





Energy homeostasis and medical vs. surgical methods to overcome it
Obesity is now a global pandemic that continues to accelerate despite the often Herculean efforts by afflicted individuals to lose weight. These efforts are thwarted by a physiological system that regulates body weight in a manner analogous to that by which a thermostat controls ambient temperature. For each individual, there is a highly genetically influenced level of adiposity that is defended by this adipostatic control system, wherein alterations in body fat stores trigger compensatory changes in appetite and energy expenditure that resist weight change (1). It is hypothesized that these processes evolved to defend against malnutrition in times of famine, and hence, the adaptive responses to weight loss appear to be more robust than are those to weight gain (as any dieter can attest). Because of this body weight regulation system, known as energy homeostasis, nonsurgical methods are notoriously ineffective at achieving major, long-term weight reduction. In general, no more than 5–10% of body weight is lost through dieting, exercise, and the few available antiobesity medications, and recidivism after dietary weight reduction is nearly universal (2–5). Importantly, even mild weight loss confers disproportionate health benefits, in terms of ameliorating obesity-related comorbidities (6). Nevertheless, more substantial and durable weight reduction would improve these ailments even more effectively, as well as lessen the stigmatization and emotional suffering often endured by obese individuals.
At present, bariatric surgery is the most effective method to achieve major, long-term weight loss (7, 8). The best operations reduce body weight by 35–40%, and most of this effect is maintained for at least 15 yr (Refs.7–10 ; and Pories, W. J., personal communication). Postsurgical weight loss improves all obesity-related comorbidities examined to date, including diabetes, hypertension, dyslipidemias, nonalcoholic steatohepatitis, sleep apnea and obesity-hypoventilation syndrome, cardiac dysfunction, reflux esophagitis, pseudotumor cerebri, arthritis, infertility, stress incontinence, and venous stasis ulcers (4, 8, 9). The net effect is an increase in quality of life and decrease in overall mortality (11, 12). Estimates of the cost of bariatric surgery per quality-adjusted life year (QALY) range from $5,400 to $36,600/QALY, well under the $50,000/QALY benchmark that is generally regarded in the United States as being cost effective (13, 14). Unquestionably, obesity surgery is a drastic approach that is not without risks; but these are usually outweighed by the risks of morbid obesity, especially when considering the most modern and increasingly safe bariatric operations. Among these, Roux-en-Y gastric bypass (RYGB) appears to offer the best balance of effectiveness vs. risk, and it is the most widely used surgery for morbidly obese people in the United States (15). Not surprisingly, massive weight loss after this procedure reduces obesity-related comorbidities and mortality; but the operation may improve glucose homeostasis through physiological changes not explained by weight loss alone (16).
The mechanisms underlying the effects of RYGB on body weight and glucose metabolism are incompletely understood. Elucidating these mechanisms is a high priority, because such knowledge may facilitate the development of novel antiobesity medications that could achieve at least some of the weight loss caused by RYGB, without surgical risks. Here, we examine the known and hypothesized mechanisms mediating the effects of RYGB, hopefully highlighting avenues for future research to help uncover the secrets of this intriguing operation.
The spectrum of bariatric surgery
Intestinal malabsorption and gastric restriction are the two most obvious mechanisms to explain weight loss after bariatric surgery, and the types of operations are traditionally categorized based on which of these changes they induce (Figs. 1 and 22). Malabsorptive procedures reconstruct the small intestine to reduce the area of mucosa available for nutrient absorption. The earliest incarnation of this strategy was the jejunoileal bypass (JIB) (17). Imposing no restriction on the flow of food, this procedure simply diverted enteral nutrients around most of the small intestine, via an anastomosis between the proximal jejunum (∼14 in. from the ligament of Treitz) and the terminal ileum (∼4 in. from the cecum; Fig. 1A). Weight loss was impressive, but the operation was plagued with complications that ultimately led to its abandonment from clinical practice. These included oxalate nephrolithiasis, protein malnutrition, metabolic bone disease, hypocalcemia, arthritis, and deficiencies of vitamins B12 and D (8). The most serious morbidity of JIB was hepatic cirrhosis, hypothesized to result from bacterial overgrowth in the blind-loop intestinal segment, leading to chronic hepatic inflammation from foreign antigens in portal blood. The procedure was succeeded by the biliopancreatic diversion (BPD), with or without a duodenal switch (Fig. 1, B and C). These operations are also malabsorptive but create no blind intestinal loops. Malabsorption occurs because pancreatic and biliary secretions are diverted to the distal approximately 50 cm of the ileum. Thus, most of the small intestine contains either digestive juices without food or food without digestive juices, and absorption is limited to the terminal ileum where these two are briefly combined in a common channel. Although BPD promotes durable weight loss as effectively as any bariatric procedure (7), it often causes significant complications, including protein malnutrition, hypocalcemia and metabolic bone disease, foul-smelling diarrhea, and deficiencies of iron, vitamin B12, and fat-soluble vitamins (8). Consequently, most American surgeons are reluctant to perform this operation, and it is generally reserved for the superobese [body mass index (BMI) > 50 kg/m2].
