 Inês Almada-Correia
Inês Almada-Correia Pedro Miguel Neves
Pedro Miguel Neves Antti Mäkitie
Antti Mäkitie Paula Ravasco
Paula Ravasco- 1Centre for Interdisciplinary Research in Health, Universidade Católica Portuguesa, Lisbon, Portugal
- 2Department of Otorhinolaryngology-Head and Neck Surgery, Helsinki University Hospital and University of Helsinki, Helsinki, Finland
- 3Research Programme in Systems Oncology, Faculty of Medicine, University of Helsinki, Helsinki, Finland
- 4Division of Ear, Nose and Throat Diseases, Department of Clinical Sciences, Intervention and Technology, Karolinska Institutet and Karolinska University Hospital, Stockholm, Sweden
- 5University Hospital of Santa Maria, Universidade de Lisboa, Lisbon, Portugal
Introduction: Head and neck cancer (HNC) patients show a high risk of malnutrition due to the lifestyle habits adopted prior to the diagnosis as well as to the compromising impact of both the anatomical location of the tumor and the treatment modalities on food intake. Weight change, measurement of skinfold thickness, biochemical parameters, bioelectrical impedance analysis (BIA), computed tomography (CT), magnetic resonance (MRI), or dual-energy x-ray absorptiometry (DXA) are available techniques to evaluate nutritional status and/or body composition in the clinical practice. Evaluating body composition alterations in HNC patients is essential to be able to offer the best therapeutical interventions. In this paper, we review the existing literature regarding body composition evaluation in HNC patients to determine, which is the most suitable method for this population, regarding availability in the day-to-day practice, patient burden, cost, sensibility, and specificity.
Methodology: A literature search for relevant papers indexed in MEDLINE, Cochrane Library and Scielo was conducted, with no publication date restriction and for all published articles until the 31 January, 2019. All the papers written in English, with interventions in humans, exclusively considering HNC patients were selected.
Results: A total of 41 studies with different methodologies were included in this review. In 15 studies BIA was the used assessment method and three of them also evaluated skinfold thickness and one was a bioelectric impedance vector analysis (BIVA). Body composition assessment was made with DXA in eight studies, one of which also included muscle biopsies. In two studies the chosen method was both BIA and DXA. CT/ positron emission tomography-CT was applied in 11 studies and one also included MRI. In two studies body composition was assessed with skinfold measurements alone and one study only used BIVA.
Conclusions: Despite the different existing body composition assessment tools, it seems that skeletal muscle mass (SMM) measurement at the level of cervical spine C3 vertebra may be a reliable method for SMM assessment as it strongly correlates with cross-sectional area measures at the level of L3 and it allows a cost-effective body composition assessment without the need for additional radiation exposure.
Introduction
Head and neck cancer (HNC) is responsible for ~300.000 annual deaths worldwide, with a 40–50% survival rate (1). Beside the hypercatabolic characteristics of cancer, HNC patients show a high risk of malnutrition due to the lifestyle habits, such as smoking and alcohol consumption, adopted prior to the diagnosis as well as to the compromising impact that both the anatomical location of the tumor and the various treatment modalities may have on food intake (2, 3). It is estimated that about 60% of these patients show poor nutritional status and about 80% lose weight during treatment (2, 3). Malnourished patients have a higher risk of infection, delayed wound healing, impaired cardiac and respiratory function, muscular weakness, depression, poor quality of life, higher rate of postoperative complications, higher risk of refeeding syndrome, impaired response to treatments, higher mortality rate as well as longer hospitalization time (2). In order to counter malnutrition, its' early detection is critical.
Some authors suggest that ~70% of the weight loss identified in HNC patients corresponds to lean body mass (LBM) (4–6). Loss of LBM has been presented as an important prognostic factor (4, 7) with influence in treatment toxicities (8), risk of recurrence and mortality (9), impaired muscle strength, a decline in physical activity and functional performance (6). It seems that, in HNC patients, LBM depletion may provide additional and relevant information as an outcome predictor beside weight loss alone and furthermore, high BMI, and low LBM may associate with each other (10). For these reasons, considering LBM as a predictor of clinical outcome would take into account also patients with sarcopenic obesity (11). The main component of LBM is skeletal muscle mass (SMM). Sarcopenia is characterized by low SMM combined with low muscle strength or low physical performance, may be highly prevalent in HNC patients (12). Low SMM seems to have the most significant impact on the incidence of complications, prolonged hospital stay, lower overall survival, lower disease-free survival, and decreased survival in surgical oncology (13).
Weight loss alone cannot predict LBM loss (14), and several studies have underlined the importance of body composition evaluation in HNC patients (8). Besides questionnaires like Patient-Generated Subjective Global Assessment (PG-SGA) that allow the assessment of the nutritional status, weight change, measurement of skinfold thickness, bioelectrical impedance analysis (BIA), computed tomography (CT), magnetic resonance (MRI), or dual-energy x-ray absorptiometry (DXA) are techniques to evaluate nutritional status and/or body composition (10). DXA is considered the gold standard for total body composition analysis (8, 15), but it is a medical exam and not a regular part of the treatment and assessment protocol for HNC patients (10, 12).
Evaluating body composition alterations in HNC patients is essential in order to establish the best therapeutical intervention, but is also a challenging task. We review the existing literature regarding body composition evaluation in HNC patients to determine the most suitable method for this population, regarding availability in the routine clinical practice, patient burden, cost, sensibility, and specificity.
Methodology
A literature search for relevant papers indexed in MEDLINE, Cochrane Library and Scielo was conducted, with no publication date restriction and for all published articles until the 31 January 2019. All the papers wrote in English, with interventions in humans, exclusively considering HNC patients, were selected. Figure 1 describes the selection process of articles. The following conjugated search terms were used: head and neck cancer OR larynx cancer OR hypopharynx cancer OR oropharynx cancer OR lip cancer OR oral cavity cancer or salivary gland cancer OR nasopharynx cancer OR nasal cavity cancer OR paranasal sinus cancer OR middle ear cancer; physical activity; body composition OR bioelectrical impedance analysis OR phase angle OR computed tomography OR magnetic resonance OR dual-energy x-ray absorptiometry OR bioimpedance spectroscopy OR bioelectrical impedance spectroscopy OR BIS OR multiple-frequency BIA OR MFBIA, MF-BIA OR single-frequency OR SFBIA OR BIVA OR bioimpedance vector analysis OR SF-BIA OR bioelectrical impedance vector analysis OR magnetic resonance imaging OR MRI or MRI Scan OR CT scan OR computed tomography scan OR computed axila tomography scan OR DEXA or DXA or CT imaging; LBM OR lean tissue OR FFM OR lean soft tissue OR fat mass OR anthropometric assessment OR body cell mass assessment OR intracellular water.
