INTRODUCTION
The most widely consumed legal psychoactive substances in the world, tobacco and alcohol, confer a heavy health burden on almost all populations. Approximately one third of the world’s population reportedly smokes; and in developed countries, 80% of men and 60% of women have consumed alcohol at some point in their lives, with lower, but still substantial, consumption rates in developing countries.[1–4]
The negative health effects of smoking and alcohol are well known, as are their repercussions on the individual, family and society. Yet, more and more young people are initiating tobacco and alcohol use.[5,6]
The use and abuse of these substances contribute significantly to morbidity, premature mortality, disability and lower quality of life; and are associated with more than 60 conditions affecting health.[7,8] Although risk of disease or death from use of either substance vary according to factors such as amount used chronically, almost all organs of the human body can be affected.[1,7]
There is consensus that a gender differential exists, with women more vulnerable to harm from tobacco and alcohol use.[9–11] Women are more susceptible to tobacco’s carcinogenic effects on the lungs and metabolize nicotine differently. With respect to alcohol, women are more susceptible to its damaging effects because the enzymatic processes for oxidizing alcohol in the female liver are slower than in the male’s. While men metabolize up to 30% of alcohol ingested, women metabolize only 10%, and thus have higher blood alcohol levels for the same amount of alcohol consumed.[12,13]
As a result, women with higher intakes of these substances are more likely to have health problems such as complications of pregnancy and increased likelihood of bearing children with disorders such as sudden infant death syndrome and fetal alcohol syndrome. These women are also more likely to suffer from high blood pressure, menstrual cycle alterations and sleep disorders, as well as mental health problems—including depression, stress, anxiety or guilt—that can trigger self-destructive behavior.[14–16]
Problems of tobacco and alcohol use are now being seen in populations that until recently had not been so affected. In recent decades, the social role of women has changed in many societies, and with this has come changes in their patterns of tobacco and alcohol use. Cigarette manufacturers have also deliberately targeted women, another contributing factor to rising rates of smoking among women in many developing countries.[15,16]
Reportedly, at least 10–12% of women smoke worldwide, although stigmatization of women smoking may cause underreporting in some regions. Tobacco use by women varies geographically: male:female differences are greater in the Pacific region and smaller in Europe and the Americas, where approximately 1 in 4 women smoke. Alcohol consumption in women in this last region is approximately 40% above the world average.[5,15]
Cuba’s Second National Survey on Risk Factors and Chronic Diseases (2001) (Spanish acronym, ENFRENT II), a nationwide study of the urban population aged ≥15 years, found smoking prevalence of 23% in women and 41% in men.[17]
In 2007, 12% and 3.7% of all deaths globally were attributable to smoking and alcohol, respectively. Alcohol was responsible for 4% of the global burden of disability-adjusted years of life lost. In the same year, mortality attributable to tobacco use in Cuba—based on data for three disease groups: cardiovascular diseases, cancer, and chronic bronchitis—was estimated at 18% (15,083 deaths). Women accounted for one third of these deaths (5027).[18–21]
Several socioeconomic factors in Cuba—including long traditions of tobacco farming and rum production and permissive cultural attitudes—are associated with social acceptance of smoking and alcohol use. Public health strategies through 2015 in Cuba highlight the need for effective prevention and control of use, abuse and addiction related to both these substances.[22,23]
Implementation of sound and sustainable multisectoral interventions regarding alcohol and smoking requires better epidemiological data and analysis. Although local studies provide some information on specific population groups, no national studies have been published specifically addressing these health-related problems in Cuban women, which are necessary to support effective strategies to lower substance-use prevalence.
This article’s objective is to describe for the first time the socioeconomic profile of women aged ≥15 years who use tobacco and alcohol, resulting in a baseline to analyze results of the new national study under way, to evaluate trends over time, and the effectiveness of preventive and control strategies.
