Article Text

Abstract
Background: The external intercostal muscles are chronically exposed to increased inspiratory loading and to continuous hypoxia-reoxygenation cycles in patients with obstructive sleep apnoea syndrome (OSAS). It was therefore hypothesised that oxidative stress levels would be increased in these muscles, and that treatment with continuous positive airway pressure (CPAP) would modify the oxidative stress levels and improve muscle dysfunction.
Methods: A case-control study and a case-case study were conducted on the external intercostal muscles of 12 patients with severe OSAS (before and after 6 months of treatment with CPAP) and 6 control subjects. Reactive carbonyl groups, malondialdehyde (MDA)-protein and hydroxynonenal (HNE)-protein adducts, antioxidant enzyme levels, 3-nitrotyrosine and fibre type proportions were measured using immunoblotting and immunohistochemistry.
Results: Compared with controls, the intercostal muscles of patients with OSAS had higher levels of protein carbonylation (median values 3.06 and 2.45, respectively, p = 0.042), nitration (median values 1.64 and 1.05, respectively, p = 0.019) and proportions of type I fibres (median values 57% and 48%, respectively, p = 0.035) and reduced respiratory muscle endurance (median values 3.2 and 9.5 min, respectively, p = 0.001). Positive correlations were found between MDA-protein and HNE-protein adducts (r = 0.641, p = 0.02 and r = 0.594, p = 0.05, respectively) and 3-nitrotyrosine (r = 0.625, p = 0.03) and the apnoea-hypopnoea index (AHI) in all the patients with OSAS. Although treatment with CPAP significantly improved the AHI and oxygen desaturation, muscle oxidative stress levels and respiratory muscle endurance were not affected.
Conclusions: This study suggests that inspiratory muscle performance is not completely restored after long-term treatment with CPAP.
Statistics from Altmetric.com
Obstructive sleep apnoea syndrome (OSAS) is a highly prevalent condition characterised by recurrent upper airway obstruction during sleep.1 As inspiratory muscles of patients with OSAS must generate greater negative intrathoracic pressures than usual in order to overcome the obstructive apnoea, they may be subjected to mechanical overloading.2 The diaphragm appears to be the primary inspiratory muscle during apnoea in some patients with OSAS, while the intercostals muscles are the main inspiratory muscles in other patients.2 Indeed, hypercapnic respiratory failure has been recognised in patients with severe OSAS.3 Furthermore, in patients with OSAS, daytime ventilatory muscle force and diaphragm strength were both shown to be preserved while inspiratory muscle endurance was significantly reduced.4 Interestingly, the administration of nocturnal continuous positive airway pressure (CPAP) to these patients attenuated the decrease in respiratory muscle resistance.4 However, the underlying mechanisms of this respiratory muscle dysfunction in OSAS are still unknown.
Reactive oxygen species (ROS) are usually synthesised at low levels in muscles and are required for normal force generation. Their levels progressively increase in response to muscle activation, and excessive production of ROS results in oxidative stress which, in turn, leads to a decline in muscle force production. Oxidative stress has been implicated in the pathogenesis of different chronic conditions5 6 and in aging.7 Importantly, increased superoxide anion production and lipid peroxidation have been reported in the blood of patients with OSAS with and without cardiovascular disease.8 9 Furthermore, a growing body of evidence shows that oxidative stress is one of the mechanisms clearly involved in skeletal muscle dysfunction in different conditions such as chronic obstructive pulmonary disease (COPD) and sepsis.10–14
Few studies have examined whether oxidative stress develops in the respiratory muscles of patients with OSAS. On the grounds that the production of ROS within skeletal muscle fibres is regulated in part by strong muscle contractions, and that during night time patients with severe OSAS are chronically exposed to increased inspiratory muscle loading and to continuous hypoxia-reoxygenation cycles, we hypothesised that their respiratory muscles might generate increased levels of oxidative stress. To test this hypothesis we first sought to determine the levels of protein carbonylation and nitration in the external intercostal muscles of patients with OSAS compared with a control group of subjects and to examine whether CPAP treatment can reduce these levels. We then explored the levels of several antioxidant mechanisms in these muscles and finally investigated whether oxidative stress indices were associated with either the severity of the disease or respiratory muscle function of such patients.