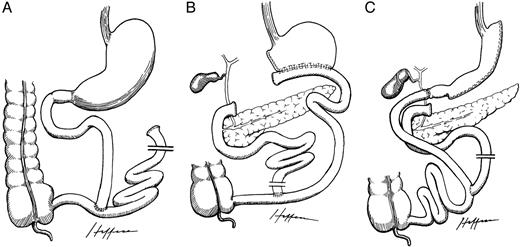
Malabsorptive bariatric operations. A, Jejunoileal bypass; B, biliopancreatic diversion; C, duodenal switch. Drawings rendered by Dr. Alejandro Heffess and generously provided by Edward C. Mun.
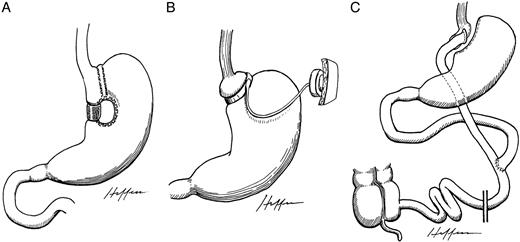
Restrictive bariatric operations. A, Vertical banded gastroplasty; B, adjustable gastric banding; C, Roux-en-Y gastric bypass. Drawings were rendered by Dr. Alejandro Heffess and generously provided by Edward C. Mun.
Purely restrictive bariatric operations cause weight loss by limiting the capacity of the stomach to accommodate food and constricting the flow of ingested nutrients. Gastroplasty, commonly dubbed “stomach stapling,” is the original exemplar. This procedure initially involved placing a horizontal staple line to partition the stomach into a small, proximal pouch and large distal remnant, connected to one another via a narrow stoma (18). The operation often failed due to dilation of the stoma and/or proximal pouch, or dehiscence of the horizontal gastroplasty. To avoid these problems, Mason (19) modified the operation into the vertical banded gastroplasty (VBG), in which the partitioning line extends upward from the angle of His (to exclude the easily dilatable fundus), and a polypropylene mesh band reinforces the stoma (Fig. 2A). Although VBG effectively limits the amount of food that can be consumed at one sitting and causes 30–50% reduction of excess body weight within the first 1–2 yr, long-term results are disappointing (8). Patients often accommodate to gastric restriction by eating frequent, small meals and calorie-dense foods, such as milkshakes (7). A nearly 80% failure rate has been reported after 10 yr (20), and randomized, prospective as well as sequential, comparative studies consistently show that RYGB is more effective than VGB at inducing and maintaining weight loss (21–25). Consequently, VBG has fallen out of favor (7, 10).
Adjustable gastric banding (AGB) is an increasingly popular, purely restrictive bariatric procedure used extensively worldwide and approved by the U.S. Food and Drug Administration in 2001 for use in the United States (Fig. 2B). Essentially an adjustable variant of VBG, this approach involves placement of a prosthetic band around the upper stomach to partition it into a small, proximal pouch and a large, distal remnant, connected through a narrow constriction (26, 27). Free of anastomoses, this approach eliminates the possibility of staple-line dehiscence and is readily accomplished laparoscopically. Moreover, the band aperture can be modified noninvasively as needed. Risks include band slippage or erosion into the stomach and reflux esophagitis. Weight loss after gastric banding is usually less than that expected from RYGB, but short- and long-term complications are also less frequent (7).
