





Abstract
Fundoplication may improve survival after lung transplantation. Little is known about the effects of fundoplication on quality of life in these patients. The aim of this study was to assess the safety of fundoplication in lung transplant recipients and its effects on quality of life.
Between June 1, 2008 and December 31, 2010, a prospective study of lung transplant recipients undergoing fundoplication was undertaken. Quality of life was assessed before and after surgery. Body mass index (BMI) and pulmonary function were followed up.
16 patients, mean±sd age 38±11.9 yrs, underwent laparoscopic Nissen fundoplication. There was no peri-operative mortality or major complications. Mean±sd hospital stay was 2.6±0.9 days. 15 out of 16 patients were satisfied with the results of surgery post fundoplication. There was a significant improvement in reflux symptom index and DeMeester questionnaires and gastrointestinal quality of life index scores at 6 months. Mean BMI decreased significantly after fundoplication (p=0.01). Patients operated on for deteriorating lung function had a statistically significant decrease in the rate of lung function decline after fundoplication (p=0.008).
Laparoscopic fundoplication is safe in selected lung transplant recipients. Patient benefit is suggested by improved symptoms and satisfaction. This procedure is acceptable, improves quality of life and may reduce deterioration of lung function.
Chronic microaspiration, secondary to extra-oesophageal reflux, may contribute to bronchiolitis obliterans syndrome (BOS) after lung transplantation. Up to 75% of lung transplant patients have demonstrable gastro-oesophageal reflux disease (GORD) [1–5]. Elevated biomarkers, pepsin and bile salts, have been documented in the bronchoalveolar lavage fluid after lung transplantation, suggesting microaspiration [6–8]. Early anti-reflux surgery may lead to protection of lung function and increased survival through preventing microaspiration. Most of the impetus has been from Duke University (Durham, NC, USA), where the majority of evidence originates [5]. There is a lack of basic information in this patient group, including safety and assessments of quality of life. Such information is important because physiological post-operative complications are common afetr fundoplication, and may lead to a reduction in quality of life, despite resolution of reflux symptoms. Specific complications include temporary dysphagia, nausea [9, 10], discomfort from gas bloating and increased flatulence [2]. Only one study has looked at the effects of fundoplication on quality of life in this population, despite a high prevalence of foregut dysfunction [11]. This puts these patients at risk of physiological dysfunction and reduced quality of life after surgery. To date, no transplant studies have been performed assessing the response of extra-oesophageal reflux symptoms to fundoplication.
The aim of this study was to assess the safety of fundoplication in lung transplant recipients and its effects on quality of life.
METHODS
A prospective study of all lung transplant recipients undergoing anti-reflux surgery between June 1, 2008 and December 31, 2010 at the Northern Oesophago-Gastric Unit (Royal Victoria Infirmary, Newcastle-upon-Tyne, UK) was carried out. All lung transplant recipients in this unit are routinely prescribed prophylactic proton pump inhibitor (PPI) therapy to prevent steroid-induced ulceration. There was no distinction in patient management made between underlying pathologies (e.g. cystic fibrosis). Surgery was considered for patients with symptomatic reflux alone, refractory to PPI therapy, or for reflux associated with deteriorating lung function. Patients with asymptomatic reflux were only considered for surgery if there were concerns about microaspiration. Maximal medical therapy was not considered for failed PPI therapy or suspected microaspiration, as it was felt that a mechanical barrier to reflux would better protect the allografts from microaspiration. Ethical approval for patient follow-up was obtained from a local ethics committee (County Durham and Tees Valley 2 Research Ethics Committee). Written consent was obtained for patients to be observed overall post lung transplant, but not specifically for this study.
Reflux status was assessed on PPI therapy by oesophageal manometry, pH impedance (Ohmega; MMS™, Utrecht, the Netherlands) and endoscopy. Patients underwent a thorough pre-operative assessment to ensure fitness for surgery. Reflux status was defined by the presence of oesophageal or extra-oesophageal symptoms combined with objective evidence of GORD on pH impedance and/or endoscopy. Patients did not undergo a post-fundoplication pH impedance or endoscopic measurement of reflux status. Pulmonary function tests and bronchoscopy were routinely performed in the pre-operative work-up.
