
Abstract
Background
How to evaluate the prognostic significance of lymphatic metastasis in patients with small bowel (jejunoileal) neuroendocrine tumors (SBNETs) is still not conclusive.
Methods
Data for patients with SBNETs, but without distant metastasis, were retrieved from the Surveillance, Epidemiology, and End Results database. Recursive partitioning analysis (RPA) was used for classification development by combining examined lymph nodes (ELNs) and lymph node ratio (LNR).
Results
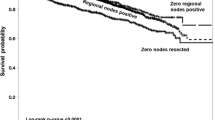
Overall, 1925 patient records were retrieved. Patients with N0 and N1 disease (based on the definition of the European Neuroendocrine Tumor Society [ENETS] staging classification) did not have different OS (p = 0.7867), nor did patients with N0, N1 (< 12 positive nodes), and N2 (≥ 12 positive nodes) disease based on the definition of American Joint Committee on Cancer (AJCC) 8th edition staging classification (p = 0.5276). However, Cox regression analysis indicated that both ELNs (hazard ratio [HR] 0.968, 95% confidence interval [CI] 0.949–0.987; p = 0.0013) and LNR (HR 2.288, 95% CI 1.122–3.682; p = 0.0006) were prognostic factors. Using RPA, we combined ELNs and LNR, and patients were reclassified into three groups (group 1: ELNs ≥ 12, any LNR; group 2: ELNs < 12, LNR < 0.35; group 3: ELNs < 12, LNR ≥ 0.35). Survival analysis and multivariate Cox regression showed that groups 1, 2, and 3 had progressively worse survival. Furthermore, we found that ELNs ≥ 12 could remarkably improve patient survival (p < 0.001).
Conclusions
The current definition of lymphatic metastasis could not help predict patient survival. Our newly proposed classification of lymphatic metastasis is better than the ENETS and AJCC 8th edition staging classifications in evaluating the prognostic significance of lymphatic metastasis in SBNETs. Systematic resection of lymph nodes (≥ 12) could help improve patient survival.




Similar content being viewed by others


References
Dasari A, Shen C, Halperin D, et al. Trends in the incidence, prevalence, and survival outcomes in patients with neuroendocrine tumors in the United States. JAMA Oncol. 2017;3(10):1335–1342.
Chen L, Zhou L, Zhang M, et al. Clinicopathological features and prognostic validity of WHO grading classification of SI-NENs. BMC Cancer. 2017;17(1):521.
Howe JR, Cardona K, Fraker DL, et al. The surgical management of small bowel neuroendocrine tumors: consensus guidelines of the North American Neuroendocrine Tumor Society. Pancreas. 2017;46(6):715–731.
Partelli S, Bartsch DK, Capdevila J, et al. ENETS consensus guidelines for standard of care in neuroendocrine tumours: surgery for small intestinal and pancreatic neuroendocrine tumours. Neuroendocrinology. 2017;105(3):255–265.
Rindi G, Kloppel G, Couvelard A, et al. TNM staging of midgut and hindgut (neuro) endocrine tumors: a consensus proposal including a grading system. Virchows Arch. 2007;451(4):757–762.
Strosberg JR, Weber JM, Feldman M, Coppola D, Meredith K, Kvols LK. Prognostic validity of the American Joint Committee on Cancer staging classification for midgut neuroendocrine tumors. J Clin Oncol. 2013;31(4):420–425.
Amin MB, Edge SB, Greene FL, et al. AJCC cancer staging manual. 8th ed. New York: Springer; 2016.
Landry CS, Lin HY, Phan A, et al. Resection of at-risk mesenteric lymph nodes is associated with improved survival in patients with small bowel neuroendocrine tumors. World J Surg. 2013;37(7):1695–1700.
Kim MK, Warner RR, Ward SC, et al. Prognostic significance of lymph node metastases in small intestinal neuroendocrine tumors. Neuroendocrinology. 2015;101(1):58–65.
Pasquer A, Walter T, Hervieu V, et al. Surgical management of small bowel neuroendocrine tumors: specific requirements and their impact on staging and prognosis. Ann Surg Oncol. 2015;22(Suppl 3):742–749.
Norlen O, Stalberg P, Oberg K, et al. Long-term results of surgery for small intestinal neuroendocrine tumors at a tertiary referral center. World J Surg. 2012;36(6):1419–1431.
Fata CR, Gonzalez RS, Liu E, Cates JM, Shi C. Mesenteric tumor deposits in midgut small intestinal neuroendocrine tumors are a stronger indicator than lymph node metastasis for liver metastasis and poor prognosis. Am J Surg Pathol. 2017;41(1):128–133.
Valsangkar NP, Bush DM, Michaelson JS, et al. N0/N1, PNL, or LNR? The effect of lymph node number on accurate survival prediction in pancreatic ductal adenocarcinoma. J Gastrointest Surg. 2013;17(2):257–266.
Lee HY, Choi HJ, Park KJ, et al. Prognostic significance of metastatic lymph node ratio in node-positive colon carcinoma. Ann Surg Oncol. 2007;14(5):1712–1717.
Strosberg J. Neuroendocrine tumours of the small intestine. Best Pract Res Clin Gastroenterol. 2012;26(6):755–773.
Funding
This research was supported by the Guangzhou Science and Technology Plan (201804010078).
Disclosure
Luohai Chen, Yunda Song, Yu Zhang, Minhu Chen, and Jie Chen have no personal conflicts of interest in relation to this study.
Author information
Authors and Affiliations
Corresponding authors
Rights and permissions
About this article

Cite this article
Chen, L., Song, Y., Zhang, Y. et al. Exploration of the Exact Prognostic Significance of Lymphatic Metastasis in Jejunoileal Neuroendocrine Tumors. Ann Surg Oncol 25, 2067–2074 (2018). https://doi.org/10.1245/s10434-018-6511-9
Received:
Published:
Issue Date:
DOI: https://doi.org/10.1245/s10434-018-6511-9