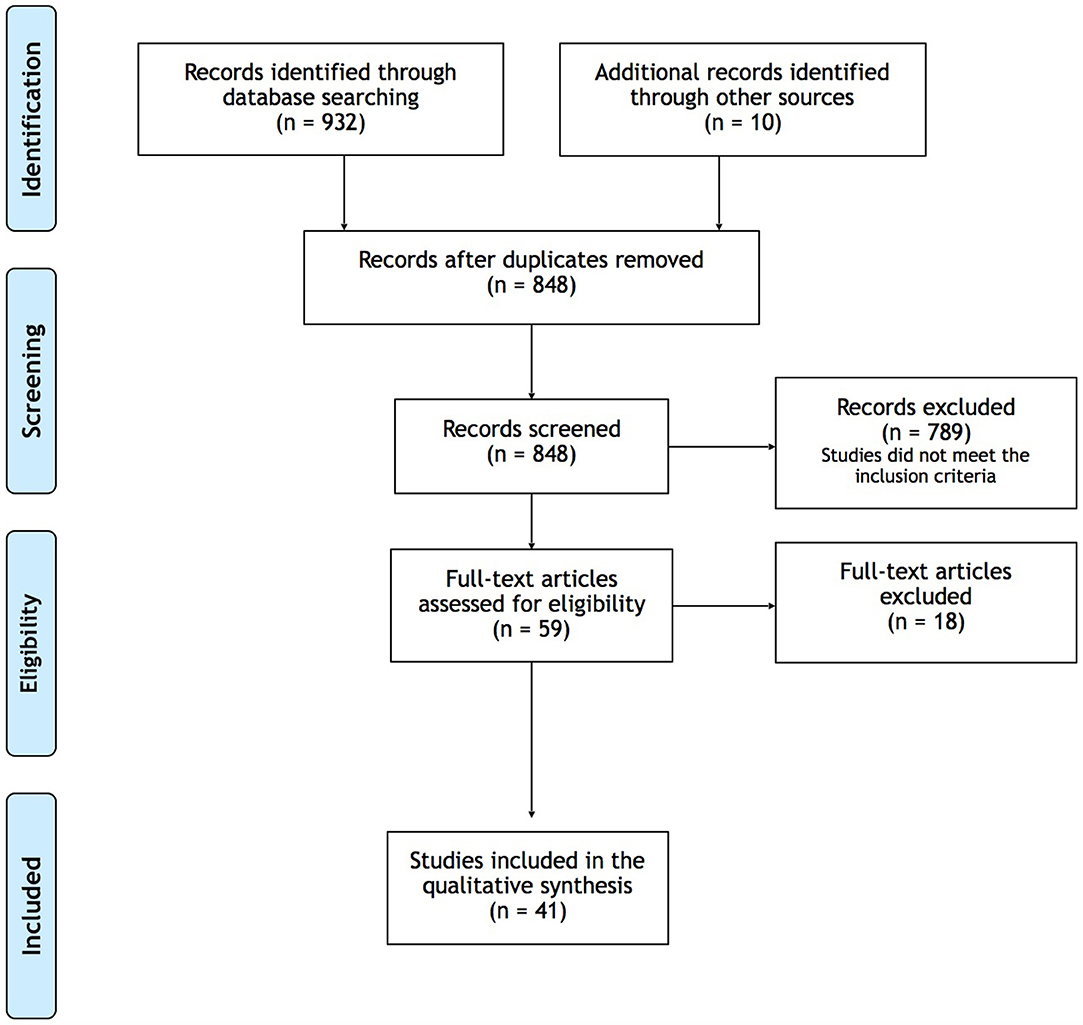
Figure 1. Flow diagram of the study selection process.
The first selection of articles was based on the titles and abstracts, and then full texts were evaluated. All the articles that included body composition evaluation using BIA, MRI, CT, DXA, or skinfold measures, in HNC patients over 18 years old, were included in this review. The articles only considering BMI or with body composition evaluations in a population with other cancer sites than the head and neck area, were not included. All study designs were included. Data were collected from each individual study and then systematically recorded in a document that included the following parameters: author, study methodology, study objectives, number of participants, mean age, gender, cancer stage, treatment, median BMI, inclusion and exclusion criteria, body composition assessment (technique, variables assessed, assessment timing), study limitations and conclusions.
Results
The search of the databases MEDLINE, Cochrane Library and Scielo, resulted in 932 records. After removal of duplicate papers, 848 records were screened, ten papers were found by consulting the references of the screened papers, and after excluding the studies that did not meet the inclusion criteria, 59 full-text articles were assessed for eligibility, 18 of which were excluded for the following reasons:
- Only describing study protocol (n = 2);
- Only assessing nutritional status and not body composition (n = 4);
- Only assessing phase-angle variations during radiotherapy (RT) (n = 1);
- Study population including multiple cancer sites (n = 1);
- The final version of the submitted article was not accessible (n = 3).
A total of 41 studies were included in this review, with different methodologies: one systematic review (16), one consensus paper (17), one data descriptor (18), nine randomized trials (6, 11, 19–25), 12 cohort studies (3, 7–9, 15, 26–32), three randomized controlled trials (4, 5, 33), three cross-sectional studies (34–36), two prospective non-randomized trials (37, 38), eight retrospective studies (10, 12–14, 39–42), and one case-control study (43).
Population
The studies included in this review comprised a total of 2,708 participants, 81% were male, and 19% female, with a mean age ranging between 46 and 66 years. Only one study included just male participants (40). The mean baseline BMI ranged from 19.5 to 29.6 kg/m2.
The most frequent exclusion criteria were comorbidities (liver, kidney or cardiac disease, chronic obstructive pulmonary disease, muscular disease, or uncontrolled diabetes mellitus), metastatic disease, treatment with steroids and other malignancies.
Body Composition Assessment
In 15 studies BIA was the assessment method used (3, 5, 7, 8, 20, 21, 23–26, 30, 33, 34, 36, 43), three of which also evaluated skinfolds (23, 25, 30) and one applied bioelectric impedance vector analysis (BIVA) (42). In eight studies, the body composition assessment was made with DXA (4, 6, 9, 11, 19, 22, 29, 31), one of which also included muscle biopsies (9). In two studies, the chosen method was both BIA and DXA (27, 28). CT/ positron-emission tomography-CT (PET-CT) was applied in 11 studies (10, 12–15, 18, 32, 39–42) and one also included MRI (39). In two studies, body composition was assessed with skinfold measures alone (35, 38), one of which also used circumferences (35) and one study only used BIVA (37).
Considering the studies that assessed the patients' body composition with CT/PET, five used the 3rd lumbar vertebra (L3) (10, 14, 18, 32, 42) as a landmark point, one used the 4th lumbar vertebra (L4) (15) and five used the 3rd cervical vertebra (C3) (12, 13, 39–41).
Swartz et al. (12) found a good correlation between the L3 muscle cross-sectional area (CSA) and the C3 muscle CSA in the evaluation of SMM and the method used by these authors was replicated in two other studies (40, 41).