METHODS
Subjects
All individuals were Caucasian. Twelve consecutive male patients with a polysomnographically confirmed diagnosis of OSAS (clinic referrals recently diagnosed and without CPAP therapy) were included. Six male healthy non-smoker controls with similar anthropometric characteristics without OSAS, as indicated by clinical history and a negative sleep study (polysomnography), were also recruited from the general population. The sample size of both patient and control populations was calculated on the basis of formerly published studies by our group where similar physiological and biological approaches were used.10 12 13 Exclusion criteria included previous treatment with CPAP, female sex in order to avoid sex-related effects on muscles,15 COPD, bronchial asthma, cardiovascular disease, chronic metabolic diseases including diabetes, suspected paraneoplastic or myopathic syndromes and/or treatment with drugs known to alter muscle structure and/or function (see additional information in online supplement available at http://thorax.bmj.com/supplemental).
Study design
This study had a twofold design: case-control (OSAS patients vs controls) and case-case (OSAS patients before and after treatment with CPAP). The study was designed in accordance with both the ethical standards on human experimentation in our institution and the World Medical Association guidelines for research on human beings. The Ethics Committee on Human Investigation at the Institute of Tuberculosis and Lung Diseases in Warsaw approved all experiments. Informed written consent was obtained from all individuals.
Clinical, nutritional and functional assessment
Clinical evaluation included medical history, a complete physical examination, thorax radiography and electrocardiogram. Nutritional evaluation included anthropometric and analytical parameters. Pulmonary and respiratory muscle function, general exercise capacity and peripheral muscle strength were evaluated16–20 (see additional information in online supplement available at http://thorax.bmj.com/supplemental).
Polysomnography
Standard polysomnographic examination was performed in the sleep laboratory according to the standards of the American Sleep Disorders Association.21 The diagnosis of OSAS was established by obtaining an apnoea-hypopnoea index (AHI) of >10/h of sleep.4 8 9 21 When the diagnosis of OSAS was clearly established, patients underwent a second polysomnographic examination for manual CPAP titration. CPAP treatment (REMstar, Respironics, Murrysville, Pennsylvania, USA) was applied to all patients for at least 6 months. Adherence to CPAP treatment over this period was monitored by the built-in time counter in the CPAP device. Good compliance with treatment was established as a mean usage of CPAP of >4 h/night. All patients also completed the Epworth Sleepiness Scale (ESS)22 (normal: ESS score <10; borderline: ESS score 10–12; excessive sleepiness: ESS score >12) before and after the 6-month CPAP treatment period. CPAP treatment was administered to all patients 7–10 days after undergoing baseline muscle biopsy surgery (see additional information in online supplement available at http://thorax.bmj.com/supplemental).
Muscle biopsies
Biopsy specimens (≈40 mg) were taken from the external intercostal muscles before and after the 6-month period of treatment with CPAP following procedures published elsewhere23 (see additional information in online supplement available at http://thorax.bmj.com/supplemental).
Biological muscle studies
All the muscle biology analyses were conducted in a blind manner in the same laboratory at Hospital del Mar-IMIM, Barcelona.
Immunoblotting
The effects of oxidants on muscle proteins and lipids were evaluated according to methods published elsewhere.10 12–14 Immunoblotting experiments were specifically designed so that muscle homogenates from control subjects (n = 6) and from patients with OSAS before (n = 12) and after (n = 12) CPAP treatment were always run together and kept in the same order. The following antibodies were used to detect the different antigens and phenomena: anti-DNP moiety antibody (Oxyblot kit, Chemicon International Inc, Temecula, California, USA), anti-MDA antibody (Academy Bio-Medical Company Inc, Houston, Texas, USA), anti-HNE antibody (Alpha Diagnostics International Inc, San Antonio, Texas, USA), anti-3-nitrotyrosine antibody (Cayman Chemical Inc, Ann Arbor, Michigan, USA), anti-Mn SOD antibody (StressGen, Victoria, BC, Canada) and anti-catalase antibody (Calbiochem, San Diego, California, USA). Blots were scanned with an imaging densitometer and optical densities (OD) of specific proteins were quantified with Diversity Database 2.1.1 (BioRad, Philadelphia, Pennsylvania, USA) (see additional information in online supplement available at http://thorax.bmj.com/supplemental).