Patients were followed up clinically with emphasis on lung function, satisfaction with treatment and quality of life. The following questionnaires were used: the DeMeester Reflux Questionnaire, a validated standard reflux questionnaire; the Reflux Symptom Index (RSI) questionnaire, a validated laryngopharyngeal reflux questionnaire; and the Gastro-intestinal Quality of Life Index (GIQLI), a validated gastrointestinal-specific quality of life questionnaire [12–14]. These questionnaires covered oesophageal reflux symptoms (heartburn and dysphagia), extra-oesophageal reflux symptoms (cough and wheeze) and functional gastrointestinal symptoms that could be affected by fundoplication (bloating and flatus). These were assessed pre- and post-operatively. Pre- and post-fundoplication body mass index (BMI) were recorded. Patient satisfaction was assessed by direct questioning of patients.
Lung function was assessed in accordance with European Respiratory Society guidelines [15]. BOS scores were calculated using forced expiratory volume in 1 s (FEV1) in accordance with International Society for Heart and Lung Transplantation guidelines [16, 17]. The rate of decline in FEV1 was calculated in accordance with previous studies, namely, the measures of FEV1 before fundoplication were plotted and the gradient between points from the baseline FEV1 level to the time fundoplication was calculated in millilitres per month. The same was done for the FEV1 measurements after fundoplication, the last FEV1 being either the current one in patients still alive or the final FEV1 in the patients who died [18].
In our unit, bronchoscopy is routinely performed at 1 week, and at 1, 3 and 6 months, and 1 yr post-transplant. Further bronchoscopies are carried out when clinically indicated by an unexplained drop in FEV1. Pulmonary function tests are carried out routinely at every outpatient visit, on average every 3 months.
The RSI, DeMeester reflux and GIQLI questionnaires were completed pre-operatively, and 6 weeks and 6 months post-operatively. The GIQLI score was subdivided into symptomatic questions (n=17) and functional questions (n=19) to assess whether changes in quality of life were due to changes in symptoms or social functioning. Patients were asked about overall satisfaction with the result of surgery at 6 weeks and 6 months post-operatively. Questionnaires were completed by patients, with expert advice on hand to explain any concerns about questions and to offer one-to-one advice.
Surgical technique
Laparoscopic Nissen fundoplication was performed. Access to the abdominal cavity was via four ports and an epigastric stab incision for the Nathanson retractor to retract the liver. Initially, the oesophageal hiatus was dissected to mobilise the oesophagus. The posterior vagus was preserved and a window was created behind the oesophago-gastric junction. The posterior crura were repaired to tighten the hiatus, and a loose 360° wrap was tailored with three Ethibond™ sutures (Ethicon, Somerville, NJ, USA). One further suture was used to anchor the wrap to the oesophagus and right crus. Percutaneous endoscopic gastrostomy (PEG) fistulae were repaired when present. These were divided with an Endostapler™ device (Ethicon). The PEG wound was excised and the deficit in the abdominal wall and skin were closed. Local anaesthesia was inserted into the peritoneal cavity and infiltrated in the wounds at the end of the procedure.
Statistical analysis was carried out with the help of a statistician. Initially, a Kolmogorov–Smirnov test was performed to assess normality. Subsequently, paired t-tests and two-way ANOVAs were performed with a post-test Bonferroni correction. Figures were created using GraphPad Prism™ software (GraphPad, San Diego, CA, USA).
RESULTS
During the study period, 109 lung transplants were performed. 17 patients were considered for fundoplication. One patient was managed conservatively due to lack of objective evidence of GORD on pH impedance and endoscopy. Of 17 patients offered fundoplication, 16 (10 females and six males) with a mean±sd age of 38.2±11.9 yrs, consented to and underwent fundoplication. Indications for lung transplant were: cystic fibrosis in 10; chronic obstructive pulmonary disease (COPD)/asthma in one; COPD in one; pulmonary fibrosis in three; and pulmonary fibrosis/asthma in one patient. 13 patients underwent single sequential lung transplant, two had a right single lung transplant and one had a left single lung transplant. Indications for fundoplication were objective evidence of GORD on pH impedance and/or endoscopy with either typical reflux symptoms (heartburn) (n=8) or typical (heartburn) and atypical extra-oesophageal symptoms (cough and wheeze) with deteriorating lung function (n=8). Symptoms occurred despite PPI therapy. Mean pre-operative BMI±sd was 23.8±4.4 kg·m−2. Patient demographics are summarised in table 1.
