 Jungyo Suh
Jungyo Suh Jae Hyun Jung1
Jae Hyun Jung1 Chang Wook Jeong
Chang Wook Jeong Ja Hyeon Ku
Ja Hyeon Ku- 1Department of Urology, Seoul National University College of Medicine, Seoul, South Korea
- 2Department of Urology, Seoul Metropolitan Government- Seoul National University Boramae Medical Center, Seoul, South Korea
Purpose: We performed a study-level meta-analysis to summarize the current evidence on the correlation between pretreatment neutrophil-to-lymphocyte ratios (NLR) and oncological outcomes in each type of management for urothelial carcinoma.
Method: All articles published until February 2017 in PubMed, Scopus, and EMBASE database were collected and reviewed. The current evidence on correlations between pretreatment NLR and oncological outcomes in each type of management for urothelial carcinoma, including transurethral resection of bladder tumor (TURBT), radical cystectomy (RCx), chemotherapy (CTx), and nephroureterectomy (NUx), were summarized.
Results: Thirty-eight studies containing clinical information on 16,379 patients were analyzed in this study. Pooled hazard ratios (HR) and odds ratios (OR) with 95% confidence intervals were calculated after weighing each study. Heterogeneity among the studies and publication bias were assessed. Pretreatment NLR was significantly associated with muscle invasiveness (OR: 4.27), recurrence free survival (RFS, HR: 2.32), and progression-free survival (PFS, HR: 2.45) in TURBT patients. In the RCx patients, high NLR was negatively associated with both disease status (extravesical extension and lymph-node positivity, OR: 1.14 and 1.43, respectively) and oncological outcomes [overall survival (OS), PFS], and cancer specific survival (CSS, HR: 1.18, 1.12, and 1.35, respectively). Pretreatment NLR was negatively correlated with pathologic downstaging (OR: 0.79) and positively correlated with PFS (HR: 1.30) and OS (HR: 1.44) in CTx patients. For patients who underwent NUx, pretreatment NLR was significantly associated with OS (HR: 1.72), PFS (HR: 1.63), and CSS (HR: 1.68).
Conclusions: Pretreatment NLR is a useful biomarker for disease aggressiveness, oncological outcome, and treatment response in the management of patients with urothelial carcinoma. More evidence is needed to clarify these results.
Introduction
Urothelial carcinoma of the bladder is the third most common and the eighth most lethal malignancy in the United States (1), showing a high incidence in developed countries (2). This malignancy originates from normal urothelial cells and can occur in any part of the urinary tract, including the renal pelvis, ureter, bladder, and urethra. The majority of urothelial carcinomas is present in the lower urinary tract, mostly in the bladder. Muscle invasiveness is the most important parameter in the management of bladder urothelial carcinoma. Non-muscle invasive bladder cancer (NMIBC) can be managed by transurethral resection of bladder tumors (TURBT). Muscle-invasive bladder cancer (MIBC) is treated with radical surgery or systemic treatment. The standard treatment for upper urinary tract urothelial carcinoma (UTUC) is radical nephroureterectomy with bladder cuffing. Since urothelial carcinoma shows a variety of clinical manifestations, selecting the proper treatment is one of the most critical issues in the management of patients with urothelial carcinoma.
Recent studies have revealed that the inflammatory response plays an essential role in tumor development, progression, and prognosis (3). Elevation of C-reactive protein (CRP), the presence of some cytokines, and changes in the proportion of white blood cells in the peripheral blood are common findings reflecting the systemic inflammatory response. Among these changes, the peripheral neutrophil-to-lymphocyte ratio (NLR) is one of the most widely studied prognostic biomarkers in many solid tumors because of its easy calculation and cost-effectiveness (4). High NLR tends to be negatively correlated with poor survival in urothelial carcinoma (5). Some studies have suggested a link between high NLR with the pathologic stage of urothelial carcinoma, including muscle invasiveness (6, 7), extravesical extension (8–10), and lymph-node positivity (10, 11). Moreover, recent research has indicated that NLR is a predictive biomarker of treatment response (12). However, one large-scale study did not find a correlation between high preoperative NLRs and extra-vesical extension (11). Thus, the clinical utility of preoperative NLR as a prognostic or predictive biomarker in urothelial carcinoma is still controversial.
Therefore, the objective of this study was to determine the correlation between pretreatment NLRs and oncological outcomes in each type of management for urothelial carcinoma, including TURBT, radical cystectomy (RCx), chemotherapy (CTx), and nephroureterectomy (NUx), through a meta-analysis of published studies.
Materials and Methods
Search Strategy
This study was performed following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. The PubMed, SCOPUS, and EMBASE databases were searched to collect suitable literature published up to February 2017. The search used a combination of “Neutrophil; Lymphocyte; Bladder; Cancer” and “Neutrophil; Lymphocyte; Urothelial; and Cancer” terms. To identify additional shrouded studies, we carefully examined the references of each article.
Inclusion and Exclusion Criteria
Two reviewers (CWJ and CK) screened all titles and abstracts of the initially searched articles. After screening, the full-text articles were separately evaluated by two different reviewers (HHK and JHK) to determine study eligibility. Disagreement on study eligibility was resolved through discussion. The inclusion criteria for eligibility were that the report: (1) investigated urothelial carcinoma, (2) had patient neutrophil-to-lymphocyte ratios, (3) evaluated the relationship between pathologic features and prognosis, and (4) had enough information to calculate odds ratios (OR), or hazard ratios (HR) with 95% confidence intervals (CI). Studies not written in English, case reports, editorial letters or reviews, and those not performed in humans were excluded. If the investigations were conducted on similar patients by the same research group, only the largest and newest article was included in the systematic review.
Data Extraction and Handling
Two reviewers (JHJ and JS) independently extracted information from the selected studies. Data tables were constructed to record all associated data from the texts, tables, and figures of each study. The study information (name of authors, publication year, region), the number of patients, follow-up information, and disease status were obtained. After completing the data tables for each study, both reviewers compared their results and arrived at a consensus for any differences.
Statistical Analysis
The DerSimonian and Laird random-effects model (13) was selected to weigh each study for the meta-analysis. Odds ratios and 95% CIs were used to assess the relationship between NLR and disease status for each specific situation, including muscle invasion in TUR, extravesical extension, or lymph node positivity in radical cystectomy, and pathologic downstaging after neoadjuvant chemotherapy. Hazard ratios and 95% CI were used to estimate the effects of NLR on survival. The heterogeneity of the studies was assessed by Chi-squared tests. Statistical significance was considered for p-values of < 0.05. The I2 statistic was also calculated to determine the heterogeneity of the studies. I2 values larger than 75%, <25%, and between 25 and 75% indicated a high risk of heterogeneity among studies, no heterogeneity, and moderate heterogeneity among studies, respectively.
Publication bias was assessed by funnel plots, rank correlation analysis (Begg test), and linear regression analysis (Egger test). In the funnel plots, a symmetric, inverted funnel shape indicated no publication bias. A p-value < 0.05 by Begg and Egger's test was considered publication bias (Supplementary Data 1). The pooled ORs and HRs of the meta-analyses were calculated using RevMan 5.0 (the Cochrane Collaboration, Copenhagen) software. All statistical analyses were performed with R program 3.5.0 (R Development Core Team, Vienna, http://www.R-project.org).
Data quality and the risk of bias assessment were performed by three investigators (JHK, JS, and JHJ). Each reviewer independently read the published articles and performed a quality assessment based the Newcastle-Ottawa Scale (NOS) (14). The NOS assesses the methodologic quality of each study in three domains: selection of the study groups, comparability of the groups, and ascertainment of exposure and outcome. The risk of bias was stratified on three levels. Quality scores of NOS of >7, 4 to 6, and < 4 indicated high quality, moderate quality, and low-quality studies, respectively. The methodologic quality scores of all included studies are shown in Figure 1. Specific quality assessment scores and data are shown in Supplementary Datas 2, 3.