In the studies using C3 as the reference point and calculating the cross-sectional area at L3 (39, 41), the cut-off point for low SMM was <43.2 cm2/m2, and CSA at L3 was calculated with the formula:
CSA at L3 (cm2) = 27.304 + 1.363*CSA at C3 (cm2)−0.671*Age (years) + 0.640*Weight (kg) + 26.442*Sex (Sex = 1 for female, 2 for male).
One study (40) considered the PVM CSA below 815 mm2/m2 as a potential prognostic indicator of postoperative wound complications.
Among the studies using BIA as an assessment method, seven did not report the frequencies applied (3, 5, 8, 21, 26, 28, 37); eight used a frequency of 50 kHz (7, 23–25, 30, 33, 34, 43) and three also used other frequencies besides 50 kHz (20, 27, 36). Only two studies mentioned the equations used in the LBM and FBM (Fat Body Mass) calculations (7, 27). None of the studies referred to complications having an association with any of the methods used in the evaluations, such as pain, discomfort, nausea, or dyspnea.
Tables 1–5 resume the information regarding the body composition assessment methods of each study included in this review.
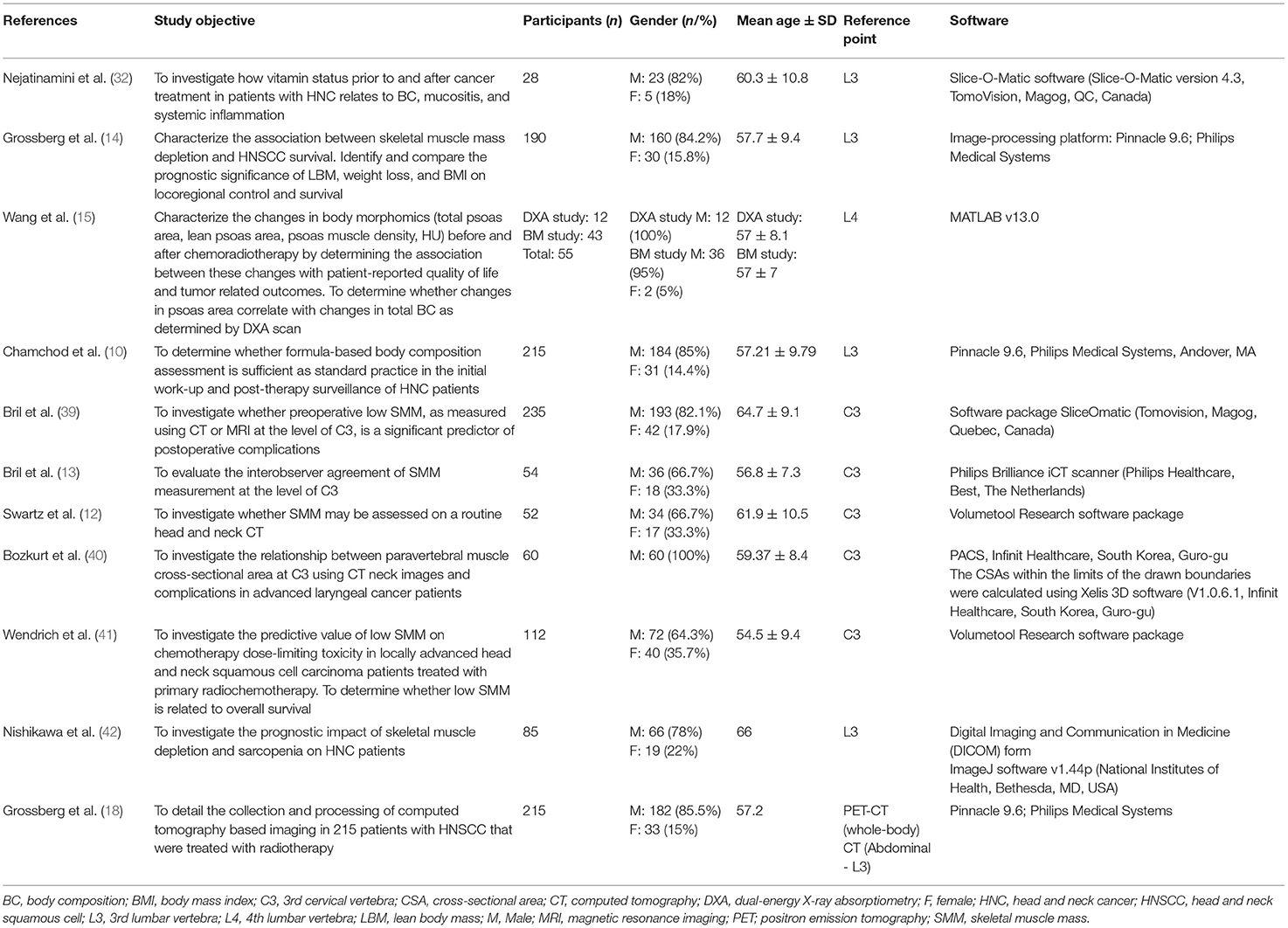
Table 1. Body composition assessment: CT scan.
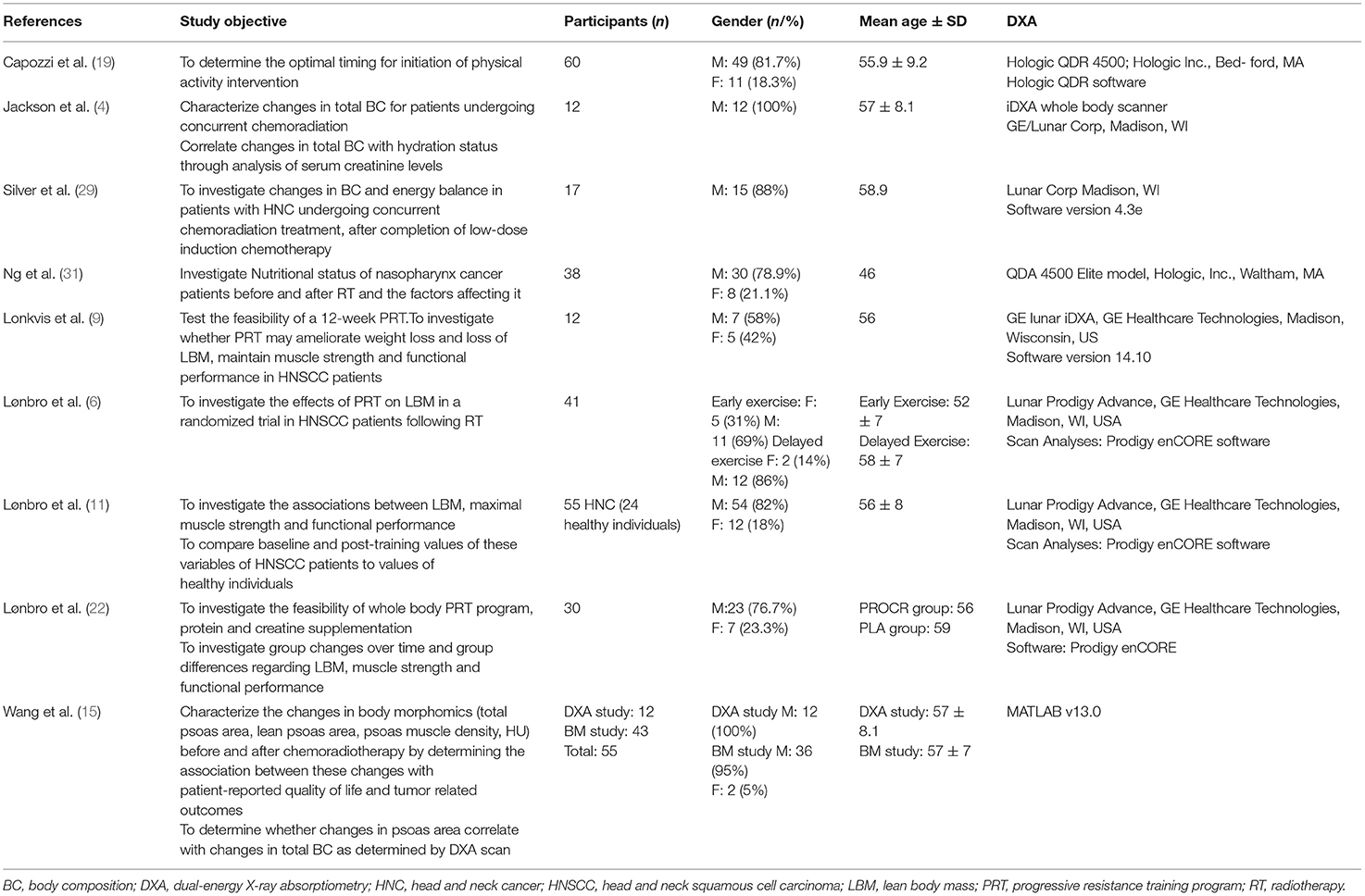
Table 2. Body composition assessment: DXA.
