
Abstract
Background
Obesity is one of the most important underlying risk factors for chronic disease. Dramatically increasing and following complication of obesity should be alerted to health politicians and practitioners to prevent associated health risks. This review aimed to give a better insight into the prevalence of obesity and overweight in different areas of Iran.
Method
All published internal (SID, Irandoc, Iranmedex), and international (Web of Knowledge, Pubmed, Scopus) source studies, reported the prevalence of overweight/obesity among normal population samples, during Jan 2005 through Jan 2014, were assessed in this review. Paper selection processes were done by two researchers separately. Studies which met the eligible criteria were included in this review.
Result
One hundred ninety three eligible studies enter into our review. Of 193 final selected studies, 86 (15 national, 71 sub national) of them were reported the prevalence of obesity/overweight in adult, and 107 studies (11 national, 96 sub national) in under-18 by individual. The range of overweight and obesity prevalence in national studies in adult, was 27.0-38.5 (95% CI: 26.8-27.1, 37.2-39.8), and 12.6-25.9 (95% CI: 12.2-13.0, 24.9-26.8), separately. In under-18 the range of overweight and obesity prevalence in national studies were 5.0-13.5 (95% CI: 4.5-5.5, 13.4-13.6), and 3.2-11.9 (95% CI: 3.0-3.4, 11.3-12.4).
Conclusion
Obesity as an important public health problem has been discussed in recent few decades worldwide. Although the national reported prevalence of obesity in Iran was not considerably diverse, but remarkable differences were seen in the sub national prevalence which must be noticed more in political health programs especially among women and children.
Similar content being viewed by others


Introduction
Obesity as an epidemic of 21st century is a major public health problem worldwide which its prevalence is dramatically increasing in both developed and developing countries [1],[2]. Obesity or overweight are physiologically defined as fat accumulation in an abnormal or excessive pattern in adipose tissue may cause some serious health concerns [3].
The Body Mass Index (BMI) is the most prevalent and practical indicator for evaluation of overweight and obesity in adults around the world [4], based on it, individuals with BMI 25–30 kg/m2 and >30 are defined as overweight and obese, respectively [5]. Although there is no general agreement on a cutoff point of overweight or obesity in children and adolescents, International Obesity Task Force (IOTF) and The US Centers for Disease Control and Prevention (CDC), are more acceptable [6].
Obesity is a serious health problem with side effects can vary from a complaint of disability to premature death. So decreasing in quality of life (QOL) is unavoidable [7],[8]. Some studies have proclaimed that maybe increasing rate of obesity prevalence is associated with the notable changes in the life style especially dietary habits (consumption of unhealthy outdoor foods) and inadequate daily activity in both rural and urban regions [3],[9]. Genetic factors; different pattern of eating; and low socioeconomic status are some of the ethnic dimensions that can be underlying basis for obesity as well [10]-[13].
Overweight is the sixth most important risk factor causative to the total worldwide disease [14]. Some studies found that obesity increases the risk of some chronic and life threatening disorders such as type 2 diabetes, Cardiovascular disease, hypertension, hyperlipidemia, sleep apnea, and followed by, it has been estimated to reduce life expectancy around 7 years [15]-[17]. So researchers are always looking for appropriate treatment methods for obesity [17],[18].
Along with, we will be faced a big health problem by growing demands in based on obesity co-morbidity disorders that definitely required to spend huge funds and limitation resources in the near future [10],[19].
Based on global evaluations by WHO in 2005, the number of overweight and obese individuals throughout the world reach to 1.6 and 400 million person respectively [5],[20], and expected to get to 2-3 billion overweight and more than 700 million obese in 2015. Studies revealed that the prevalence of overweight and obesity in most Asian countries as well [4],[10].
We conducted this literature review to evaluate the prevalence of obesity and overweight in Iran with particular attention to differences living classes (urban, rural), type of study (national, sub-national), gender (male, female) in two age categories (adult, under-18-years-old).
Methods
In this systematic review we endeavored to assess all the related studies that report prevalence of obesity and overweight in all regions of Iran. The detail of this study strategy will be mentioned in following.
Search strategy
Electronic search strategies were designed by an experienced medical information specialist in consultation with the review team. Search strategy was assessed and accepted in a peer review board of Endocrinology and Metabolism Research Institute of Tehran University of Medical Sciences. We searched in English databases; Scopus, ISI web of Sciences and PubMed and also in Persian databases; IranMedex, Scientific Information System (SID), and Irandoc to obtain all related studies, during time ranged Jan 2005 up to Jan 2014. All databases were assessed in title, keyword, and abstract.
The medical subject headings (MESH) were; “obesity”, “overweight”, “Iran”, and “prevalence” for searching in English databases and also the equivalent Persian- language of these terms were used for searching in Persian databases. Besides, hand-searching was conducted to find articles which not found in electronic search.
Forasmuch as the differences in cut of points between adult and children/adolescents, the standard cutoff points in each study were recorded. The reports for children/adolescents prevalence were based on standards CDC (The Centers for Disease Control and Prevention), WHO (World Health Organization), and IOTF (The International Obesity Task Force). CDC is based on growth curves that released new international growth standards for children aged 5 years or younger that include BMI-for-age growth charts defines obesity and overweight as higher than the 95th, and 85-95th percentile of body mass index, respectively. The National Center for Health Statistics/World Health Organization NCHS/WHO cut-Off percentile classification for age including: underweight < 5th BMI-for-age; normal weight 5th < BMI-for-age < 85th; overweight 85th BMI-for-age < 95th; and obese BMI-for-age > 95th. The same percentiles cut-offs were considered for the CDC as well. IOTF used data from six national studies carried out in different countries to provided percentile curves that passed through the widely used cut-off points of 25 kg/m2 and 30 kg/m2 for adult overweight and obesity [21].
Study selection
We included all related population-based studies including national, province, and local surveys which were carried out on individuals with no restraint in age or gender. Extracted information of children and adults was recorded in two separate sheets of Excel software (Microsoft office package 2010) including; name of the first author, year of publication, study region, level of study (national, province, local), number of sample size (total, and sex or regional subgroups number), standard cut-off point for obesity and overweight, reported prevalence and its 95% confidence interval.
Exclusion criteria
We excluded studies with fewer than 200 individuals, non-population-based, and non-randomized. Duplicated citation and review articles were excluded from the study. English duplicated studies were emitted by Endnote software, and Persian studies by hand.
Data extraction
Evaluation of inclusion and exclusion criteria was conducted by assessing title and abstracts of studies in the first and second steps respectively. Then full texts were reviewed in cases which were not sufficient by reading their abstracts. As regards BMI as a conventional variable was be noted in many studies, we are proposed to study full text to extract prevalence of obesity or overweight even in cases with no main aim of determination of obesity or overweight prevalence. All procedures were performed by two researchers independently. In cases there were no agreement, the debate was conducted to achieve consensus. Otherwise the third expert reviewer was asked to decide in that case. Finally information was inserted in two separate tables for adult and under-18-individuals.
Results
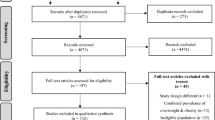
In primary search we found 2173 full text articles based on the related keywords to our topic. Of those, 982 were obtained from English data bases and the rest attained in Persian databases. After excluding overlapped studies, and considering inclusion and exclusion criteria in two separate steps (title and abstract review), finally 194 (86 for under-18 and 108 for adult) qualified studies were selected to enter to our review. The number of primary research results and the detailed process to select appropriate studies are shown in the Figure 1.

Flow diagram of the study selection process.
The extracted data from these studies are shown separately in 2 tables (Additional file 1: Table S1 and Additional file 2: Table S2) which include the level, location, year of publication, number of population, and prevalence of obesity and overweight in adults and under-18-years-old in Iran. Some studies reported the prevalence of obesity and overweight together, so for not losing the data, they were put on the separate columns in tables as well. In cases which were reported the prevalence in male/female or urban/Rural areas, the extracted data put in the tables separately. In view of the differences in standard diagnosis criteria for obesity and overweight in under-18-related studies, the criteria in these studies put in the table as well.
We found 15 and 12 National, and 71 and 96 sub national studies in adult and under-18 y related studies, respectively. There were found 4 common studies which carried out among adult and under-18 individuals. Considering the wide range of prevalence in different studies, to find a better overview of studies, we placed a summary of maximum and minimum reported prevalence in national and sub national studies in Additional file 3: Table S3.
