
Abstract
Introduction
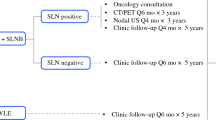
Adjuvant therapy trials required completion lymph node dissection (CLND) for sentinel lymph node (SLN)-positive melanoma prior to systemic treatment, but nodal surveillance without CLND is now common. For patients receiving adjuvant therapy without CLND, patterns of recurrence are unknown and the value of regional nodal ultrasound alongside cross-sectional imaging is not well-defined.
Methods
In a retrospective cohort of SLN-positive melanoma patients managed with nodal surveillance from June 2014 to June 2019, we evaluated the association between adjuvant treatment and location of first recurrence (locoregional, nodal, distant, or multisite) using Chi-square tests. We compared methods of recurrence detection and cost by surveillance intensity using Chi-square and Dunn’s tests.
Results
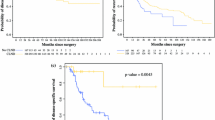
Among 177 nodal surveillance patients, 66 (37%) received adjuvant therapy. Median follow-up was 24 months, during which 48 patients (27%) recurred. Adjuvant treatment did not alter patterns of initial recurrence (p = 0.76). Adjuvant therapy recipients more often had both nodal ultrasound and cross-sectional imaging surveillance (p < 0.01). Among 13 isolated nodal recurrences, 85% were within the first year and 85% were detected by examination and/or ultrasound. Increasing surveillance intensity was not associated with recurrence detection rates but increased overall cost and cost per detected recurrence.
Conclusion
Regardless of adjuvant treatment, most nodal recurrences occurred in the first year and were initially detected clinically or by ultrasound. Findings support continued use of examination and nodal basin ultrasound in addition to any planned cross-sectional imaging surveillance.

Similar content being viewed by others

References
Svedman FC, Pillas D, Taylor A, Kaur M, Linder R, Hansson J. Stage-specific survival and recurrence in patients with cutaneous malignant melanoma in Europe—a systematic review of the literature. Clin Epidemiol. 2016;8:109–22. https://doi.org/10.2147/CLEP.S99021.
Leiter U, Stadler R, Mauch C, et al. Final analysis of DeCOG-SLT trial: no survival benefit for complete lymph node dissection in patients with melanoma with positive sentinel node. J Clin Oncol. 2019;37(32):3000–8. https://doi.org/10.1200/JCO.18.02306.
Kwak M, Farrow NE, Salama AKS, et al. Updates in adjuvant systemic therapy for melanoma. J Surg Oncol. 2019;119(2):222–31. https://doi.org/10.1002/jso.25298.
Leiter U, Stadler R, Mauch C, et al. Complete lymph node dissection versus no dissection in patients with sentinel lymph node biopsy positive melanoma (DeCOG-SLT): a multicentre, randomised, phase 3 trial. Lancet Oncol. 2016;17(6):757–67. https://doi.org/10.1016/S1470-2045(16)00141-8.
Faries MB, Thompson JF, Cochran AJ, et al. Completion dissection or observation for sentinel-node metastasis in melanoma. N Engl J Med. 2017;376(23):2211–22. https://doi.org/10.1056/NEJMoa1613210.
Broman K, Hughes T, Dossett L, et al. Active surveillance of melanoma patients with sentinel node metastasis: an international multi-institution evaluation of post-MSLT-2 adoption and early outcomes. Cancer. 2021;127(13):2251–61.
Farrow NE, Raman V, Williams TP, Nguyen KY, Tyler DS, Beasley GM. Adjuvant therapy is effective for melanoma patients with a positive sentinel lymph node biopsy who forego completion lymphadenectomy. Ann Surg Oncol. 2020;27(13):5121–5. https://doi.org/10.1245/s10434-020-08478-7.
Bredbeck BC, Mubarak E, Zubieta DG, et al. Management of the positive sentinel lymph node in the post-MSLT-II era. J Surg Oncol. 2020;122(8):1778–824. https://doi.org/10.1002/jso.26200.
Eggermont AMM, Chiarion-Sileni V, Grob J-J, et al. Adjuvant ipilimumab versus placebo after complete resection of high-risk stage III melanoma (EORTC 18071): a randomised, double-blind, phase 3 trial. Lancet Oncol. 2015;16(5):522–30. https://doi.org/10.1016/S1470-2045(15)70122-1.
Eggermont AMM, Chiarion-Sileni V, Grob J-J, et al. Prolonged survival in stage III melanoma with ipilimumab adjuvant therapy. N Engl J Med. 2016;375(19):1845–55. https://doi.org/10.1056/NEJMoa1611299.
Weber J, Mandala M, Del Vecchio M, et al. Adjuvant nivolumab versus ipilimumab in resected stage III or IV melanoma. N Engl J Med. 2017;377(19):1824–35. https://doi.org/10.1056/NEJMoa1709030.
Long GV, Flaherty KT, Stroyakovskiy D, et al. Dabrafenib plus trametinib versus dabrafenib monotherapy in patients with metastatic BRAF V600E/K-mutant melanoma: long-term survival and safety analysis of a phase 3 study. Ann Oncol. 2019;30(11):1848. https://doi.org/10.1093/annonc/mdz221.