The modern RYGB is the result of several improvements on a gastric bypass operation first developed in 1969 by Mason (28), who had observed that postgastrectomy patients with a small residual gastric remnant experienced substantial weight loss. The stomach is divided into a small, proximal pouch and a separate, large, distal remnant. The upper pouch is joined to the proximal jejunum through a narrow gastrojejunal anastomosis (Roux-en-Y configuration, Fig. 2C). Thus, storage capacity of the stomach is reduced to approximately 5% of its normal volume, and ingested food bypasses approximately 95% of the stomach, the entire duodenum, and a small portion (15–20 cm) of the proximal jejunum. The results are impressive. Patients typically lose 35–40% of total body weight, and most of this effect is maintained for at least 15 yr (Refs.7–10 ; and Pories, W. J., personal communication). As expected, such massive weight loss ameliorates all obesity-related morbidities, most impressively diabetes (vide infra) (9). Perioperative mortality, largely from pulmonary embolism or sepsis, is typically reported as approximately 1% in the literature (4) but may be more in the hands of less experienced surgeons. Postoperative complications occur in approximately 10% of cases and include deep venous thrombosis, anastomotic leaks, internal hernias, gastrointestinal bleeding, ulcers in the bypassed segments, torsion or volvulus of the roux limb, closed loop obstruction, stomal stenosis, wound complications, staple-line disruption, and gallstone formation with rapid weight loss (7–9). Bypassing of the stomach and duodenum impairs absorption of iron, calcium, thiamine, and vitamin B12; thus, supplements of these micronutrients and periodic monitoring for deficiencies are required. The increasingly common use of laparoscopic RYGB should lessen surgical complications overall. Operative risk is measured against the medical benefits of massive weight loss. In a study with a mean 9-yr follow-up, overall annual mortality was reduced to 1.0% among 154 patients who underwent RYGB, compared with 4.5% among 78 morbidly obese people referred for RYGB who did not undergo the operation for personal reasons (P < 0.001) (16, 29). In 1991, a National Institutes of Health (NIH) Consensus Development Panel endorsed only VBG, gastric banding, and RYGB (15), and the last of these has emerged as the gold standard (30). The panel recommended that surgical treatment be considered for people with a BMI of 40 kg/m2 or greater and for those with a BMI of at least 35 kg/m2 plus serious comorbidities. Based on recommendations from a panel of experts that convened in May 2004, a new consensus statement is being developed by the American Society for Bariatric Surgery and other organizations dedicated to the treatment of morbid obesity.
Mechanisms of weight loss after Roux-en-Y gastric bypass
Although the mechanisms causing weight loss after purely malabsorptive or restrictive bariatric operations are apparent, less obvious physiological changes may also contribute to the profound impact of RYGB on body weight and glucose homeostasis. Unquestionably, gastric restriction plays a role. Because of reduced gastric capacity, post-RYGB patients experience early satiety and, consequently, eat smaller meals (31, 32). If this were the only mechanism at work, however, the energy homeostasis system would drive patients to compensate with increased meal frequency and to favor calorie-dense foods in response to massive weight loss. Instead, people who have undergone gastric bypass typically eat fewer meals and snacks per day (32, 33). They also voluntarily restrict consumption of calorie-dense foods, such as fats, concentrated carbohydrates, ice cream, and sweetened beverages (32, 33). Presumably because of these changes in eating behavior, RYGB is more effective than VBG, although the degree of gastric restriction (i.e. proximal pouch volume and stomal aperture) is at least as great after VBG as after RYGB (34). In several randomized, prospective trials, RYGB has caused 50–80% loss of excess body weight, as opposed to only 30–50% after the equally restrictive VBG (21–25). Moreover, weight loss after RYGB is considerably more durable than that after VBG.