All patients had a diagnostic gastroscopy. 15 out of 16 patients had a hiatus hernia (2–6 cm). eight out of 16 has oesophagitis: grade A, n=4; grade B, n=3; and grade C, n=1. One patient had a small tongue of Barrett's oesophagus confirmed on histological assessment. Three patients had oesophageal candidiasis, which was treated pre-operatively. A summary of pre-operative oesophageal physiology is shown in table 2.
Operation
Pre-operative American Society of Anaesthesiology score was 2 (n=5) or 3 (n=11). Mean±sd FEV1 was 80±5% predicted or FEV1 was 2.4±0.97 L. Fundoplication was performed at a mean of 1,053±881 days post-transplant.
Mean intra-operative time was 93±20 min. All patients had blood loss of <100 mL. Four patients had a PEG fistula excised and no patients required an intensive treatment unit stay, although five out of 16 patients were admitted electively to our high-dependency unit for observation for 24 h. Mean hospital stay was 2.6±0.9 days; longer stays were due to post-operative pain (in two patients with PEG fistulae repair), peri-operative dysphagia (one patient), a return to theatre or difficulty arranging transport home.
Morbidity and mortality
There were no deaths or serious post-operative complications. Two patients developed post-operative dysphagia. One of these patients returned to theatre the following day and underwent a laparoscopy and minor revision of fundoplication, and subsequently made an uneventful recovery. In the other patient, barium swallow revealed no significant blockage and symptoms subsequently resolved spontaneously.
Overall satisfaction with fundoplication
Overall, 15 out of 16 patients reported being satisfied at 6 weeks and 15 out of 16 patients reported satisfaction at 6 months. At 6 weeks one patient was unsatisfied due to dysphagia. At 6 months, one patient was unsatisfied due to pain at the site of their PEG fistula and abdominal bloating.
Quality of life
There was a statistically significant improvement in symptoms and quality of life scores over the first 6 months post-fundoplication. Kolmogorov–Smirnov analysis revealed the questionnaire data to be normally distributed. Questionnaires were completed by 15 out of 16 patients. One patient, despite reporting high levels of satisfaction with their result, did not wish to spend time completing these questionnaires. Patient symptom and quality of life questionnaire scores are summarised in table 3.
RSI questionnaire
Pre-fundoplication RSI was positive in eight out of 15 patients, and this decreased to three out of 15 being positive for RSI by 6 weeks and two out of 15 being positive at 6 months. The two-way ANOVA revealed a statistically significant improvement in RSI score over the three time-points (p<0.001). Post-test Bonferroni correction revealed a statistically significant improvement in the mean±sd RSI score from 14±7.1 pre-operatively to 6.7±7.9 at 6 weeks post-fundoplication (p=0.021) and 5.9±6.5 at 6 months (p=0.003) (fig. 1a). The Bonferroni correction did not show a statistically significant difference between RSI scores at 6 weeks and 6 months.

a) Reflux Symptom Index (RSI) score, b) DeMeester Reflux Questionnaire Score and c) Gastro-intestinal Quality of Life Index (GIQLI) score over the first 6 months post-fundoplication. The dotted line indicates a score of 13, the cut-off for a normal/abnormal score. Horizontal lines represent the mean and error bars represent the standard deviation. Pre-op: pre-operative. ***: p<0.001 compared to pre-op; #: p=0.008 compared to pre-op.
DeMeester reflux questionnaire score
The two-way ANOVA revealed a statistically significant improvement in DeMeester Reflux Questionnaire score over the three time-points (p<0.001). Post-test Bonferroni correction revealed a statistically significant improvement in the mean±sd DeMeester questionnaire score from 3.7±1.7 pre-operatively to 1.5±1.6 at 6 weeks post-fundoplication (p=0.012) and 1.2±0.8 at 6 months (p=0.003) (fig. 1b). The Bonferroni correction did not show a statistically significant difference between DeMeester questionnaire scores at 6 weeks and 6 months.
