Article Text

Abstract
Complex respiratory events, which may have a detrimental effect on both quality of sleep and control of nocturnal hypoventilation, occur during sleep in patients treated with non-invasive ventilation (NIV). Among these events are patient-ventilator asynchrony, increases in upper airway resistance (with or without increased respiratory drive) and leaks. Detection of these events is important in order to select the most appropriate ventilator settings and interface. Simple tools can provide important information when monitoring NIV. Pulse oximetry is important to ensure that adequate oxygen saturation is provided and to detect either prolonged or short and recurrent desaturations. However, the specificity of pulse oximetry tracings during NIV is low. Transcutaneous capnography helps discriminate between hypoxaemia related to ventilation/perfusion mismatch and hypoventilation, documents correction of nocturnal hypoventilation and may detect ventilator-induced hyperventilation, a possible cause for central apnoea/hypopnoea and glottic closure. Data provided by ventilator software help the clinician by estimating ventilation, tidal volume, leaks and the rate of inspiratory or expiratory triggering by the patient, although further validation of these signals by independent studies is indicated. Finally, autonomic markers of sympathetic tone using signals such as pulse wave amplitude of the pulse oximetry signal can provide reliable information of sleep fragmentation.
- Non invasive ventilation
- respiratory muscles
- sleep apnoea
Statistics from Altmetric.com
Introduction
Home non-invasive ventilation (NIV) aims to correct daytime and nocturnal hypoventilation and associated symptoms and to ensure adequate nocturnal oxygen saturation measured by pulse oximetry (Spo2). During sleep, specific respiratory events may occur resulting both from sleep-related physiological changes and use of NIV.1 Among these events, described in another article in this series,2 are repetitive leaks, upper airway instability and residual obstructive events, recurrent decreases in ventilatory command with or without glottic closure, or patient-ventilator asynchrony. An appropriate strategy for monitoring these respiratory events is necessary. Monitoring tools can be limited to the recognition of their consequences such as oxygen desaturation or increases in transcutaneous carbon dioxide tension (Ptcco2). The latest generation of home ventilators3 are often equipped with sophisticated built-in software capable of recording a wide range of parameters over several months, and thus offering information to the clinician on items such as compliance and leaks, among many other respiratory parameters.
This review describes the contributions, limits and caveats of non-invasive assessment of NIV during sleep through simple techniques such as pulse oximetry, combined capnography and pulse oximetry, built-in ventilator software and autonomic markers of sleep fragmentation. More complex and complete evaluations can be performed by polygraphic or polysomnographic recordings which will be discussed in a later article in this series.2
Pulse oximetry and non-invasive ventilation
Nocturnal oxygen desaturation is considered as one of the major determinants of adverse neurocognitive and cardiovascular consequences occurring during chronic respiratory failure and sleep apnoea syndrome.4–6 Pulse oximetry has the advantages of simplicity, short set-up time and short time response (seconds); disadvantages are motion artefacts and sensitivity to perfusion. Information provided by pulse oximetry also depends on the device used and its settings, particularly signal averaging time; the magnitude of desaturations decreases when averaging time increases and this influences the sensitivity of the technique. In the field of sleep apnoea it has been shown that the number of hypopnoeas associated with desaturations of ≥4% could change significantly according to the device used and this could affect clinical decisions.7 Sampling frequency (on average 25 times/s) and signal averaging time may vary considerably between devices (reported range 2–21/s). New generation pulse oximeters usually average Spo2 signals over <10 s; high speed signal averaging also improves detection of motion artefacts, which can be quite frequent in subjects with sleep-disordered breathing.8 9 The accuracy of Spo2 measurements reported in sleep studies is 2–6% compared with arterial blood-derived determinations of haemoglobin saturation which are in the range 75–100%. When >90%, the accuracy of Spo2 readings is ±2%; at values <80%, however, the accuracy can decrease considerably with a trend towards under-reading.