The two mechanisms cited most often to explain the greater efficacy of RYGB over VBG are malabsorption and dumping syndrome. However, clinically significant malabsorption, measured by indices such as albumin, prealbumin, and fecal fat, is not observed after the standard proximal RYGB (7, 35–37). Moreover, randomized, prospective trials show that weight loss after RYGB is comparable to that after the radical, malabsorptive JIB (Fig. 1A) (38, 39), although only approximately 3 ft of small intestine is bypassed with RYGB, compared with 12–18 ft with JIB (34). Dumping symptoms (nausea, bloating, colic, diarrhea, lightheadedness, diaphoresis, and palpitations) occur in some patients, typically after high-carbohydrate meals. Although these can promote a negative conditioning response to sweets that may contribute to weight loss in selected individuals, the severity of dumping correlates poorly with the efficacy of RYGB, and it is unlikely that dumping plays a major role in weight loss overall.
In our opinion, RYGB is more effective than VBG primarily because of the profound loss of appetite that typically results from RYGB but is less consistent after VBG (7). This decrease in hunger is not explained by early satiety from gastric restriction alone, because it extends well beyond the immediate postprandial period. Moreover, it occurs despite a lack of change in the perception of sweets as being delicious or in the overall enjoyment of food (11, 32, 40). Levels of the two most well-established adiposity hormones, leptin and insulin (1), decrease appropriately after RYGB (41, 42), as expected with weight loss. Thus, these hormones do not account for the reduction in hunger and the regulation of body weight at a new, reduced level. Alterations in gut hormones have long been hypothesized to mediate these effects, but those initially examined, cholecystokinin, serotonin, and vasoactive intestinal peptide, are unaffected by gastric bypass (43, 44).
In 2002, we published a report suggesting that impairment of ghrelin secretion might account, in part, for the loss of hunger that accompanies RYGB, potentially contributing to weight loss (45). Ghrelin is an enteric peptide hormone that is the only known circulating orexigen (appetite stimulant) (46–49). Endogenous levels increase before meals and decrease after food intake in humans and other species, both among individuals fed on a fixed schedule and in those initiating meals voluntarily in the absence of cues related to time or food (25, 50, 51). These and other findings support the hypothesis that ghrelin stimulates mealtime hunger and contributes to meal initiation. Other data also implicate ghrelin in long-term body weight regulation, a potential orexigenic counterpart to leptin (25). Among the evidence supporting this role is the observation that ghrelin levels increase with weight loss resulting from numerous causes, including caloric restriction, cancer anorexia, exercise, eating disorders, and chronic failure of the heart, liver, or kidneys (25, 45). The implication is that an increase in ghrelin levels may constitute one of the adaptive responses to weight loss that characterizes long-term energy homeostasis.
Ghrelin is produced principally by the stomach and, to a lesser extent, the duodenum, the areas affected by RYGB (52). Because ingested nutrients are dominant regulators of ghrelin production and because the majority of ghrelin-producing tissue is permanently excluded from contact with ingested nutrients after RYGB, we hypothesized that RYGB disrupts ghrelin regulation. In a study examining 24-h ghrelin profiles, we found that among people who had undergone RYGB 1.4 ± 0.4 yr earlier, integrated area-under-the-curve ghrelin values were 77% lower than those of lean controls and 72% lower than those of matched-obese controls (45). These low ghrelin levels were especially remarkable in view of the 36% weight loss that had been experienced by the RYGB group, a change that would stimulate ghrelin if achieved by other means. Moreover, the 24-h profiles of post-RYGB individuals were completely flat, displaying neither the prandial oscillations nor diurnal rhythm characteristic of normal ghrelin profiles.
Following this publication, numerous other groups examined the effect on ghrelin of RYGB, as performed at their centers, and we are aware of 11 reports on this topic. Three prospective studies found that ghrelin levels decreased after RYGB, despite massive weight loss (53–55). Three others, including our own, reported abnormally low levels of ghrelin in post-RYGB patients, compared with matched-obese controls (45, 56, 57). Four additional prospective studies found no change in ghrelin levels after RYGB despite massive weight loss, an observation interpreted as reflecting an impairment of the normal response of ghrelin to weight loss (42, 58–60). Finally, one group reported that ghrelin levels increased after RYGB, as expected with other modes of weight loss (61). Although the last study is an outlier, in many ways it is the best investigation of this topic to date, with the largest number of subjects and a prospective design. The implication of this heterogeneity is that there may be subtle differences in surgical technique that lead to suppression or at least constraint of ghrelin levels after RYGB, in many but not all surgeons’ hands. If it is ultimately proven that impairment of the ghrelin response to weight loss contributes to the long-lasting efficacy of RYGB, it will be important to elucidate the mechanisms by which this occurs, so that the effect can be sought expressly.