The range of overweight and obesity prevalence in sub national studies in adult, were 12.8-76.4 (95% CI: (9.2-17.3, 75.1-77.6), and 2.4-35.4 (95% CI: 1.0-4.9, 31.4-39.6), respectively. The range of overweight and obesity among adult national studies were 27.0- 38.5 (95% CI: 26.8-27.1, 37.2-39.8), and 12.6-25.9 (95% CI: 12.2-13.0, 24.9-26.8). The first, second and third greatest national reported prevalence of obesity and overweight were 25.9, 25.1, and 22.3 among adult, and 11.9, 10.4, and 6.5 among under-18 population. The range of overweight and obesity in sub national studies among under-18 y were 2.4-67.1 (95% CI: 1.5-3.7, 63.3-70.8), and 0.6-27.7 (95% CI: 0.3-1.1, 25.4-30.0). The range of national reported prevalence of overweight and obesity in national studies among under-18 y were 5.0-13.5 (95% CI: 4.5-5.5, 13.4-13.6), and 3.2-11.9 (95% CI: 3.0-3.4, 11.3-12.4). The lowest and the highest prevalence of obesity in adult appertain to Shiraz and Rasht, and among under-18 y concern to Kerman and Gorgan.
Discussion
Obesity is the most apparent demonstration of an inappropriate sedentary lifestyle and increase in high caloric food consumption [22]. In 2005, a study of global burden of obesity, reported the estimated total numbers of overweight and obesity in adults, 937 million (23.2%), and 396 million (24.0%), respectively. It were projected the number of overweight and obese people in 2030 reach to 1.35 billion and 573 million [23]. The National Health and Nutrition Examination Survey in the United States as a country with a high prevalence of obesity and overweight, in 2010, more than one third of adult were obese [24]. In another adult population study in Spain, the prevalence of obesity was 22.9% (24.4% in men and 21.4% in women) [25]. The prevalence of overweight in Turkey was 19.0% in 2007 (17.4% in men, 20.4% in women) [26]. Among Asian countries, it is reported that the prevalence of obesity was 10.3%, and the prevalence of overweight and obesity together were 25.0% in Pakistan [27]. In our review the prevalence of overweight and obesity in adult national studies were higher with range 27.0-38.5 and 12.6-25.9, respectively.
On the other hand, obesity among children and adolescents has more than doubled and quadrupled in the past 3 decades [28]. Based on NCHS data brief in 2010, almost 17% of youth were obese [24]. Obese children are more likely to suffer from obesity in adulthood. Obesity at young ages is responsible for increasing risk of obesity-related diseases in children, even some disease in the past known as adult diseases such as type-2 diabetes. Therefore, this issue should be investigated with more attention. The prevalence of obesity among children and adolescents in the United States reaches from 7% and 5% in 1980, to nearly 18% and 21% in 2012 [29]. In 2005, 9.7% (11.3% for boys, 8.0% for girls) of South Korean children and adolescents were obese; 19.0% were overweight or obese [30]. Based on the MONICA project (monitoring of cardiovascular diseases) in 1998, Iran was one of seven countries with a high prevalence of obesity among children [31]. In this study, increasing prevalence of obesity/overweight is totally detectible especially in stepwise studies [32]-[34]. The national maximum prevalence of overweight and obesity were 13.5 and 11.9 in our study which are similar to the result of mentioned studies. The range of national report of the prevalence of overweight (adult: 27.0- 38.5, <18 y: 5.0-13.5) and obesity (adult: 12.6-25.9, <18 y: 3.2-11.9) was totally different with sub national overweigh (adult: 12.8-76.4, <18 y: 2.4-67.1) and obesity (adult: 2.4-35.4, <18 y: 0.6-27.7) reports, that he wide reported range in sub national studies can be related to the lower number of sample size.
Although the estimated prevalence of overweight and obesity are different in various studies around the world, but it is increasing in most of them as a common factor [23]. There were seen extensive variations in prevalence of obesity/overweight in different regions of Iran as well, which may relate to various cultural affiliations, and socioeconomic factors among different provinces. Iran is a multiethnic country, so the multiplicities in socio-cultural, environmental, and genetic factors, directly affect eating habits and lifestyle in every region. Climate variability as an environmental factor influences on dietary habits, mood, and activity level. The urbanization phenomenon is considered as an important factor underlying obesity which is noticeably increasing in Iran. It seems lack of appropriate job opportunities, and the desire to take advantage of urban amenities, encourage the rural population to migrate to big cities such as Tehran. Although consumption of fast foods and not home-made foods as an important causes of obesity are increasing in major cities, in rural regions consuming home-made foods are still common. So we are faced a big problem, a huge and growing urban population and following unhealthy lifestyles that surly affect the increasing prevalence of obesity in near future. Jafar TH in their study found that the prevalence of obesity in urban inhabitants in Pakistan was 2.5 greater of obesity in inhabitants rural [27]. The prevalence of obesity and its acceleration rate are more perceptible among big cities of Iran, especially provincial capital [35]-[40]. In the latest overweight and obesity prevalence in Tehran, which was conducted in 2013 among 20–84 aged, the prevalence of overweight and obesity was reported 34.1% (95% CI: 32.3-35.9), and 15.4% (95% CI: 14.0-16.8), respectively [41]. In a survey in ten provinces of china, the prevalence rates of overweight and obesity were 1.4%-7.6% and 0.6%-3.1% among children [42]. These rates substantially are higher among children in our study. Although most of national and Iranian studies were asserted that the prevalence of overweight/obesity are greater in urban areas [43]-[46], but there are some studies with inconsistent result, such a study in Turkey which was reported the higher prevalence of obesity in rural (17%) in comparison to urban areas (15.2%) [26]. Despite these differences, all the stepwise studies showed a noticeable increasing in obesity/overweight prevalence in last decade in all age and sex groups [32],[33],[47],[48].
In our review most of the studies reported higher prevalence of overweight and obesity among women than men [48]-[52], that may be due to lower physical activity among women in some areas.
Conclusion
This review were assessed all related studies which were reported the prevalence of obesity and overweight in normal population of Iran since 2005. There was seen noticeable increase in overweight and obesity prevalence among all ages and both sex of Iranian people as the worldwide growing repots. Due to the higher population of young people in Iran, Ignoring the complications, and Lack of effective preventive policy, burden of obesity in the near future will be problematic. So mothers’ education, particularly among house workers has an important role in managing dietary habits in their family. Their awareness about the side effects of obesity can be more efficient which not only improve their health condition, but also provide a healthy life style for their children as well.
Considering a lot of life- threatening complications following overweight/obesity, it is very important to have national organized educational and preventive programs. Mapping of obesity in Iranian children and adults, and meta-analysis based on geographic and climate areas is recommended.
Additional files
References
Ayatollahi S, Ghoreshizadeh Z: Prevalence of obesity and overweight among adults in Iran. Obes Rev 2010, 11(5):335–337.
Janghorbani M, Amini M, Willett WC, Gouya MM, Delavari A, Alikhani S: First nationwide survey of prevalence of overweight, underweight, and abdominal obesity in Iranian adults. Obesity 2007, 15(11):2797–2808.
Marinou K, Tousoulis D, Antonopoulos AS, Stefanadi E, Stefanadis C: Obesity and cardiovascular disease: from pathophysiology to risk stratification. Int J Cardiol 2010, 138(1):3–8.
Gill T: Epidemiology and health impact of obesity: an Asia Pacific perspective. Asia Pac J Clin Nutr 2006, 15(Suppl):3–14.
Organization WH:Obesity and Overweight. Fact Sheet No. 311. 2006.
Kelishadi R: Childhood overweight, obesity, and the metabolic syndrome in developing countries. Epidemiol Rev 2007, 29(1):62–76.
Carreira H, Pereira M, Azevedo A, Lunet N: Trends of BMI and prevalence of overweight and obesity in Portugal (1995–2005): A systematic review. Public Health Nutr 2012, 15(6):972–981.
Hasani-Ranjbar S, Nayebi N, Larijani B, Abdollahi M: A systematic review of the efficacy and safety of herbal medicines used in the treatment of obesity. World J Gastroenterol 2009, 15(25):3073.
Tee E: Obesity in Asia: prevalence and issues in assessment methodologies. Asia Pac J Clin Nutr 2002, 11(s8):S694-S701.
Lal A, Moodie M, Ashton T, Siahpush M, Swinburn B: Health care and lost productivity costs of overweight and obesity in New Zealand. Aust N Z J Public Health 2012, 36(6):550–556.
Hasani-Ranjbar S, Amoli MM, Tabatabaei-Malazy O, Rumi Y, Tavakkoly-Bazzaz J, Samimi H, Abbasifarid E: Effect of adiponectin gene polymorphisms on waist circumference in patients with diabetes. J Diabetes Metab Disord 2012, 11(1):14.