Spo2 is obviously an important item to monitor in home ventilated patients. During spontaneous breathing it has been suggested that nocturnal oximetry could be specific for identifying sleep-related breathing disturbances,10 but that the morphological pattern of Spo2 desaturations could not accurately separate central from obstructive events.11 In patients using NIV at night, variations in Spo2 should be interpreted more cautiously. Indeed, pulse oximetry tracings during NIV may show a wide variety of events. The major limitation of the technique is the absence of specificity of the Spo2 variations. Recurrent desaturations may reflect, for instance, upper airway instability and residual obstructive events, decreases in ventilatory command with or without glottic closure, or repetitive leaks interrupted by microarousals. Central events such as decreases in ventilatory command with or without glottic closure may be residual events insufficiently corrected by NIV in subjects with central sleep apnoea syndromes or induced by ventilation per se (figure 1A).12 13 During spontaneous breathing, prolonged desaturations may reflect ventilation/perfusion (V/Q) mismatch in severe obstructive or restrictive disorders, position-dependent V/Q mismatch in severe obesity or persistence of alveolar hypoventilation. Prolonged desaturations (10–30 min) with concurrent acceleration of heart frequency occurring approximately every 90–120 min during the night are also typical of REM sleep hypoventilation. In ventilated patients, however, the same aspect can also result from prolonged leaks or insufficient pressure support irrespective of sleep stage (figure 1B). Furthermore, in subjects with oxygen supplementation, pulse oximetry is unreliable for the detection of hypoventilation.14 