Our initial hypothesis was that RYGB suppresses ghrelin secretion through a process known as “override inhibition” (45). This is a phenomenon in which hormones that are normally secreted in response to an episodic stimulus are paradoxically inhibited when that stimulus occurs continuously. By this mechanism, gonadotropins and GH are paradoxically suppressed by continuous delivery of their normally pulsatile secretagogues, GnRH and GHRH, respectively (62, 63). In the case of ghrelin, the normal stimulus would be an empty stomach and duodenum, a condition that is rendered permanent by RYGB. The possibility that ghrelin-producing cells in the gut are subject to override inhibition is suggested by several lines of evidence that we have summarized elsewhere (25). The override inhibition hypothesis predicts that bariatric procedures that do not exclude the majority of ghrelin-producing tissue (i.e. the gastric fundus) from contact with enteral nutrients would not impair ghrelin secretion. Consistent with this prediction, weight loss achieved by AGB or BPD is associated with either unchanged or increased ghrelin levels in longitudinal studies (Cummings, D. E., and K. Clément, unpublished observations; and Refs.42 , 54 , 64 , 65).
The override inhibition hypothesis, if valid, has clinical implications for surgical design (66). According to this model, the position of the staple line partitioning the stomach in RYGB could be a critical determinant of weight loss. Placing this partition even slightly too far to the left would include part of the fundus—the richest source of ghrelin—in the upper gastric pouch, thus failing to exclude it from contact with food and undermining override inhibition. It is conceivable that this physiology contributes to the lesser efficacy of horizontal- than vertical-banded gastric bypasses (8). Similarly, a short biliopancreatic limb (between the distal gastric remnant and the jejunojejunal anastomosis) could allow reflux of ingested nutrients from the Roux anastomosis into the ghrelin-rich stomach and duodenum. Interestingly, in the one published study that did not find an impaired ghrelin response to weight loss (61), patients had among the shortest biliopancreatic limbs and the widest upper gastric pouches of RYGB patients examined in ghrelin investigations to date (66). That study also reported less weight loss (29.7%) than is typically seen after RYGB (35–40%) and less than was reported in most other studies of RYGB and ghrelin (66).
Doubt is cast on the override inhibition hypothesis, however, by our recent rat experiments designed to locate the putative sensor that detects ingested nutrients and suppresses ghrelin levels in response to them. Unexpectedly, we and our colleagues in the laboratory of Drs. Harvey Grill and Joel Kaplan found that nutrients infused into the stomach and constrained there with a reversible pyloric cuff did not affect ghrelin levels, which were significantly suppressed when the cuff was opened (67). Moreover, nutrients infused into the proximal jejunum suppressed ghrelin as well as did those infused into either the stomach or proximal duodenum (68). In other words, prandial ghrelin regulation does not require the presence of nutrients in either the stomach or duodenum, the principal sites of ghrelin production. Thus, it seems less likely that exclusion of ingested nutrients from these areas after RYGB would disrupt ghrelin regulation. An alternate hypothesis is that ghrelin regulation is perturbed after RYGB because of denervation of autonomic input to ghrelin-producing tissue in the foregut. We found in rats that vagotomy eliminated the normal response of ghrelin to weight loss, as is often observed after RYGB (69). Severing of vagal input to the foregut is accomplished variably by different surgeons performing RYGB, so this hypothesis could explain some of the heterogeneity in data pertaining to the effect of this operation on ghrelin levels (66). A neural mechanism might also explain the very rapid decline in ghrelin levels that was recently observed within 24 h of the operation, before suppression via override inhibition from an empty stomach and duodenum would be predicted to occur (54).