Tabatabaei-Malazy O, Hasani-Ranjbar S, Amoli MM, Heshmat R, Sajadi M, Derakhshan R, Amiri P, Namakchian M, Rezazadeh E, TavaKkoly-Bazzaz J, Keshtkar A, Larijani B: Gender-specific differences in the association of adiponectin gene polymorphisms with body mass index. Review Diabetic Stud 2010, 7(3):241.
Bazzaz JT, Shojapoor M, Nazem H, Amiri P, Fakhrzadeh H, Heshmat R, Parvizi M, Hasani Ranjbar S, Amoli MM: Methylenetetrahydrofolate reductase gene polymorphism in diabetes and obesity. Mol Biol Rep 2010, 37(1):105–109.
Ezzati M, Lopez AD, Rodgers A, Vander Hoorn S, Murray CJ: Selected major risk factors and global and regional burden of disease. Lancet 2002, 360(9343):1347–1360.
Ramachandran A, Snehalatha C: Rising burden of obesity in Asia. J Obes 2010, ᅟ: ᅟ.
Payab M, Hasani-Ranjbar S, Larijani B: Whether all obese subjects both in metabolic groups and non-metabolic groups should be treated or not. J Diabetes Metabolic Disord 2014, 13(1):21.
Hasani-Ranjbar S, Jouyandeh Z, Abdollahi M: A systematic review of anti-obesity medicinal plants-an update. J Diabetes Metab Disord 2013, 12(1):28.
Mohammad K, Larijani B: A systematic review of the antioxidant, anti-diabetic, and anti-obesity effects and safety of triphala herbal formulation. J Med Plants Res 2013, 7(14):831–844.
Musaiger AO: Overweight and obesity in Eastern Mediterranean Region: Prevalence and possible causes. J Obes 2011, 2011: 17. doi:10.1155/2011/407237
Low S, Chin MC, Deurenberg-Yap M: Review on epidemic of obesity. Ann Acad Med Singap 2009, 38(1):57.
Bahreini N, Noor MI, Koon PB, Talib RA, Lubis SH, Dashti MG, Salehi-Abarghouei A, Esmeilzadeh A: Weight status among Iranian adolescents: Comparison of four different criteria. J Res Med Sci 2013, 18(8):641.
Azizi F, Azadbakht L, Mirmiran P: Trends in overweight, obesity and central fat accumulation among Tehranian adults between 1998–1999 and 2001–2002: Tehran lipid and glucose study. Ann Nutr Metab 2005, 49(1):3–8.
Kelly T, Yang W, Chen C, Reynolds K, He J: Global burden of obesity in 2005 and projections to 2030. Int J Obes 2008, 32(9):1431–1437.
Ogden CL: Statistics NCfH: Prevalence of obesity in the United States, 2009–2010. In NCHS Data Brief, no 82. National Center for Health Statistics, ᅟ; 2012.
Gutiérrez-Fisac J, Guallar-Castillón P, León-Muñoz L, Graciani A, Banegas J, Rodríguez-Artalejo F: Prevalence of general and abdominal obesity in the adult population of Spain, 2008–2010: the ENRICA study. Obes Rev 2012, 13(4):388–392.
Delibasi T, Karaaslan Y, Ustun I, Koroglu E, Hosgor S: National prevalence of underweight, overweight and obesity in Turkey: cross sectional study of a representative adult population. Central European J Med 2007, 2(3):294–303.
Jafar TH, Chaturvedi N, Pappas G: Prevalence of overweight and obesity and their association with hypertension and diabetes mellitus in an Indo-Asian population. Can Med Assoc J 2006, 175(9):1071–1077.
Ogden CL, Carroll MD, Kit BK, Flegal KM: Prevalence of childhood and adult obesity in the United States, 2011–2012. JAMA 2014, 311(8):806–814.
Statistics NCfH:Health, United States, 2011: With Special Feature on Socioeconomic Status and Health. Statistics NCfH, USA; 2012.
Oh K, Jang MJ, Lee NY, Moon JS, Lee CG, Yoo MH, Kim YT: Prevalence and trends in obesity among Korean children and adolescents in 1997 and 2005. Korean J Pediatrics 2008, 51(9):950–955.
Dobson AJ, Evans A, Ferrario M, Kuulasmaa KA, Moltchanov VA, Sans S, Tunstall-Pedoe H, Tuomilehto JO, Wedel H, Yarnell J: Changes in estimated coronary risk in the 1980s: data from 38 populations in the WHO MONICA Project. Ann Med 1998, 30(2):199–205.
Kelishadi R, Mohammadifard N, Sarrazadegan N, Nouri F, Pashmi R, Bahonar A, Heidari H, Asgari S, Boshtam M, Mardani A: The effects of a comprehensive community trial on cardiometabolic risk factors in adolescents: Isfahan Healthy Heart Program. ARYA Atherosclerosis 2012, 7(4):184–190.
Barzin M, Hosseinpanah F, Saber H, Sarbakhsh P, Nakhoda K, Azizi F: Gender differences time trends for metabolic syndrome and its components among Tehranian children and adolescents. Cholesterol 2012, 2012: 6. doi:10.1155/2012/804643
Motlagh ME, Kelishadi R, Ziaoddini H, Mirmoghtadaee P, Poursafa P, Ardalan G, Dashti M, Aminaee T: Secular trends in the national prevalence of overweight and obesity during 2007–2009 in 6-year-old Iranian children. J Res Med Sci 2011, 16(8):979.
Heshmat R, Khashayar P, Meybodi H, Homami MR, Larijani B: The appropriate waist circumference cut-off for Iranian population. Acta Med Indones 2010, 42(4):209–215.
Nuri R, Moghadasi M, Moraveji F: Association between Obesity and Overweight with Lifestyle Status and Physical Fitness Level in Shiraz Adults. Iran J Endocrinol Metabol 2012, 14(3):241–247.
Shirani S, Heidari K, Sabzghabaee AM, Mirmoghtadaee P, Hoseini L, Aalifar H, Aalifar H, Fadaei H, Esnaashari H, Soltani R: The modifiable noncommunicable risk factors among an Iranian population. Southeast Asian J Tropical Med Public Health 2012, 43(5):1227.
Lankarani KB, Ghaffarpasand F, Mahmoodi M, Lotfi M, Zamiri N, Heydari ST, Fallahzadeh MK, Maharlouei N, Babaeinejad M, Mehravar S, Geramizadeh B: Non alcoholic fatty liver disease in southern Iran: a population based study. Hepatitis 2013, 13(5):6. doi:10.5812/hepatmon.9248
Dastgiri S, Mahdavi R, TuTunchi H, Faramarzi E: Prevalence of obesity, food choices and socio-economic status: a cross-sectional study in the north-west of Iran. Public Health Nutr 2006, 9(08):996–1000.
Yarahmadi S, Etemad K, Hazaveh AM, Azhang N: Urbanization and non-communicable risk factors in the capital city of 6 big provinces of iran. Iranian J Public Health 2013, 42(Supple1):113.
Moghimi-Dehkordi B, Safaee A, Vahedi M, Pourhoseingholi A, Pourhoseingholi M, Ashtari S, Zali MR: Overweight and obesity and related factors in urban Iranian population aged between 20 to 84 years. Ann Med Health Sci Res 2013, 3(2):171–176.
Xie S, Wang J, Li N, Jiang W, Yang S, Li X, Ling Z, Zhang J: [Survey on overweight and obesity of preschool children in rural areas from ten provinces of China]. Zhonghua liu xing bing xue za zhi=. Zhonghua Liuxingbingxue Zazhi 2014, 35(4):425–428.
Maddah M, Sharami SH: Obesity among Iranian old adult women in urban and rural areas in Guilan. Int J Cardiol 2010, 145(1):44–45.
Rashidy-Pour A, Malek M, Eskandarian R, Ghorbani R: Obesity in the Iranian population. Obes Rev 2009, 10(1):2–6.
Veghari G, Sedaghat M, Joshaghani H, Hoseini A, Niknezhad F, Angizeh A, Tazik E, Moharloei P: The prevalence of obesity and its related risk factor in the north of Iran in 2006. J Research Health Sci 2010, 10(2):116–121.
Veghari G, Sedaghat SM, Maghsoodloo S, Banihashem S, Angizeh A, Tazik E: Obesity and some related socioeconomic factors: an epidemiological study. J Iran Institute Health Sci Res 2012, 11(6):807–813.