In spite of these limitations, pulse oximetry is a valuable screening tool for patients established on home ventilation who do not appear to have any problems related to NIV and who are not receiving supplemental oxygen. Among the advantages of the technique are its low cost, ease of basic interpretation, possible use in telemedicine programmes and transmission of devices with recordings by mail.15
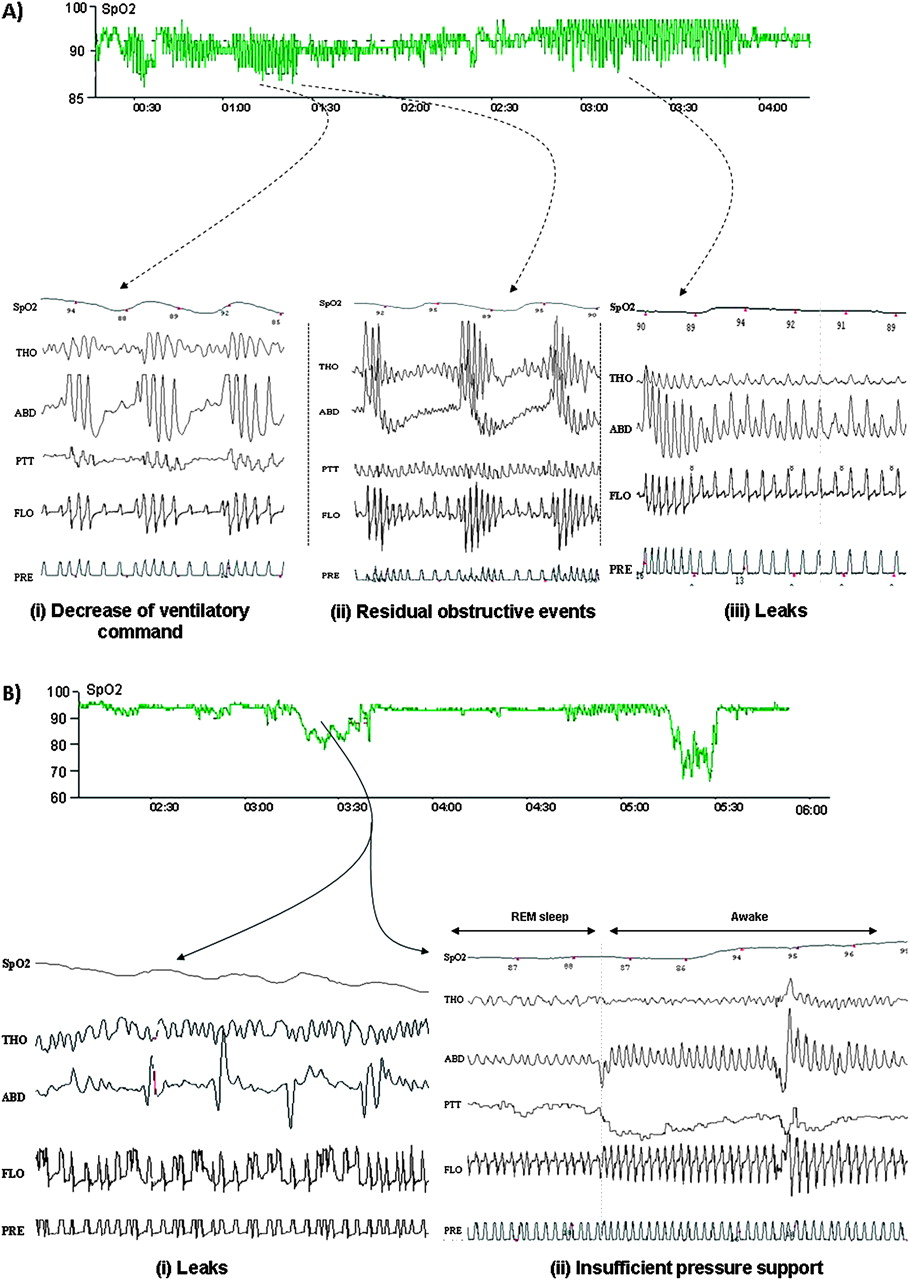
Interpretation of oxygen saturation measured by pulse oximetry (Spo2) patterns in patients using non-invasive ventilation (NIV). (A) Recurrent oscillations of Spo2 in a patient treated with NIV. This pattern is sensitive but not specific and can be associated with (i) central events resulting from respiratory instability under NIV, (ii) persistent obstructive events occurring in upper airways, (iii) intermittent non-intentional leaks. (B) Sustained Spo2 desaturations during NIV (>10 min). This non-specific pattern can result from residual hypoventilation or prolonged non intentional leaks.
Microarousals are associated with momentary increases in sympathetic activity.16 A wide range of physiological cardiovascular parameters such as heart rate, blood pressure, pulse transit time and pulse wave amplitude are related to sympathetic tone and have been implemented as indirect methods for detecting sleep fragmentation. Pulse wave amplitude (PWA) measured by photoplethysmography can easily be recorded using conventional pulse oximeters (figure 2). Peripheral vasoconstrictor responses associated with microarousals are visually identifiable by marked reductions in PWA (figure 2).17 Thus, a simple oximetric recording during NIV can provide information not only on residual oxygen desaturations but also on sleep fragmentation.