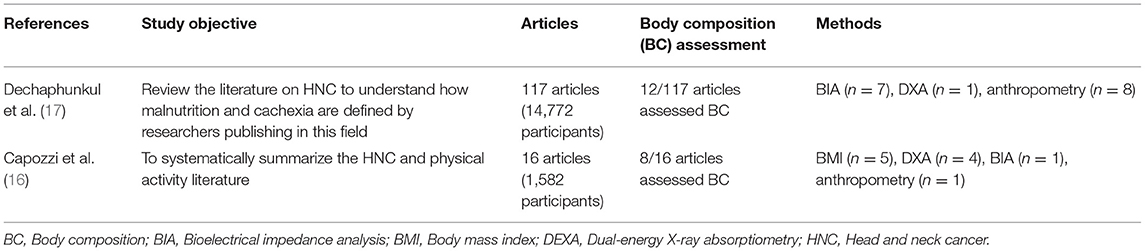
Table 3. Body composition assessment: review articles.
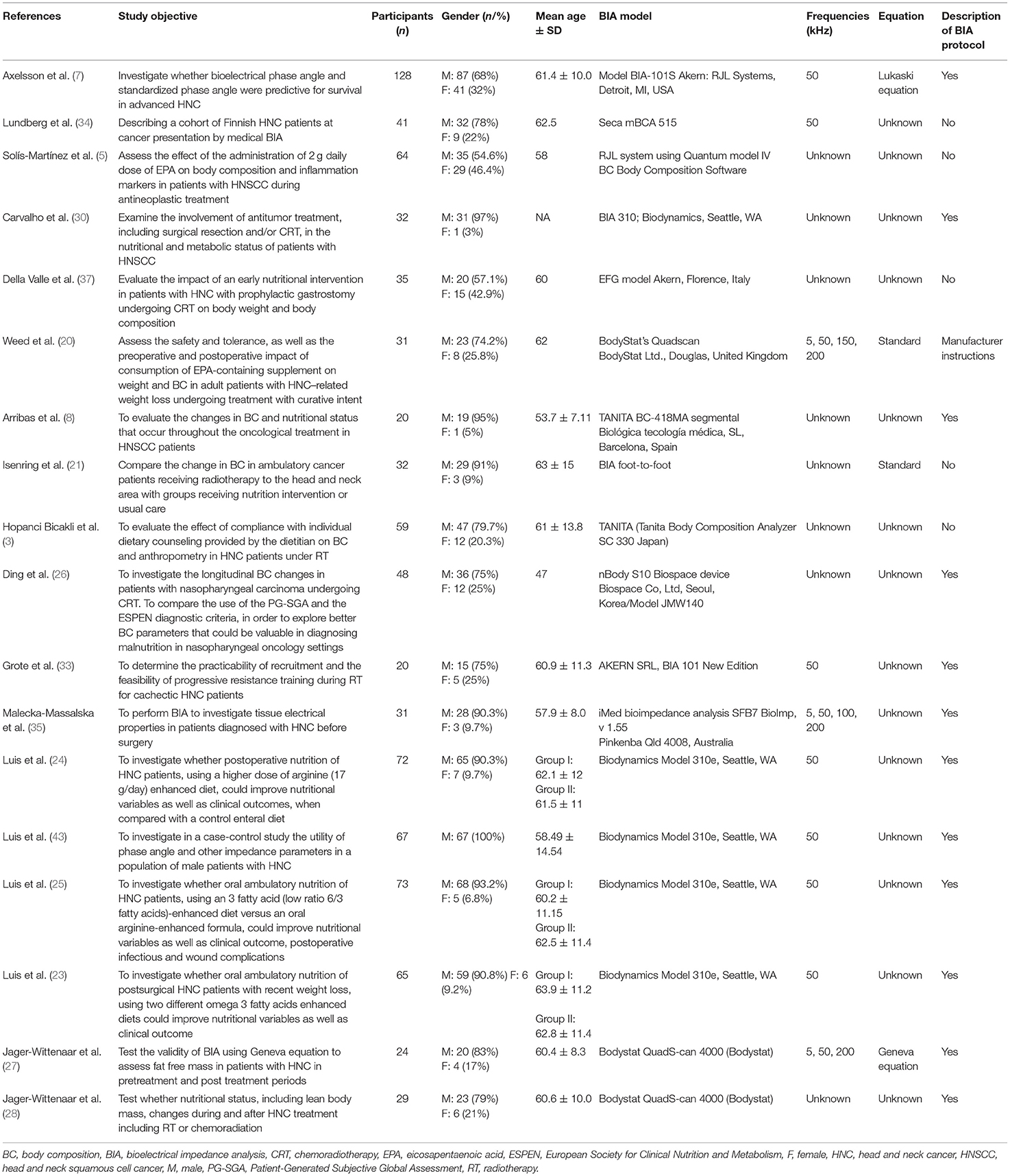
Table 4. Body composition assessment: BIA.

Table 5. Body composition assessment: Anthropometry.