Immunohistochemistry
Immunohistochemical experiments were performed according to methods published elsewhere.10 12 Briefly, myosin heavy chain I and II isoforms were identified on 3 μm muscle paraffin embedded sections using anti-myosin heavy chain I (clone MHC, Biogenesis Inc, Poole, UK) and anti-myosin heavy chain II (clone MY-32, Sigma, St Louis, Missouri, USA) primary antibodies, respectively, as well as markers of oxidative stress.
Statistical analysis
Data are presented as median (interquartile range) values in table 1 and as box and whisker plots in the figures. Mann-Whitney non-parametric tests were used for comparisons between controls and patients with OSAS at baseline, and the Wilcoxon test was used to compare variables before and after CPAP treatment in patients with OSAS. Spearman’s coefficient was used to assess correlations between biological and physiological variables among the patients with OSAS. A p value of ⩽0.05 was considered significant.
RESULTS
Characteristics of study subjects
Table 1 shows the main characteristics of the control subjects and patients with OSAS at baseline and after CPAP treatment. No significant differences in age, nutritional status (as assessed by body mass index) or lung function parameters were observed between control subjects and patients with OSAS before CPAP treatment. However, the following sleep variables were significantly reduced in the patients before CPAP treatment compared with control subjects: mean arterial oxygen saturation (Sao2) during the night, nadir Sao2 and time spent at Sao2 <90%. The ESS score was significantly increased in patients (>12), indicating excessive sleepiness compared with controls (<10). Interestingly, all these parameters significantly improved after CPAP treatment for 6 months. Patients adequately complied with CPAP treatment, with a mean usage of 5.4 h. Exercise capacity and respiratory and peripheral muscle strength were preserved in patients with OSAS and were not significantly modified after CPAP treatment. In contrast, endurance time of the respiratory muscles was significantly reduced in patients with OSAS compared with controls and did not improve after CPAP treatment.
Muscle structure
The proportion of type I fibres was significantly increased while the proportion of type II fibres was decreased in the intercostal muscles of patients with OSAS compared with controls (table 1). Interestingly, after CPAP treatment the proportions of fibres were significantly reversed to values observed in control subjects.
Protein carbonylation
Total carbonyl group formation
The intercostal muscles of the patients had significantly higher levels of protein carbonylation than control muscles (median values 3.06 and 2.45, respectively, p = 0.042; fig 1A). In the patients with OSAS a significant inverse relationship was found between protein carbonylation and nadir Sao2 (r = −0.711, p = 0.032). An almost significant inverse correlation (r = −0.643, p = 0.1) was also found between protein carbonylation and the endurance time of the respiratory muscles in patients with OSAS. No other correlations were observed between protein carbonylation and lung or respiratory muscle function, sleep variables or exercise tolerance. The levels of total protein carbonylation were not significantly reduced after CPAP treatment in patients with OSAS (median value 3.39, p = 0.859; fig 1A). Immunostaining with anti-DNP antibody revealed the presence of carbonyl groups diffusely localised within the intercostal muscle fibres in patients with OSAS and control subjects (fig 1B).