GIQLI
The two-way ANOVA revealed a statistically significant improvement in RSI score over the three time-points (p=0.008). Post-test Bonferroni correction revealed a statistically significant improvement in the mean±sd GIQLI score from 96.5±34.4 pre-operatively to 112.4±22.4 at 6 months (p=0.036) (fig. 1c). The Bonferroni correction did not show a statistically significant difference between GiQLI scores pre-operatively and at 6 weeks (mean±sd score 105.1±27.6), or at 6 weeks or 6 months (p=0.1).
GIQLI sub-analysis
Symptoms
The two-way ANOVA revealed a statistically significant improvement in symptom score from our GIQLI sub-analysis score over the three time-points (p<0.001). Post-test Bonferroni correction revealed a statistically significant improvement in mean±sd symptom score from our GIQLI sub-analysis from 49.7±10.5 pre-operatively to 56.9±9.1 at 6 weeks post-fundoplication (p=0.03) and 58.7±7.6 at 6 months (p=0.006). The Bonferroni correction did not show a statistically significant difference between symptom score from our GIQLI sub-analysis at 6 weeks and 6 months.
Functional
The two-way ANOVA revealed a statistically significant improvement in functional score from our GIQLI sub-analysis over the three time-points (p=0.036). Post-test Bonferroni correction did not reveal which pairs reached statistical significance in their improvement in mean±sd functional score from our GIQLI sub-analysis score from 51.9±19.2 pre-operatively to 54±19.2 at 6 weeks post-fundoplication and 59.1±13.1 at 6 months (p=0.09), although there was a mean improvement of 7.2 points from the pre-operative score to the score at 6 months. There was a trend to significance from the pre-operative to the 6-month score (p=0.09) and from the 6-week to the 6-month score (p=0.11).
Body mass index
Kolmogorov–Smirnov analysis revealed this data to be normally distributed. Mean±sd BMI significantly decreased from 23.8±4.4 kg·m−2 pre-fundoplication to 22.6±4.6 kg·m−2 at 6 months post-fundoplication (p=0.01) (fig. 2).

Body mass index (BMI) score pre-operatively (pre-op) and at 6 months post-fundoplication (post-op). Horizontal lines represent the mean and error bars represent the standard deviation. #: p=0.001 compared with pre-op.
Lung function
Pre-fundoplication, nine patients had no evidence of BOS, whilst the remaining seven patients had BOS 0p (a new grade of BOS created in 2002 to denote “early BOS”) (n=1), BOS score 1 (n=2), BOS 2 (n=1) and BOS 3 (n=3). Two patients had a worsening BOS score from BOS 0 to 1 and BOS 2 to 3. Despite a slowing rate of decline, the patient who deteriorated from BOS 2 to 3 died 482 days post-fundoplication from respiratory failure. The patient with BOS 0p had a reversal of this to BOS 0. All other patients remained stable.
Patients were followed up for a mean of 476±180 days post-fundoplication. FEV1 was similar pre-fundoplication (2.4±0.97 L) and post-fundoplication (2.4±0.71 L) (p=0.08).