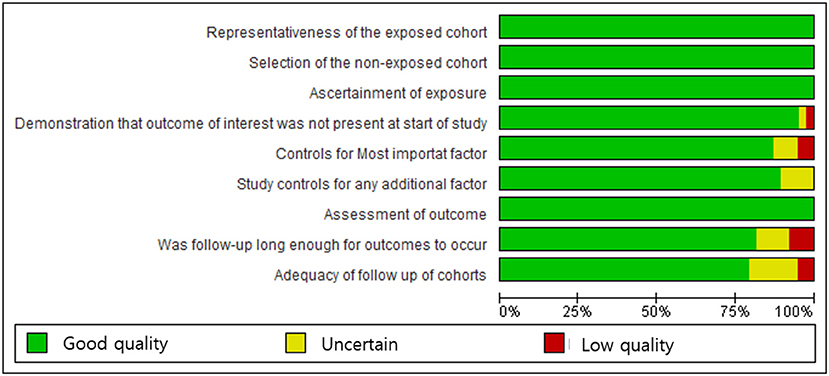
Figure 1. Newcastle-Ottawa Scale graph: the review authors' judgments on each parameter are presented as percentages across all included studies.
Results
Literature Search and Study Selection
A total of 675 articles was primarily identified by database searching. After removing duplicated work, 343 articles remained for screening. After reviewing the running title and abstract by two investigators, 82 articles remained eligible for assessment. Full-text reviews were performed by the two investigators. Finally, 38 studies were selected for meta-analysis (Figure 2), including seven articles on TURBT (6, 7, 15–19), 15 on radical cystectomy (8–12, 20–28), five on chemotherapy (29–33), and 11 on nephroureterectomy for upper ureter urothelial carcinoma (34–44).
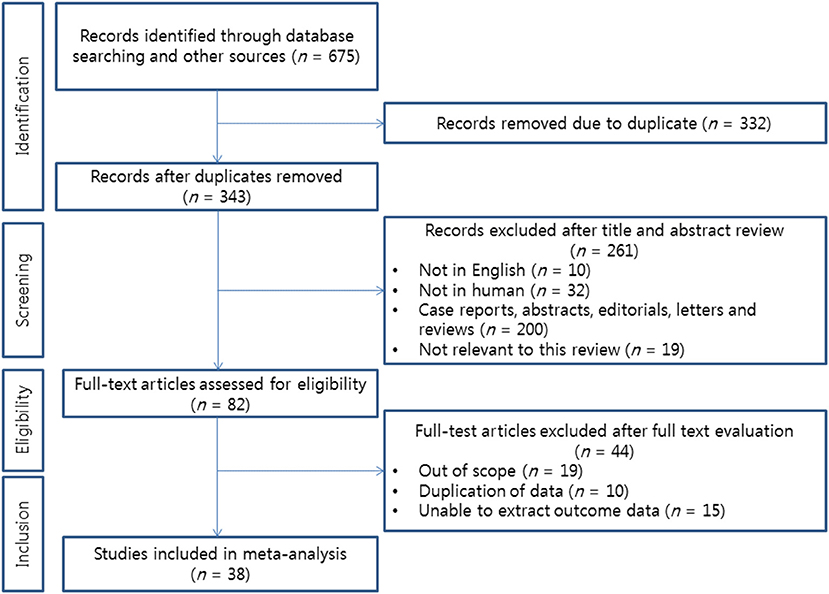
Figure 2. Flow chart of the literature search for this meta-analysis.
Study Characteristics
The characteristics of the selected 38 studies are summarized in Tables 1–4. Seven articles evaluated the clinical significance of NLR in TURBT patients. Only two studies were eligible for assessing the link between NLR and invasiveness in TURBT patients (6, 7). One study performed in Italy was prospectively designed (16). Others were retrospective studies. The majority of those studies were conducted in Turkey (7, 17, 19). However, a study from Japan had the largest study population (15). The cutoff value for NLR varied from 2.2 to 3.89 depending on the study (Table 1). Fifteen articles were eligible for a meta-analysis of radical cystectomies (Table 2). Only extravesical extension, lymph node positivity, and downstaging after NAC had sufficient information to evaluate the correlation between preoperative NLR and disease status. Regarding the parameters of oncological outcomes, cancer-specific survival (CSS), overall survival, and progression-free survival (PRS) had sufficient data for linkage analysis with preoperative NLRs. Most studies set cutoff values for NLR from 2.3 to 5, however, three studies used it as a continuous variable (12, 23, 25). The studies were conducted in many countries. Two large multi-center retrospective studies were performed in the USA (10) and Europe (11). Five articles were eligible for correlation analysis of pretreatment NLRs with oncologic outcomes in chemotherapy patients (Table 3). All studies provided information for overall survival. However, only two studies (31, 32) provided progression-free survival data. European, American, and East Asian (Japan, China) data were included in this meta-analysis. The cutoff values for the NLR ranged from 3 to 5. One study conducted a retrospective analysis from 10 prospective phase II clinical trials (29). Eleven studies were eligible for meta-analysis of NLR association with oncological outcomes in nephroureterectomy patients (Table 4). Eight studies provided enough information to analyze the relationship between preoperative NLRs and PFS (34, 36, 39–42, 44, 46) and CSS (34, 36, 39–42, 44, 46). Most of those studies were conducted in East Asia. Two studies contained information on Western population patients (34, 43). All studies used NLR as a discrete variable, with cutoff values ranging from 2.0 to 3.22.
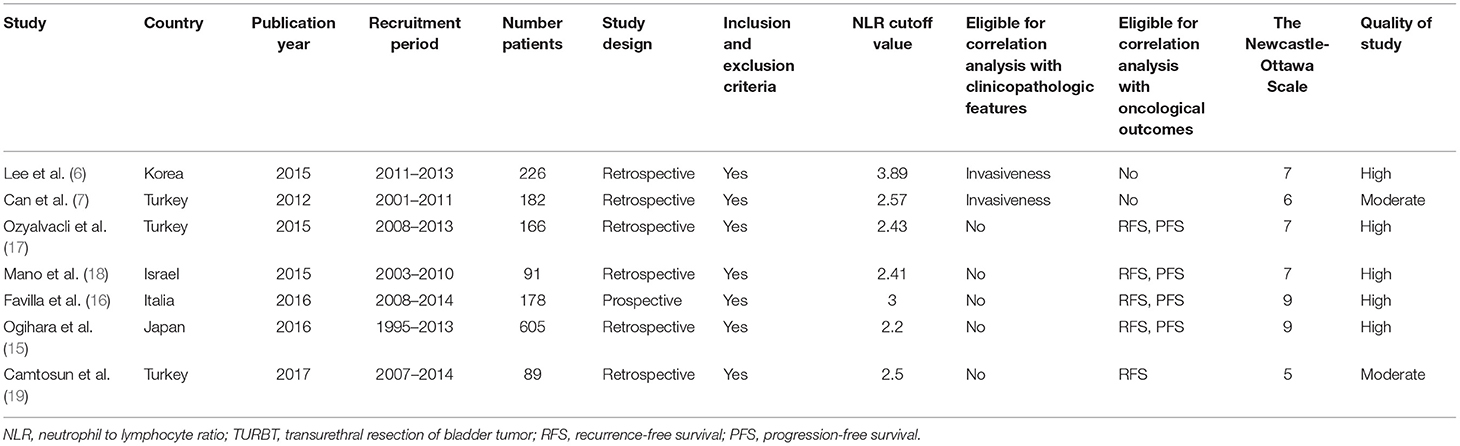
Table 1. Characteristics of studies eligible for TURBT analysis.