METHODS
Data on tobacco and alcohol consumption by Cubans aged ≥15 years resident in urban areas of Cuba (where 75% of the Cuban population lives)[24] were obtained from the Second National Survey on Risk Factors and Chronic Diseases (2001), a descriptive cross-sectional study, to determine the frequency and epidemiological characteristics of the main chronic disease risk factors.[17] While the population of interest was women, data on both sexes were analyzed for comparison purposes.
The survey used a complex stratified multi-stage cluster design prepared by the National Statistics Bureau. The 14 (at the time) provinces were the strata; clusters consisted of sampled geographic areas, blocks and sections.
In each systematically-sampled geographic area, a block was selected in two sections of which all households were visited to interview all permanent residents aged ≥15 years. Sample size was calculated for each stratum to permit stratum-specific estimates; the national sample was formed by aggregating provincial strata. A weighting factor was used consisting of the inverse of individual selection probability, taking into account age and sex, to compensate for possible bias in population estimates. Sampling was equiprobable at the provincial level, but not nationally. Included were 9260 households (23,743 individuals) and 22,851 individuals surveyed, 52% (11,882) of whom were women. Together, they represented 6.8 million Cubans in this age group.[25]
After obtaining informed consent, professional surveyors conducted structured interviews in selected households to gather demographic information on individuals and families, economic conditions, risk perception regarding specific behaviors, selected chronic non-communicable diseases and their risk factors, medication use, violent behavior, disability and preventive practices. This paper reports on the following: sex, age in years (15–19, 20–39, 40–59, ≥60); educational level completed (primary, middle, high school, university); skin color (white, black, mestizo); marital status (unmarried, married or cohabiting, divorced or separated, widowed); occupation (manager, administrator, upper- or middle-level technician, laborer, service worker); perceived economic situation (excellent, good, fair, poor, very poor); and tobacco and alcohol use.
Investigators defined tobacco and alcohol use as any use in the 30 days prior to the survey.
Prevalence of tobacco and alcohol use, separately and combined, was estimated for both sexes, although conclusions refer only to women, consistent with the study’s objective.
Absolute numbers and percentages were calculated, with 95% confidence intervals (CI) around point estimates; differences were considered significant if confidence intervals did not overlap. Percentages were rounded to one decimal place. Male:female prevalence ratios (PR) were calculated. Data were processed using Statistical Analysis Software (SAS) version 8.02, and presented in tables and figures.
RESULTS
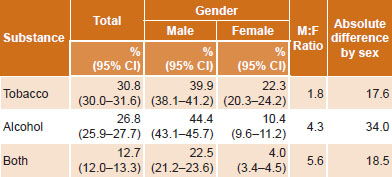
Survey response was high at 96%. Estimated prevalence of smoking in women was 22.3% (95% CI 20.3–24.2), for alcohol use 10.4% (95% CI 9.6–11.2) and for both 4.0% (95% CI 3.4–4.5). Male:female PR for smoking was 1.8, for drinking 4.3 and for use of both tobacco and alcohol, 5.6 (Table 1).
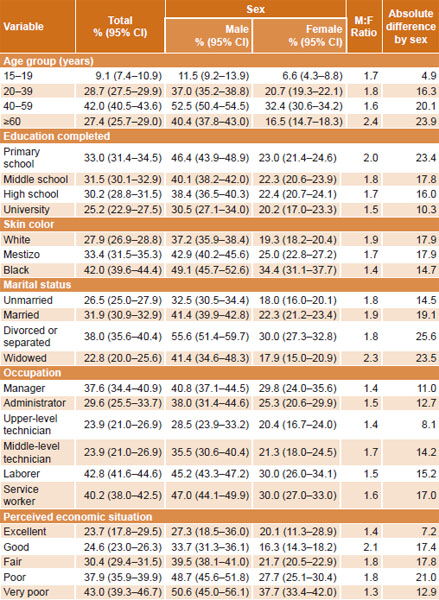
Tobacco use Prevalence was highest in the group aged 40–59 years: 42.0% (95% CI 40.5–43.6). In all age groups, smoking was approximately twice as common in men as in women—male:female ratios ranged from 1.6 to 2.4—with the smallest absolute difference observed in adolescents (4.9%) (Table 2).