Antidiabetic effects of gastric bypass
The obesity-related comorbidity most dramatically ameliorated by RYGB is type 2 diabetes mellitus (DM). In five published studies examining a total of 3568 people undergoing RYGB, diabetic patients enjoyed complete remission of their disease at rates ranging from 82–98%, with most studies showing resolution in approximately 83% of cases (9, 70–73). The reversal of impaired glucose tolerance without DM was nearly universal. Patients whose DM remitted were able to discontinue all diabetic medications and manifest normal fasting glucose and glycosylated hemoglobin levels. In a longitudinal study of obese people with impaired glucose tolerance followed for approximately 5.5 yr, bariatric surgery lowered the rate of progression to DM by more than 30-fold (74). Thus, RYGB is a highly effective method to reverse DM, which is traditionally regarded as a progressive, unrelenting disease. The most obvious mechanism to explain this effect is the beneficial impact of weight loss on insulin sensitivity. Indeed, patients who have lost substantial weight after RYGB display increased levels of adiponectin (which increases insulin sensitivity) and muscle insulin-receptor concentration, as well as reductions in intramuscular lipids and fatty acyl-coenzyme A molecules (moieties that cause insulin resistance) (75–77). As predicted, insulin sensitivity, measured by minimal modeling, is increased approximately 4- to 5-fold after RYGB-induced weight loss (75, 77). The beneficial effects of RYGB on DM, however, cannot be accounted for by weight loss alone. Perhaps the most impressive observation is that previously diabetic patients typically discontinue all of their DM medications at the time of discharge from the hospital after RYGB (∼1 wk), long before major weight loss has occurred (16, 70).
What mechanisms could explain this dramatic, rapid reversal of DM? The most pedestrian (although quite possibly valid) is that patients consume no food in the immediate postoperative period, so their pancreatic β-cells are not challenged. Starvation-induced alleviation of DM is well known. A few days later, patients gradually escalate their oral intake; but by the time they begin to eat reasonably normally at home, they are losing weight and in a state of negative energy balance, a condition that improves glucose tolerance. Eventually, amelioration of DM can be accounted for by the well-known effect of weight loss to increase insulin sensitivity, thereby decreasing glucotoxicity and lipotoxicity and improving β-cell function.
A more interesting possibility, which may act in concert with the above mechanism, is that favorable alterations in gut hormone release after RYGB improve insulin secretion and/or action. Ghrelin, which may decrease after this operation, exerts several diabetogenic effects. Exogenous injections in humans increase levels of GH, cortisol, and epinephrine, three of the four classical counterregulatory hormones (25). Ghrelin administration also suppresses insulin levels in humans, even in the face of ghrelin-induced hyperglycemia (78). Finally, ghrelin directly antagonizes insulin-mediated intracellular signaling events pertaining to glucose metabolism in cultured hepatocytes (79). Thus, at least at pharmacological doses, ghrelin hinders insulin secretion and action, and chronic administration of ghrelin receptor agonists impairs glucose tolerance in humans (80). If these effects are physiological and ghrelin acts as an anti-incretin to limit peripheral glucose utilization in the fasted and preprandial state, then suppression of ghrelin levels after RYGB could enhance glucose disposal.
An even more attractive candidate mediator of the antidiabetic effects of RYGB is glucagon-like peptide-1 (GLP-1). This hormone and glucose-dependent insulinotropic peptide (GIP) are the classical incretins that stimulate insulin secretion in response to enteral nutrients. Furthermore, GLP-1 exerts proliferative and antiapoptotic effects on pancreatic β-cells (81). It may also improve insulin sensitivity, at least indirectly (82). Accordingly, methods to enhance GLP-1 signaling show great promise for the treatment of type 2 DM (83). Moreover, GLP-1 inhibits gastric emptying and can decrease food intake (83). GLP-1 is secreted primarily by the hindgut after food ingestion, and part of this response results from direct contact between enteral nutrients and the intestinal L cells that produce GLP-1. After RYGB, ingested nutrients reach the hindgut more readily, bypassing part of the foregut and unimpeded by the pylorus. The larger postprandial bolus of nutrients in the hindgut should increase GLP-1 levels after RYGB. Although reports of the effect of this operation on GLP-1 are not published, several studies of JIB, which also expedites nutrient delivery to the hindgut, show increased GLP-1 levels after surgery, both within the first year and as late as 20 yr postoperatively (84–86). Biliopancreatic diversion creates a similar shortcut to the ileum; this operation also increases hormone secretion from L cells and is at least as effective as RYGB at ameliorating DM (87).