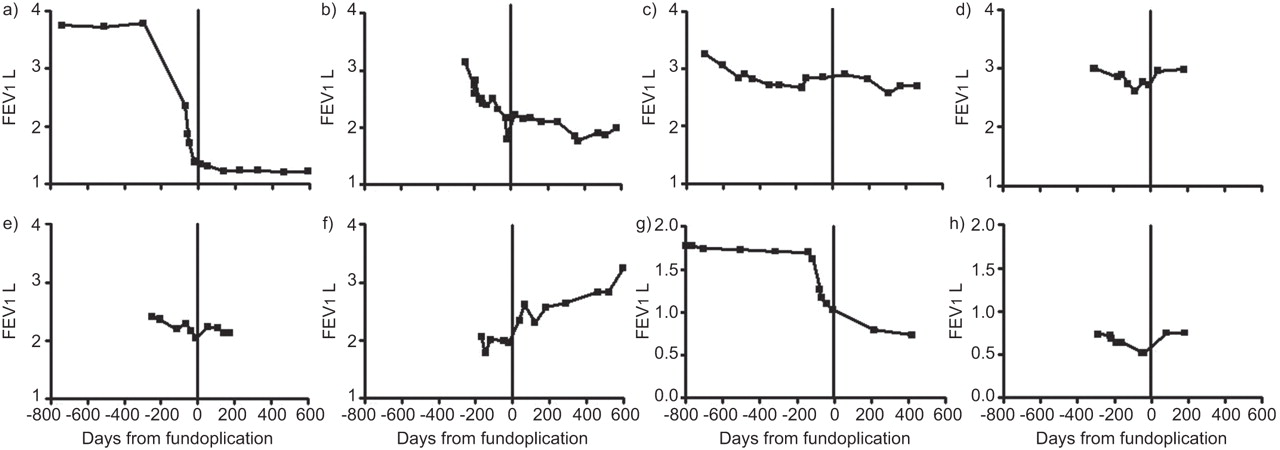
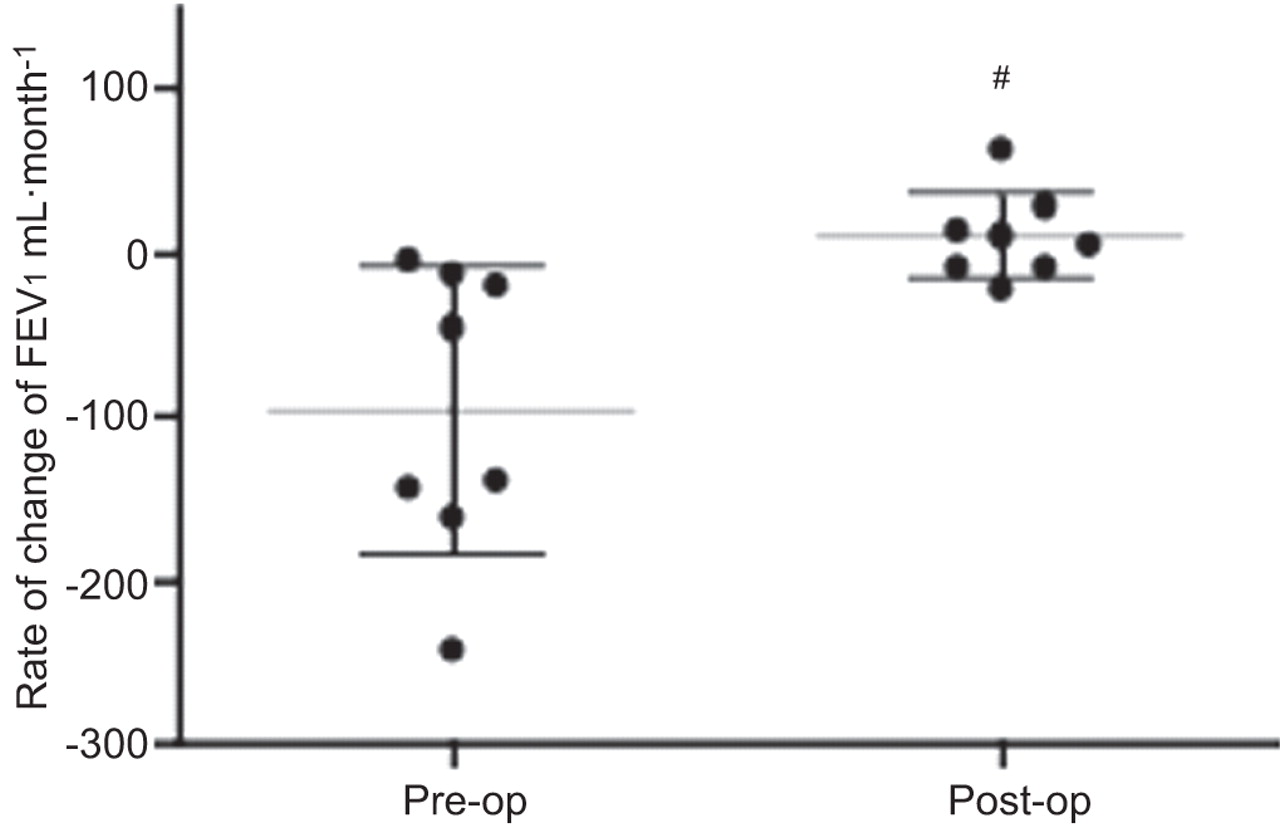
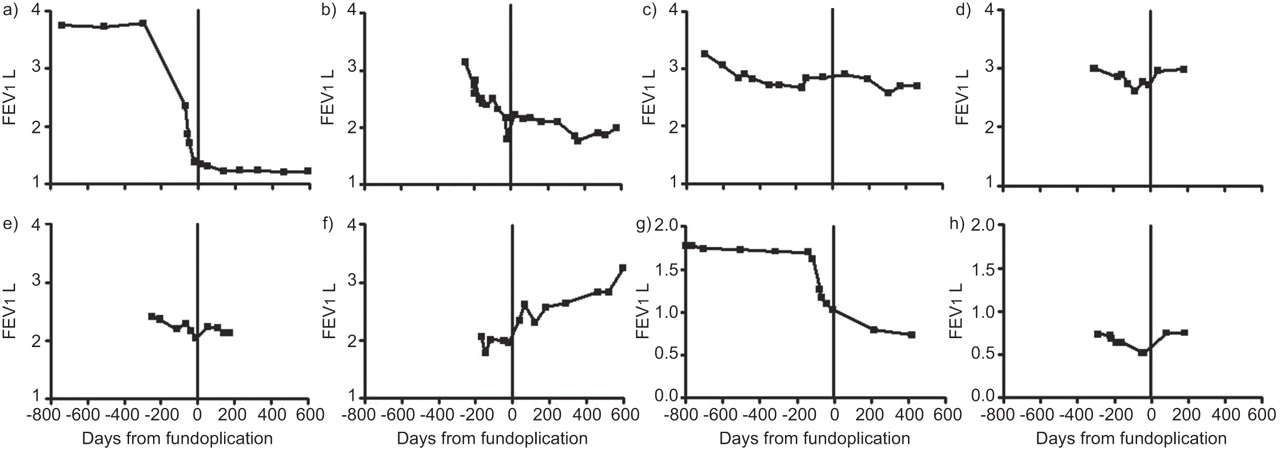
Eight patients were operated on for deteriorating lung function. Of these eight, one patient had a reversal of BOS, two had a stabilisation of lung function and five had a decrease in the rate of deterioration. Kolmogorov–Smirnov analysis revealed this data to be normally distributed. In the eight patients operated on for deteriorating lung function, there was a statistically significant decrease in the rate of decline of FEV1 per month post-fundoplication from a mean change±sd of -96.7±87.3 mL·month−1 pre-fundoplication to +9.5±26.5 mL·month−1 post-fundoplication (p=0.008) (fig. 3). Individual traces are shown in figure 4.
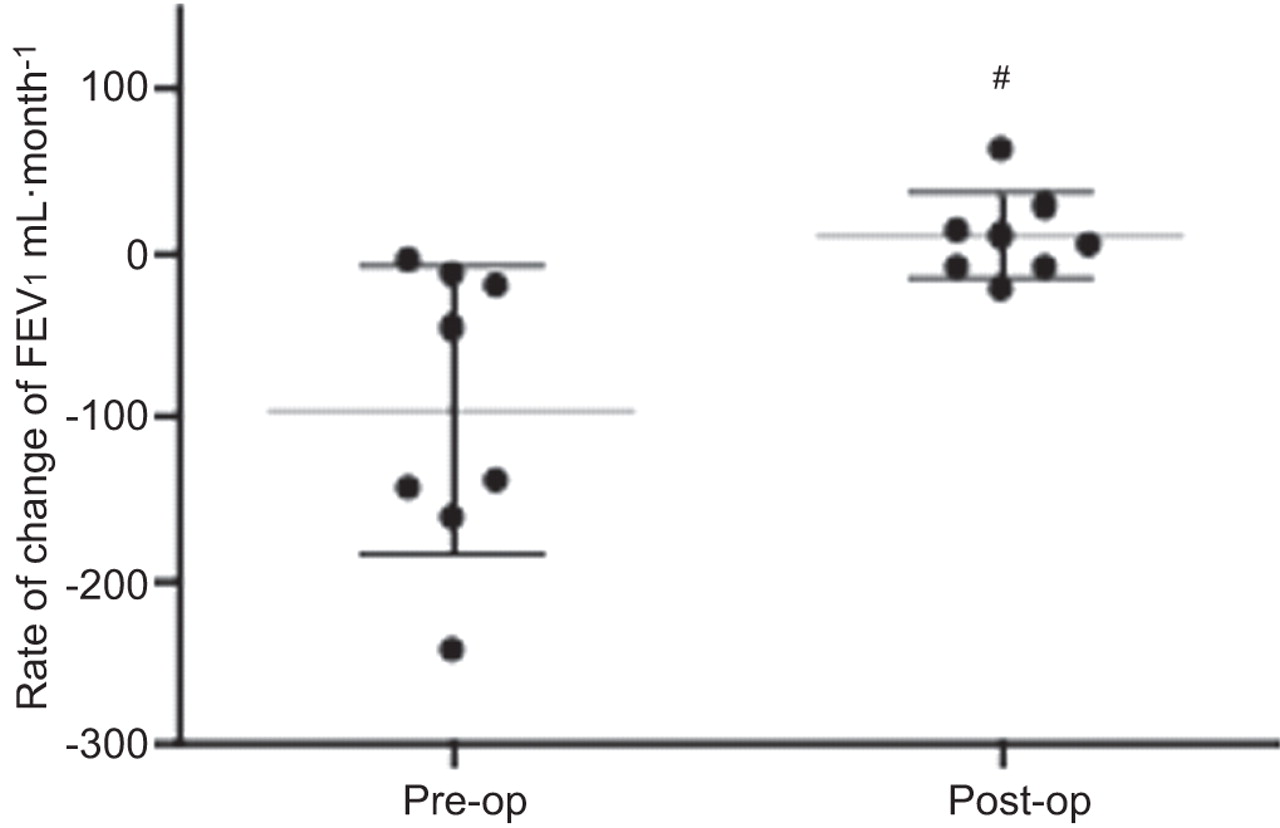
Rate of change of forced expiratory volume in 1 s (FEV1) pre- and post-fundoplication (pre- and post-op) in patients with deteriorating lung function. Horizontal lines represent the mean and error bars the standard deviation. #: p=0.008 compared with pre-op.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Changes in of forced expiratory volume in 1 s (FEV1) over time pre- and post-fundoplication in patients with deteriorating lung function.
DISCUSSION