Discussion
Establishing a reliable and easy to use method for body composition assessment in clinical settings remains a challenge. The studies included in this literary review comprised heterogeneous methodologies, objectives as well as methods to assess body composition in HNC patients, which makes it difficult to compare them. We present a review of the existing evidence.
Formula-based body composition assessment (using the Hume formula, Boer formula, and James formula) failed to accurately estimate LBM in HNC patients submitted to radiation treatment when the results were compared with the ones obtained through CT image-based evaluation of L3 (10).
Anthropometry
Anthropometric measures are widely available, easy to assess and inexpensive. Although it is known that BMI is not sensitive to body composition variations and that in obese populations, it is a poor predictor of muscle mass (10), it is still widely used in clinical settings (44). BMI was also evaluated in all the studies included in this review, and its variations during cancer treatments were reported. With the increase in obesity prevalence in the HNC patient population (10), and as it seems that weight loss alone cannot predict LBM loss (8), methods allowing a more detailed evaluation are needed.
Skinfold thickness measurement allows evaluating subcutaneous fat in sites such as biceps, triceps, subscapular, and supra iliac area using a caliper. One study (38) used it as a single method to assess body composition and aimed to compare 33 patients randomized between a group with a percutaneous endoscopic gastrostomy tube (PEG) and a group with a nasogastric tube for feeding evaluation purposes. Although the authors did not refer to any limitations related to the assessment method, it is known to be sensitive to technician skills, type of caliper and prediction equations used (44). One other study (35) used both skinfold thickness and mid-upper arm (MUAC) and mid-arm muscle circumference (MAMC), to evaluate the outcome and nutritional status at the time of the procedure, of 234 patients who underwent PEG, as well as the association of nutritional status/outcome, creating a predictive survival model. Low MUAC was present in 84% of the patients, and low MAMC was present in 75% of the patients. The authors mention that the slow changes of the anthropometric measurements may make this method inadequate to perceive malnutrition early.
BIA
Prediction of body composition based on the electrically conductive properties of both lean tissue (good electrical conductor) and fat mass (poor electrical conductor due to the absence of water) is the principle of BIA (44, 45). BIA measures can use single-frequency (SF), which passes through the extracellular fluid or multi-frequency current (MF), which passes through both the extracellular and the intracellular fluid. BIA is an indirect (43) and quick (7) method that estimates total body water (TBW) and through this estimation determines LBM, assuming a constant hydration factor of 73% (33). Fat body mass is calculated from the weight difference between LBM and body weight (33). It is a validated method to assess body composition in patients with cancer (26, 36) and was used in 17 studies in this review.
Both BIA and skinfold measurements were used in three studies (23, 25, 30) that assessed the changes in body composition and nutritional status during cancer treatment with (23, 25) or without (30) nutrition interventions. Foot-to-foot BIA was used by Isenring et al. (21). Despite providing some additional information when compared to BMI or weight loss, it is a method that does not measure the entire body (46) and for that reason gives incomplete information. BIA and BIVA were both used in one study (34), and one other study only used BIVA (37). BIVA is a qualitative evaluation method of hydration, cell integrity and body cell mass that can contribute with additional information to BIA measures. It seems that this (34) was the first study in the population of HNC patients to include BIVA measures. The authors concluded that both BIA and BIVA are useful tools in the assessment of body composition. BIA is an inexpensive method when compared to more sophisticated ones, easy-to-use, non-invasive, and reproducible (26). It has been considered to have good consistency (particularly FFM) in evaluating body composition during HNC treatments (8). However, to enhance accuracy in LBM variations, the evaluations should be done under the same circumstances and taking into consideration an adequate fluid balance (33, 46) and food intake (33). The following possible sources of error should be taken into account: nutrition status, physical activity, phase of the menstrual cycle, placement of electrodes, limb length, blood chemistry (44), altered fluid balance, edema, endocrine diseases that influence body composition, treatment with growth hormone, acute illness, intensive care treatment, organ transplantation, position of the body, and movements during the measure, type of electrodes, use of oral contraceptives (46). This method also loses accuracy when patients are in the extremes of BMI ranges (<= 16 kg/m2 or >= 35 kg/m2) (7, 46) and although at baseline the patients of the studies included in this review had BMI classifications ranging between normal weight and pre-obesity (with the mean BMI ranging from 21.8 to 29.6 kg/m2), it can be a significant limitation in a population susceptible to weight loss during treatments, as HNC patients are (8). Regarding the hydration status, dehydration, or overhydration may underestimate or overestimate LBM or FBM (46), and the studies results are heterogeneous. Luis et al. (43), identified altered electric properties of the tissues in a population of 32 HNC men, but a total body hydration disorder was excluded when comparing the resistance (R) component with one of healthy subjects. On the other hand, Malecka-Massalska et al. (36) mentions a higher electric current resistance due to a smaller distribution of water between the extracellular and intracellular compartments in HNC patients. As an indirect method, it relies on a large number of prediction equations using linear regression to estimate body composition based on a variety of predetermined variables that may differ between different populations and were derived from healthy individuals (46). Two studies (27, 28) in this review used BIA and DXA. One aimed (27) to validate BIA using Geneva equation to assess LBM in 35 HNC patients. In this study, three frequencies were used (5, 50, and 200 kHz) at three-time points (before the start of cancer treatment, 1 and 4 months after the end of treatment). Each BIA measurement was followed by a DXA scan, and the authors only found a slight underestimation (without statistical significance) of LBM using BIA with Geneva equation and considered that this method is acceptable for LBM assessment in this population. The other study was a prospective cohort study with 29 HNC patients. The authors evaluated if the nutritional status changed during HNC treatment. The same previously mentioned three-time points were evaluated, and the alterations in LBM and FBM were registered. No comparison was made between the results obtained with the two methods.
The tendency toward underestimation of both TBW and LBM has already been identified (45, 46). In regards to the oncological patients, Haverkort et al. (46) concluded that BIA estimations could be useful if used longitudinally.
Taking into consideration raw measurements like R, reactance (X) and phase angle can be an advantage in situations in which the equations do not apply as well as to evaluate tissue hydration status (43, 46). This is important as it seems that different BIA devices measuring the entire body, as long as well-calibrated, will give comparable results. However, more studies will be needed to evaluate the clinical applicability of these data (45).
DXA
DXA measures regional or total body fat, muscle, and bone mineral. It is the gold standard for bone density measurements as well as for determining total body composition (15). It is also a quick method with low radiation exposure and warrants only little preparation and low technical skills (44, 45). DXA is a validated method to assess LBM and body composition in cancer patients (6).
Five studies (4, 6, 11, 19, 22) assessed body composition using DXA to assess the results of a progressive resistance training (PRT) program. The authors reported good feasibility and no complications.
Jackson et al. (4), noted LBM alterations in clinically dehydrated patients and mentioned that the variation in LBM observed on DXA could be a variation in hydration status, as it seems that DXA has failed to determine if changes in hydration occurred in LBM or FBM (4). The variation in hydration status can be a confounding factor, as cancer patients often show fluid status fluctuations, especially during treatments.