Sarrafzadegan N, Kelishadi R, Sadri G, Malekafzali H, Pourmoghaddas M, Heidari K, Shirani S, Bahonar A, Boshtam M, Asgary S, Mohammadifard N, Sadeghi M, Eshrati B, Hadipour E, Esmaillzadeh A, O’Loughlin JL: Outcomes of a comprehensive healthy lifestyle program on cardiometabolic risk factors in a developing country: the Isfahan Healthy Heart Program. Arch Iran Med 2013, 16(1):4–11.
Hosseinpanah F, Barzin M, Eskandary PS, Mirmiran P, Azizi F: Trends of obesity and abdominal obesity in Tehranian adults: a cohort study. BMC Public Health 2009, 9(1):426.
Alikhani S, Delavari A, Alaedini F, Kelishadi R, Rohbani S, Safaei A: A province-based surveillance system for the risk factors of non-communicable diseases: A prototype for integration of risk factor surveillance into primary healthcare systems of developing countries. Public Health 2009, 123(5):358–364.
Delavari A, Forouzanfar MH, Alikhani S, Sharifian A, Kelishadi R: First Nationwide Study of the Prevalence of the Metabolic Syndrome and Optimal Cutoff Points of Waist Circumference in the Middle East The National Survey of Risk Factors for Noncommunicable Diseases of Iran. Diabetes Care 2009, 32(6):1092–1097.
Kelishadi R, Alikhani S, Delavari A, Alaedini F, Safaie A, Hojatzadeh E: Obesity and associated lifestyle behaviours in Iran: findings from the first national non-communicable disease risk factor surveillance survey. Public Health Nutr 2008, 11(03):246–251.
Rostambeigi N, Shaw JE, Atkins RC, Ghanbarian A, Cameron AJ, Forbes A, Momenan A, Hadaegh F, Mirmiran P, Zimmet PZ, Azizi F, Tonkin AM: Waist circumference has heterogeneous impact on development of diabetes in different populations: longitudinal comparative study between Australia and Iran. Diabetes Res Clin Pract 2010, 88(1):117–124.
Azadbakht L, Mirmiran P, Shiva N, Azizi F: General obesity and central adiposity in a representative sample of Tehranian adults: prevalence and determinants. Int J Vitam Nutr Res 2005, 75(4):297–304.
Gargari BP, Behzad MH, Ghassabpour S, Ayat A: Prevalence of overweight and obesity among high-school girls in Tabriz, Iran, in 2001. Food Nutri Bullet 2004, 25(3):288–291.
Pourshams A, Malekzadeh R, Monavvari A, Akbari MR, Mohamadkhani A, Yarahmadi S, Sedighi N, Mohamadnejad M, Sotoudeh M, Madjlesii A: Prevalence and etiology of persistently elevated alanine aminotransferase levels in healthy Iranian blood donors. J Gastroenterol Hepatol 2005, 20(2):229–233.
Vahidi Nia AA, Sardarian K: Assessment of nutritional status in rural regions of Hamadan city/Iran, 2003. Iran South Med J 2006, 8(2):187–193.
Mostafavi H, Dabaghmanesh M, Zare N: Prevalence of obesity and over weight in adolescents and adult population in Shiraz. Iran J Endocrinol Metabol 2005, ᅟ: ᅟ.
Agheli N, Assef Zadeh S, Rajabi M: The prevalence of cardiovascular risk factors among population aged over 30 years in Rasht and Qazvin. J Qazvin Univ of Med Sci 2005, 35: 59–65.
Mozafari M, Nosrati S, Purmansour G, Rezaei M: Factors affecting the prevalence of obesity among 15–49- years old women referred to urban health clinics in Ilam in −2004. Ilam Univer Med Sci 2006, 14(1):8–17.
Alavi Naieny A, Dorosti Motlagh A, Aghdak P: Survey of obesity, underweight and associated factors in elderly people, using some of anthropometric indices in Isfahan City, 2004. J Mazandaran Univer Med Sci 2006, 16(52):117–123.
Hajian K, Hiedari B: Prevalence of abdominal obesity in a population aged 20 to 70 years in urban Mazandaran (northeran Iran, 2004). Iran J Endocrinol Metabol 2006, 8(2):147–156.
Sarshar N, Khajavi A: The prevalence of obesity in females of 15–65 years of age in Gonabad, Iran. Quarterly Horizon Med Sci 2006, 12(3):38–43.
Abdollahi AA, Hoseini SA, Molaee E, Kalagari S: The frequency of obesity and waist-hip ratio in the urban population of Golestan province. J Gorgan Bouyeh Faculty Nurs Midwifery 2006, 3(2):10–15.
Bahrami H, Sadatsafavi M, Pourshams A, Kamangar F, Nouraei M, Semnani S, Brennan P, Boffetta P, Malekzadeh R: Obesity and hypertension in an Iranian cohort study; Iranian women experience higher rates of obesity and hypertension than American women. BMC Public Health 2006, 6(1):158.
Rezaeian M, Salem Z: Prevalence of obesity and abdominal obesity in a sample of urban adult population within South East of Iran. Pakistan J Med Sci 2007, 23(2):193.
Amani R: Comparison between bioelectrical impedance analysis and body mass index methods in determination of obesity prevalence in Ahvazi women. Eur J Clin Nutr 2006, 61(4):478–482.
Siasi F, Jalali Mahmoud MS: Assessment of Body Mass Index and its Relationship with Iron Status Indices among Women in Rural Areas of Kerman Province. Koomesh, Iran; 2007.
Hajian-Tilaki K, Heidari B: Prevalence of obesity, central obesity and the associated factors in urban population aged 20–70 years, in the north of Iran: a population-based study and regression approach. Obes Rev 2007, 8(1):3–10.
Veghari G, Mansourian A: The comparative study of obesity among mothers with different ethnic groups in Northern IRAN. Iranian J Public Health 2007, 36(3):71–76.
Mazloomzadeh S, Moosani A, Dinmohammadi H: Epidemiology of overweight and obesity in Zanjan province 1383. ZUMS Journal 2006, 14(56):57–64.
Zare N, Keshavarzi S, Zeighami B: Some risk factors of obesity in rural women of Zarrindasht: using linear regression odds ratio. Zahedan J Res Medical Sci 2007, 9(2):133–140.
Hosseinpanah F, Rambod M, Azizi F: Population attributable risk for diabetes associated with excess weight in Tehranian adults: a population-based cohort study. BMC Public Health 2007, 7(1):328.
Kelishadi R, Gharipour M, Sadri G, Tavasoli A, Amani A: Cardiovascular disease risk factors, metabolic syndrome and obesity in an Iranian population. East Mediterr Health J 2008, 14(5):1070–1079.
Bakhshi E, Eshraghian MR, Mohammad K, Foroushani AR, Zeraati H, Fotouhi A, Siassi F, Seifi B: Sociodemographic and smoking associated with obesity in adult women in Iran: results from the National Health Survey. J Public Health 2008, 30(4):429–435.
Nemati A, Naghizadeh BA: Assessment of nutritional status in post menopausal women of Ardebil. Iran J Biol Sci 2008, 8(1):196–200.
Esteghamati A, Khalilzadeh O, Anvari M, Ahadi MS, Abbasi M, Rashidi A: Metabolic syndrome and insulin resistance significantly correlate with body mass index. Arch Med Res 2008, 39(8):803–808.
Nabipour I, Amiri M, Imami S, Jahfari S, Nosrati A, Iranpour D, Soltanian AR: Unhealthy lifestyles and ischaemic electrocardiographic abnormalities: the Persian Gulf Healthy Heart Study. East Mediterr Health J 2008, 14(4):858–868.
Asgari F, Aghajani H, Haghazali M, Heidarian H: Non-communicable diseases risk factors surveillance in Iran. Iranian J Public Health 2009, 38(Suppl. 1):119–122.
Azimi–Nezhad M, Ghayour–Mobarhan M, Safarian M, Esmailee H, Parizadeh SMR, Rajabi-Moghadam M, Gholami A, Oladi MR, Ferns GA: Anthropometric indices of obesity and the prediction of cardiovascular risk factors in an Iranian population. Scientific World J 2009, 9: 424–430.
Barzin M, Mirmiran P, Afghan M, Azizi F: The Prevalence of Obesity, Central Obesity and Their Relationship with Nutritional Status and Physical Activity among 18 to 25 Year-Old Females Referring to Premarriage Consultation Centers (Tehran, Iran, Summer 2008). Pajoohandeh J 2009, 14(2):59–65.
Hasani-Ranjbar S, Shirzad N, Mashayekh bakhshi F: A 3-year-old boy with severe obesity and pseudoacromegaly; short course treatment with Orlistat™. Iranian J Diabetes Lipid Disorders 2010, 9(0):43–48.