This study demonstrates that laparoscopic fundoplication in a transplant setting is safe. Patients reported a high level of satisfaction with the results of surgery at 6 weeks and 6 months. This study also demonstrated that, in this specialised patient population, laparoscopic anti-reflux surgery is effective in reducing symptoms of GORD and improves quality of life. Our study also supports the possibility that fundoplication may impact positively on the loss of lung function seen in BOS.
These findings are important as there is little knowledge regarding laparoscopic fundoplication in these patients, and such surgery could potentially have negative effects. Our data demonstrating improvements in symptoms and quality of life are, therefore, reassuring. More speculatively, the reduction of decline in lung function observed in this open study supports the theory that fundoplication may protect the lung allograft from microaspiration injury, and suggests the need for further trials.
There is no consensus regarding fundoplication in lung transplant recipients [19]. Small series of fundoplication have been reported in patients with end-stage lung disease [20, 21]. Not all these patients will undergo transplant and there are significant risks associated with performing this procedure in patients with very poor lung function. We have adopted a pragmatic approach, operating in the post-transplant period on patients with symptomatic reflux and those with evidence of reflux and deteriorating lung function. Based on the available transplant evidence, laparoscopic Nissen fundoplication was favoured in our practice [22].
In the study of safety from Duke University, compared with the nontransplant population, there were no significant differences in operative time and blood loss [23]. Our study has comparable intra-operative data and no patients in our series have needed conversion to an open operation. No intra-operative or peri-operative deaths have been reported by the Duke University group [5, 23, 24], although, recently, one post-fundoplication death has been reported [25]. We have experienced no mortality to date and no major complications were encountered. The Duke group have reported increased length of stay in the transplant population and a higher readmission rate, due to transplant comorbidity [23]. Our results are comparable with this experience. The long post-operative stay may be partially explained by the fact that transplant patients have to travel greater distances than a local population. Overall, our results suggest that laparoscopic fundoplication is safe in selected lung transplant recipients.