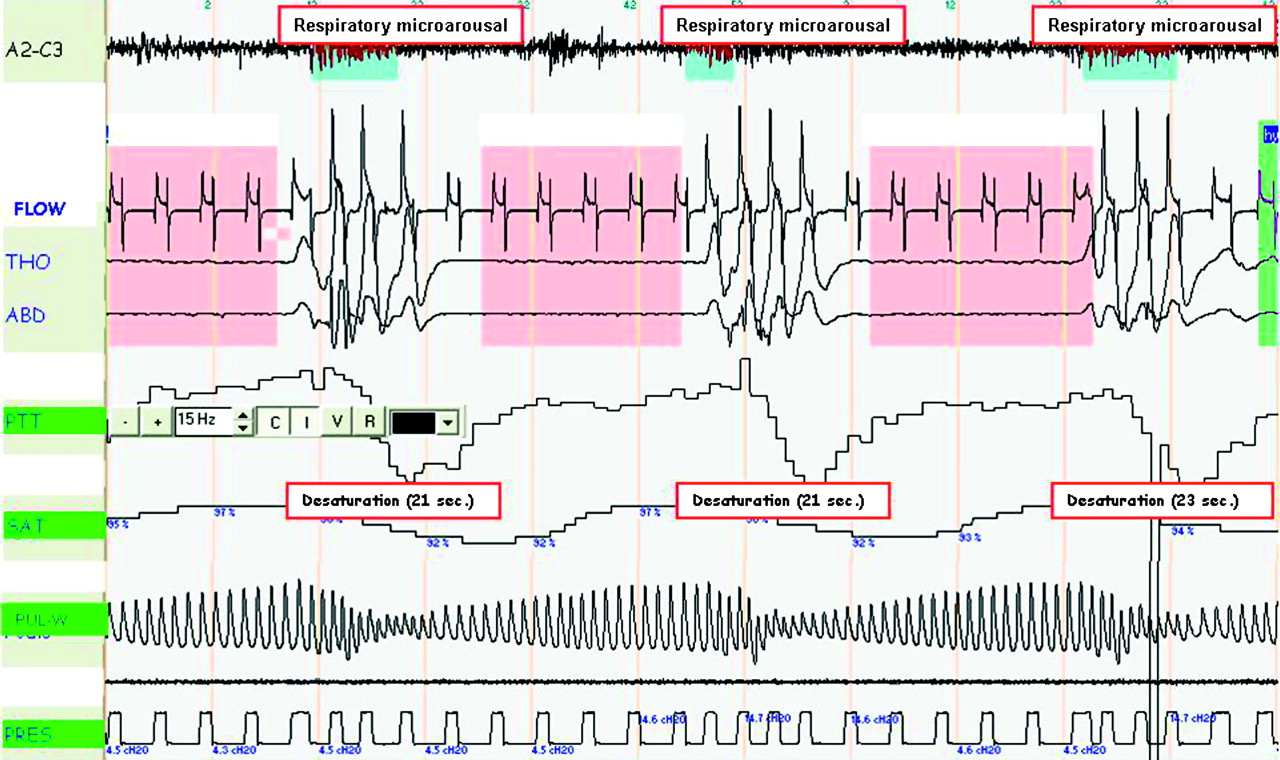
Indirect assessment of sleep fragmentation under non-invasive ventilation (NIV) using variations in pulse wave amplitude (PWA). PWA measured by photoplethysmography can easily be recorded using conventional pulse oxymeters. From top to bottom: EEG; flow; thoracic (THO) and abdominal (ABD) movements; pulse transit time (PTT); Spo2 (SAT), PWA and mask pressure (PRES). Tracing shows respiratory microarousals ending recurrent glottic closure episodes, causing transient desaturations in a patient treated by NIV with simultaneous marked reduction in PWA.
Interestingly, there are no precise guidelines as to what should be considered as satisfactory in terms of nocturnal oxygenation during home NIV; however, maintaining an adequate nocturnal Spo2 most probably decreases secondary pulmonary hypertension, improves respiratory muscle function and, in patients with diurnal hypoxaemia, survival. As stated by Langevin et al,18 Spo2 is a key feature of nasal ventilation monitoring; without at least adequate control of oxygenation, ventilator settings cannot be accepted as correct. A reasonable goal is to adjust ventilator settings to obtain a mean nocturnal Spo2 ≥90%, with <10% of the total recording time <90% after correction of leaks.19 Oxygen supplementation should be provided only in case of V/Q mismatch incompletely treated by NIV.