Smoking rates were lowest in university graduates: 25.2% (95% CI 22.9–27.5), and both absolute and relative differences between sexes were least in these, compared to those with less education.
Smoking rates were higher in people with black skin, both women and men, than in other skin color groups, with a male:female PR of 1.4, compared to ratios of 1.9 and 1.7 in white and mestizo persons respectively (Table 2).
Divorced or separated individuals more frequently reported smoking than did unmarried, married or widowed, but absolute prevalence differences by sex were least in the unmarried group. The male:female PR did not differ appreciably by marital status (range 1.8–2.3) (Table 2).
Table 1: Prevalence of tobacco and alcohol use by sex in Cuba, 2001
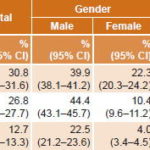
Source: ENFRENT II
Table 2: Prevalence of tobacco use by sociodemographic variables in Cuba, 2001
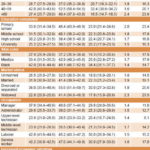
Source: ENFRENT II
Overall, smoking was more prevalent in laborers, service workers and managers than in technical and administrative personnel. In male laborers, service workers and managers, smoking was more prevalent in than in upper-level technical workers. Women laborers and service workers had higher smoking prevalence than technical workers (middle- and upper-level). The lowest absolute difference in smoking prevalence by sex (8.1%) was observed in upper-level technical workers, in whom confidence intervals for male and female prevalences overlapped, indicating a non-significant difference.
In both men and women, smoking prevalence varied inversely with perceived economic situation. Women smokers most frequently perceived their economic situation as very poor; the male:female ratio for that category 1.3. In contrast, in those perceiving their economic situation as excellent, confidence intervals around prevalences in men and women overlapped, indicating a non-significant difference (PR 1.4). The greatest absolute difference between male and female prevalence was in those perceiving their economic situation as poor.
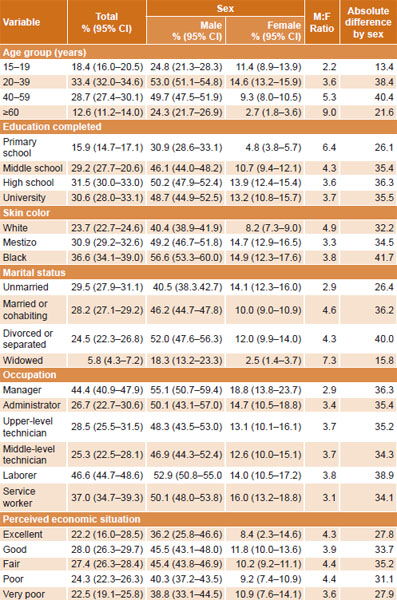
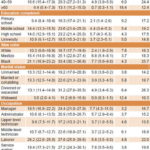
Alcohol use Overall population prevalence of alcohol use in the previous 30 days was 26.8% (95% CI 25.9–27.7). Male:female PR was 4.3 (Table 1). The smallest male:female PR and absolute sex difference were observed in the group aged 15–19 years (PR 2.2, difference 13.4%). Prevalence ratios ranged from 3.6 to 9.0 in the other age groups (Table 3).
Overall prevalence of alcohol use was lowest in those who had completed only primary school; this was observed in both sexes, but it was also the age group with the highest male:female PR (6.4 vs. 3.6–4.3 in the other educational attainment groups) (Table 3).
Alcohol use was more prevalent in black than in mestizo or white Cubans. Prevalence in black women was higher than in white women, but similar to that in mestizo women (Table 3).