Over the last 20 yrs, quality of life assessments have been established as end-point outcomes. The GIQLI questionnaire has been recommended by the European Association for Endoscopic Surgery for the assessment of quality of life after fundoplication [26]. The DeMeester reflux questionnaire is validated to assess reflux symptoms and the RSI has been validated in nontransplant patients as a marker of extra-oesophageal reflux [13], and has been used to assess the effects of fundoplication on extra-oesophageal reflux [27, 28].
In nontransplant patients, fundoplication has been shown to ameliorate reflux symptoms and improve quality of life [29]. This study showed that, in lung transplant recipients, there was an improvement in typical reflux symptoms. Although this may be expected, it has also shown an improvement in quality of life post-fundoplication, despite the high prevalence of foregut dysfunction in this population [11]. Our sub-analysis of the data showed that improvement in quality of life occurs via both amelioration of symptoms and improved social functioning.
Questionnaires designed for the assessment of extra-oesophageal reflux have not previously been used in lung transplant recipients. Our finding of improvement in extra-oesophageal reflux symptoms in lung transplant recipients after fundoplication is, therefore, novel. These symptoms include cough and hoarseness, which can be caused by extra-oesophageal reflux, but may also represent primary respiratory symptoms. This finding further supports the theory that these patients experience laryngopharyngeal reflux [13, 27], which may precede micro-aspiration. It is unknown how the evolving changes in the lung transplant and BOS may affect extra-oesophageal reflux symptoms, but we believe improvements are possibly attributable to fundoplication.
The Melbourne group's study of fundoplication in lung transplantation described a decrease in mean BMI from 23 kg·m−2 6 months pre-operatively to 21 kg·m−2 6 months post-operatively. The current study's results are similar, with a decrease in mean BMI from 23.8 kg·m−2 to 22.6 kg·m−2 6 months post-operatively. The significance of this is unknown, but, in selected patients, post-fundoplication dietary advice and intervention may have an important role.
The Duke University Transplant Group has published several papers [5, 23, 24, 30, 31], each an update of a continuing programme, with results suggesting that anti-reflux surgery may lead to increased survival and improved lung function post-transplantation [5]. Our study was not designed to assess the impact of fundoplication on lung function. In our series, mean FEV1 did not deteriorate post-fundoplication. Those patients operated on for deteriorating lung function underwent a statistically significant reduction in the loss of lung function, and one patient had a reversal of a subtle defect in lung function.
Our current study has several limitations. The numbers involved were small and patients had a variety of indications for surgery. Fundoplication was performed at different times after transplant and no patients were operated on within 90 days of transplant, the suggested optimum time for intervention [5], although this study did not seek to define an optimum time for intervention. No control group was analysed and the study was not randomised. Further studies could include a focus on the effects of early fundoplication (within 90 days) on allograft function and long-term survival.
Almost all the evidence supporting fundoplication post-lung transplant originates from a single centre and only three other centres have published case series. Based on this evidence, we have tried to develop a series of pragmatic indications for those to be offered surgical interventions. The improvement in GORD symptoms and quality of life in these patients suggests that the developing indications for fundoplication post-lung transplant may include symptomatic GORD in fit patients. The reduction in deterioration of lung function post-fundoplication further supports a possible role of this therapy in the prevention of BOS, but further evidence is required, including formal trials. Our study suggests that, with careful design, such studies are possible and can be safe in an extended series of patients.
Acknowledgments
We would like to thank C. Hannah (Freelance Art Director, Glasgow, UK) for our illustrations.
Footnotes
Support Statement
A.G.N. Robertson received funding from the European Society for Organ Transplantation and the British Lung Foundation; P.A. Corris and C. Ward received funding from the Medical Research Council.
Statement of Interest
None declared.
- Received April 8, 2011.
- Accepted June 28, 2011.
- ©ERS 2012
REFERENCES