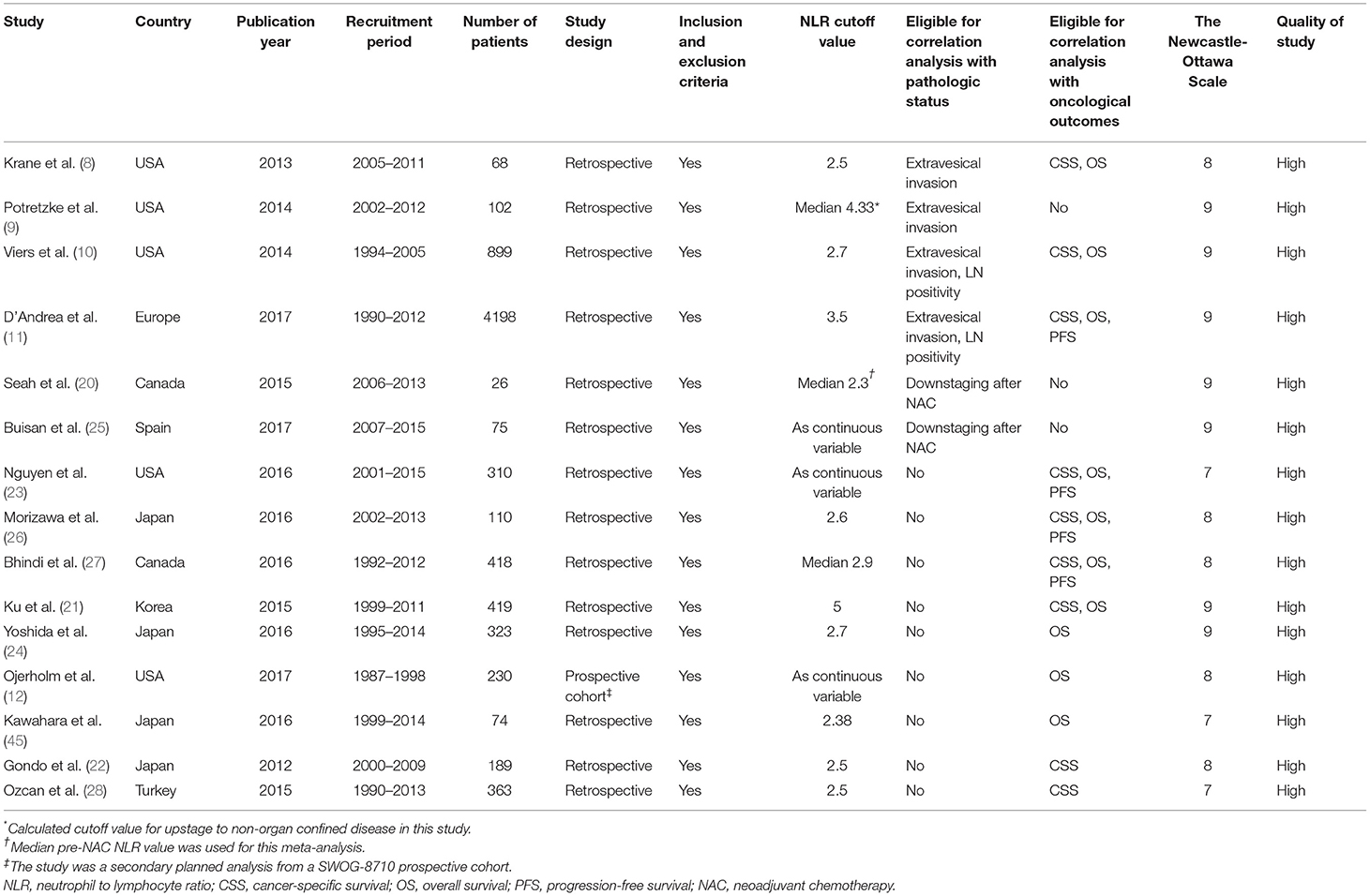
Table 2. Characteristics of studies eligible for radical cystectomy analysis.
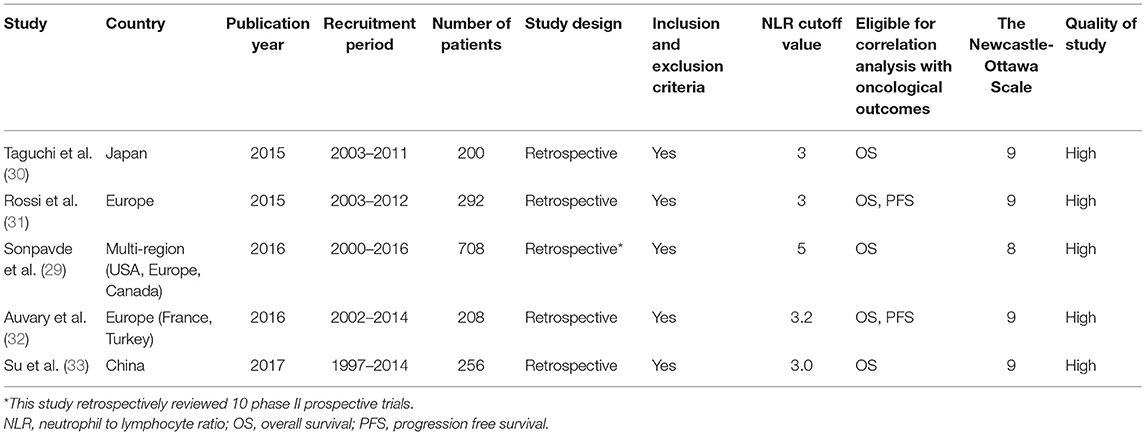
Table 3. Characteristics of studies eligible for chemotherapy analysis.
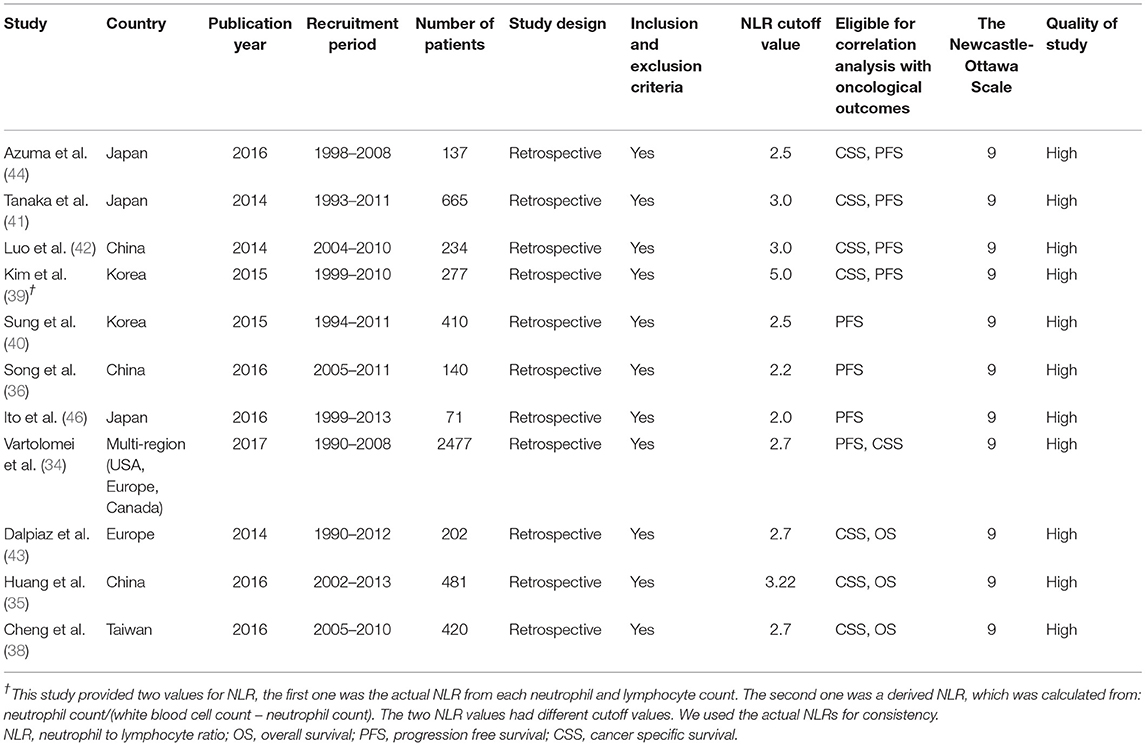
Table 4. Characteristics of studies eligible for nephroureterectomy analysis.
Clinical Significance of NLR in TURBT Patients
Correlation of NLR With Clinicopathologic Feature (Invasiveness)
Only two studies reported the correlation between preoperative NLRs and muscle invasiveness. The pooled OR was 4.27 (95% CI: 1.51–27.31) and moderate level of inter-study heterogeneity was present (I2 = 58%, p = 0.12) (Figure 3A). Publication bias was not assessable owing to the limited number of studies.