MDA-protein adduct formation
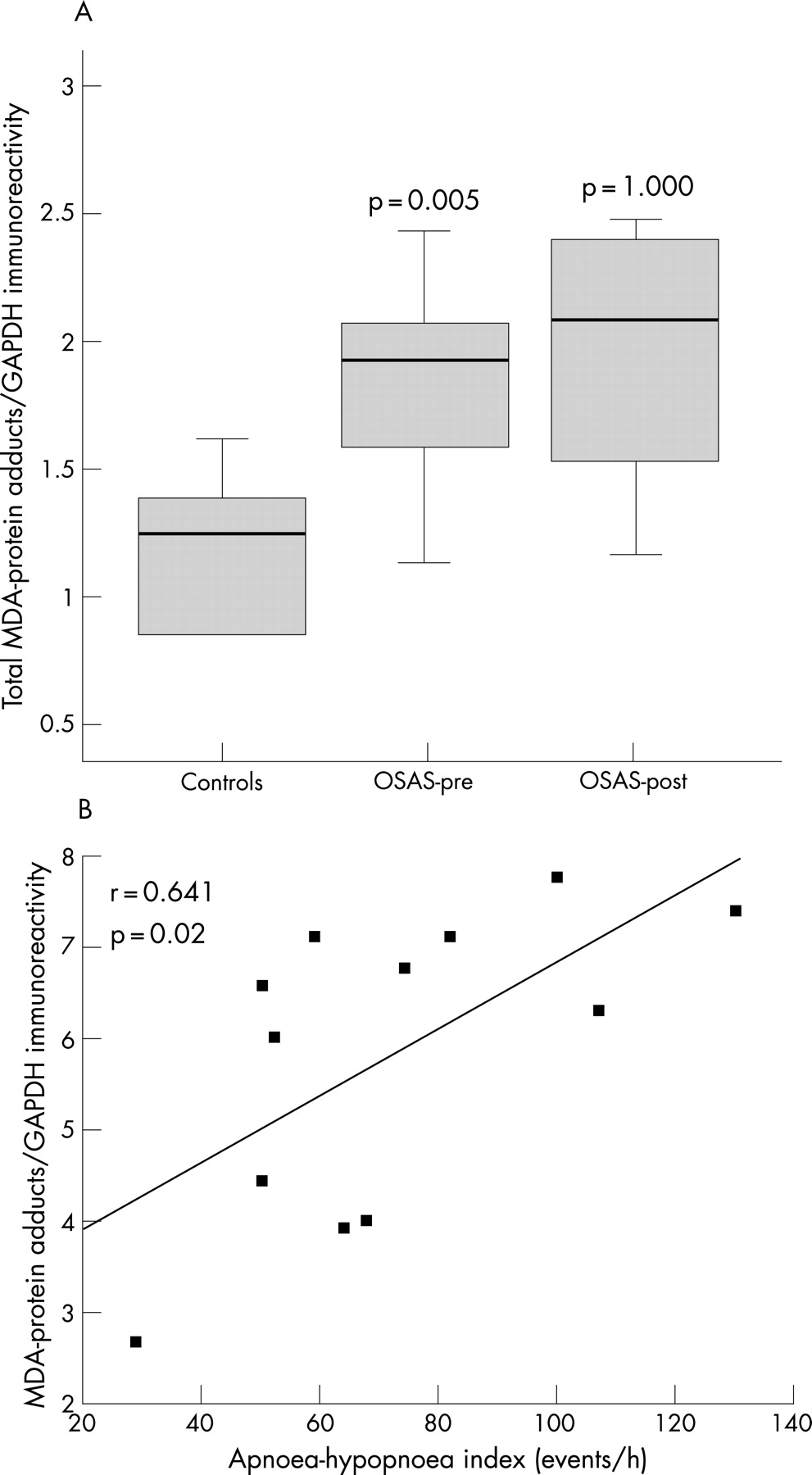
The intercostal muscles of the patients with OSAS had significantly higher levels of MDA-protein adducts than those of the controls (median values 1.91 and 1.24, respectively, p = 0.005; fig 2A). Among all patients with OSAS, the intensity of total intercostal MDA-protein adducts directly correlated with the severity of their disease as measured by the AHI (fig 2B). No other correlations were observed between MDA-protein adduct levels and lung or respiratory muscle function, sleep variables or exercise tolerance. The levels of MDA-protein adducts were not significantly reduced after CPAP treatment in patients with OSAS (median value 2.07, p = 1.0; fig 2A).

HNE-protein adducts
The intercostal muscles of the patients with OSAS had significantly higher levels of HNE-protein adducts than control muscles (median values 1.15 and 0.63, respectively, p = 0.002; fig 3). Among all patients with OSAS, the intensity of total intercostal HNE-protein adducts directly correlated with the severity of their disease as measured by the AHI (r = 0.594, p = 0.05). No other correlations were observed between HNE-protein adducts and lung or respiratory muscle function, sleep variables or exercise tolerance. The levels of HNE-protein adducts were not significantly reduced after CPAP treatment in patients with OSAS (median value 0.87, p = 0.327; fig 3).

