
Abstract
OBJECTIVES: Few have compared socio-economic disparities in screening tests for cancer with recommended tests for other chronic diseases. We examined whether receipt of testing for colorectal, cervical and breast cancer, as well as diabetes and high cholesterol, differs by neighbourhood-level socio-economic and recent immigrant status.
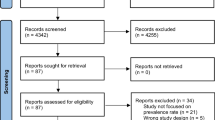
METHODS: We conducted a population-based retrospective cohort study of patients identified as screen-eligible in 2009 living in Ontario, Canada. Postal codes were used to assign residents to a dissemination area (DA). Using Canadian census data, DAs were stratified by income quintile and proportion of recent immigrants. Prevalence of screening for cancer (colorectal, cervical, breast), diabetes, and high cholesterol, using administrative data, and prevalence ratios (least/most advantaged) were calculated.
RESULTS: The cohort comprised 7,652,592 people. Receipt of screening for colorectal cancer (women 61.6%; men 55.1%) and breast cancer (59.9%) were the lowest and diabetes (women 72.9%; men 61.4%) and high cholesterol (women 82.4%; men 70.3%) were the highest. We found disparities in the receipt of all tests, with the lowest uptake and largest disparities for cancer screening among those living in both low-income and high-immigration DAs: colorectal–women 48.6%; RR 0.77; 95% CI (0.74-0.79) and men 40.6%; RR 0.71 (0.68-0.74); cervical–52.0%; RR 0.80 (0.78-0.81) and breast—45.7%; RR 0.74 (0.72-0.77).
CONCLUSION: People living in low-income and high-immigration DAs had the lowest screening participation for all tests, although disparities were highest for cancer. An organized integrated chronic disease screening strategy leveraging the higher diabetes and high cholesterol screening participation may increase screening for cancer and other chronic diseases in never- and underscreened populations.
Résumé
OBJECTIFS: Peu d’études comparent les disparités socioéconomiques dans le recours aux tests de dépistage du cancer et aux tests recommandés pour dépister d’autres maladies chroniques. Nous avons cherché à déterminer si le recours aux tests de dépistage du cancer colorectal, du col utérin et du sein, ainsi que du diabète et de l’hypercholestérolémie, diffère selon le niveau socioéconomique du quartier et le statut d’immigrant récent.
MÉTHODE: Nous avons mené une étude de cohortes populationnelle rétrospective auprès de patients vivant en Ontario (Canada) identifiés comme étant admissibles au dépistage en 2009. Les codes postaux ont servi à affecter chaque résident à une aire de diffusion (AD). À l’aide des données du Recensement du Canada, les AD ont été stratifiées selon le quintile de revenu et la proportion d’immigrants récents. Nous avons calculé la prévalence du dépistage du cancer (colorectal, du col utérin, du sein), du diabète et de l’hypercholestérolémie à l’aide de données administratives, ainsi que les ratios de prévalence (moins/mieux nantis).
RÉSULTATS: La cohorte comptait 7 652 592 personnes. La participation au dépistage du cancer colorectal (femmes 61,6 %; hommes 55,1 %) et du cancer du sein (59,9 %) était la plus faible, et la participation au dépistage du diabète (femmes 72,9 %; hommes 61,4 %) et de l’hypercholestérolémie (femmes 82,4 %; hommes 70,3 %) était la plus élevée. Nous avons constaté des disparités dans le recours à tous les tests, la participation la plus faible et les plus grandes disparités dans le dépistage du cancer étant observés chez les résidents des AD à faible revenu et à forte immigration: cancer colorectal–femmes 48,6 %; RT 0,77; IC de 95 % (0,74–0,79) et hommes 40,6 %; RT 0,71 (0,68–0,74); cancer du col utérin–52,0 %; RT 0,80 (0,78–0,81) et cancer du sein–45,7 %; RT 0,74 (0,72–0,77).
CONCLUSIONS: Les résidents des AD à faible revenu et à forte immigration affichaient la plus faible participation au dépistage pour l’ensemble des tests, mais avec des disparités plus prononcées pour le dépistage du cancer. Une stratégie structurée et intégrée de dépistage des maladies chroniques misant sur la participation plus élevée au dépistage du diabète et de l’hypercholestérolémie pourrait accroître le dépistage du cancer et d’autres maladies chroniques dans les populations jamais ou insuffisamment dépistées.