Two studies (29, 31) investigated the body composition alterations in HNC patients during cancer treatments and identified the expected decrease in both LBM and FBM.
A single study used both DXA and muscle biopsy (9), in a feasibility test of a 12-week PRT program, including 12 HNC patients. Muscle biopsy was used to analyse further the major alterations registered in LBM during antineoplastic treatments, characterizing muscle fiber types and the enzymes metabolic pathways involved. During treatments, the authors reported a decrease in LBM even during PRT that reverted after the completion of the treatments and mentioned that it was a feasible intervention as a whole and that patients were satisfied with the program.
CT
CT images are usually part of the routine imaging protocol before and after treatment (4) and CT images of L3 are frequently used in studies assessing body composition in cancer patients (8, 42), as the cross-sectional area (CSA) of L3 have a high correlation to whole body muscle mass (32, 42). It was the chosen method for body composition assessment in four studies (10, 14, 15, 32), which all had different objectives.
The images were mostly taken for diagnostic purposes and after completion of the treatments. The authors of one of the studies identified a considerable weight loss (7,1 kg) with equal losses of muscle (3,4 kg) and fat, during cancer treatment (32) and in another study (14), it was reported that low SMM both before and after treatment is associated with decreased overall and cancer-specific survival.
Body morphomics analysis (BMA) was used in one study (15). It is a CT-based technique that analyses the body composition and characterizes the changes in regional body composition, measuring CSA and densities of the psoas muscle. In this study, the BMA measurements at the level of the L4 were compared to DXA results. The authors found similar results between both techniques and univariate analysis revealed that the total psoas area predicted mortality in oropharyngeal cancer patients.
CT imaging of the L3 is not routinely performed during HNC cancer treatments (8, 13, 14). In fact, some studies pinpoint the exclusion of patients without this exam as a study limitation (15, 42). CT images at the level of C3 may be a cost-effective and a reliable alternative (12, 39, 41), that have the advantage of being a routinely performed imaging method in the majority of HNC patients (39) and in addition causing less radiation exposure and therefore less patient burden. In our review, this method showed a significant correlation with L3 measures considering the sum of paravertebral muscles (PVM) and sternocleidomastoid muscles (SCM).
Although one study (13) included in this review has found an excellent interobserver agreement of SMM measurements at the level of C3 for all CSA measures, the authors advise the use of a training data set to minimize errors in the delineation of SMM and single slice selection. The automatic determination of skeletal muscle area (in a window of −29 to +150 Hounsfield Unit) should be preferred instead of visual delineation of the muscles (12), to avoid overestimation of muscle mass.
Lymph node metastases, which are common in HNC patients at the time of diagnosis, can impair SCM measurement (12, 40). In one study this limitation was minimized, with good results, by doubling the area of the SCM that could be measured (12) and in another study by excluding the SCM from the CSA calculations, as CSA at L3 correlates with CSA PVM alone (40).
In Table 6 are resumed the advantages and limitations of each body composition assessment method in HNC.
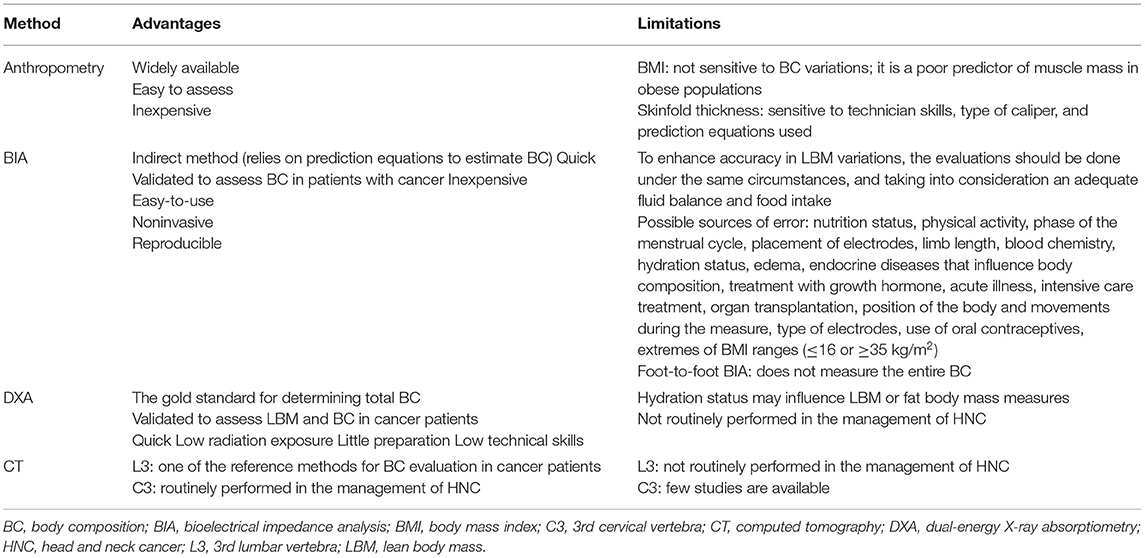
Table 6. Advantages and limitations of each body composition assessment method in HNC.
Limitations
This review has some limitations such as the heterogeneity in methodologies, objectives, and assessment methods of the included HNC studies. Only a few studies had as the primary outcome the evaluation of the body composition and not all the studies included detailed results of the performed assessments. Regarding the methods used, there are no validated methods for this specific patient population. Furthermore, the outcome measures can differ between different nationalities.
Conclusion
This review is a qualitative synthesis of the available evidence regarding body composition assessment methods in HNC patients.
The studies included used different body composition assessment tools, making it challenging to summarize the results.
The reference methods for body composition evaluation in cancer patients are DXA and CT at L3, but these examinations are not routinely performed in the management of HNC. Since variations in body composition in HNC patients are very prevalent, it is of utmost importance to find a tool with low costs and with a low burden to the patient.
Despite the different existing body composition assessment tools, it seems that SMM measurement at the level of C3 may be a reliable method for SMM assessment as it strongly correlates with CSA measures at the level of L3 and it allows a cost-effective body composition assessment without the need for additional radiation exposure.
Data Availability Statement
The datasets analyzed in this manuscript are not publicly available. Requests to access the datasets should be directed to pedrompneves@gmail.com.
Author Contributions
IA-C conceived the study, participated in its design and coordination, draft and authored the manuscript. AM and PR participated in the study design, interpretation of the data, and helped to draft manuscript revisions. PN was responsible for scientific writing and manuscript editing. All authors have read and approved the final manuscript.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
1. Head and Neck Cancer. Union for International Cancer Control, 2014 Review of Cancer Medicines on the WHO List of Essential Medicines (2014).