Esmaeily H, Azimi-Nezhad M, Ghayour-Mobarhan M, Parizadeh M-R, Safarian M, Parizadeh M-J, Hasankhani B, Salarini E, Hushang ZK, Javad H, Oladi MR, Ferns G: Association between socioeconomic factors and obesity in Iran. Pak J Nutr 2009, 8(1):53–56.
Esteghamati A, Meysamie A, Khalilzadeh O, Rashidi A, Haghazali M, Asgari F, Kamgar M, Gouya MM, Abbasi M: Third national Surveillance of Risk Factors of Non-Communicable Diseases (SuRFNCD-2007) in Iran: methods and results on prevalence of diabetes, hypertension, obesity, central obesity, and dyslipidemia. BMC Public Health 2009, 9(1):167.
Harati H, Hadaegh F, Saadat N, Azizi F: Population-based incidence of Type 2 diabetes and its associated risk factors: results from a six-year cohort study in Iran. BMC Public Health 2009, 9(1):186.
Sharifi F, Mousavinasab S, Saeini M, Dinmohammadi M: Prevalence of metabolic syndrome in an adult urban population of the west of Iran. Exp Diabetes Res 2009, 2009: 5. doi:10.1155/2009/136501
Nematy M, Sakhdari A, Ahmadi-Moghaddam P, Aliabadi M, Kimiagar M, Ilaty A, Azim-Nejad M, Shakeri MT, Ghayour-Mobarhan M, Sahebkar A, Ferns G: Prevalence of obesity and its association with socioeconomic factors in elderly Iranians from Razavi-Khorasan province. Sci World J 2009, 9: 1286–1293.
Mohammad K, Golestan B, Majdzadeh R, Chaman R, Nedjat S, Karimloo M: Socioeconomic Status and Obesity Relationship in Non-Menopause Women Aged 15–49 Years in Tehran. Iran Iranian J Public Health 2009, 38(3):84–89.
Abdollahi AA, Vagari G: The correlation between age, gender and education with obesity in urban population of Golestan province. Iranian J Endocrinol Metabol 2010, 12(3):276–282.
Ebrahimi M, Mansournia MA, Haghdoost AA, Abazari A, Alaeddini F, Mirzazadeh A, Yunesian M: Social disparities in prevalence, treatment and control of hypertension in Iran: second National Surveillance of Risk Factors of Noncommunicable Diseases, 2006. J Hypertens 2010, 28(8):1620–1629.
Esteghamati A, Khalilzadeh O, Mohammad K, Meysamie A, Rashidi A, Kamgar M, Abbasi M, Asgari F, Haghazali M: Secular trends of obesity in Iran between 1999 and 2007: National Surveys of Risk Factors of Non-communicable Diseases. Metab Syndr Relat Disord 2010, 8(3):209–213.
Veghari G, Sedaghat M, Joshaghani H, Hoseini SA, Niknezad F, Angizeh A, Tazik E, Moharloei P: Association between socio-demographic factors and diabetes mellitus in the north of Iran: A population-based study. Int J Diabetes Mellitus 2010, 2(3):154–157.
Ahmadnia A, Emamghole Khooshehcheen T, Ahmadnia H, Falakalaflake B: An Investigation about Anthropometric Indicator for Inhabitants of Zanjan in Comparison with NCHS Standards. ZUMS J 2010, 18(71):70–80.
Najafi I, Attari F, Islami F, Shakeri R, Malekzadeh F, Salahi R, Yapan Gharavi M, Hosseini M, Broumand B, Nobakht Haghighi A, Larijani B, Malekzadeh R: Renal function and risk factors of moderate to severe chronic kidney disease in Golestan Province, northeast of Iran. PLoS One 2010, 5(12):e14216.
Maddah M, Nikooyeh B: Factors associated with overweight in children in Rasht, Iran: gender, maternal education, skipping breakfast and parental obesity. Public Health Nutr 2010, 13(02):196–200.
Maddah M, Nikooyeh B: Obesity among Iranian adolescent girls: location of residence and parental obesity. J Health Popul Nutr 2010, 28(1):61.
Paknahad Z, Saboktagin M: Studying the Blood Pressure in Isfahan Rural Residents and Its Relationship with BMI. J Health Syst Res 2010, 6(3):506–512.
Delavar M, Lye M, Hassan S, Khor G, Hanachi P: Physical activity, nutrition, and dyslipidemia in middle-aged women. Iranian JPublic Health 2011, 40(4):89.
Naghashpour M, Shakerinejad G, Haghighizadeh M, Hajinajaf S, Jarvandi F: Prevalence of Obesity and its Association with Demographic Indices in Referents to University Jahad Khozestan Clinic. Jundishapur Sci Med J 2011, 10(1):21–35.
Hatmi ZN, Mahdavi-Mazde M, Hashemi-Nazari SS, Hajighasemi E, Nozari B, Jalilian N, Mahdavi A: Relationship between the pattern of coronary artery disease risk factors and lipid ratios with five groups of body mass index in 28566 healthy adults. Acta Medica Iranica 2011, 49(11):730–736.
Sepandi M, Haghighi-Zadeh M-H, Taghdir M: Relationship between Body Mass Index and Demographic Features in Women. J Knowedge Health 2011, 6(1):15–18.
Heydari S-T, Seyed-Mohammad-Taghi Ayatollahi NZ: Diagnostic value of bioelectrical impedance analysis versus body mass index for detection of obesity among students. Asian J Sports Med 2011, 2(2):68.
Sadeghi-Bazargani H, Jafarzadeh H, Fallah M, Hekmat S, Bashiri J, Hosseingolizadeh G, Soltanmohammadzadeh MS, Mortezazadeh A, ShakerA DM, Zohouri A, Khosravi O, Nasimidoust R, Malekpour N, Kharazmi E, Babaei M, Nadirmohammadi M, Mashhadi-Abdollahi E: Risk factor investigation for cardiovascular health through WHO STEPS approach in Ardabil. Iran Vasc Health Risk Manage 2011, 7: 417.
Navadeh S, Sajadi L, Mirzazadeh A, Asgari F, Haghazali M: Housewives’ Obesity Determinant Factors in Iran; National Survey-Stepwise Approach to Surveillance. Iranian J Public Health 2011, 40(2):87.
Namayandeh S, Sadr S, Ansari Z, Rafiei M: A cross-sectional study of the prevalence of coronary artery disease traditional risk factors in Yazd urban population, Yazd healthy heart project. Iran Cardiovasc Res J 2011, 5(1):7–13.
Hosseini S, Cumming R, Sajjadi P, Bijani A: Chronic diseases among older people in Amirkola, northern Islamic Republic of Iran. EMHJ 2011, 17(11):843–849.
Faramarzi H, Bagheri P, Bahrampour A, Halimi L, Rahimi N, Ebrahimi M: The comparison of prevalence of diabete and hypertension between rural areas of fars and rural area of emro region. IJEM 2011, 13(2):157–164.
Moghadasi M, Naser K, Shakerian S, Razavi A: Prevalence of Overweight, Obesity and Physical Fitness in Shiraz Adolescents. Iranian J Endocrinol Metabo 2011, 12(5):476–482.
Mohammadi N, Shobeiri F, KHEIROLAHI A, OMIDI A, AMINI R: Frequency of Over Wieght & Obesity of Women in Referents to Medical and Health Centers in Hamadam City. Nasim-Danesh (Sci J Hamadan Nurs Midwifery Faculty) 2011, 19(36):36–41.
Biglarian A, Seifi B, Bakhshi E, Mohammad K, Rahgozar M, Karimlou M, Serahati S: Low back pain prevalence and associated factors in Iranian population: findings from the national health survey. Pain ResTreatment 2012, 2012: 5. doi:10.1155/2012/653060
Gharakhanlou R, Farzad B, Agha-Alinejad H, Steffen LM, Bayati M: Anthropometric measures as predictors of cardiovascular disease risk factors in the urban population of Iran. Arq Bras Cardiol 2012, 98(2):126–135.
Zarei S, Bigizadeh S, Pourahmadi M, Ghobadifar MA: Chronic pain and its determinants: a population-based study in Southern Iran. Korean J Pain 2012, 25(4):245–253.
Najafipour H, Mirzazadeh A, Haghdoost A-A, Shadkam M, Afshari M, Moazenzadeh M, Nasri HR, Masoomi M, Mirzaiepour F, Sarvar Azimzadeh B, Forood A, Bahreini F, Mahmoudi MR, Sanjari M, Malek Mohamadi T, Banivaheb GH, Naderi MA, Moshtaghi Kashanian GH, Malekpour Afshar R, Ghazanfari Z, Navadeh S, Shah Esmaeili A: Coronary artery disease risk factors in an urban and peri-urban setting, Kerman, Southeastern Iran (KERCADR study): methodology and preliminary report. Iranian J Public Health 2012, 41(9):86–92.