Similar content being viewed by others

References
Miller AB, Anderson G, Brisson J, Laidlaw J, LePitre N, Malcolmson P, et al. Report of a national workshop on screening for cancer of the cervix. CMAJ 1991;145:1301–25.
Hewitson P, Glasziou P, Watson E, Towler B, Irwig L. Cochrane systematic review of colorectal cancer screening using the fecal occult blood test (Hemoccult): An update. Am J Gastroenterol 2008;103:1541–49.
Leddin DJ, Enns R, Hilsden R, Plourde V, Rabeneck L, Sadowski DC, Singh H. Canadian Association of Gastroenterology position statement on screening individuals at average risk for developing colorectal cancer. Can J Gastroenterol 2010;24:705–14.
The Canadian Task Force on Preventive Health Care. Recommendations on screening for breast cancer in average-risk women aged 40-74 years. CMAJ 2011;183:1991–2001.
Murphy J, Kennedy EB, Dunn S, McLachlin M, Fung Kee Fung M, Gzik D, et al. Cervical screening: A guideline for clinical practice in Ontario. J Obstet Gynaecol Can 2012;34(5):453–58.
Krzyzanowska MK, Barbera L, Elit L, Kwon J, Lofters A, Saskin R, et al. In: Bierman AS (Ed.), Project for an Ontario Women’s Health Evidence-Based Report. Volume 1. Toronto, ON: St. Michael’s Hospital and the Institute for Clinical Evaluative Sciences, 2009.
Stuart G, Taylor G, Bancej CM, Beaulac J, Colgan T, Franco EL, et al. Report of the 2003 pan-Canadian forum on cervical cancer prevention and control. J Obstet Gynaecol Can 2004;26:1004–28.
American Cancer Society. Cancer prevention and early detection, facts and figures, 2012. Available at: http://www.cancer.org/acs/groups/content/@epidemiologysurveilance/ documents/document/acspc-033423.pdf (Accessed July 30, 2012).
Finkelstein, MM. Preventive screening: What factors influence testing? Can Fam Physician 2002;48:1494–501.
Sambamoorthi U, McAlpine, DD. Racial, ethnic, socioeconomic, and access disparities in the use of preventive services among women. Prev Med 2003;37:475–84.
Glazier RH, Creatore MI, Gozdyra P, Matheson FI, Steele LS, Boyle E, Moineddin R. Geographic methods for understanding and responding to disparities in mammography use in Toronto, Canada. J Gen Intern Med 2004;19:952–61.
Singh SM, Paszat LF, Li C, He J, Vinden C, Rabeneck L. Association of socioeconomic status and receipt of colorectal cancer investigations: A population based retrospective cohort study. CMAJ 2004;171:461–65.
Lofters AK, Glazier RH, Agha MM, Creatore MI, Moineddin R. Inadequacy of cervical cancer screening among urban recent immigrants: A populationbased study of physician and laboratory claims in Toronto, Canada. Prev Med 2007;44:536–42.
Johnston GM, Boyd CJ, MacIsaac, MA. Community-based cultural predictors of Pap smear screening in Nova Scotia. Can J Public Health 2004;95:95–98.
Lofters A, Moineddin R, Hwang SW, Glazier, RH. Low rates of cervical cancer screening among urban immigrants: A population-based study in Ontario, Canada. Med Care 2010;48:611–18.
Genest J, McPherson R, Frohlich J, Anderson T, Campbell N, Carpentier A, Ehud U. 2009 Canadian Cardiovascular Society/Canadian guidelines for the diagnosis and treatment of dyslipidemia and prevention of cardiovascular disease in the adult–2009 recommendations. Can J Cardiol 2009;25:567–79.
Pottie K, Jaramillo A, Lewin G, Dickinson J, Bell N, Brauer P, et al. with the Canadian Task Force on Preventive Health Care. Recommendations on screening for type 2 diabetes in adults. CMAJ 2012;184:1687–96.