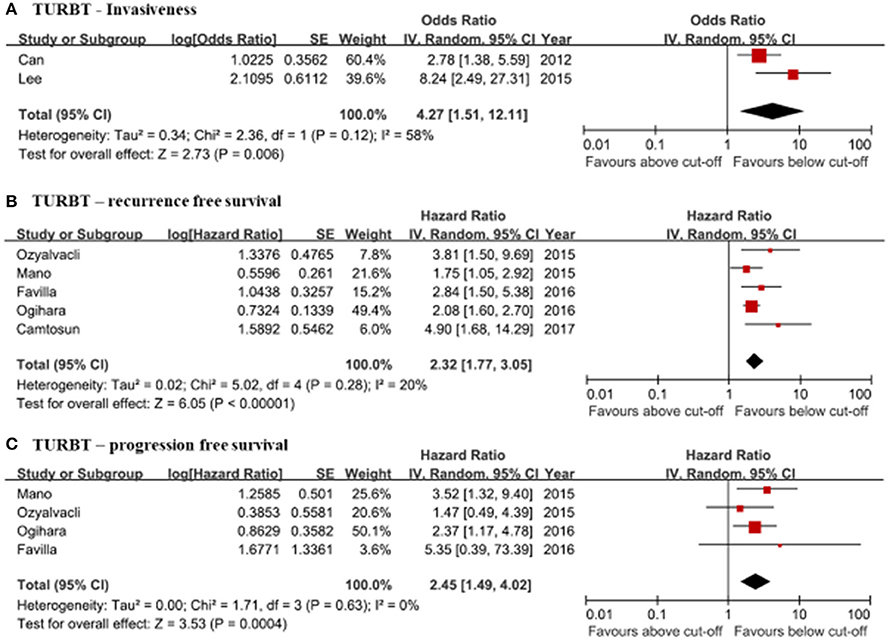
Figure 3. Forrest plots of the relationship between neutrophil-to-lymphocyte ratios (NLR) and clinical information of the TURBT patients. (A) TURBT—Invasiveness. (B) TURBT—recurrence free survival. (C) TURBT—progression free survival.
Correlation of NLR With Oncological Outcomes (Recurrence, Progression)
Five studies were eligible for assessing the relationship between NLRs and RFS (15–19). The results from the meta-analysis of RFS showed a negative association between high NLRs and RFS. The pooled HR was 2.32 (95% CI: 1.77–3.05). Heterogeneity was not present (I2 = 20%, p = 0.28) (Figure 3B). PFS was analyzed using data from four studies (15–18). NLRs above the cutoff value of each study were associated with a higher probability of recurrence (pooled HR: 2.45, 95% CI: 1.49–4.02). Inter-study heterogeneity was not found (I2 = 0%, p = 0.63) (Figure 3C). Publication bias was not founded in either meta-analysis.
Clinical Significance of NLR in Radical Cystectomy Patients
Correlation of NLR With Clinicopathologic Features (Extravesical Extension, Lymph Node Positivity) and Prediction of Clinical Response (Downstaging After Neoadjuvant Chemotherapy)
In four studies (8–11), extravesical extension was evaluated for pathologic up-staging to analyze the correlation with preoperative NLRs. The pooled OR was 1.14 (95% CI: 0.91–1.43) and inter-study heterogeneity was present (I2 = 72%, p = 0.01) (Figure 4A). The correlation between NLRs and lymph node (LN) positivity was assessed in two large, retrospective studies (10, 11). The pooled OR was 1.43 (95% CI: 0.83–2.46). Heterogeneity between the two studies was highly present (I2 = 97%, p < 0.00001) (Figure 4B). Pathologic downstaging after neoadjuvant chemotherapy was evaluated in two studies (20, 25). The pooled OR was calculated to be 0.79 (95% CI: 0.64–0.99). Heterogeneity between the two studies was not present (I2 = 0%, p = 0.67) (Figure 4C). Publication biases could not be assessed due to the limited number of studies for LN positivity and pathologic downstaging after NAC. Publication bias was not found in the meta-analysis of extravesical extension.
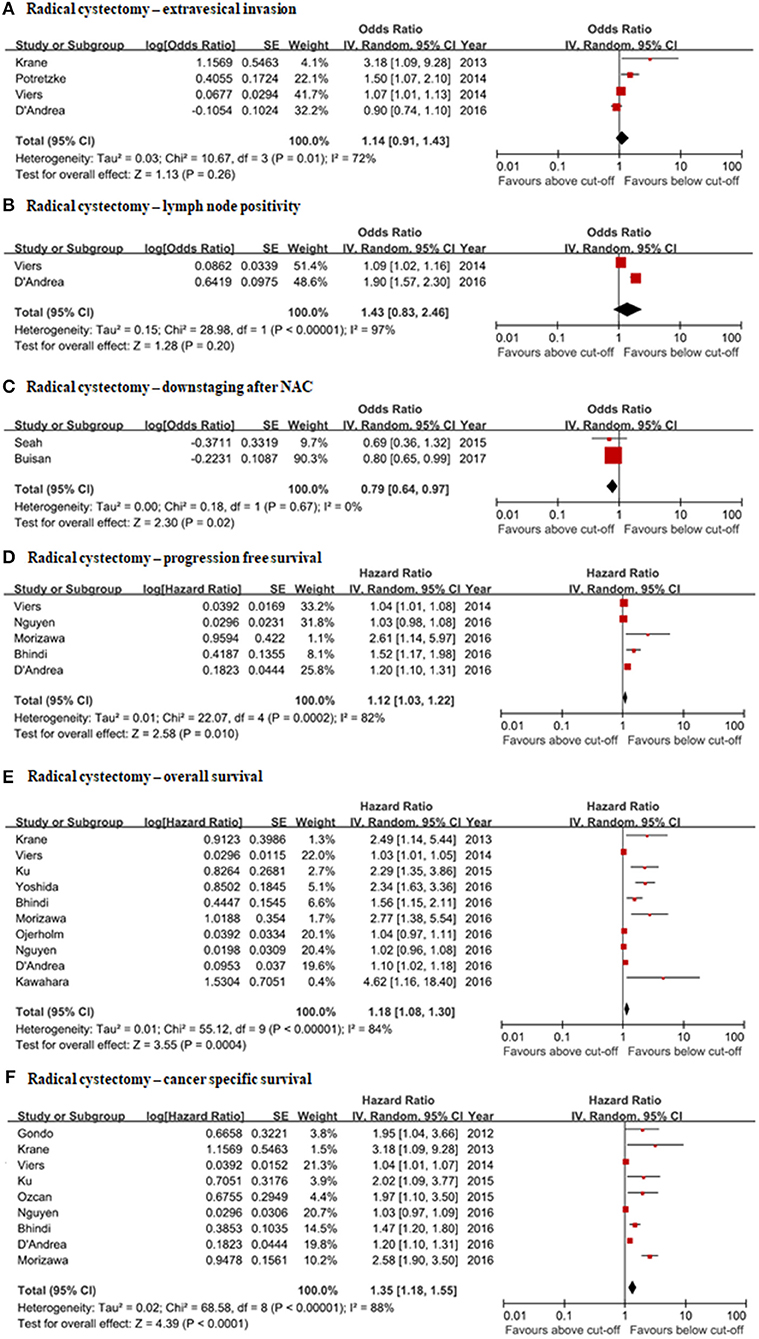
Figure 4. Forrest plots of the relationship between NLRs and clinical information of radical cystectomy patients. (A) Radical cystectomy—extravesical invasion. (B) Radical cystectomy—lymph node positivity. (C) Radical cystectomy—downstaging after NAC. (D) Radical cystectomy—progression free survival. (E) Radical cystectomy—overall survival. (F) Radical cystectomy—cancer specific survival.
Correlation of NLR With Oncological Outcomes (Overall Survival, Cancer-Specific Survival, Progression-Free Survival)
PFS was evaluated by meta-analysis in five studies (10, 11, 23, 26, 27). The pooled hazard ratio was 1.12 (95% CI: 1.03–1.31). There was a high inter-study heterogeneity (I2 = 82%, p = 0.0002) (Figure 4D). Ten studies were eligible for assessing pooled HRs of the NLRs associated with overall survival in radical cystectomy patients (8, 10–12, 21, 23, 24, 26, 27, 45). The pooled HR from meta-analysis was 1.18 (95% CI: 1.08–1.30). There was high inter-study heterogeneity (I2 = 84%, p < 0.00001) (Figure 4E). Nine studies had qualified data for evaluating the correlation of NLR with cancer-specific survival (8, 10, 11, 21–23, 26–28). The pooled HR was 1.35 (95% CI: 1.18–1.55). There was high heterogeneity (I2 = 88%, p < 0.00001) (Figure 4F). Publication bias could not be excluded for OS, CSS, or PFS by inverted funnel plots. Not publishing negative results was suspected.