Protein tyrosine nitration
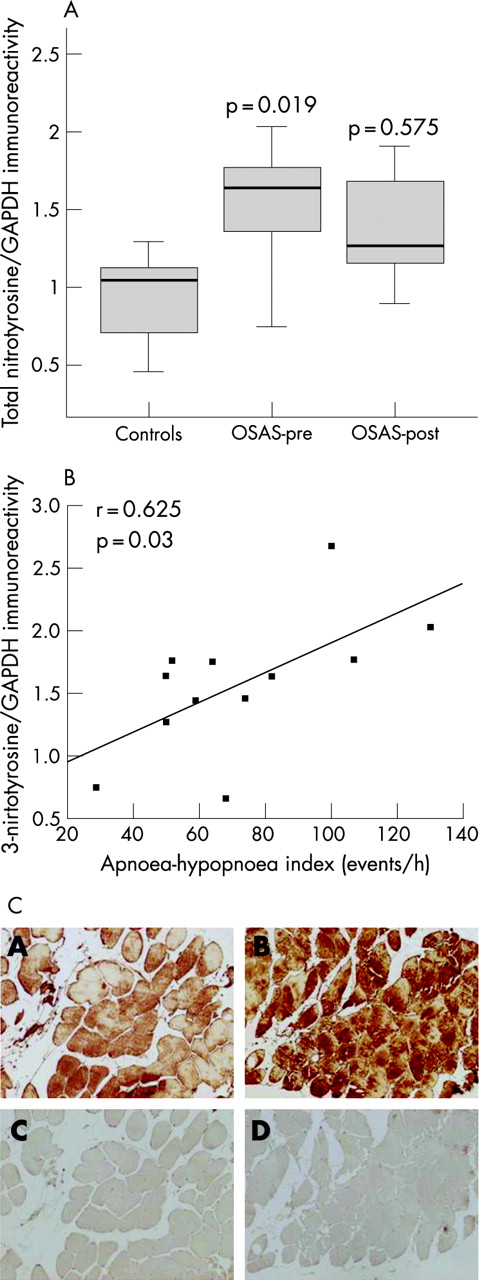
The intercostal muscles of the patients with OSAS had significantly greater levels of tyrosine nitrated proteins than control muscles (median values 1.64 and 1.05, respectively, p = 0.019; fig 4A). Among all patients with OSAS, the intensity of total 3-nitrotyrosine immunoreactivity positively correlated with the severity of their disease as measured by the AHI (fig 4B). No other correlations were observed between protein tyrosine nitration and lung or respiratory muscle function, sleep variables or exercise tolerance. The levels of 3-nitrotyrosine immunoreactivity were not significantly reduced after CPAP treatment in patients with OSAS (median value 1.27, p = 0.575; fig 4A). Immunostaining with anti-nitrotyrosine antibody revealed the presence of tyrosine nitrated proteins diffusely localised within the intercostal muscle fibres in both patients with OSAS and controls (fig 4C).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Antioxidant enzymes
Both manganese superoxide dismutase and catalase were detected in the external intercostal muscles of patients with OSAS and controls. No significant differences in the intensity of manganese superoxide dismutase (median values 0.99 and 0.88, respectively, p = 0.437) or catalase (median values 1.13 and 1.09, respectively, p = 0.964) were observed between the two groups. The levels of manganese superoxide dismutase (median value 0.66) or catalase (median value 1.23) were not significantly modified after treatment with CPAP in patients with OSAS (p = 0.674 and p = 0.263, respectively).
DISCUSSION
The main findings of this study are that, in the external intercostal muscles of patients with OSAS compared with those from control subjects:
the endurance time of the respiratory muscles was significantly reduced;
reactive carbonyl group levels were significantly increased and inversely correlated with the nadir Sao2 and had an almost significant inverse relationship with the endurance time;
both MDA-protein and HNE-protein adducts were significantly greater and were correlated with the severity of the disease as measured by the AHI;
protein tyrosine nitration was significantly increased and also correlated with the severity of the disease;
the levels of the antioxidant enzymes were not significantly modified; and
the endurance time of the respiratory muscles and the levels of these four indices of oxidative stress remained unmodified after a 6-month period of treatment with CPAP.