Poorolajal J, Zamani R, Mir-Moeini R, Amiri B, Majzoobi M, Erfani H, Bathaei SJ: Five-year Evaluation of Chronic Diseases in Hamadan, Iran: 2005–2009. Iranian J Public Health 2012, 41(3):71.
Jafari E, Sebghatollahi V, Kolahdoozan S, Elahi E, Pourshams A: Body Mass Index and ABO Blood Groups amongDifferent Ethnicities of the Golestan Cohort Study Subjects. Govaresh 2012, 17(1):50–54.
Veghari G, Sedaghat M, Maghsodlo S, Banihashem S, Moharloei P, Angizeh A, Tazik E, Moghaddami A: Influence of education in the prevalence of obesity in Iranian northern adults. J Cardiovasc Disease Res 2013, 4(1):30–33.
Veghari G, Sedaghat M, Maghsodlo S, Banihashem S, Moharloei P, Angizeh A, Tazik E, Moghaddami A: Differences in the Prevalence of Obesity among Fars-Native, Turkman, and Sisstanish Ethnic Groups in Iranian Northern Adults in 2010. Intern Cardiovas Res J 2013, 7(2):56–61.
Hesar KM, Mollanovruzi A, Hamedinia M: The prevalence of obesity and its related factors in 30–50 year old women of neyshabur with an emphasis on physical activity. Iranian Journal of Endocrinology & Metabolism 2013, 14(5):472–478.
Rashidi H, Ramezani Tehrani F, Bahri Khomami M, Tohidi M, Azizi F: To what extent does the use of the Rotterdam criteria affect the prevalence of polycystic ovary syndrome? A community-based study from the Southwest of Iran. European Journal of Obstetrics & Gynecology and Reproductive Biology 2014, 174: 100–105.
Kabir A, Pourshams A, Khoshnia M, Malekzadeh F: Normal Limit for Serum Alanine Aminotransferase Level and Distribution of Metabolic Factors in Old Population of Kalaleh, Iran. Hepat Mon 2013, 13(10):e10640.
Jahangiri H, Norouzi A, Dadsetan P, Mirbagheri SA: Prevalence and correlates of obesity among older adults. Life Sci J 2013, 10(4s):90–96.
Valizadeh M, Sohbatloo F: Mousavinasab n. A Survey of Anthropometric Indices [Weight, Height, and Body Mass Index (BMI)] in Secondary School Girls of Zanjan 2004–2005. ZUMS J 2005, 13(52):30–36.
Sotoudeh G, Khosravi S, Khajehnasiri F, Khalkhali HR: High prevalence of overweight and obesity in women of Islamshahr. Iran Asia Pac J Clin Nutr 2005, 14(2):169–172.
Mostafavi H, Dabagh Manesh M, Zare N: Prevalence of obesity and over weight in adolescents and adult population in Shiraz. Iranian J Endocrinol Metabol 2005, 7(1):57–66.
Soheilifar J, Emdadi M: Relation Between Breast Feeding with Overweight and Obesity in Hamadan Primary School Children. Scientific J Hamadan Univ Med Sci 2005, 12(2):54–57.
Nader F, Aramesh K: Assessment of the status of the health of shiraz’s primary schools’children; 2001–2002. J Mazandaran Univ Med Sci 2005, 15(46):56–64.
Bazhan M, Kalantari N, Ghaffarpoor M, Houshiar-Rad A, Alavi MH: Prevalence of obesity, fat distribution and its relationship with food consumption pattern in secondary school girls in Lahijan. Iranian J Endocrinol Metabol 2005, 7(1):37–46.
Jazayeri SMHM: Overweight and obesity among school-aged children of metropolitan Tehran. Iran Pakistan J Nutr 2005, 4(5):342–344.
Khaji A, Khodaii S, Karbakhsh M, Faeghi A, Azizi S, Firoozian A, Jafari J: Blood pressure and obesity in young adolescents in Tehran. Iran J Pediatr 2006, 16(1):45–50.
Montazery Fard F, Karaji Bani M, Dashipour A: The prevalence of obesity and wasting and their correlation with food intake in female junior school students in Zahedan, 2004. Iranian South Med J 2006, 9(1):66–76.
Moayeri H, Bidad K, Aghamohammadi A, Rabbani A, Anari S, Nazemi L, Gholami N, Zadhoush S, Nadia Hatmi Z: Overweight and obesity and their associated factors in adolescents in Tehran, Iran, 2004–2005. Eur J Pediatr 2006, 165(7):489–493.
Abtahi M, HoushiarRad A, Abdollahi M, Mazaheri N, Mohammadpour B: Prevalence of stunting, wasting and overweight among Iranian under 5 year-old children: A national study. In Annals of Nutrition and Metabolism. Karger Allschwilerstrasse 10, Ch-4009 Basel, Switzerland; 2007.
Amini M, Omidvar N, Kimiagar M: Prevalence of overweight and obesity among junior high school students in a district of Tehran. J Res Med Sci 2007, 12(6):315–319.
Haji Faraji M, Esfarjani F, Roustaee R, Khoshfetrat M, Kamrani Z: Assessment of Anthropometric Status of Adolescents in Public Guidance Schools in East Tehran, 2006. Iranian J Nutrit Sci Food Technol 2007, 2(2):37–43.
Maddah M: Overweight and obesity among Iranian female adolescents in Rasht: more overweight in the lower social group. Public Health Nutr 2007, 10(05):450–453.
Sadeghi M, Alizadeh F: Association between dental caries and body mass index-for-age among 6–11-year-old children in Isfahan in 2007. J Dental Res 2007, 1(3):119.
Mozaffari H, Nabaei B: Obesity and related risk factors. Indian J Pediatrics 2007, 74(3):265–267.
Gholamreza V, Mohsen S: The comparative study of body mass index distribution among preschool children in a 7 years period in north of Iran. J Appl Sci 2007, 7: 2681–2685.
Ayatollahi S, Mostajabi F: Prevalence of obesity among schoolchildren in Iran. Obes Rev 2007, 8(4):289–291.
Dorosty AR, Karamsoltani Z, Jazayeri A, Siyasi F, Eshraghian MR: Association between obesity, food security and related family factors. J School Public Health InstitPublic Health Res 2008, 6(1):1–9.
Khabazkhoob M, Fotouhi A, Moradi A, Mohammad K: Thinness and Obesity Based on Body Mass Index in Dezfool Schoolchildren in 2004. Iranian J Epidemiol 2008, 3(3):35–43.
Taheri F, Kazemi T, Taghizadeh B, Najibi G: Prevalence of Overweight and Obesity in Birjand Adolescents. Iran J Endocrinol Metabol 2008, 10(2):121–126.
Golestan M, Akhavan-Karbasi S, Fallah-Tafti M, Sharafaddini M: Prevalence of Obesity, Overweight and Underweight in Guidance School Students. J Shahid Sadoughi Univer Med Sci 2008, 16(2):35–1.
Kelishadi R, Ardalan G, Gheiratmand R, Majdzadeh R, Hosseini M, Gouya M, Razaghi MR, Delavari A, Motaghian M, Barekati H, Mahmoud-Arabi MS, Lock K: Thinness, overweight and obesity in a national sample of Iranian children and adolescents: CASPIAN Study. Child Care Health Dev 2008, 34(1):44–54.
Dorosty AR, Baygi F, Eshraghian MR: Prevalence of obesity among school children in Neishabour (2005). J Qazvin Univer Med Sci 2008, 12(1):73–79.
Hajian K, Sajadi P, Rezvani A: Prevalence of overweight and underweight among primary school children aged 7–12 years (babol__awt_nokt_comma__ 2006). J Babol Univer Med Sci 2008, 10(3):83–91.
Bidad K, Anari S, Tavasoli S, Nazemi L, Gholami N, Zadhush S, Moayeri H: Dietary intakes of adolescent girls in relation to weight status. Iran J Public Health 2008, 37(1):114–118.
Alavian SM, Mohammad-Alizadeh AH, Esna-Ashari F, Ardalan G, Hajarizadeh B: Non alcoholic fatty liver disease prevalence among school aged children and adolescents in Iran and its association with biochemical and anthropometric measures. Liver Int 2009, 29(2):159–163.
Houshiar Rad A, Dorosty A, Kalantari N, Abdollahi M, Abtahi M: Prevalence of stunting, underweight, wasting and overweight among Iranian under-five-year-old children (2000–2002). Iran J Nutri Sci Food Technol 2009, 3(4):49–56.