Clinical Significance of NLR in Chemotherapy Patients
Correlation of NLR With Oncological Outcomes (Progression-Free Survival, Overall Survival)
The pooled analysis of OS was based on five studies (29–33). Pretreatment NLRs were significantly associated with OS (HR: 1.44, 95% CI: 1.28–1.62) (Figure 5A). Only two studies reported information on PFS (31, 32). The pooled hazard ratio of PFS in these studies was 1.30 (95% CI: 1.02–1.64) (Figure 5B). Inter-study heterogeneity was moderately present in the meta-analyses of OS (I2 = 30%, p = 0.22) and PFS (I2 = 64%, p = 0.09). Publication bias was not shown by funnel plots. However, the number of studies for PFS was too small to accurately evaluate.
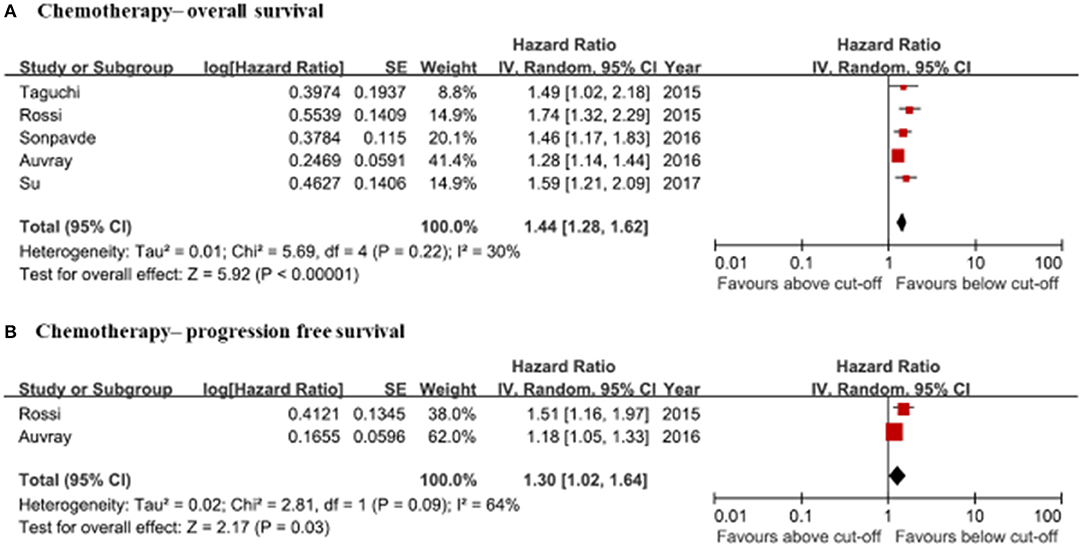
Figure 5. Forrest plots of the relationship between NLRs and clinical information in chemotherapy patients. (A) Chemotherapy—overall survival. (B) Chemotherapy—progression free survival.
Clinical Significance of NLR in Nephroureterectomy Patients
Correlation of NLR With Oncological Outcomes (Progression-Free Survival, Overall Survival, Cancer-Specific Survival)
Pooled hazard ratios were calculated for PFS, OS, and CSS in this meta-analysis. A total of eight studies reported the relationship between preoperative NLRs and PFS. Preoperative NLRs were significantly associated with PFS (HR: 1.63, 95% CI: 1.22–2.18) (Figure 6A). Preoperative NLRs lower than the cut-off value were also associated with better CSS (HR: 1.68, 95% CI: 1.23–2.31) (Figure 6B). The HR of preoperative NLR for overall survival in nephroureterectomy patients was 1.72 (95% CI: 1.31–2.25) based on the meta-analysis results of three eligible studies (Figure 6C). Heterogeneity among these enrolled studies was moderately present for CSS and PFS but was not present for OS. There was a risk of publication bias with a possible risk of not reporting negative results.
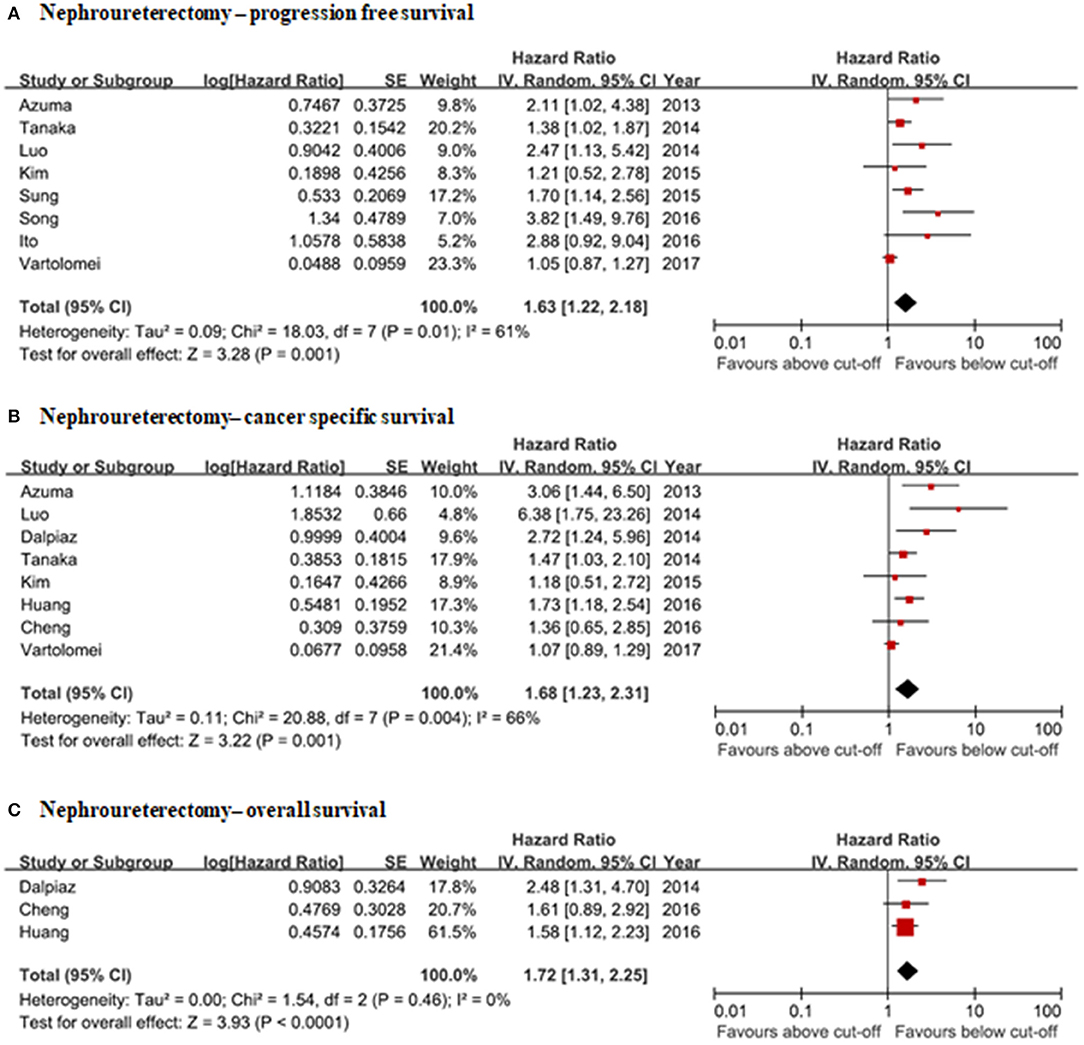
Figure 6. Forrest plots of the relationship between NLRs and clinical information in nephroureterectomy patients. (A) Nephroureterectomy—progression free survival. (B) Nephroureterectomy—cancer specific survival. (C) Nephroureterectomy—overall survival.