Secretion of other hindgut hormones, if similarly enhanced after RYGB, could also contribute to the effects of this procedure on glucose homeostasis and energy balance. Recently, peptide YY3–36 (PYY) was shown to decrease food intake in humans and body weight in rodents (88, 89). Because this, too, is primarily a hindgut hormone, its levels, especially postprandial, should increase after RYGB, an effect that might contribute to weight loss. Fasting and postprandial PYY levels do increase after other surgeries that expedite nutrient delivery to the hindgut, including extensive small-bowel resection (90) and JIB (9 months and 20 yr postoperatively) (84, 86). As predicted, unpublished studies indicate that postprandial PYY levels are also markedly elevated after RYGB (Bloom, S. R., personal communication).
Roles of the foregut and hindgut in the effects of gastric bypass
Although all bariatric operations promote weight loss and improve glucose homeostasis, gastric bypass and BPD are the fastest and most effective procedures for both endpoints (70, 91, 92). Both operations cause durable remissions of DM in more than 80% of cases, typically within a few days after surgery (9, 41, 92, 93). Because these two procedures exclude the intestinal foregut from digestive continuity, whereas other bariatric operations do not, it has been hypothesized that bypass of this hormonally active region is an important determinant of the effects of bariatric surgery (41, 91). As articulated above, suppression or constraint of ghrelin secretion from the bypassed foregut is one candidate mechanism to explain some of the effects of RYGB on weight loss and glucose homeostasis. To integrate extant ghrelin data into the foregut hypothesis, one would predict that standard BPD, which leaves the ghrelin-rich gastric fundus in digestive continuity, would not significantly impair ghrelin secretion, whereas the duodenal switch, in which most ghrelin-producing tissue is either resected or bypassed, would suppress ghrelin levels (Fig. 1).
A very recent, elegant study by Rubino and Marescaux (94) provides additional data supporting the foregut hypothesis. Using Goto-Kakizaki rats, a spontaneous, nonobese model of type 2 DM, these investigators isolated the effects of RYGB that are related to exclusion of the duodenum and proximal jejunum from those related to gastric restriction and bypass. The stomach was left unperturbed, but food was diverted from the pyloric area to the proximal jejunum with a gastrojejunal anastomosis. This gastrojejunal bypass (GJB) represents a stomach-sparing bypass of approximately the same amount of intestinal foregut as is excluded in RYGB. (The entire duodenum was bypassed. Of the jejunum, 12 cm was included in the Roux limb and 8 cm in the biliopancreatic limb. Thus, 20 cm of jejunum was incapable of absorbing nutrients, i.e. approximately 20% of the approximately 100-cm-long rat jejunum.) Experimental animals displayed similar food intake and body weight as did sham-operated controls, indicating that foregut bypass alone is not sufficient to cause weight loss. This is not surprising, because the GJB creates no gastric restriction, leaves most ghrelin-producing tissue in digestive continuity, and does not involve a vagotomy. The results support assertions made above that malabsorption after foregut bypass (as in RYGB) is unlikely to be a major contributor to weight loss. The most interesting finding in this study was that GJB rats showed significant improvement in glucose tolerance compared with sham-operated controls, despite equivalent body weights in the two groups. Compared with controls, bypassed animals had lower fasting glucose levels at all postoperative time points for 9 months; a lower glucose nadir after insulin injection; and lower area-under-the-curve glucose values in response to an oral glucose load at 1, 2, and 32 wk after surgery. The GJB resulted in better glycemic control than did either rosiglitazone therapy or substantial weight loss from food restriction. The implication of these findings is that bypass of the intestinal foregut (e.g. as accomplished by RYGB and BPD) can ameliorate type 2 DM independently of weight loss, through mechanisms that remain unclear. The authors hypothesize alterations in gut hormones, but candidate molecules are not obvious. The incretin hormone, GIP, produced primarily by the foregut, is stimulated by ingested nutrients and promotes insulin secretion. Bypass of the foregut should, theoretically, decrease GIP levels, and there is little consensus on the actual effect of intestinal bypass operations on this hormone; various reports claim decreased, unchanged, or increased postoperative levels.