Eftekhari M, Mozaffari-Khosravi H, Shidfar F: The relationship between BMI and iron status in iron-deficient adolescent Iranian girls. Public Health Nutr 2009, 12(12):2377–2381.
Akhavan-Karbasi S, Fallah R, Golestan M, Sadr-Bafghi M: Prevalence and Risk Factors of Obesity and Overweight among Primary School Children in Yazd. J Shahid Sadoughi Univer Med Sci 2009, 16(5):8–13.
Ataei N, Hosseini M, Iranmanesh M: The relationship of body mass index and blood pressure in Iranian children < 7 years old. J Trop Pediatr 2009, ᅟ: 5. https://doi:10.1093/tropej/fmp014
Maddah M, Rashidi A, Mohammadpour B, Vafa R, Karandish M: In-school snacking, breakfast consumption, and sleeping patterns of normal and overweight Iranian high school girls: a study in urban and rural areas in Guilan, Iran. J Nutr Educ Behav 2009, 41(1):27–31.
Taheri F, Kazemi T: Prevalence of overweight and obesity in 7 to 18 year-Old children in birjand/Iran. Iran J Pediatr 2009, 19(2):135–140.
Veghari G, Marjany A, Abdollahy A, Rahmani H, Molaei E, Hosseiny SA, Bemani M, Ebrahim Kordjazi M: The comparison of children physical growth status between turkman and Non-tutkman in rural area in gorgan, north of Iran. J Gorgan Univer Med Sci 2009, 11(3):47–52.
Salem Z, Vazirinejad R: Prevalence of obesity and metabolic syndrome in adolescent girls in South East of Iran. Pak J Med Sci 2009, 25(2):196–200.
Faghih S, Taleban F, Abadi A, Ansari N: Trends of overweight and obesity among 14–18 years old urban adolescent girls among senior high schools, Ahvaz, Iran. Iran J Diabetes Lipid Disord 2009, 1(1):19–26.
Maddah M: Risk factors for overweight in urban and rural school girls in Iran: skipping breakfast and early menarche. Int J Cardiol 2009, 136(2):235–238.
Maddah M: Overweight among rural girls in Iran: A terrifying prospects of cardiometabolic disorders. Int J Cardiol 2009, 132(3):442–444.
Fallahzadeh H, Golestan M, Rezvanian T, Ghasemian Z: Breast-feeding history and overweight in 11 to 13-year-old children in Iran. World J Pediatr 2009, 5(1):36–41.
Haeri Behbahani B, Dorosty AR, Eshraghian MR: Assessment of obesity in children: Fat mass index versus body mass index. Tehran Univer Med J 2009, 67(6):408–414.
Montazerifar F, Karajibani M, Rakhshani F, Hashemi M: Prevalence of underweight, overweight and obesity among high-school girls in Sistan va Baluchistan. East Mediterr Health J 2009, 15(5):1293–1300.
Fesharakinia A, Zarban A, Sharifzadeh G-R: Relationship of body mass index with serum lipids in elementary school students. Indian J Pediatrics 2009, 76(7):729–731.
Rahmanpour H, Heidari R, Mousavinasab S, Sharifi F, Fekri S: The Prevalence of Polycystic Ovarian Syndrome in 14–18 year old girls of Zanjan High Schools, 2008. ZUMS J 2009, 17(67):79–88.
Mirhosseini N-Z, Mohd Yusoff NA, Shahar S, Parizadeh SMR, Ghayour Mobarhen M, Shakery MT: Prevalence of the metabolic syndrome and its influencing factors among adolescent girls in Mashhad, Iran. Asia Pac J Clin Nutr 2009, 18(1):131.
Rafraf M, Gargari BP, Safaiyan A: Prevalence of prehypertension and hypertension among adolescent high school girls in Tabriz. Iran Food Nutri Bullet 2010, 31(3):461–465.
Ahmadi S, Shahsavari S, Ahmadi H, Tabatabaei Far T: Prevalence of Overweight, Obesity and Underweight Among High School Students in Sanandaj: 2006–2007. Iran J Endocrinol Metabol 2010, 12(2):153–159.
Mortazavi Z, Roudbari M: Breakfast Consumption and Body Mass Index in Primary, Secondary and High School Boys in Zahedan 2005–2006. Iran J Endocrinol Metabol 2010, 12(4):345–351.
Amidi Mazaheri M, Hoseini M: Prevalence of underweight, overweight and obesity among high school girls in Isfahan. J Health Syst Res 2010, 6(1):1–6.
Ahmadi E, Tehrani AR, Ahmadi A: Prevalence of obesity, overweight and underweight among elementary school children in southern Iran, 2009. Am J Appl Sci 2010, 7(11):1439.
Hosseini M, Ataei N, Aghamohammadi A, Yousefifard M, Taslimi S, Ataei F: The relation of body mass index and blood pressure in Iranian children and adolescents aged 7–18 years old. Iran J Public Health 2010, 39(4):126.
Salem Z, Vazirinejad R: Prevalence of the metabolic syndrome components among 7–11 year-old children in Rafsanjan, 2008. Iran J Nutri Sci Food Technol 2010, 5(2):63–71.
Pourghassem Gargari B, Hamed Behzad M, Seied Sajadi N, Kooshavar D, Karami S: Relation of Body Mass Index to Eating Attitude in Tabrizian High School Girls. Med J Tabriz Univer Med Sci Health Service 2010, 32(3):24–29.
Mohammadian S, Khoddam H, Kaveh M: Related factors of obesity and overweight among secondary school girls (Gorgan-Iran). J Gorgan Univer Med Sci 2010, 12(3):57–62.
Maddah M: Association of parental diabetes with overweight in Iranian children and adolescents. Int J Cardiol 2010, 144(1):126–128.
Vafa M, Afshari , Moslehi N, Salehpoor A, Hosaini F, Goharinezhad M, Zarif Yeganeh M, Hosaini S: Relationship Between Infant Nutrition Feeding and Childhood Obesity in First Grade Tehranian Students of Primary Schools, 2009. Iranian J Endocrinol Metab 2011, 12(5):505–512.
Dahri M, Safaria M, Hajifaraji M, Houshiar Rad A, Abadi A: The Association of Overweight and Obesity with Menarche Age and Nutritional Status in Girls Aged 11–15 in Mashhad. Med J Mashhad Univer Med Sci 2011, 53(4):245–253.
Maddah M, Shahraki T, Shahraki M: Underweight and overweight among children in Zahedan, south-east Iran. Public Health Nutr 2010, 13(10):1519–1521.
Ziaoddini H, Kelishadi R, Kamsari F, Mirmoghtadaee P, Poursafa P: First nationwide survey of prevalence of weight disorders in Iranian children at school entry. World J Pediatr 2010, 6(3):223–227.
Ahmadi S, Shahsavari S, Ahmadi H, Tabatabaeifar T: Prevalence of Overweight, Obesity and Underweight Among High School Students in Sanandaj: 2006–2007. Iran J Endocrinol Metabol 2010, 12(2):153–159.
Bazhan M, Kalantari N, Hoshyarrad A: Diet composition and risk of overweight and obesity in Iranian adolescent girls. RMJ 2011, 36(1):26–30.
Hosseini Kakhk SAR, Safari M, Hamedinia M: Health-Related Factors in Physical Fitness in 12–14 Year-old Male Adolescents in Sabzevar. Iran 2 2011, 18(1):55–66.
Mohkam M, Karimi A, Eslami N, Khatami A, Fallah F, Maham S, Jadali F, Abdollah Gorji F: Blood pressure screening in school-aged children in Tehran. Iran J Kidney Diseases 2011, 5(4):229–233.
Mirzaeian S, Fakhari M, Hassanzadeh AAE: Association between duration of breast feeding and subsequent overweight and obesity in female adolescents. Iranian J Nutri Sci Food Technol 2011, 6(2):65–74.
Hajian-Tilaki K, Sajjadi P, Razavi A: Prevalence of overweight and obesity and associated risk factors in urban primary-school children in Babol, Islamic Republic of Iran. East Mediterr Health J 2011, 17(2):109–114.
Alvani SR, Alvani S: The effect of obesity on self-esteem among pre university Iranian students in Kashan city of Iran April 2009. Eur J Soc Sci 2011, 24(1):48–54.
Gaeini A, Kashef M, Samadi A, Fallahi A: Prevalence of underweight, overweight and obesity in preschool children of Tehran, Iran. J Res Med Sci 2011, 16(6):821.
Veghari G: Related Factors among Iranian Northern School Children. J Biol Sci 2011, 11(8):487–491.