Discussion
The neutrophil-to-lymphocyte ratio (NLR) is one of the most actively studied biomarkers for predicting disease status in various cancer types (4, 47). The clinical evidence for the usefulness of NLR as a biomarker in urothelial carcinoma has been accumulating over the last several years, but the topic is still under debate. We conducted a systematic review and meta-analysis to assess the correlation between pretreatment NLRs with pathologic features and the prognosis of urothelial carcinoma patients. This study collected a total of 38 studies containing clinical information and oncological outcomes on 16,379 patients. To our knowledge, this is the largest and latest meta-analysis evaluating the clinical significance of pretreatment NLRs for each specific urothelial carcinoma management situation.
Our evidence supports pretreatment NLR as a useful biomarker for assessing disease aggressiveness and oncological outcomes in TURBT, radical cystectomy, chemotherapy, and nephroureterectomy patients. High NLR was associated with muscle invasiveness (OR: 4.27), poor RFS (HR: 2.32), and PFS (HR: 2.45) in TURBT patients. The major focus of trans-urethral management of superficial bladder urothelial carcinoma is controlling recurrence and progression to muscle-invasive disease. If bladder cancer presents with muscle-invasion and a high risk of progression or recurrence, guidelines recommend radical cystectomy (48, 49). The TURBT procedure always has the risk of failing to obtain the detrusor muscle in the specimen, which is important for proper staging and disease management (50). For this reason, repeated TURBTs should be considered in high-risk bladder NMIBC. The pretreatment NLR before TURBT could provide additional information for selecting the proper treatment strategies for the management of bladder urothelial carcinoma. High NLR values were associated with a higher chance of extravesical extension (OR: 1.14), lymph-node positivity (OR: 1.43), and worse oncological outcomes. The pooled hazard ratios for PFS, CSS, and overall survival were 1.2, 1.35, 1.18, respectively. Patients with low pretreatment NLRs showed better response rates after NAC followed by radical cystectomy, with a higher chance of pathologic down-staging (OR: 0.79). The oncological outcomes of chemotherapy and nephroureterectomy also revealed negative correlations with pretreatment NLRs. We presumed that the correlation between high pretreatment NLRs and poor outcomes after treatment for urothelial carcinoma was a result of more aggressive presentations, however, further well-designed studies are needed to clarify this hypothesis.
Although results from many studies favor NLR as a useful biomarker under many clinical situations, its predictive mechanism remains unclear. We generally accepted that there is a correlation between inflammation and cancer, however, a causal relationship is ambiguous. Chronic inflammation caused by infection or toxic materials leads to tumorigenesis in many solid tumors. About 20% of tumors are associated with prior viral, microbial, and parasite infections, including infections with the hepatitis virus, human papillomavirus, Helicobacter pylori, and Schistosoma haematobium (51). Additionally, recent studies showed an inverse correlation between non-steroid anti-inflammatory drugs (NSAID) and cancer risk (52). Inflammatory cells are recruited to the tumor microenvironment in the situation of tumor advancement with invasion or the distant migration of tumor cells (53). The cancer-related immune response is paradoxical. Molecular evidence has demonstrated that tumor-infiltrated inflammatory cells eradicate nascent tumors (54). However, some studies have shown that increased systemic inflammation enhanced tumor development, progression, and metastasis (55). Because of the unclear mechanism of the NLR to predict disease prognosis, the clinical utility of the NLR is very limited. Moreover, we have only limited evidence for the association of NLR and prognosis compared to important prognostic factors, such as pathologic stage and surgical margins. Thus, a targeted study evaluating the prognostic impact of NLR after adjusting for covariable factors is needed.
The definition of an optimum NLR value is another problem. In studies included in this meta-analysis, the cutoff value of NLR varied from 2.0 to 5.0 and some studies even used NLR as a continuous variable (12, 23, 25). In addition, NLR is a dynamic marker of the systemic immune response. Thus, we could not judge the optimal cutoff value easily. NLR is not only related to bladder cancer but also related to many benign and malignant diseases. Therefore, it can be increased without the advancement of tumors. Recently, some studies used a derived NLR introduced by Proctor et al. (56) that makes the clinical utility of NLR more complex.
This systematic review and meta-analysis had some limitations. First, most studies on the relationship of NLR with many clinical parameters and oncological outcomes were retrospectively designed. There was no prospective, randomized controlled study that met our search criteria. Variable differences in study design, patient numbers, the definition of oncological outcomes, and NLR cutoff values also affected the inter-study heterogeneity. Publication bias was another limitation, especially in the sub-group analysis of cystectomy, and nephroureterectomy patients. In addition, we could not include immune-oncological agent targeted studies, which are promising treatments for advanced urothelial carcinoma and thought to be strongly correlated with systemic immune responses. Finally, this meta-analysis used articles written in English only. Thus, we could not exclude language bias in the favorable positive results. Despite these limitations, this study-level meta-analysis provided a generalized view of NLRs on disease aggressiveness, oncological outcomes, and treatment responses in patients with urothelial carcinoma.
Conclusion
This study-level meta-analysis showed that pretreatment NLRs were useful biomarkers for disease aggressiveness, oncological outcomes, and treatment responses in the management of urothelial carcinoma. However, inter-study heterogeneity, the possibility of publication bias, the limited number of eligible studies, and no randomized controlled study were limitations of the study. A large, well-designed, prospective study is needed to provide clear evidence that the pretreatment NLR is a useful biomarker for urothelial carcinoma.
Author Contributions
JK: conception and design. CJ, CK, HK, and JK: collection and assembly of data. JS: manuscript writing. All authors data analysis and interpretation, final approval of manuscript, and accountable for all aspects of the work.
Funding
This study was supported by a grant (2016R1A2B4011623) from the National Research Foundation (NRF) funded by the Ministry of Science, ICT, and Future Planning (MSIP), Republic of Korea. This work was supported by a Basic Science Research Program through the National Research Foundation of Korea (NRF) funded by the Ministry of Education (NRF-2019R1F1A1050507).
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Supplementary Material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fonc.2019.01365/full#supplementary-material
Supplementary Data 1. Funnel plots of each analysis.
Supplementary Data 2. New Castle Ottawa Scale Summary: The review authors' judgments on each parameter for each included study.
Supplementary Data 3. The New Castle Ottawa Scale detailed review of each study.