Although nocturnal pulse oximetry combined with daytime arterial blood gases are often used as the only evaluation of home NIV, daytime arterial blood gases may reflect nocturnal values of arterial carbon dioxide tension (Paco2) poorly,20 21 and an acceptable average Spo2 may be associated with important nocturnal respiratory events or poor control of nocturnal hypoventilation.22 Thus, visual inspection of oximetry traces is important for the detection of nocturnal respiratory events. However, the only way of determining whether decreased average Spo2 values or prolonged desaturations are related to V/Q mismatch or hypoventilation is through measurement of nocturnal carbon dioxide. To summarise, pulse oximetry (including visual inspection of traces) should be used as a screening tool in stable home-ventilated patients without supplemental oxygen to identify and exclude patients who do not require more detailed, expensive and time-consuming investigations (figure 3). Further studies, however, are needed to determine the most cost-effective procedure between systematic polygraphy or polysomnography or use of oximetry as a screening tool to avoid more expensive procedures in patients with normal arterial oxygen saturation (Sao2) tracings.

Suggested algorithm for monitoring non-invasive ventilation (NIV) during sleep. IPAP, inspiratory positive airway pressure; Paco2, arterial carbon dioxide tension; Ptcco2, transcutaneous pressure of carbon dioxide; Sao2, arterial oxygen saturation; Spo2, oxygen saturation measured by pulse oximetry; Vt, tidal volume.
Non-invasive assessment of nocturnal arterial carbon dioxide tension
Assessment of Paco2 is essential for evaluating the adequacy of alveolar ventilation when monitoring patients treated by NIV. To date, repeated sampling of arterial blood remains the ‘gold standard’ for estimating the adequacy of ventilatory support. However, repeated sampling of arterial blood does not reliably assess control of nocturnal hypoventilation because the patient will usually wake. Arterial catheterisation needs costly equipment, specially trained personnel and, in most cases, the environment of an intensive care unit. Furthermore, repeated arterial punctures or arterial catheterisation are additional sources of discomfort for the patient and are not appropriate for routine assessment in stable patients. The simplest approach is to measure Paco2 by arterial puncture at the end of the night to document night-to-morning increases in Paco2. However, blood is most often sampled after arousal and thus after a short period of appropriate ventilation. In this condition, a normal morning Paco2 does not actually reflect the abnormal time course of Paco2 during the night.20 21 Non-invasive assessment of Paco2 can be performed by measuring transcutaneous carbon dioxide tension (Ptcco2) or peak expired carbon dioxide (Petco2).
Peak expired carbon dioxide
Simple portable devices are available for measuring Petco2. However, Petco2 is a poor predictor of Paco2. The relationship between Paco2 and Petco2 depends on the physiological dead space (Vd) and the patients' ventilatory mode (tidal volume, Vt): Petco2 = Paco2 (1 − Vd/Vt). The relationship between Paco2 and Petco2 therefore depends on the type and extent of the underlying parenchymal disorder. Since Vt decreases physiologically during sleep, the [Paco2 − Petco2] gradient increases during sleep studies because of a higher Vd/Vt ratio. Also, in most patients with NIV ventilation is not homogeneous and expired CO2 does not reach an adequate plateau. Petco2 is therefore unreliable in patients with chronic respiratory failure, particularly in chronic obstructive pulmonary disease (COPD); it is technically difficult to measure with the continuous flow through the mask related to bilevel pressure support.
In summary, because of limitations related to underlying diseases and additional problems induced by non-intentional leaks associated with nasal ventilation, Petco2 measurements are not reliable and should not be used for nocturnal monitoring of these patients.
Transcutaneous measurement of carbon dioxide
Technical background
Transcutaneous measurement of CO2 theoretically appears more appropriate for monitoring Paco2. This measurement is based on the observation that CO2 has a high tissue solubility and diffuses easily through the skin. Most capnometers use the Severinghaus electrode.23 Briefly, it consists of a pH-sensitive glass electrode, a silver/silver chloride reference electrode and a heater; the electrodes are bathed in an electrolyte solution which is covered with a gas-permeable Teflon membrane. The collar of the sensor heats the skin; this induces a local hyperaemia which improves the permeability of the skin to gas diffusion and ‘arterialises’ the capillary blood to obtain Ptcco2 readings closer to Paco2 values without inducing local skin reactions or skin burns. CO2 diffuses from the skin through the membrane. It reacts with water to form H2CO3 which, in turn, dissociates into H+ and HCO3−; the H+ production modifies the pH in the electrolyte solution. Changes in pH are related to Ptcco2 according to the Henderson–Hasselbach equation. The signal produced is the voltage difference between the pH electrode and the silver/silver chloride reference electrode. Values of Ptcco2 reported by the sensor reflect correction factors used by the system software to compensate for both patient temperature and sensor temperature.
