Article Text

Statistics from Altmetric.com
Pneumonia is characterised by a disturbed alveolar fibrin turnover which is the net result of activation of coagulation and attenuation of fibrinolysis.1,2 We have recently shown, in patients developing ventilator associated pneumonia (VAP), that suppression of fibrinolysis precedes the clinical diagnosis while procoagulant effects mainly occur afterwards.2 We have extended these findings by investigating the relationship in time between changes in the anticoagulant protein C (PC) pathway and VAP.
Levels of PC, activated PC (APC), and soluble thrombomodulin (sTM) were measured in non-directed bronchial lavage fluid collected every other day from critically ill patients during mechanical ventilation. APC was measured with an enzyme capture assay using monoclonal antibody HAPC 1555 and chromogenic substrate Spectrozyme PCa (American Diagnostica, Greenwich, CT, USA);3 PC activity was measured with an amidolytic assay using chromogenic substrate S2366 (Chromogenix, Milan, Italy); and sTM was measured with an ELISA (Diagnostica Stago, Asnières-sur-Seine, France). Serial data from patients were evaluated using analysis of repeated measures with a linear mixed model, as described previously.2 Data are presented as medians (interquartile ranges).
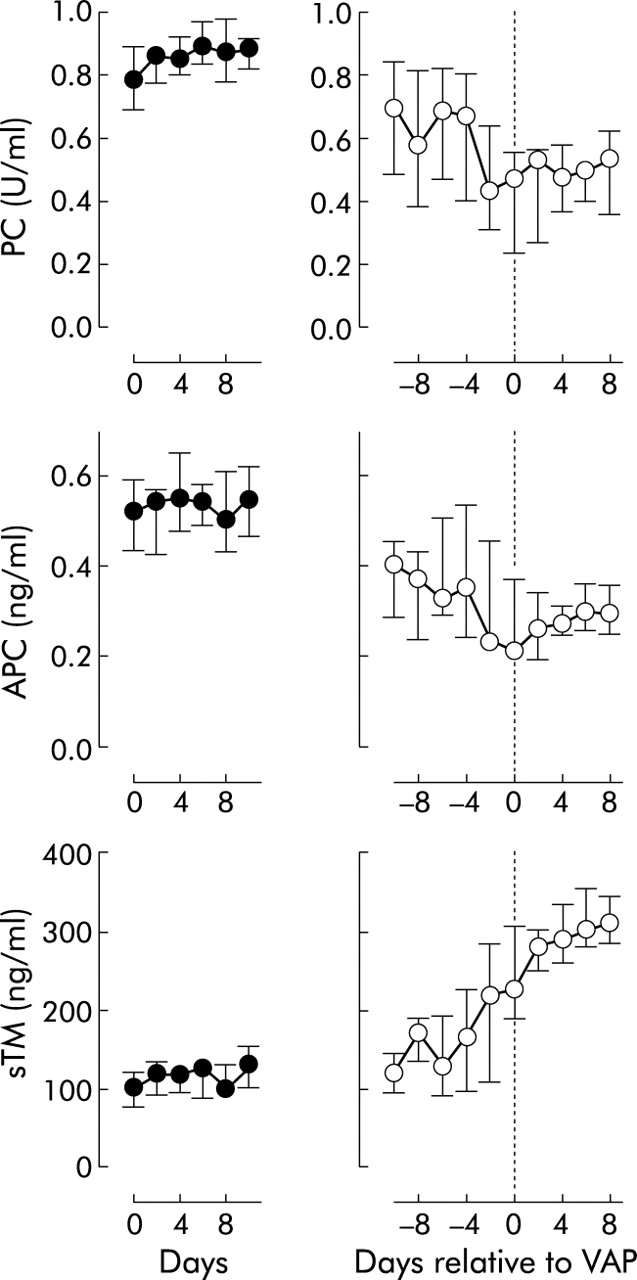
The patient population was as previously described.2 In short, specimen collection was initiated in 60 consecutive patients; 28 patients were selected for final analysis, which required at least three sample sets (minimum ventilation duration ⩾5 days). Nine patients developed VAP and 19 showed no signs of pulmonary infection during the clinical course. There were no significant differences between patients who did and did not develop VAP with regard to baseline characteristics, mechanical ventilation settings, and baseline levels of PC, APC, and sTM. Median (IQR) baseline concentrations for patients without and with VAP were as follows: PC: 0.78 (0.69–0.89) v 0.82 (0.72–0.90) U/ml; APC: 0.52 (0.44–0.59) v 0.47 (0.36–0.59) ng/ml; sTM: 102 (79–123) v 98 (75–131) ng/ml (differences not statistically significant). In patients who developed VAP the clinical diagnosis was preceded by a fall in pulmonary PC levels, as measured in lavage fluids, from 0.69 (0.45–0.86) U/ml before VAP to 0.47 (0.24–0.56) U/ml on the day of diagnosis of VAP (p<0.0001; fig 1). In patients who did not develop VAP, pulmonary PC levels remained unchanged (p = 0.07). The decline in PC levels in the infected lungs was accompanied by a decrease in levels of APC, which fell from 0.40 (0.25–0.46) ng/ml before VAP to 0.21 (0.21–0.37) ng/ml on the day of diagnosis (p<0.01; fig 1). The suppression of APC occurred before the clinical diagnosis of VAP was made. Furthermore, in patients who developed VAP a significant increase in sTM levels was observed. Local levels of sTM increased from 95 (120–151) ng/ml before VAP to 214 (186–312) ng/ml on the day of diagnosis (p<0.0001; fig 1), thereafter increasing to 274 (311–362) ng/ml 8 days after VAP was diagnosed. In patients who did not develop VAP during the study, sTM increased to a lesser extent from 102 (79–123) ng/ml at admission to 130 (102–156) ng/ml on day 10 of mechanical ventilation (p<0.01; fig 1).
{kind=link}
Levels of protein C (PC), activated protein C (APC), and soluble thrombomodulin (sTM) in non-directed bronchial lavage fluid prospectively collected in mechanically ventilated patients. Left panels: patients who did not develop pneumonia; day 0 denotes start of mechanical ventilation. Right panels: patients who developed ventilator associated pneumonia (VAP); day 0 corresponds to the day at which VAP was clinically diagnosed. Data represent medians with interquartile ranges.
In sepsis, low levels of APC contribute, at least in part, to the systemic procoagulant shift of the haemostatic balance, potentially evolving into disseminated intravascular coagulation.4 Correction of the systemic haemostatic balance has been acknowledged as a pivotal goal in the treatment of patients with sepsis. Indeed, treatment with recombinant human APC has been found to reduce mortality in patients with severe sepsis.5 Our results show that, during the pathogenesis of pneumonia, the PC pathway is locally suppressed. We suggest that this is the net result of increased PC consumption, cleavage of PC by neutrophil elastase, as well as inadequate PC activation due to oxidation of TM and shedding of TM from the cell surface (resulting in soluble fragments of TM).4 Presumably, the insufficient anticoagulant PC system contributes to the local procoagulant environment at the site of infection during pneumonia. Correction of the local PC system may be a target in the treatment of pneumonia.
Footnotes
-
This study was funded in part by the Oxford Health Services Research Committee (research project number 593).
-
The authors thank Gerrit-Jan Weverling for assistance and advice with regard to the statistical analyses.
The study protocol was reviewed and approved by the Central Oxford regional ethics committee.