References
1. Siegel RL, Miller KD, Jemal A. Cancer statistics, 2019 (US statistics). CA Cancer J Clin. (2019) 69:7–34. doi: 10.3322/caac.21551
2. Torre LA, Bray F, Siegel RL, Ferlay J, Lortet-tieulent J, Jemal A. Global cancer statistics, 2012. CA Cancer J Clin. (2015) 65:87–108. doi: 10.3322/caac.21262
3. Diakos CI, Charles KA, Mcmillan DC, Clarke SJ. Cancer-related infl ammation and treatment eff ectiveness. Lancet Oncol. (2014) 15:e493–503. doi: 10.1016/S1470-2045(14)70263-3
4. Templeton AJ, McNamara MG, Šeruga B, Vera-Badillo FE, Aneja P, Ocaña A, et al. Prognostic role of neutrophil-to-lymphocyte ratio in solid tumors: a systematic review and meta-analysis. J Natl Cancer Inst. (2014) 106:dju124. doi: 10.1093/jnci/dju124
5. Marchioni M, Primiceri G, Ingrosso M, Filograna R, Castellan P, De Francesco P, et al. The clinical use of the neutrophil to lymphocyte ratio (NLR) in urothelial cancer: a systematic review. Clin Genitourin Cancer. (2016) 14:473–84. doi: 10.1016/j.clgc.2016.04.008
6. Lee SM, Russell A, Hellawell G. Predictive value of pretreatment inflammation-based prognostic scores (neutrophil-to-lymphocyte ratio, platelet-to-lymphocyte ratio, and lymphocyte-to-monocyte ratio) for invasive bladder carcinoma. Korean J Urol. (2015) 56:749–55. doi: 10.4111/kju.2015.56.11.749
7. Can C, Baseskioglu B, Yilmaz M, Colak E, Ozen A, Yenilmez A. Pretreatment parameters obtained from peripheral blood sample predicts invasiveness of bladder carcinoma. Urol Int. (2012) 89:468–72. doi: 10.1159/000343278
8. Krane LS, Richards KA, Kader AK, Davis R, Balaji KC, Hemal AK. Preoperative neutrophil/lymphocyte ratio predicts overall survival and extravesical disease in patients undergoing radical cystectomy. J Endourol. (2013) 27:1046–50. doi: 10.1089/end.2012.0606
9. Potretzke A, Hillman L, Wong K, Shi F, Brower R, Mai S, et al. NLR is predictive of upstaging at the time of radical cystectomy for patients with urothelial carcinoma of the bladder. Urol Oncol Semin Orig Investig. (2014) 32:631–6. doi: 10.1016/j.urolonc.2013.12.009
10. Viers BR, Boorjian SA, Frank I, Tarrell RF, Thapa P, Karnes RJ, et al. Pretreatment neutrophil-to-lymphocyte ratio is associated with advanced pathologic tumor stage and increased cancer-specific mortality among patients with urothelial carcinoma of the bladder undergoing radical cystectomy. Eur Urol. (2014) 66:1157–64. doi: 10.1016/j.eururo.2014.02.042
11. D'Andrea D, Moschini M, Gust KM, Abufaraj M, Özsoy M, Mathieu R, et al. Lymphocyte-to-monocyte ratio and neutrophil-to-lymphocyte ratio as biomarkers for predicting lymph node metastasis and survival in patients treated with radical cystectomy. J Surg Oncol. (2017) 115:455–61. doi: 10.1002/jso.24521
12. Ojerholm E, Smith A, Hwang WT, Baumann BC, Tucker KN, Lerner SP, et al. Neutrophil-to-lymphocyte ratio as a bladder cancer biomarker: assessing prognostic and predictive value in SWOG 8710. Cancer. (2017) 123:794–801. doi: 10.1002/cncr.30422
13. DerSimonian R, Laird N. Meta-analysis in clinical trials. Control Clin Trials. (1986) 7:177–88. doi: 10.1016/0197-2456(86)90046-2
14. Wells GA, Shea B, O'Connell D, Peterson J, Welch V, Losos M, et al. The Newcastle-Ottawa Scale (NOS) for Assessing the Quality of Nonrandomised Studies in Meta-Analyses. Available online at: http://www.ohri.ca/programs/clinical_epidemiology/oxford.asp (accessed November 25, 2019).
15. Ogihara K, Kikuchi E, Yuge K, Yanai Y, Matsumoto K, Miyajima A, et al. The preoperative neutrophil-to-lymphocyte ratio is a novel biomarker for predicting worse clinical outcomes in non-muscle invasive bladder cancer patients with a previous history of smoking. Ann Surg Oncol. (2016) 23:1039–47. doi: 10.1245/s10434-016-5578-4
16. Favilla V, Castelli T, Urzì D, Reale G, Privitera S, Salici A, et al. Neutrophil to lymphocyte ratio, a biomarker in non-muscle invasive bladder cancer: a single-institutional longitudinal study. Int Braz J Urol. (2016) 42:685–93. doi: 10.1590/S1677-5538.IBJU.2015.0243
17. Ozyalvacli ME, Ozyalvacli G, Kocaaslan R, Cecen K, Uyeturk U, Kemahli E, et al. Neutrophil-lymphocyte ratio as a predictor of recurrence and progression in patients with high-grade pT1 bladder cancer. Can Urol Assoc J. (2015) 9:126–31. doi: 10.5489/cuaj.2523
18. Mano R, Baniel J, Shoshany O, Margel D, Bar-on T, Nativ O, et al. Neutrophil-to-lymphocyte ratio predicts progression and recurrence of non – muscle-invasive bladder cancer. Urol Oncol Semin Orig Investig. (2015) 33:67.e1–e7. doi: 10.1016/j.urolonc.2014.06.010
19. Camtosun A, Celik H, Altintas R, Topcu I, Tasdemir C. Does preoperative neutrophil-to-lymphocyte ratio have a value in predicting recurrence in bladder tumour after intravesical BCG treatment? Biomed Res. (2017) 28:36–40. Available online at: https://www.alliedacademies.org/articles/does-preoperative-neutrophiltolymphocyte-ratio-have-a-value-in-predicting-recurrence-in-bladder-tumour-after-intravesical-bcg-trea.html
20. Seah JA, Leibowitz-Amit R, Atenafu EG, Alimohamed N, Knox JJ, Joshua AM, et al. Neutrophil-lymphocyte ratio and pathological response to neoadjuvant chemotherapy in patients with muscle-invasive bladder cancer. Clin Genitourin Cancer. (2015) 13:e229–33. doi: 10.1016/j.clgc.2015.02.001
21. Ku JH, Kang M, Kim HS, Jeong CW, Kwak C, Kim HH. The prognostic value of pretreatment of systemic inflammatory responses in patients with urothelial carcinoma undergoing radical cystectomy. Br J Cancer. (2015) 112:461–7. doi: 10.1038/bjc.2014.631
22. Gondo T, Nakashima J, Ohno Y, Choichiro O, Horiguchi Y, Namiki K, et al. Prognostic value of neutrophil-to-lymphocyte ratio and establishment of novel preoperative risk stratification model in bladder cancer patients treated with radical cystectomy. Urology. (2012) 79:1085–91. doi: 10.1016/j.urology.2011.11.070
23. Nguyen DP, Al Awamlh BAH, O'Malley P, Khan F, Lewicki PJE, Golombos DM, et al. Factors impacting the occurrence of local, distant and atypical recurrences after robot-assisted radical cystectomy: a detailed analysis of 310 patients. J Urol. (2016) 196:1390–6. doi: 10.1016/j.juro.2016.05.101
24. Yoshida T, Kinoshita H, Yoshida K, Mishima T, Yanishi M, Komai Y, et al. Perioperative change in neutrophil-lymphocyte ratio predicts the overall survival of patients with bladder cancer undergoing radical cystectomy. Jpn J Clin Oncol. (2016) 46:1162–7. doi: 10.1093/jjco/hyw129
25. Buisan O, Orsola A, Areal J, Font A, Oliveira M, Martinez R, et al. Low pretreatment neutrophil-to-lymphocyte ratio predicts for good outcomes in patients receiving neoadjuvant chemotherapy before radical cystectomy for muscle invasive bladder cancer. Clin Genitourin Cancer. (2017) 15:145–51.e2. doi: 10.1016/j.clgc.2016.05.004
26. Morizawa Y, Miyake M, Shimada K, Hori S, Tatsumi Y, Nakai Y, et al. Neutrophil-to-lymphocyte ratio as a detection marker of tumor recurrence in patients with muscle-invasive bladder cancer after radical cystectomy. Urol Oncol Semin Orig Investig. (2016) 34:257.e11–e17. doi: 10.1016/j.urolonc.2016.02.012
27. Bhindi B, Hermanns T, Wei Y, Yu J, Richard PO, Wettstein MS, et al. Identification of the best complete blood count-based predictors for bladder cancer outcomes in patients undergoing radical cystectomy. Br J Cancer. (2016) 114:207–12. doi: 10.1038/bjc.2015.432
28. Ozcan C, Telli O, Ozturk E, Suer E, Gokce MI, Gulpinar O, et al. The prognostic significance of preoperative leukocytosis and neutrophil-to-lymphocyte ratio in patients who underwent radical cystectomy for bladder cancer. J Can Urol Assoc. (2015) 9:E789–94. doi: 10.5489/cuaj.3061