Continuous Ptcco2 recordings show good agreement with arterial measurements even if high levels of Paco2 may increase the Paco2/Ptcco2 bias.24 A reported limitation of the technique is the requirement for periodic recalibration and changes of membrane in order to ensure sufficient precision of transcutaneous measurements, although these limitations have been greatly improved in recent devices. Ptcco2 sensor drift has also been reported during overnight recordings. Compensation of this drift has been proposed by using linear interpolation, but this requires two arterial measures of Paco2 (at the beginning and at the end of Ptcco2 recording).
Use of transcutaneous carbon dioxide tension for NIV monitoring
Importantly, the good agreement between Ptcco2 and Paco2 measurements is preserved when patients are treated by continuous positive airway pressure (CPAP) or pressure support.24–26 Ptcco2 recording is also accurate in obese subjects.27 One study has shown that, during NIV, Ptcco2 recordings could be performed continuously for 8 h at a probe temperature of 43°C without any local discomfort or significant signal drift.25 More recent devices combining Ptcco2 and Spo2 earlobe sensors and validated in acute care and chronic clinical settings are designed for continuous recording over 8 h periods without requiring recalibration and are feasible for routine use (figure 4).26 28 29

{kind=link}
{kind=link}
{kind=link}
{kind=link}
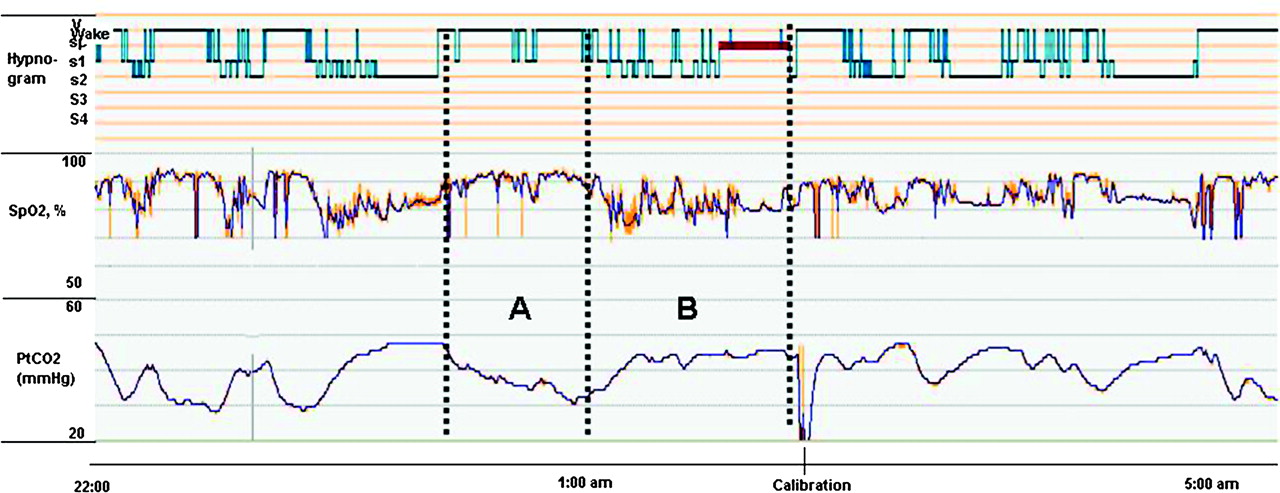
Transcutaneous measurement of carbon dioxide (Ptcco2) during night in a ventilated patient. Note normalisation of Ptcco2 (A) during periods of wakefulness versus (B) hypoventilation related to continuous major leaks during sleep. Spo2, oooxygen saturation measured by pulse oximetry.