Mirmohammadi S-J, Hafezi R, Mehrparvar AH, Rezaeian B, Akbari H: Prevalence of overweight and obesity among Iranian school children in different ethnicities. Iran J Pediatr 2011, 21(4):514.
Taheri F, Zangoie M, Kazemi T, Zangoi Fard M, Movahed Fazel M: Prevalence of overweight and obesity in 11–15 years old (mid-school) students in Birjand, 2005. Modern Care (Scientific Quarterly of Birjand Nursing & Midwifery Faculty 2011, 8(2):58–64.
Zareei M, Hamedi Nia M, Haghighi A, Chamri M, Beroghani M: The epidemiology of overweight and obesity and their association with physical activity and dietary patterns in adolescents aged 12–14 in Sabzevar. J Iran Institute Health Sci Res 2011, 10(2):243–253.
Kajbaf TZ, Asar S, Alipoor MR: Relationship between obesity and asthma symptoms among children in Ahvaz, Iran: a cross sectional study. Ital J Pediatr 2011, 37(1):1.
Azarbayjani MA, Tojari F, Habibinejad M: The relation between obesity, physical activity and socioeconomic status among girl students living in northern Tehran. KAUMS J (FEYZ) 2011, 15(2):132–138.
Moghadasi M, Naser K, Ghanbarzadeh M, Shakerian S, Razavi A: Prevalence of Overweight, Obesity and Physical Fitness in Shiraz Adolescents. Iran J Endocrinol Metabol 2011, 12(5):476–482.
Asadi Noghabi F: Prevalence of obesity and overweight among children in Bandar Abbas. Bimonthly J Hormozgan Univer Med Sci 2011, 15(3):218–226.
Mirzaei M, Karimi M: Prevalence of Overweight And Obesity Among The First Grade Primary Students in Yazd. J Ilam Univer Med Sci 2011, 18(4):43–49.
Amanollahi A, Sohrabi M, Montazeri A, Abadi A, Kolahi A: Prevalence of owerweight and obesity among primary school girls. J Iran Institute Health Sci Res 2011, 11(1):89–95.
Nouhjah S, Karandish M, Malihi R, Tamadon F: Prevalence of overweight and obesity in 2–5 years children based on new WHO growth standards in Ahwaz. Iran J Jentashapir 2011, 2(2):62–68.
Ghergherechi R, Shoari N: Age of puberty and its association with body mass index among girls in Tabriz. J Tabriz Univer Med Sci 2011, 33(2):63–68.
Mozaffari-Khosravi H, Hosseinzadeh-Shamsi-Anar M, Shariati Bafghi SE, Mozaffari-Khosravi V: Prevalence of Eating Disorders and Obesity in High School Girl Students in Yazd, 2010–2011. J Tolo-e-Behdasht 2011, 10(1):38–49.
Behzadnia S, Vahidshahi K, Hosseini SH, Anvari S, Ehteshami S: Obesity and related factors in 7–12 year-old elementary school students during 2009–2010 in Sari. Med Glas, Iran; 2011.
Ebrahimzadehkoor B, Kalantary N, Kabir MJ: Abadi AR Correlation between obesity, exclusively breast feeding and breast feeding duration among infants, Bandar Turkmen district Northern, Iran. J Gorgan Univer Med Sci 2011, 13(2):107–111.
Vafa M, Moslehi N, Afshari S, Hossini A, Eshraghian M: Relationship between breastfeeding and obesity in childhood. J Health Popul Nutr 2012, 30(3):303.
Mohamadpour Koldeh M, Fouladvand MA, Avakh KM: Prevalence of overweight and obesity among Bushehrian high-school girls at aged 14–17 years old. Iran South Med J 2012, 15(3):221–232.
Ebrahimzadeh B, Kalantari N, Abadi A: The prevalence of obesity and its relative factors among less than 5 years aged children, Bandar Turkmen district, Iran. J Kerman Univer Med Sci 2012, 19(4):384–391.
Mehrkash M, Kelishadi R, Mohammadian S, Mousavinasab F, Qorbani M, Hashemi MEF, Asayesh H, Poursafa P, Shafa N: Obesity and metabolic syndrome among a representative sample of Iranian adolescents. Southeast Asian J Tropical Med Public Health 2012, 43(3):756.
Aazami M, Akbari M, Heshmati B, Alikhani M: The Growth Pattern among Elementary School Students in Kermanshah. Iran J Isfahan Med School 2012, 30(181):313.
Doustmohammadian A, Abdollahi M, Bondarianzadeh D, Houshiarrad A, Abtahi M: Parental determinants of overweight and obesity in Iranian adolescents: a national study. Iran J Pediatr 2012, 22(1):35.
Fatemeh T, Hassanzadeh-Taheri M-M, Kazemi T, Afsaneh N, Sharifzadeh G: Prevalence of overweight and obesity in preschool children (2–5 year-olds) in Birjand, Iran. BMC Res Notes 2012, 5(1):529.
Hajian-Tilaki K, Heidari B: Prevalences of overweight and obesity and their association with physical activity pattern among Iranian adolescents aged 12–17 years. Public Health Nutr 2012, 15(12):2246–2252.
Khodaverdi F, Bahram A, Jafarabadi MA: Quality of life, motor ability, and weight status among school-aged children of Tehran. Iran J Public Health 2012, 41(6):97.
Esmaeilzadeh S, Ebadollahzadeh K: Physical fitness, physical activity and sedentary activities of 7 to 11 year old boys with different body mass indexes. Asian J Sports Med 2012, 3(2):105.
Zakeri M, Sedaghat M, Motlagh ME, Ashtiani RT, Ardalan G: BMI correlation with psychiatric problems among 10–18 years Iranian students. Acta Med Iran 2012, 50(3):177–184.
Basiratnia M, Derakhshan D, Ajdari S, Saki F: Prevalence of childhood obesity and hypertension in south of Iran. Iran J Kidney Dis 2013, 7(4):282–289.
Ghavamzadeh S, Khalkhali HR, Alizadeh M: M. TV Viewing, Independent of Physical Activity and Obesogenic Foods, Increases Overweight and Obesity in Adolescents. J Health Popul Nutr 2013, 31(3):334.
Hajian-Tilaki K, Heidari B: Childhood Obesity, Overweight, Socio-Demographic and Life Style Determinants among Preschool Children in Babol, North¬ ern Iran. Iran J Public Health 2013, 42(11):1283–1291.
Taheri F, Kazemi T, Chahkandi T, Namakin K, Zardast M, Bijari B: Prevalence of overweight, obesity and central obesity among elementary school children in Birjand, East of Iran, 2012. J Res Health Sci 2013, 13(2):157–161.
Salehi-Abargouei A, Abdollahzad H, Bameri Z, Esmaillzadeh A: Underweight, overweight and obesity among Zaboli adolescents: a comparison between international and Iranians’ national criteria. Intern J Preventive Med 2013, 4(5):523.
Mirzaeian S, Esmaillzadeh A, Rashidkhani B: Association Between Nuts Consumption and Abdominal Obesity, Overweight and Obesity in Female Adolescents: An Epidemiological Study. Iran J Endocrinol Metabol 2013, 15(3):244–252.
Patricia K, Ramin H, Qorbani M, Mostafa M, Esmaeil M, Aminaee T, Ardalan G, Farrokhi-Khajeh-Pasha Y, Taslimi M, Larijani B, Kelishadi R: Metabolic syndrome and cardiovascular risk factors in a national sample of adolescent population in the middle east and north Africa: the CASPIAN III study. Int J Endocrinol 2013, 2013: 8. doi.org/10.1155/2013/702095
Kelishadi R, Ardalan G, Qorbani M, Ataie-Jafari A, Bahreynian M, Taslimi M, Esmaeili Motlagh M, Heshmat R: Methodology and early findings of the fourth survey of childhood and adolescence surveillance and prevention of adult non-communicable disease in Iran: The CASPIAN-IV study. Intern J Preventive Med 2013, 4(12):1451–1460.
Author information
Authors and Affiliations
Corresponding author
Additional information
Competing interests
The authors declare that they have no competing interests.
Authors’ contributions
All authors read and approved the final manuscript.
Electronic supplementary material
Authors’ original submitted files for images
Below are the links to the authors’ original submitted files for images.
Rights and permissions
This article is published under license to BioMed Central Ltd. This is an Open Access article distributed under the terms of the Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly credited. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

{kind=link}
Cite this article
Jafari-Adli, S., Jouyandeh, Z., Qorbani, M. et al. Prevalence of obesity and overweight in adults and children in Iran; a systematic review. J Diabetes Metab Disord 13, 121 (2014). https://doi.org/10.1186/s40200-014-0121-2
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s40200-014-0121-2