29. Sonpavde G, Pond GR, Rosenberg JE, Bajorin DF, Choueiri TK, Necchi A, et al. Improved 5-factor prognostic classification of patients receiving salvage systemic therapy for advanced urothelial carcinoma. J Urol. (2015) 195:1–6. doi: 10.1016/j.juro.2015.07.111
30. Taguchi S, Nakagawa T, Matsumoto A, Nagase Y, Kawai T, Tanaka Y, et al. Pretreatment neutrophil-to-lymphocyte ratio as an independent predictor of survival in patients with metastatic urothelial carcinoma: a multi-institutional study. Int J Urol. (2015) 22:638–43. doi: 10.1111/iju.12766
31. Rossi L, Santoni M, Crabb SJ, Scarpi E, Burattini L, Chau C, et al. High neutrophil-to-lymphocyte ratio persistent during first-line chemotherapy predicts poor clinical outcome in patients with advanced urothelial cancer. Ann Surg Oncol. (2015) 22:1377–84. doi: 10.1245/s10434-014-4097-4
32. Auvray M, Elaidi R, Ozguroglu M, Guven S, Gauthier H, Culine S, et al. Prognostic value of baseline neutrophil-to-lymphocyte ratio in metastatic urothelial carcinoma patients treated with first-line chemotherapy: a large multicenter study. Clin Genitourin Cancer. (2017) 15:e469–76. doi: 10.1016/j.clgc.2016.10.013
33. Su YL, Hsieh MC, Chiang PH, Sung MT, Lan J, Luo HL, et al. Novel inflammation-based prognostic score for predicting survival in patients with metastatic urothelial carcinoma. PLoS ONE. (2017) 12:e0169657. doi: 10.1371/journal.pone.0169657
34. Vartolomei MD, Mathieu R, Margulis V, Karam JA, Rouprêt M, Lucca I, et al. Promising role of preoperative neutrophil-to-lymphocyte ratio in patients treated with radical nephroureterectomy. World J Urol. (2017) 35:121–130. doi: 10.1007/s00345-016-1848-9
35. Huang J, Yuan Y, Wang Y, Zhang J, Kong W, Chen H, et al. Prognostic value of preoperative plasma fibrinogen level and platelet-to-lymphocyte ratio (F-PLR) in patients with localized upper tract urothelial carcinoma. Oncotarget. (2017) 8:36761–71. doi: 10.18632/oncotarget.13611
36. Song X, Zhang GM, Ma XC, Luo L, Li B, Chai DY, et al. Comparison of preoperative neutrophil–lymphocyte, lymphocyte–monocyte, and platelet–lymphocyte ratios in patients with upper urinary tract urothelial carcinoma undergoing radical nephroureterectomy. Onco Targets Ther. (2016) 9:1399–407. doi: 10.2147/OTT.S97520
37. Ito K, Asakuma J, Kuroda K, Tachi K, Sato A, Horiguchi A, et al. Preoperative risk factors for extraurothelial recurrence in N0M0 patients with renal pelvic cancer treated by radical nephroureterectomy. Mol Clin Oncol. (2016) 4:530–6. doi: 10.3892/mco.2016.754
38. Cheng YC, Huang CN, Wu WJ, Li CC, Ke HL, Li WM, et al. The prognostic significance of inflammation-associated blood cell markers in patients with upper tract urothelial carcinoma. Ann Surg Oncol. (2016) 23:343–51. doi: 10.1245/s10434-015-4781-z
39. Kim M, Chul K, Woo M, Choi S. Prognostic value of systemic inflammatory responses in patients with upper urinary tract urothelial carcinoma. World J Urol. (2015) 33:1439–57. doi: 10.1007/s00345-015-1484-9
40. Sung HH, Gyun Jeon H, Jeong BC, Seo SI, Jeon SS, Choi HY, et al. Clinical significance of prognosis using the neutrophil-lymphocyte ratio and erythrocyte sedimentation rate in patients undergoing radical nephroureterectomy for upper urinary tract urothelial carcinoma. BJU Int. (2015) 115:587–94. doi: 10.1111/bju.12846
41. Tanaka N, Kikuchi E, Kanao K, Matsumoto K, Shirotake S, Miyazaki Y, et al. A multi-institutional validation of the prognostic value of the neutrophil-to-lymphocyte ratio for upper tract urothelial carcinoma treated with radical nephroureterectomy. Ann Surg Oncol. (2014) 21:4041–8. doi: 10.1245/s10434-014-3830-3
42. Luo HL, Chen YT, Chuang YC, Cheng YT, Lee WC, Kang CH, et al. Subclassification of upper urinary tract urothelial carcinoma by the neutrophil-to-lymphocyte ratio (NLR) improves prediction of oncological outcome. BJU Int. (2014) 113:144–9. doi: 10.1111/bju.12582
43. Dalpiaz O, Ehrlich GC, Mannweiler S, Hernández JMM, Gerger A, Stojakovic T, et al. Validation of pretreatment neutrophil-lymphocyte ratio as a prognostic factor in a European cohort of patients with upper tract urothelial carcinoma. BJU Int. (2014) 114:334–9. doi: 10.1038/bjc.2014.180
44. Azuma T, Matayoshi Y, Odani K, Sato Y, Sato Y, Nagase Y, et al. Preoperative neutrophil-lymphocyte ratio as an independent prognostic marker for patients with upper urinary tract urothelial carcinoma. Clin Genitourin Cancer. (2013) 11:337–41. doi: 10.1016/j.clgc.2013.04.003
45. Kawahara T, Furuya K, Nakamura M, Sakamaki K, Osaka K, Ito H, et al. Neutrophil-to-lymphocyte ratio is a prognostic marker in bladder cancer patients after radical cystectomy. BMC Cancer. (2016) 16:185. doi: 10.1186/s12885-016-2219-z
46. Ito K, Kuroda K, Asakuma J, Hamada S, Tachi K, Tasaki S, et al. Preoperative risk factors for extraurothelial recurrence in patients with ureteral cancer treated with radical nephroureterectomy. Mol Clin Oncol. (2015) 4:530–6. doi: 10.1016/j.juro.2013.12.048
47. Yang J-J. Prognostic significance of neutrophil to lymphocyte ratio in pancreatic cancer: a meta-analysis. World J Gastroenterol. (2015) 21:2807. doi: 10.3748/wjg.v21.i9.2807
48. Babjuk M, Böhle A, Burger M, Capoun O, Cohen D, Compérat EM, et al. EAU guidelines on non-muscle-invasive urothelial carcinoma of the bladder: update 2016. Eur Urol. (2017) 71:447–61. doi: 10.1016/j.eururo.2016.05.041
49. Power NE, Izawa J. Comparison of guidelines on non-muscle invasive bladder cancer (EAU, CUA, AUA, NCCN, NICE). Bl Cancer. (2016) 2:27–36. doi: 10.3233/BLC-150034
50. Herr HW, Donat SM. Quality control in transurethral resection of bladder tumours. BJU Int. (2008) 102:1242–6. doi: 10.1111/j.1464-410X.2008.07966.x
51. Plummer M, de Martel C, Vignat J, Ferlay J, Bray F, Franceschi S. Global burden of cancers attributable to infections in 2012: a synthetic analysis. Lancet Glob Heal. (2016) 4:e609–16. doi: 10.1016/S2214-109X(16)30143-7
52. Zhang Z, Chen F, Shang L. Advances in antitumor effects of NSAIDs. Cancer Manag Res. (2018) 10:4631–40. doi: 10.2147/CMAR.S175212
53. Giraldo NA, Becht E, Vano Y, Sautès-Fridman C, Fridman WH. The immune response in cancer: from immunology to pathology to immunotherapy. Virchows Arch. (2015) 467:127–35. doi: 10.1007/s00428-015-1787-7
54. Candido J, Hagemann T. Cancer-related inflammation. J Clin Immunol. (2013) 33:S79–84. doi: 10.1007/s10875-012-9847-0
55. Munn LL. Cancer and inflammation. Wiley Interdiscip Rev Syst Biol Med. (2017) 9:e1370. doi: 10.1002/wsbm.1370
Keywords: urothelial carcinoma, neutrophil-lymphocyte ratio, trans-urethral resection of bladder tumor, cystectomy, chemotherapy, oncological outcome
Citation: Suh J, Jung JH, Jeong CW, Kwak C, Kim HH and Ku JH (2019) Clinical Significance of Pre-treated Neutrophil-Lymphocyte Ratio in the Management of Urothelial Carcinoma: A Systemic Review and Meta-Analysis. Front. Oncol. 9:1365. doi: 10.3389/fonc.2019.01365
Received: 30 July 2019; Accepted: 19 November 2019;
Published: 16 December 2019.
Edited by:
Kent William Mouw, Dana–Farber Cancer Institute, United StatesReviewed by:
Mohamed Saad Zaghloul, Cairo University, EgyptGuru Sonpavde, Dana–Farber Cancer Institute, United States
Copyright © 2019 Suh, Jung, Jeong, Kwak, Kim and Ku. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Ja Hyeon Ku, randyku@hanmail.net