Patterns of alcohol use by marital status differed between the sexes. Overall prevalence was lowest in widowed Cubans (5.8%, 95% CI 4.3–7.2), and this held for both sexes (widowers 18.3%, 95% CI 13.2–23.3; widows 2.5%, CI 1.4–3.7). The highest prevalence in women was in the unmarried (14.1%, 95% CI 12.3–16.0), but the confidence interval for this group overlapped with that of divorced women (12.0 95% CI 9.9–14.0), which in turn overlapped with that of married women (10.0%, 95% CI 9.0–10.9). In men, the married (46.2%, 95% CI 44.7–47.8) and divorced (52.0%, 95% CI 47.6–56.3) reported alcohol use most frequently.
There was no observable pattern of alcohol use by occupation in men and women analyzed separately, but overall prevalence was higher in managers (44.4%, 95% CI 40.9–47.9) and laborers (46.6%, 95% CI 44.7–48.6), followed by service workers (37.0%, 95% CI 34.7–39.3). No differences were observed between administrative workers and upper- and middle-level technicians. Male:female PRs ranged from 2.9 in managers to 3.8 in laborers but there was overlap in confidence intervals.
No clear pattern emerged for perceived economic situation, neither overall nor for either sex.
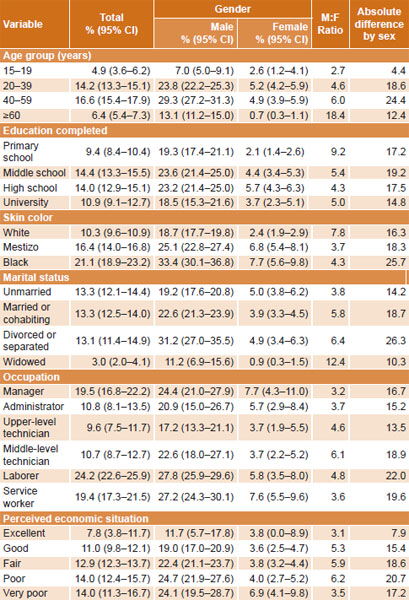
Alcohol and tobacco use combined Overall, 12.7% of respondents used both tobacco and alcohol; prevalence in women was 4.0% (95% CI 3.4–4.5). Male:female PR was 5.6 (Table 1).
Table 3: Prevalence of alcohol use by sociodemographic variables, Cuba, 2001

Source: ENFRENT II
The highest overall prevalence was observed in the groups aged 40–59 years (16.6%, 95% CI 15.4–17.9), and 20–39 years (14.2%, 95% CI 13.3–15.1). Male:female PRs were 6.0 for the former age group and 4.6 for the latter. In women, no significant differences were observed between these age groups. Lowest prevalence was consistently seen in the oldest and youngest groups, globally and in both sexes. The youngest group had the lowest overall prevalence (4.9%, 95% CI 3.6–6.2) and the lowest male:female PR (2.7) and absolute difference (4.4%) (Table 4).
Overall prevalence of tobacco and alcohol use was higher in those who had completed middle (14.4%, 95% CI 13.3–15.5) and high school (14.0%, 95% CI 12.9–15.1) than in those with only primary education (9.4%, 95% CI 8.4–10.4) or who had completed university (10.9%, 95% CI 9.1–12.7). In women, prevalence was lowest in those with only primary education (2.1%, 95% CI 1.4–2.6). Male:female PR difference was lowest in the most educated group (14.8%).
Use of tobacco and alcohol was more common in black (21.1%, 95% CI 18.9–23.2) and mestizo (16.4%, 95% CI 14.0–16.8) than in white Cubans (10.3%, 95% CI 9.6–10.9). The smallest absolute difference in prevalence by sex was observed in the latter (16.3% vs 18.3% and 25.7%, in mestizo and black Cubans, respectively), although the male:female PR was the highest (7.8) where the smallest gender difference was observed. However, in black women, both addictions were reported 3 times more than in white women: 7.7% (5.6–9.8) vs. 2.4% (1.9–2.9), respectively.