Assessing Ptcco2 overnight is essential for evaluating correction of nocturnal hypoventilation by NIV or for identifying periods of hyperventilation leading to ventilatory instability and, potentially, to central events with or without glottic closure.12 13 30 However, all Ptcco2 sensors have a lag time (approximately 2 min) which precludes monitoring of rapid changes in Paco2 such as those which could be associated with recurrent apnoeas, hypopnoeas or brief leaks.31
In summary, nocturnal Ptcco2 should be considered as a reliable non-invasive tool to monitor nocturnal Paco2 for patients treated with NIV on a long-term basis. Limitations of the technique are the cost of the devices, the increase in bias between arterial and transcutaneous values at high Paco2 values24 and the occasional occurrence of unexplained errant values. Recent devices are, however, easy to use with user-friendly software and can be connected to polysomnography software. Finally, nocturnal Ptcco2 reveals the occurrence of episodes of hypoventilation but provides no information as to their cause (eg, inappropriate settings, leaks).
Data available from NIV machines
Most NIV device designers and manufacturers have incorporated flow and pressure sensors and the possibility of storing raw data of these parameters on a long-term basis. Specific software allows home care providers or clinicians to download these data onto a personal computer.
Downloaded data can be separated into three categories. The first is a synthesis report (ie, trend of each parameter recorded during a given period). Depending on the manufacturers and the machines (table 1), compliance, settings, estimations (not absolute values) of leaks, tidal volume, respiratory frequency, minute ventilation and respiratory cycles triggered by the patient are provided. The second category is a detailed data analysis in which raw data of a given parameter can be analysed cycle by cycle, and the third category is a polygraphic data analysis. In this situation, by adding an external module connected to the machine, physiological parameters such as oxygen saturation, heart rate and respiratory effort can be recorded and displayed in addition to the signals already stored by the device.
Summary of data available from built-in software in home ventilators.
There are large discrepancies in parameters provided by the different software. This reflects the fact that relevant parameters for monitoring NIV have not yet been clearly defined by clinicians and that recommendations in this field should be proposed by scientific societies. Second, the validity of several parameters estimated by the NIV devices (minute ventilation, Vt, apnoea-hypopnoea index) must be further validated by independent clinical and/or bench test studies. In the absence of such validation, information provided should only be considered as indicators of trends without any guarantee as to linearity of the estimations provided.
Compliance and pattern of daily use of ventilator
Medical history is often unreliable when assessing compliance with NIV and recorded data in the ventilator are therefore very helpful for assessing average daily use of the ventilator and also for documenting special patterns of ventilator use which may suggest inappropriate settings and patient discomfort (eg, fragmented nocturnal use, multiple short periods of ventilator use).
Tidal volume
Vt as reported by ventilator software is an indicator of effective ventilation although subject to variability in accuracy according to leaks. On average, the target for vt is ≈10 ml/kg, taking into account ideal body weight.32 A high variability of Vt may suggest leaks or periodic breathing, spontaneous or ventilator-induced.
Respiratory rate and percentage of spontaneous versus imposed respiratory cycles
Respiratory rate (RR) analysis allows an estimation of the difference between spontaneous RR and the preset back-up RR. Indeed, ventilators detect breaths either triggered by the patient or by the ventilator (unrewarded inspiratory efforts are not reported although some may be detected through the analysis of detailed flow curves if provided). Whether a high or low back-up RR is preferable is subject to debate. Restrick et al33 found no difference in terms of efficacy of ventilation (assessed by Spo2 and Ptcco2) between a spontaneous mode and a back-up rate of 10/min. Conversely, Parreira et al34 found that a controlled mode (back-up RR at 17 or 25/min) was more effective than the S mode. In many centres back-up RR is usually set at approximately two breaths below spontaneous RR; this can be easily adjusted using RR monitoring by ventilator. However, for patients with neuromuscular diseases, ‘capturing’ the patient's spontaneous RR is also common practice. The percentage of respiratory cycles triggered by the patient is also an estimation which should be interpreted with caution; a low percentage of triggered (spontaneous) cycles can be interpreted either as ‘the patient's RR is captured by the ventilator’ or ‘the ventilator does not detect the patient's inspiratory efforts’.