An alternate possibility, which we will dub the “hindgut hypothesis,” is that bariatric operations that expedite delivery of ingested nutrients to the hindgut promote weight loss by accentuating the ileal brake. In this phenomenon, the presence of nutrients in the ileum suppresses gastrointestinal motility, gastric emptying, small intestinal transit, and thus, food intake. Neural mechanisms are implicated in this response, as well as hormones, including PYY, GLP-1, neurotensin, and enteroglucagon—all of which are increased in response to meals and/or at baseline after JIB (43, 84–87, 95). Enteroglucagon, a marker of secretion from the intestinal L cells that produce GLP-1, is also increased after RYGB and BPD (87, 96). As detailed above, enhanced GLP-1 secretion from facilitated delivery of nutrients to the hindgut could plausibly account for some of the antidiabetic effects of RYGB, JIB, and BPD. In support of the hindgut hypothesis are intriguing rodent experiments in which a portion of the ileum was resected and inserted into the midduodenum (97). Without creating any restrictive or malabsorptive physiology, such ileal interpositions caused major weight loss, possibly by placing the hormone-rich ileum in close contact with ingested nutrients and enhancing the ileal brake. Consistent with this mechanism, ileal interposition increases levels of PYY, GLP-1, and enteroglucagon, and it delays gastric motility and emptying (97–99).
In summary, the mechanisms mediating weight loss and improved glucose tolerance after RYGB may include the following: 1) gastric restriction, leading to early satiety, small meal size, and negative conditioning; 2) bypass of the foregut, impairing ghrelin secretion via still-cryptic mechanisms, and causing mild malabsorption in the case of long-limb variations only; and 3) expedited delivery of nutrients to the hindgut, enhancing the ileal brake, and stimulating the release of PYY and GLP-1, which may decrease food intake and increase glucose tolerance. Dumping symptoms accompanying ingestion of concentrated carbohydrates may contribute in some people. These hypotheses and the others articulated herein are but a few of many possible explanations for the weight-reducing and antidiabetic effects of bariatric surgery, because numerous gut hormones have yet to be examined in this context. Clearly, this is an arena rich with opportunities for research that should ultimately elucidate all of the mechanisms underlying the dramatic effects of bariatric operations. The NIH has recently sponsored a six-center program, the Longitudinal Assessment of Bariatric Surgery (LABS), to address some of these questions over the next 5 yr or more. Hopefully, insights from this and other studies will facilitate the development of new medications that can achieve at least some of the beneficial effects of bariatric surgery, without the surgery.
Acknowledgments
This work was supported by National Institutes of Health Grant R01 DK61516.
Abbreviations:
- AGB,
Adjustable gastric banding;
- BMI,
body mass index;
- BPD,
biliopancreatic diversion;
- DM,
diabetes mellitus;
- GIP,
glucose-dependent insulinotropic peptide;
- GJB,
gastrojejunal bypass;
- GLP-1,
glucagon-like peptide-1;
- JIB,
jejunoileal bypass;
- PYY,
peptide YY3–36;
- QALY,
quality-adjusted life year;
- RYGB,
Roux-en-Y gastric bypass;
- VBG,
vertical banded gastroplasty.
References
Cummings DE, Frayo RS, Marmonier C, Aubert R, Chapelot D, Plasma ghrelin levels and hunger scores among humans initiating meals voluntarily in the absence of time- and food-related cues. Am J Physiol Endocrinol Metab, in press
Couce M, Cottam D, Esplen J, Teijeiro R, Schauer PR, Burguera B 2003 Central vs. peripheral ghrelin: impact on human obesity. NAASO annual meeting. Obes Res 11(Suppl):A35
Vidal J, Morinigo R, Casamitjana R, Moize V, Gomis R 2003 Short-term effects of gastric bypass on circulating ghrelin levels. NAASO annual meeting. Obes Res 11(Suppl):A9
Copeland P, Davis P, Kaplan L 2003 Weight loss after gastric bypass is associated with decreased plasma gastric inhibitory polypeptide without a significant change in circulating ghrelin. NAASO annual meeting. Obes Res 11(Suppl):A17
Overduin J, Frayo RS, Cummings DE 2003 Role of the duodenum and macronutrient type in prandial suppression of ghrelin. NAASO annual meeting. Obes Res 11(Suppl):A21

{kind=link}
{kind=link}