By marital status, prevalence of tobacco and alcohol use was lowest among the widowed (3.0%, 95% CI 2.0–4.1), while other marital status groups had similar prevalences of approximately 13% (unmarried 13.3%, 95% CI 12.1–14.4; married 13.3%, 95% CI 12.5–14.0; divorced 13.1%, 95% CI 11.4–14.9). A similar pattern was seen in women, but not men, in whom prevalence was substantially higher in divorced men (31.2%, 95% CI 27.0–35.5) than in married (22.6%, 95% CI 21.3–23.9) and unmarried men (19.2%, 95% CI 17.6–20.8). The lowest male:female PR was observed in the unmarried group (3.8).
By occupation, overall use of tobacco and alcohol was most common in laborers (24.2%, 95% CI 22.6–25.9), managers (19.5%, 95% CI 16.8–22.2) and service workers (19.4%, 95% CI 17.3–21.5). No important differences between occupational groups were observed in women. The lowest male:female PR was found in managers (3.2). The smallest absolute differences between men and women were observed in upper-level technical workers (13.5%), administrative workers (15.2%) and managers (16.7%). In men, prevalence of tobacco and alcohol use by upper-level technicians (17.2%, 95% CI 13.3–21.1) was lower than that in laborers (27.8%, 95% CI 25.9–29.6) and service workers (27.2%; 95% CI 24.3–30.1) (Table 4).
Prevalence of tobacco and alcohol use was lower overall in individuals whose perceived economic situation was excellent (7.8%, 95% CI 3.8–11.7) or good (11.0%, 95% CI 9.8–12.1) than in those who reported their economic situation as fair (12.9%, 95% CI 12.3–13.7) or poor (14.0%, 95% CI 12.4–15.7), a pattern also observed in men (although with overlap in confidence intervals for excellent and very bad perceived economic situation). No gradient was observed in women, in whom prevalence was much lower than in men in all age groups (male:female PR 3.1–6.2).
As self-perceived economic situation improved, absolute difference in prevalence between men and women—but not male:female PR—lessened (Table 4).
Table 4: Prevalence of combined tobacco and alcohol use by sociodemographic variables in Cuba, 2001
Source: ENFRENT II
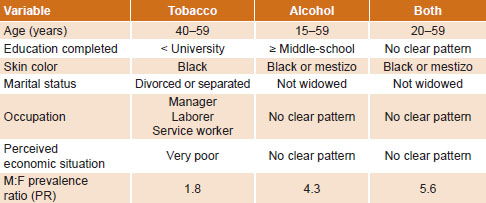
Table 5: Profi le of Cuban women most frequently using tobacco, alcohol or both, 2001

Source: ENFRENT II
The profile of Cuban women for tobacco and alcohol use, separately and combined, is displayed in Table 5.
DISCUSSION
A review of the Cuban literature found no national-level studies of men’s and women’s use of these two legal drugs. Although the data presented here are from 2001, a study limitation, they constitute the most complete available national data on tobacco and alcohol use in male and female urban residents.