2. Müller-Richter U, Betz C, Hartmann S, Brands RC. Nutrition management for head and neck cancer patients improves clinical outcome and survival. Nutr Res. (2017) 48:1–8. doi: 10.1016/j.nutres.2017.08.007
3. Hopanci Bicakli D, Ozkaya Akagunduz O, Meseri Dalak R, Esassolak M, Uslu R, Uyar M. The effects of compliance with nutritional counselling on body composition parameters in head and neck cancer patients under radiotherapy. J Nutr Metab. (2017) 2017:8631945. doi: 10.1155/2017/8631945
4. Jackson W, Alexander N, Schipper M, Fig L, Feng F, Jolly S. Characterization of changes in total body composition for patients with head and neck cancerundergoing chemoradiotherapy using dual-energy x-ray absorptiometry. Head Neck. (2014) 36:1356–62. doi: 10.1002/hed.23461
5. Solís-Martínez O, Plasa-Carvalho V, Phillips-Sixtos G, Trujillo-Cabrera Y, Hernández-Cuellar A, Queipo-García GE, et al. Effect of eicosapentaenoic acid on body composition and inflammation markers in patients with head and neck squamous cell cancer from a Public Hospital in Mexico. Nutr Cancer. (2018) 70:663–70. doi: 10.1080/01635581.2018.1460678
6. Lønbro S, Dalgas U, Primdahl H, Johansen J, Nielsen JL, Hermann AP, et al. Progressive resistance training rebuilds lean body mass in head and neck cancer patients-Results from the DAHANCA 25B trial. Radiother Oncol. (2013) 108:314–9. doi: 10.1016/j.radonc.2013.07.002
7. Axelsson L, Silander E, Bosaeus I, Hammerlid E. Bioelectrical phase angle at diagnosis as a prognostic factor for survival in advanced head and neck cancer. Eur Arch Otorhinolaryngol. (2018) 275:2379–86. doi: 10.1007/s00405-018-5069-2
8. Arribas L, Hurtós L, Taberna M, Peiró I, Vilajosana E, Lozano A, et al. Nutritional changes in patients with locally advanced head and neck cancer during treatment. Oral Oncol. (2017) 71:67–74. doi: 10.1016/j.oraloncology.2017.06.003
9. Lonkvist CK, Vinther A, Zerahn B, Rosenbom E, Deshmukh A, et al. Progressive resistance training in head and neck cancer patients undergoing concomitant chemoradiotherapy. Laryngosc Invest Otolaryngol. (2017) 2:295–306. doi: 10.1002/lio2.88
10. Chamchod S, Fuller CD, Mohamed AS, Grossberg A, Messer JA, Heukelom J, et al. Quantitative body mass characterization before and after head and neck cancer radiotherapy: a challenge of height-weight formulae using computed tomography measurement. Oral Oncol. (2016) 61:62–9. doi: 10.1016/j.oraloncology.2016.08.012
11. Lønbro S, Dalgas U, Primdahl H, Johansen J, Nielsen JL, Overgaard J, et al. Lean body mass and muscle function in head and neck cancer patients and healthy individuals–results from the DAHANCA 25 study. Acta Oncol. (2013) 52:1543–51. doi: 10.3109/0284186X.2013.822553
12. Swartz JE, Pothen AJ, Wegner I, Smid EJ, Swart KM, de Bree R, et al. Feasibility of using head and neck CT imaging to assess skeletal muscle mass in head and neck cancer patients. Oral Oncol. (2016) 62:28–33. doi: 10.1016/j.oraloncology.2016.09.006
13. Bril SI, Wendrich AW, Swartz JE, Wegner I, Pameijer F, Smid EJ, et al. Interobserver agreement of skeletal muscle mass measurement on head and neck CT imaging at the level of the third cervical vertebra. Eur Arch Otorhinolaryngol. (2019) 276:1175–82. doi: 10.1007/s00405-019-05307-w
14. Grossberg AJ, Chamchod S, Fuller CD, Mohamed AS, Heukelom J, Eichelberger H, et al. Association of body composition with survival and locoregional control of radiotherapy-treated head and neck squamous cell carcinoma. JAMA Oncol. (2016) 2:782–9. doi: 10.1001/jamaoncol.2015.6339
15. Wang C, Vainshtein JM, Veksler M, Rabban PE, Sullivan JA, Wang SC, et al. Investigating the clinical significance of body composition changes in patients undergoing chemoradiation for oropharyngeal cancer using analytic morphomics. Springerplus. (2016) 5:429. doi: 10.1186/s40064-016-2076-x
16. Capozzi LC, Nishimura KC, McNeely ML, Lau H, Culos-Reed SN. The impact of physical activity on health-related fitness and quality of life for patients with head and neck cancer: a systematic review. Br J Sports Med. (2016) 50:325–38. doi: 10.1136/bjsports-2015-094684
17. Dechaphunkul T, Martin L, Alberda C, Olson K, Baracos V, Gramlich L. Malnutrition assessment in patients with cancers of the head and neck: a call to action and consensus. Crit Rev Oncol Hematol. (2013) 88:459–76. doi: 10.1016/j.critrevonc.2013.06.003
18. Grossberg AJ, Mohamed ASR, Elhalawani H, Bennett WC, Smith KE, Nolan TS, et al. Imaging and clinical data archive for head and neck squamous cell carcinoma patients treated with radiotherapy. Sci Data. (2018) 5:180173. doi: 10.1038/s41597-018-0002-5
19. Capozzi LC, McNeely ML, Lau HY, Reimer RA, Giese-Davis J, Fung TS, et al. Patient-reported outcomes, body composition, and nutrition status in patients with head and neck cancer: results from an exploratory randomized controlled exercise trial. Cancer. (2016) 122:1185–200. doi: 10.1002/cncr.29863
20. Weed HG, Ferguson ML, Gaff RL, Hustead DS, Nelson JL, Voss AC. Lean body mass gain in patients with head and neck squamous cell cancer treated perioperatively with a protein- and energy-dense nutritional supplement containing eicosapentaenoic acid. Head Neck. (2011) 33:1027–33. doi: 10.1002/hed.21580
21. Isenring E, Capra S, Bauer J, Davies PS. The impact of nutrition support on body composition in cancer outpatients receiving radiotherapy. Acta Diabetol. (2003) 40 (Suppl 1):S162–4. doi: 10.1007/s00592-003-0054-6
22. Lønbro S, Dalgas U, Primdahl H, Overgaard J, Overgaard K. Feasibility and efficacy of progressive resistance training and dietary supplements in radiotherapy treated head and neck cancer patients–the DAHANCA 25A study. Acta Oncol. (2013) 52:310–8. doi: 10.3109/0284186X.2012.741325
23. de Luis DA, Izaola O, Aller R, Cuellar L, Terroba MC, Martin T. A randomized clinical trial with two omega 3 fatty acid enhanced oral supplements in head and neck cancer ambulatory patients. Eur Rev Med Pharmacol Sci. (2008) 12:177–81.