Eggermont AMM, Blank CU, Mandala M, et al. Adjuvant pembrolizumab versus placebo in resected stage III melanoma. N Engl J Med. 2018;378(19):1789–801. https://doi.org/10.1056/NEJMoa1802357.
Swetter S, Thompson J, Albertini M, et al. NCCN clinical practice guidelines in oncology: melanoma. Version 2.2021. Available at: NCCN.org. Accessed 23 Dec 2020.
Gard G, To YH, Gately L, et al. Impact of adjuvant chemotherapy and patient age on patterns of metastatic recurrence in stage III colorectal cancer. J Clin Oncol. 2021;39(3 Suppl):122.
Wang Y, Zhu L, Xia W, Wu L, Wang F. The impact of adjuvant therapies on patient survival and the recurrence patterns for resected stage IIa–IVa lower thoracic oesophageal squamous cell carcinoma. World J Surg Oncol. 2018;16(1):216. https://doi.org/10.1186/s12957-018-1516-1.
Borcoman E, Kanjanapan Y, Champiat S, et al. Novel patterns of response under immunotherapy. Ann Oncol. 2019;30(3):385–96. https://doi.org/10.1093/annonc/mdz003.
Rauwerdink DJW, Molina G, Frederick DT, Sharova T, Carmichael H, Boland GM. Adjuvant therapy failure patterns in the modern era of melanoma management. Ann Surg Oncol. 2020;27(13):5128–36. https://doi.org/10.1245/s10434-020-08631-2.
Xing Y, Bronstein Y, Ross MI, et al. Contemporary diagnostic imaging modalities for the staging and surveillance of melanoma patients: a meta-analysis. J Natl Cancer Inst. 2011;103(2):129–42. https://doi.org/10.1093/jnci/djq455.
Garland-Kledzik M. The utility of ultrasound in the follow-up of patients with melanoma sentinel node metastases undergoing observation: an analysis of MSLT-II. Ann Surg Oncol. 2020;20(Suppl 1):S32.
Nessim C. Survival impact of imaging surveillance for high-risk resected melanoma treated by systemic therapy at recurrence. Ann Surg Oncol. 2020;20(Suppl 1):S34.
Acknowledgments
This study was supported by the Junior Scientist Research Program at H. Lee Moffitt Cancer Center (Awardees: Kristy K. Broman, Jaileene Perez-Morales, Deepti Bettampadi).
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Disclosure
Zeynep Eroglu served on the advisory boards of Array Biopharma, Regeneron, OncoSec, Genentech, Novartis, SunPharma, and Natera, and receives research funding from Novartis. Ahmad A. Tarhini has received fees for consulting and/or advisory board participation from Partner Therapeutics, Merck, Bristol Myers Squibb, Novartis, Genentech-Roche, Array Biopharma, Sanofi-Genzyme/Regeneron, Pfizer, EMD Serono, NewLink Genetics, BioNTech, Immunocore, and Eisai; has participated in a Data Safety Monitoring Board for Incyte; and has been involved in institution contracted research with Merck, OncoSec, Genentech-Roche, Bristol Myers Squibb, and Clinigen within the last 3 years. Nikhil Khushalani has received personal fees from Regeneron, Inc./Sanofi, Array BioPharma, AstraZeneca, EMD Serono, Genentech, Immunocore, Incyte, Jounce Therapeutics Merck, and Sanofi. He has received research grants and personal fees from Amgen, Gelgene, GlaxoSmithKline, Novartis, and Regeneron, and has received stock or other ownership interest from Amarin Corporation, Bellicum Pharmaceuticals, Mazor Robotics, and TransEnterix. Amod Sarnaik is a consultant to Iovance Biotherapeutics, Guidepoint, Defined Health, and Gerson Lehman group. His institution has received research funding from Iovance Biotherapeutics and Provectus Inc., and he has received speaker fees from Physicians’ Education Resource and Medscape. Vernon K. Sondak is a paid consultant to Merck, Bristol Myers Squibb, Novartis, Regeneron, Array, Replimune, Pfizer, Genentech/Roche, Eisai, Aduro, Amgen, TRM Oncology, and Polynoma. Jonathan S. Zager has received research funding from Novartis, Philogen, Delcath Systems, Amgen, Provectus, Novartis and Castle Biosciences. He has served on advisory boards for Merck, Novartis and Pfizer, and on the speakers bureau for Pfizer, Sun Pharma, and Castle Biosciences. He also provides expert testimony to McGowan Hood and Bubalo Law. Kristy K. Broman, Deepti Bettampadi, Jaileene Pérez-Morales, James Sun, Dennis Kirichenko, Michael J. Carr, and Matthew B. Schabath reported no disclosures.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
Broman, K.K., Bettampadi, D., Pérez-Morales, J. et al. Surveillance of Sentinel Node-Positive Melanoma Patients Who Receive Adjuvant Therapy Without Undergoing Completion Lymph Node Dissection. Ann Surg Oncol 28, 6978–6985 (2021). https://doi.org/10.1245/s10434-021-10570-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1245/s10434-021-10570-5