We observed tobacco use prevalence in Cuban women to be high compared to the rest of the Americas and the world. Although prevalence varies widely internationally, in the 192 countries for which WHO reports prevalence overall and by sex, Cuba ranks among the top 33. In Latin America, Cuba’s prevalence of tobacco use in women (23.1%) is surpassed only by Chile (36.8%) and Argentina (24.2%). The smallest male:female differences regionally are reported in the Americas and Europe and the largest in the Eastern Pacific: data from China show a dramatic gap between the sexes: 63% in men and 4.0% in women.[26,27] There is also current debate about the possibility that women are more vulnerable to secondhand smoke, with no consensus. Some findings do not support this hypothesis[28,29] while others do find evidence of increased susceptibility in women, likely due to various factors, including genetic differences and the anti-estrogenic effect of tobacco smoke.[30,31]
Taken together, the foregoing suggests that reducing smoking among Cuban women could lower the high risk of preventable illness and death they now face from multiple diseases that share smoking as a risk factor—including cardiovascular, respiratory, neurological, endocrine, digestive and reproductive conditions as well as lung cancer and other neoplasms.[32]
The smaller difference in smoking prevalence between male and female adolescents in this study has been observed elsewhere; there is a need for more effective actions to prevent smoking in both sexes in this age group.[33]
Prevalence of alcohol use varies widely in the Americas region. In populations aged 15–64 years, for example, prevalence surpasses 50% in Argentina, Chile and Uruguay, is more than 40% in Bolivia and is close to 35% in Ecuador and Peru. Sex differences are less pronounced in the population aged 15–34 years, but prevalence in women is lower than in men.[20]
Prevalence of alcohol use in women aged 15–17 years has been reported as follows in several South American countries: Argentina 50.2%, Chile 50%, Colombia 63.1%, Uruguay 65.3% and Brazil 66.8%. Ecuador and Mexico are found in another group with a range of 39.8% to 50.0%. In Bolivia, prevalence is 22.7%. Lower levels of alcohol consumption were found among Cuban adolescent women, perhaps reflecting Cuba’s efforts to safeguard the health and wellbeing of children and adolescents, this age group merits careful monitoring, given the regional patterns referred to above.[34]
Many lifelong behaviors are established in adolescence, so the finding that almost one in five adolescents in this study consumed alcohol should serve as an alert. The small difference between the sexes could reflect the permanent incorporation of Cuban women into spheres of social and economic activities once traditionally the realm of men: as their social role has changed, so have their behaviors. Thus, current trends are more similar to men’s patterns, including in alcohol consumption, although with a certain tendency to hide or deny problems of substance abuse.[34]
We observed that tobacco use dropped as educational level increased, a finding reported in other studies whose authors argued more education enabled better understanding of smoking risks and benefits of not smoking, leading to self-protective behaviors. We saw this pattern only in men however; there was no such gradient in women, a phenomenon described by PAHO in the 1970s and confirmed in subsequent surveys, showing a tendency to higher smoking prevalence in more educated women. Our finding of similar smoking prevalence in women across all educational levels could indicate a weaker effect of educational level on smoking habits in women, suggesting a need for further research on the role of education and possible contribution of other factors.[35–37]
Higher rates of alcohol use observed in highly-educated individuals could be related to their greater purchasing power than in other educational groups.[38] We did not assess amount consumed.
The smaller difference in prevalence of tobacco use between unmarried women and men (14.5%) could be attributed to the preponderance in this category of youth, in whom the male:female differences in tobacco use are progressively diminishing.[26]
The higher rates of alcohol use in unmarried women could be explained by research results suggesting that women may drink, in the first place, in response to loneliness, to calm the anxiety and conflicts it induces, and to alleviate pain.[39,40]
An important limitation in the analysis of the variables of “skin color” and “perceived economic situation” associated with smoking and alcohol consumption in women is limited comparability with other studies. Notably, the highest prevalence of tobacco and alcohol use, separately and together, was observed in non-white women, perhaps a reflection of other differences that could help explain these risk behaviors.
Perceived economic situation could to a certain extent reflect objective situations in other contexts, but in Cuba, the relationship is unclear and even sometimes contradictory. This lack of clarity could partly explain the lack of relationship between perceived economic situation and combined use of tobacco and alcohol by our female respondents. It is an intriguing issue and calls for further study in the Cuban population.[39,40]
Our results call attention to the particularities of women’s relationship to tobacco and alcohol, which differs from men’s and calls for gender-specific prevention and intervention strategies. They are also consistent with findings of studies of perception of health risks, including alcohol and tobacco, in which women reported heightened perception compared to men, providing better prospects for change toward health-promoting and -protecting behaviors.[41,42]
CONCLUSIONS
Our results provide a baseline for assessment of subsequent changes in the evolution of alcohol and tobacco use in the Cuban population, particularly in women, since it is the first study to present a profile of Cuban women’s use of alcohol and tobacco. Its results may thus provide public health decision-makers with evidence to design more effective strategies to help reduce these risk behaviors and their damage to individuals, families and society.