Study model critique
Open thoracotomy is the gold standard technique to obtain biopsy specimens from the diaphragm, the main inspiratory muscle. However, this surgical practice can only be used for subjects with serious illnesses such as lung neoplasms. Furthermore, the external intercostal muscles were also shown to be the primary inspiratory muscles during apnoea in a subpopulation of patients with OSAS.2 Finally, clear accessibility of the external intercostal muscles by means of an open biopsy on an outpatient basis at two different time points, as well as the fact that this model enabled us to carefully select the subjects excluding any co-morbid condition, clearly justified the design of the current study.
Muscle structure and function
Other reports in the literature have already shown the proportions of types I and II fibres in the quadriceps and genioglossus muscles of patients with OSAS.24 25 The current study, however, is the first report on the morphometric analysis of one of the main inspiratory muscles, the external intercostal, in these patients. We have found a significant increase in the proportion of type I fibres in the intercostal muscles of patients with severe OSAS compared with controls. As these muscles must generate repeated bouts of increasing intrathoracic negative pressures in the face of apnoea throughout the entire night, one could argue that their fibres might switch to a more fatigue resistant phenotype, similar to that seen in other respiratory muscles in patients with chronic respiratory diseases such as COPD.12 However, respiratory muscle endurance time was significantly reduced in our population of patients with OSAS compared with control subjects of similar anthropometric characteristics. Although this could be somehow paradoxical, the fact that the respiratory muscles of patients with OSAS do not rest sufficiently during night time, and that their increased activity takes place during this part of the day, might account for these results.
Muscle oxidative stress before CPAP treatment
The present study is the first to provide evidence of the effects of ROS on muscle proteins and lipids of human intercostal muscles in severe OSAS. Oxidative stress, defined as the imbalance between oxidant production and antioxidant defences in favour of the former, has been implicated in the pathogenesis of several chronic conditions5 6 and in aging.7 It has also recently been suggested that oxidative stress is involved in the pathophysiology of OSAS, especially in that of cardiovascular morbidity.9
The inspiratory muscles of patients with OSAS do not rest sufficiently during night time because they have to generate increasing negative intrathoracic pressures to overcome upper airway obstruction. The lack of an adequate rest at night for the ventilatory muscles in OSAS might have deleterious consequences on muscle aerobic metabolism26 and on their daytime function,27 as well as on their antioxidant defences which, in turn, would increase oxidative stress.28 These negative biochemical events due to sleep deprivation probably counteract the training-like effects of the respiratory muscles secondary to the continuous ventilatory efforts. Furthermore, since our patients had very severe OSAS, as revealed by their AHI, it could be argued that the strong muscle contractions generated by their inspiratory muscles during the night might lead to a further increase in ROS production than that neutralised by their antioxidant systems. In fact, the patients with more severe OSAS were those with higher levels of oxidative and nitrosative stress in their intercostal muscles. Also, the higher percentage of oxidative fibres observed in the external intercostal muscles of our patients with OSAS before CPAP treatment would favour the increased production of oxidants within those fibres.
On the other hand, the recurrent upper airway obstruction during sleep leads to continuous hypoxia-reoxygenation cycles which, to a much lesser extent, resemble ischaemia-reperfusion effects on tissues. As this phenomenon was already shown to increase oxidative stress in patients with OSAS,8 9 it is reasonable to assume that continuous hypoxia-reoxygenation cycles occurring in the external intercostal muscles of our patients might also have contributed to enhance their oxidant production. Indeed, the patients with OSAS with the lowest nadir Sao2 values were those with higher levels of protein carbonylation in their external intercostal muscles. Moreover, our patients spent 80% of their sleep time at arterial oxygen saturations <90%, showing clear hypoxaemia during the night (mean Sao2 ≈84%, nadir Sao2 ≈65%), and chronic hypoxaemia has recently been shown to increase muscle oxidative stress in patients with COPD.29
The muscle content of the two antioxidant systems analysed in the current study showed similar levels to those observed in the external intercostal muscles of the control individuals. In fact, the antioxidant enzyme paraxonase-1 was shown to be reduced in another population of OSAS patients with cardiovascular disease.9 As previously reported,30 one could also speculate from these findings that, in patients with OSAS, either the content or the activity of these enzymes might be altered as well as the regulatory mechanisms responsible for their upregulation, enhancing muscle oxidative stress.