Leaks: average value and 95% percentile
The major impact of leaks on efficacy of ventilation and quality of sleep and the frequency with which major leaks occur during nasal ventilation in stable patients has been well described.35–38 Thus, measurement of leaks is potentially a very useful adjunct to information retrieved by the ventilator software, although results have yet to be independently validated for most marketed devices. Values are reported either as a total estimation of leaks (from which intentional leaks through the mask must be subtracted) or include intentional leaks by recording in the device the type of mask used. Threshold values considered acceptable by manufacturers thus vary according to whether or not intentional leaks are taken into account. Adjustment of interface and ventilator settings aims to maintain the 95th percentile of leak values under a predetermined threshold value. Rabec et al recently compared data from a commercially available system with data recorded on a bench test with a pneumotachograph and induced leaks; the results were highly significantly correlated with a low bias and limits of agreement.39
Apnoea-hypopnoea index
Although reported by ventilator software of several different devices, the effective meaning and reliability of the apnoea and apnoea-hypopnoea indices has yet to be determined. In most cases, manufacturers use the same algorithms for defining or recognising events that they developed for their auto-CPAP devices. This is inappropriate and probably largely inaccurate in patients during NIV.
Integrated multichannel modules
Certain bilevel ventilators can be coupled to multichannel modules that provide trend data on minute ventilation, respiratory rate, air leaks, Spo2 and heart rate. Such modules obtain this information from signals received through the respiratory circuit and require additional connections to a pulse oximeter with or without a detector of respiratory movements. Data can be stored on a memory card and transferred to a computer for simultaneous on-screen viewing. Rabec et al39 used a commercially available multichannel module to evaluate whether or not ventilation was efficient in clinically stable home-ventilated patients. Their criteria to define ineffective ventilation were: (1) leakage >24 l/min for >20% of the trace duration; (2) prolonged desaturations (>30% of the tracing with an Spo2 <90%), whether or not accompanied by a simultaneous reduction of minute ventilation (>10% reduction compared with baseline) in the absence of significant leaks; and (3) cumulative desaturation dips (>3%) for >10% of the trace duration. In patients receiving long-term NIV, 53% of traces were abnormal; the most frequent finding was leaks. Interestingly, neither pH nor Paco2 were predictive of abnormal recordings in these patients.
Conclusions
Simple tools are available for monitoring the efficacy of long-term NIV. Pulse oximetry is the simplest approach. It is a rough indicator of major problems related to NIV but loses sensitivity in subjects with oxygen supplementation. Abnormalities on pulse oximetry tracings are non-specific and do not allow a distinction to be made between, for instance, V/Q mismatch versus alveolar hypoventilation. However, pulse oximetry is a very useful screening tool in stable patients receiving home ventilation. By using pulse wave amplitude analysis, oximetric recordings can also provide indirect assessment of sleep fragmentation when using NIV. Transcutaneous capnography has become a routine approach in many centres: it is the only non-invasive method allowing assessment of correction of nocturnal hypoventilation. Drawbacks are the price of the equipment, occasional unexplained errant values and a lag time of several minutes which renders analysis of very short respiratory events impossible. Built-in software of home ventilators supplies very valuable data (leaks, ventilatory mode, percentage of spontaneous inspirations and expirations, residual apnoea and hypopnoea indices), although signals are estimations and must be independently validated; furthermore, the relevance of some signals has not yet been determined. Combined approaches such as integrated modules allowing recording of multiple parameters offer a very useful approach for detecting frequent problems such as leaks and their impact on Spo2.
References
Linked Articles
- Review series
- Review