24. de Luis DA, Izaola O, Cuellar L, Terroba MC, Martin T, Aller R. Clinical and biochemical outcomes after a randomized trial with a high dose of enteral arginineformula in postsurgical head and neck cancer patients. Eur J Clin Nutr. (2007) 61:200–4. doi: 10.1038/sj.ejcn.1602515
25. de Luis DA, Izaola O, Aller R, Cuellar L, Terroba MC. A randomized clinical trial with oral Immunonutrition (omega3-enhanced formula vs. arginine-enhanced formula) in ambulatory head and neck cancer patients. Ann Nutr Metab. (2005) 49:95–9. doi: 10.1159/000084742
26. Ding H, Dou S, Ling Y, Zhu G, Wang Q, Wu Y, et al. Longitudinal body composition changes and the importance of fat-free mass index in locally advanced nasopharyngeal carcinoma patients undergoing concurrent chemoradiotherapy. Integr Cancer Ther. (2018) 17:1125–31. doi: 10.1177/1534735418807969
27. Jager-Wittenaar H, Dijkstra PU, Earthman CP, Krijnen WP, Langendijk JA, van der Laan BF, et al. Validity of bioelectrical impedance analysis to assess fat-free mass in patients with head and neck cancer: an exploratory study. Head Neck. (2014) 36:585–91. doi: 10.1002/hed.23336
28. Jager-Wittenaar H, Dijkstra PU, Vissink A, Langendijk JA, van der Laan BF, Pruim J, et al. Changes in nutritional status and dietary intake during and after head and neck cancer treatment. Head Neck. (2011) 33:863–70. doi: 10.1002/hed.21546
29. Silver HJ, Dietrich MS, Murphy BA. Changes in body mass, energy balance, physical function, and inflammatory state in patients with locally advanced head and neck cancer treated with concurrent chemoradiation after low-dose induction chemotherapy. Head Neck. (2007) 29:893–900. doi: 10.1002/hed.20607
30. de Carvalho TM, Miguel Marin D, da Silva CA, de Souza AL, Talamoni M, Lima CS, et al. Evaluation of patients with head and neck cancer performing standard treatment in relation to body composition, resting metabolic rate, and inflammatory cytokines. Head Neck. (2015) 37:97–102. doi: 10.1002/hed.23568
31. Ng K, Leung SF, Johnson PJ, Woo J. Nutritional consequences of radiotherapy in nasopharynx cancer patients. Nutr Cancer. (2004) 49:156–61. doi: 10.1207/s15327914nc4902_6
32. Nejatinamini S, Debenham BJ, Clugston RD, Mawani A, Parliament M, Wismer WV, et al. Poor vitamin status is associated with skeletal muscle loss and mucositis in head and neck cancer patients. Nutrients. (2018) 10:E1236. doi: 10.3390/nu10091236
33. Grote M, Maihöfer C, Weigl M, Davies-Knorr P, Belka C. Progressive resistance training in cachectic head and neck cancer patients undergoing radiotherapy: a randomized controlled pilot feasibility trial. Radiat Oncol. (2018) 13:215. doi: 10.1186/s13014-018-1157-0
34. Lundberg M, Nikander P, Tuomainen K, Orell-Kotikangas H, Mäkitie A. Bioelectrical impedance analysis of head and neck cancer patients at presentation. Acta Otolaryngol. (2017) 137:417–20. doi: 10.1080/00016489.2016.1266510
35. Małecka-Massalska T, Smolen A, Morshed K. Altered tissue electrical properties in squamous cell carcinoma in head and neck tumors: preliminary observations. Head Neck. (2013) 35:1101–5. doi: 10.1002/hed.23091
36. Fonseca J, Santos CA, Brito J. Malnutrition and clinical outcome of 234 head and neck cancer patients who underwent percutaneous endoscopic gastrostomy. Nutr Cancer. (2016) 68:589–97. doi: 10.1080/01635581.2016.1158297
37. Della Valle S, Colatruglio S, La Vela V, Tagliabue E, Mariani L, Gavazzi C. Nutritional intervention in head and neck cancer patients during chemo-radiotherapy. Nutrition. (2018) 51–52:95–97. doi: 10.1016/j.nut.2017.12.012
38. Corry J, Poon W, McPhee N, Milner AD, Cruickshank D, Porceddu SV, et al. Randomized study of percutaneous endoscopic gastrostomy versus nasogastric tubes for enteral feeding in head and neck cancer patients treated with (chemo)radiation. J Med Imaging Radiat Oncol. (2008) 52:503–10. doi: 10.1111/j.1440-1673.2008.02003.x
39. Bril SI, Pezier TF, Tijink BM, Janssen LM, Braunius WW, de Bree R. Preoperative low skeletal muscle mass as a risk factor for pharyngocutaneous fistula and decreased overall survival in patients undergoing total laryngectomy. Head Neck. (2019) 41:1745–5. doi: 10.1002/hed.25638
40. Bozkurt G, Elhassan HA, Mahmutoglu AS, Çelebi I, Mcleod RWJ, Soytaş P, et al. Neck muscle mass index as a predictor of post-laryngectomy wound complications. Ann Otol Rhinol Laryngol. (2018) 127:841–7. doi: 10.1177/0003489418798660
41. Wendrich AW, Swartz JE, Bril SI, Wegner I, de Graeff A, Smid EJ, et al. Low skeletal muscle mass is a predictive factor for chemotherapy dose-limiting toxicity in patients with locally advanced head and neck cancer. Oral Oncol. (2017) 71:26–33. doi: 10.1016/j.oraloncology.2017.05.012
42. Nishikawa D, Hanai N, Suzuki H, Koide Y, Beppu S, Hasegawa Y. The impact of skeletal muscle depletion on head and neck squamous cell carcinoma. ORL J Otorhinolaryngol Relat Spec. (2018) 80:1–9. doi: 10.1159/000485515
43. De Luis DA, Aller R, Izaola O, Terroba MC, Cabezas G, Cuellar L. Tissue electric properties in head and neck cancer patients. Ann Nutr Metab. (2006) 50:7–10. doi: 10.1159/000089484
44. Kuriyan R. Body composition techniques. Indian J Med Res. (2018) 148:648–8. doi: 10.4103/ijmr.IJMR_1777_18
45. Borga M, West J, Bell JD, Harvey NC, Romu T, Heymsfield SB, et al. Advanced body composition assessment: from body mass index to body composition profiling. J Investig Med. (2018) 66:1–9. doi: 10.1136/jim-2018-000722
Keywords: head and neck cancer, body composition, cachexia, lean body mass, BIA, DXA, CT
Citation: Almada-Correia I, Neves PM, Mäkitie A and Ravasco P (2019) Body Composition Evaluation in Head and Neck Cancer Patients: A Review. Front. Oncol. 9:1112. doi: 10.3389/fonc.2019.01112
Received: 23 May 2019; Accepted: 07 October 2019;
Published: 07 November 2019.
Edited by:
Johannes Kaanders, Radboud University Nijmegen Medical Centre, NetherlandsReviewed by:
Remco De Bree, University Medical Center Utrecht, NetherlandsMaria Paula Curado, International Prevention Research Institute, France
Copyright © 2019 Almada-Correia, Neves, Mäkitie and Ravasco. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Paula Ravasco, p.ravasco@medicina.ulisboa.pt