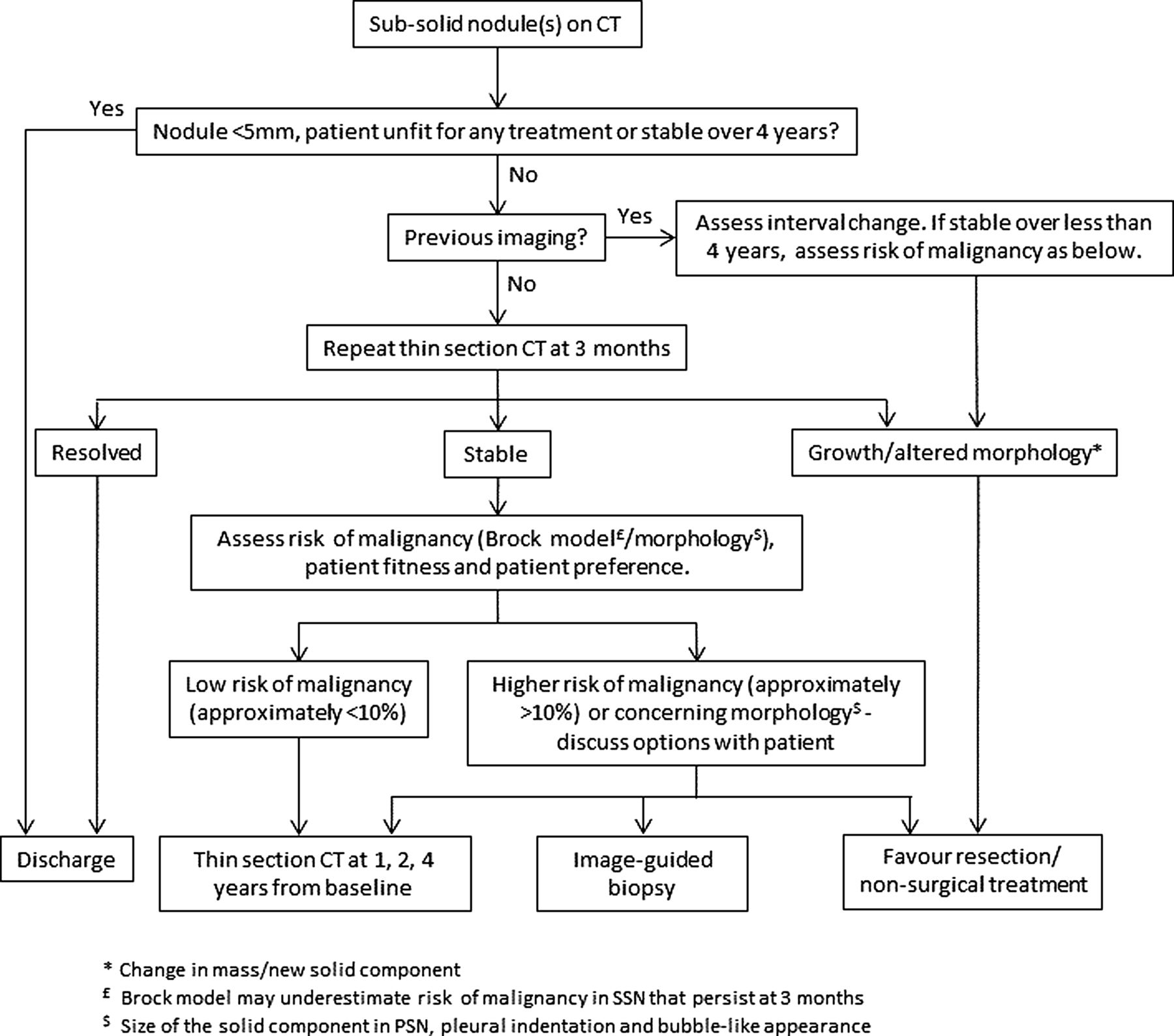
SSNs have their own section and management algorithm (figure 4). This reflects the very different growth characteristics and prognosis that these lesions confer. An initial 3-month interval thin-section CT is recommended for nodules ≥5 mm because up to one-third of these lesions may resolve. After that, management is governed by risk assessment using the Brock tool, with the proviso that it may underestimate risk (as it was developed using baseline CT data and, therefore, included those non-malignant nodules that resolved by 3 months). The risk assessment of these nodules should also take into account specific features that predict malignancy such as size of solid component, a bubble-like appearance and pleural indentation. SSNs may have longer VDTs, and these lesions may have a good prognosis even when resection is delayed. In light of this, surveillance is recommended for 4 years before discharge, and discussion of management options with patients together with an assessment of fitness, life expectancy and competing comorbidities is of paramount importance.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Subsolid pulmonary nodules algorithm. PSN, part-solid nodule; SSN, subsolid nodule.
Recommendations about treatment options for nodules depend on the fitness of the individual for surgery. Lobectomy is the treatment of choice or anatomical segmentectomy where preservation of functioning lung is important. If a diagnostic wedge resection is performed, this should be followed by frozen section and definitive anatomical resection during the same anaesthetic. Sublobar resection is recommended for pGGN, but there was insufficient evidence to make the same recommendation for PSN. Nodule localisation techniques are recommended prior to surgery for smaller nodules. Where fitness levels preclude surgery, non-surgical treatment with stereotactic ablative radiotherapy or radiofrequency ablation is recommended, even where biopsy is not possible, provided the probability of malignancy is high.
Recommendations about the information needs of patients with pulmonary nodules were based on four qualitative papers. All showed the importance of a well-structured approach, including a discussion about risk, harms of investigation and options for surveillance, biopsy or treatment.
The BTS guideline has significant implications for radiology teams who will be essential for successful implementation. The guideline makes recommendations to include semiautomated volumetry to evaluate nodules at baseline and to calculate VDT. Thin-section CT is recommended with the option of other post-processing techniques to increase accuracy of assessment. It is anticipated that the higher size threshold for discharge may offset the additional time taken for volumetry. It is also recommended that PET-CT scans be reported according to a new four-point ordinal scale so that the Herder model can be employed in risk prediction.
A short service organisation section was added following stakeholder comment, which suggests that a local, dedicated nodule service may be the best way to manage people with nodules (and implement the guideline). To further assist with implementation, the two recommended risk calculators and a tool for calculating VDT are available on the BTS website (https://www.brit-thoracic.org.uk/guidelines-and-quality-standards/pulmonary-nodules/).
The guideline is based on an extensive and detailed review of the published literature relating to the management of pulmonary nodules. It is intended to be used both as a summary in the day-to-day management of the person with a pulmonary nodule as well as a comprehensive reference text. It is hoped that implementation of the recommendations will lead to a more evidence-based and cost-effective approach to this, often debated, area of respiratory medicine.⇑
Footnotes
Contributors DRB and MEJC were responsible for the conception, drafting and final approval of the article.
Competing interests None declared.
Provenance and peer review Commissioned; internally peer reviewed.