Muscle oxidative stress after CPAP treatment
CPAP treatment has been proved to be beneficial in reducing both apnoea-hypopnoea events and oxygen desaturations, in inducing reparative sleep, and may improve long-term survival of patients with OSAS.31 In our study a 6-month period of treatment with CPAP significantly improved some lung function parameters, reduced the severity of the disease in all patients, and significantly improved oxygen desaturations (mean Sao2, nadir Sao2 and time spent below 90% Sao2), and modified the proportions of muscle fibres to values observed in the control muscles. However, endurance time of the respiratory muscles, muscle protein carbonylation and nitration, and the antioxidant enzymes did not improve significantly after CPAP treatment. All our patients with OSAS had a high level of adherence to treatment with CPAP, with a mean usage time of ⩾4 h/night. Moreover, the ESS score decreased significantly after CPAP treatment to normal values (<10).
These findings can be explained by the fact that treatment with CPAP does not restore the optimal resting length of the inspiratory muscles. In fact, long-term treatment with CPAP increases lung volumes in patients with OSAS and normal lung function.32 In other words, despite the beneficial effects of CPAP treatment on physiological and clinical parameters, the inspiratory muscles remain in a disadvantageous state, hampering oxidative stress neutralisation. In this context, the loads imposed on the inspiratory muscles by the CPAP treatment would account for the persistence of increased levels of biomarkers of muscle oxidative stress and reduced endurance in our patients with OSAS.
The metabolic syndrome has also recently been associated with increased systemic oxidative stress levels.33 In our study the proportions of patients and controls with metabolic syndrome were similar (42% and 50%, respectively) and the increase in muscle oxidative stress biomarkers among the patients was independent of the metabolic syndrome. Moreover, after CPAP treatment muscle oxidative stress levels did not differ significantly between OSAS patients with metabolic syndrome and those without it (data not shown). We therefore conclude that OSAS, rather than the metabolic syndrome, contributes more to the increased oxidative stress levels in the external intercostal muscles of our patients.
In summary, molecular events occurring within the intercostal muscle fibres before CPAP treatment as a result of inadequate night time rest, chronic hypoxaemia, reduced muscle aerobic metabolism and the inefficiency of the antioxidant mechanisms might play a role in the respiratory muscle dysfunction observed in our population of patients with severe OSAS. CPAP treatment, however, failed to offset those deleterious effects on the intercostal muscles. It is also worth mentioning that, in a previous study by our group,4 it was shown that the reduced endurance of the respiratory muscles of patients with less severe OSAS was significantly improved after 2 months of treatment with CPAP. The fact that the patients in the present study had much more severe OSAS than those recruited in the former study might account for this discrepancy.
CONCLUSIONS
Our results provide first evidence that, in severe OSAS, the external intercostal muscles exhibit increased levels of oxidative stress and such levels are associated with the severity of the disease. A high level of adherence to CPAP treatment for 6 months does not significantly decrease these levels or improve respiratory muscle endurance, suggesting that inspiratory muscle performance is not completely restored after CPAP.
Further information is given in the online supplement available at http://thorax.bmj.com/supplemental.
Acknowledgments
The authors thank Francesc Sánchez, Sandra Mas and Beatriz de la Puente for their technical assistance in the laboratory and Roger Marshall for his assistance with editing.
REFERENCES
Supplementary materials
Files in this Data Supplement:
Footnotes
This study was supported by the European Network for the study of clinical and biological implications of Respiratory Muscle failure in patients with Chronic Obstructive Pulmonary Disease (ERESMUS in COPD) (BMTH4-CT98-3406) (EU) and RESPIRA (RTIC C03/11) (Spain).
Competing interests: None.
- Abbreviations:
- AHI
- apnoea-hypopnoea index
- COPD
- chronic obstructive pulmonary disease
- CPAP
- continuous positive airway pressure
- DNP
- 2-4 dinitrophenylhydrazone
- ESS
- Epworth sleepiness scale
- GAPDH
- glyceraldehyde-3-phosphate dehydrogenase
- HNE
- hydroxynonenal
- HRP
- horseradish peroxidase
- MDA
- malondialdehyde
- OD
- optical density
- OSAS
- obstructive sleep apnoea syndrome
- PVDF
- polyvinylidene difluoride
- ROS
- reactive oxygen species
- Sao2
- arterial oxygen saturation
- SOD
- superoxide dismutase