Creatore MI, Booth GL, Manuel DG, Moineddin R, Glazier, RH. Diabetes screening among immigrants: A population-based urban cohort study. Diabetes Care 2012;35:754–61.
Wilson SE, Rosella LC, Lipscombe LL, Manuel, DG. The effectiveness and efficiency of diabetes screening in Ontario, Canada: A population-based cohort study. BMC Public Health 2010;10:506.
Cancer Care Ontario. ColonCancerCheck 2008 program report. Toronto: Cancer Care Ontario, 2010. Available at: http://www.cancercare.on.ca/ colorectalscreening (Accessed July 30, 2012).
Wilkins R. PCCF+ Version 5F User’s Guide. Automated Geographic Coding Based on the Statistics Canada Postal Code Conversion Files, Including Postal Codes through July 2009: Catalogue 82F0086-XDB, February 2010. Ottawa, ON: Health Analysis Division, Statistics Canada, 2010.
Wilkins R. Use of postal codes and addresses in the analysis of health data. Health Rep 1993;5:157–77.
Krieger N. Overcoming the absence of socioeconomic data in medical records: Validation and application of a census-based methodology. Am J Public Health 1992;82:703–10.
Davison AC, Hinkley, DV. Bootstrap Methods and Their Applications. New York, NY: Cambridge Press, 1997.
Cancer Care Ontario. Ontario Breast Screening Program 20th Anniversary Report. Toronto: Cancer Care Ontario, 2010. Available at: http://www.cancercare.on.ca/OBSP20thAnniversary (Accessed July 30, 2012).
Steven D, Fitch M, Dhaliwal H, Kirk-Gardner R, Sevean P, Jamieson J, Woodbeck H. Knowledge, attitudes, beliefs, and practices regarding breast and cervical cancer screening in selected ethnocultural groups in Northwestern Ontario. Oncol Nurs Forum 2004;31:305–11.
Davis TC, Dolan NC, Ferreira MR, Tomori C, Green KW, Sipler AM, Bennett, CL. The role of inadequate health literacy skills in colorectal cancer screening. Cancer Invest 2001;19:193–200.
Rabeneck L, Paszat L. A population based estimate of the extent of colorectal cancer screening in Ontario. Am J Gastroenterol 2004;99:1141–44.
McIssac WJ, Fuller-Thomson E, Talbot Y. Does having regular care by a family physician improve preventive care? Can Fam Physician 2001;47:70–76.
Barbara Starfield B, Shi L, Macinko J. Contribution of primary care to health systems and health. Milbank Q 2005;83:457–502.
Integrated Screening Programme Report. Singapore: Health Promotion Board, 2012. Available at: http://www.hpb.gov.sg/HOPPortal/programmes-article/ 3672. (Accessed July 30, 2012).
Lee BY, Jo, HS. Evaluation of a navigator program for cancer screening of women in Korean communities. Asian Pacific J Cancer Prev 2011;12:271–75.
Kinney AY, Bloor LE, Martin C, Sandler, RS. Social ties and colorectal cancer screening among Blacks and Whites in North Carolina. Cancer Epidemiol Biomarkers Prev 2005;14:182–89.
Subramanian SV, Chen JT, Rehkopf DH, Waterman PD, Krieger N. Comparing individual- and area-based socioeconomic measures for the surveillance of health disparities: A multilevel analysis of Massachusetts births, 1989–1991. Am J Epidemiol 2006;164:823–34.
Author information
Authors and Affiliations
Corresponding author
Additional information
Financial Support: Financial support for this study was provided in part by The Ontario Cancer Screening Research Network (PI Lawrence F. Paszat) and a grant from the Canadian Cancer Society Research Institute. The funding agreement ensured the authors’ independence in designing the study, interpreting the data, writing and publishing the paper.
Conflict of Interest: None to declare.
Rights and permissions
About this article
Cite this article
Borkhoff, C.M., Saskin, R., Rabeneck, L. et al. Disparities in Receipt of Screening Tests for Cancer, Diabetes and High Cholesterol in Ontario, Canada: A Population-based Study Using Area-based Methods. Can J Public Health 104, e284–e290 (2013). https://doi.org/10.17269/cjph.104.3699
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.17269/cjph.104.3699