 Sandro V. Porceddu1Florian Scotté2
Sandro V. Porceddu1Florian Scotté2 Matti Aapro3
Matti Aapro3 Satu Salmio4
Satu Salmio4 Ana Castro5Vincent Launay-Vacher6
Ana Castro5Vincent Launay-Vacher6 Lisa Licitra7*
Lisa Licitra7*- 1University of Queensland, Princess Alexandra Hospital, Woolloongabba, QLD, Australia
- 2Department of Medical Oncology and Supportive Care, Hôpital Foch, Suresnes, France
- 3Genolier Cancer Center, Genolier, Switzerland
- 4Merck KGaA, Darmstadt, Germany
- 5Lenitudes Medical Center & Research, Santa Maria da Feira, Portugal
- 6Service ICAR–Department of Nephrology, Hôpital Pitié-Salpêtrière, Paris, France
- 7Fondazione IRCCS Istituto Nazionale Tumori and University of Milan, Milan, Italy
Concurrent chemoradiotherapy with high-dose cisplatin (100 mg/m2 every 3 weeks) is the preferred regimen with curative intent for patients with unresected locally advanced squamous cell carcinoma of the head and neck (LA SCCHN). This treatment is associated with acute and late toxicities, including myelosuppression, severe nausea/vomiting, irreversible renal failure, hearing loss, and neurotoxicity. Because of cisplatin's safety profile, treatment adherence to high-dose cisplatin can be suboptimal. Patients commonly receive less than the total cumulative target dose of 300 mg/m2 or the minimum recommended dose of 200 mg/m2, which can have a negative impact on locoregional control and survival. Alternatively, cetuximab plus radiotherapy may be most suitable for patients at high risk of non-adherence to high-dose cisplatin. We discuss the baseline characteristics dictating the unsuitability/borderline unsuitability of cisplatin and the available alternative evidence-based treatment regimens for patients with LA SCCHN. We non-systematically reviewed published phase II and III trials and retrospective analyses of high-dose cisplatin-based chemoradiation in LA SCCHN conducted between 1987 and 2018, focusing on recent key phase III studies. We defined the baseline characteristics and associated prescreening tests to determine unsuitability and borderline unsuitability for high-dose cisplatin in combination with radiotherapy in patients with LA SCCHN. Patients with any pre-existing comorbidities that may be exacerbated by high-dose cisplatin treatment can be redirected to a non-cisplatin-based option to minimize the risk of treatment non-adherence. High-dose cisplatin plus radiotherapy remains the preferred treatment for fit patients with unresected LA SCCHN; patients who are unsuitable or borderline unsuitable for high-dose cisplatin could be identified using available tests for potential comorbidities and should be offered alternative treatments, such as cetuximab plus radiotherapy.
Introduction
Squamous cell carcinoma of the head and neck (SCCHN) is among the most frequent cancers worldwide (1). Although recurrent and/or metastatic disease has a poor prognosis, earlier-stage, and non-metastatic locally advanced (LA) SCCHN remains potentially curable. Prognosis strongly depends on factors such as the primary site, disease stage, and human papillomavirus (HPV) infection status in oropharyngeal cancer (OPC), with the intricacies of personalized treatment still being evaluated.
Radiotherapy plus concomitant chemotherapy for LA SCCHN (stage III-IV) has been shown to improve 5 year absolute survival by 6.5% compared with locoregional treatment alone, as reported in a meta-analysis (2). However, approximately half of the patients receiving chemoradiotherapy develop recurrence (3), highlighting the unmet medical need for this patient population.
According to the guidelines of the European Society for Medical Oncology (ESMO; currently being updated) and the National Comprehensive Cancer Network, concurrent cisplatin-based chemoradiotherapy is the preferred treatment for fit patients with unresectable LA SCCHN and for those with resectable LA SCCHN but with a poor prognosis, functional loss, or high-risk features in the post-operative setting (i.e., extranodal extension and/or positive margins) (4, 5). The recommended administration schedule for cisplatin in the LA setting is three cycles of 100 mg/m2 every 3 weeks (high-dose cisplatin) with conventional fractionation radiotherapy or two cycles with altered fractionation radiotherapy (4, 6).
The treatment efficacy of cisplatin-based chemoradiotherapy appears to correlate with the cumulative cisplatin dose received by the patient. Specifically, a multivariable analysis showed that overall survival (OS) is significantly lower in patients with HPV-negative LA SCCHN (including OPC, laryngo-hypopharyngeal cancer, and carcinoma of unknown primary) who receive a cumulative cisplatin dose of ≤200 mg/m2 than in those who receive >200 mg/m2 (7). However, cisplatin is associated with both acute and late, often irreversible toxicities, which manifest as detrimental short- and long-term complications for patients. Thus, treatment adherence to high-dose cisplatin is low, and administration of the necessary cisplatin dose to effectively treat LA SCCHN is not feasible for many patients (8). Indeed, large-scale trials from the past two decades using conventional fractionation showed that only 61–85% of patients with LA SCCHN were able to receive three 100 mg/m2-doses of cisplatin (6, 9, 10). Furthermore, a retrospective European study assessing compliance with cisplatin plus radiotherapy in the real-world setting (COMPLY) demonstrated that a cumulative dose of >200 mg/m2 was reached in only 45% of patients receiving the high-dose regimen (8), and a retrospective study by Espeli et al. (11) showed that ≈50% of patients are able to complete the intended treatment of three cycles of high-dose cisplatin.
Unlike the population commonly enrolled into clinical trials, patients with LA SCCHN in the real-world clinical setting often present with more challenging baseline characteristics and risk factors [e.g., poor Eastern Cooperative Oncology Group performance status (ECOG PS) and comorbidities]. Unfortunately, no standardization of supportive care during chemoradiotherapy exists, and patient volume at treatment centers can affect the quality of treatment selection and supportive care (12). Therefore, it is important to compile a set of risk factors that pose a challenge to compliance with high-dose cisplatin and a comprehensive picture of alternative options to consider during treatment decision making.
In this review, we discuss risk factors associated with high-dose cisplatin that can enable physicians to identify which patients with LA SCCHN are eligible, ineligible, or eligible with a high risk of treatment non-compliance—the so-called “borderline unsuitable”—for concurrent high-dose cisplatin chemoradiotherapy with curative intent. Most of the data described here emerged before the distinct clinical entity of HPV-associated OPC was fully understood and when the proportion of patients with HPV-associated OPC enrolled in clinical trials was likely lower than that in contemporary cohorts. Therefore, the recent results of phase III studies of HPV-positive OPC exploring the clinical outcomes of cisplatin plus radiotherapy vs. alternative regimens are important.
Cisplatin-Associated Toxicities That Can Compromise Treatment Compliance
The addition of high-dose cisplatin to radiotherapy both exacerbates known radiotherapy-associated adverse events (AEs) and causes specific cisplatin-associated AEs (Table 1), which are dose dependent. Nausea, vomiting, ototoxicity, nephrotoxicity, and neurotoxicity are also observed with cisplatin treatment (monotherapy or in combination) (36). Furthermore, these toxicities are cumulative, dose dependent, are often non-reversible (except nausea and vomiting), and can involve extensive injury to poorly regenerating or non-regenerating organs, resulting in exacerbation of pre-existing conditions and potentially a permanent impact on the quality of life (QOL) of cured patients (Table 2) (10, 11, 13, 14, 37).
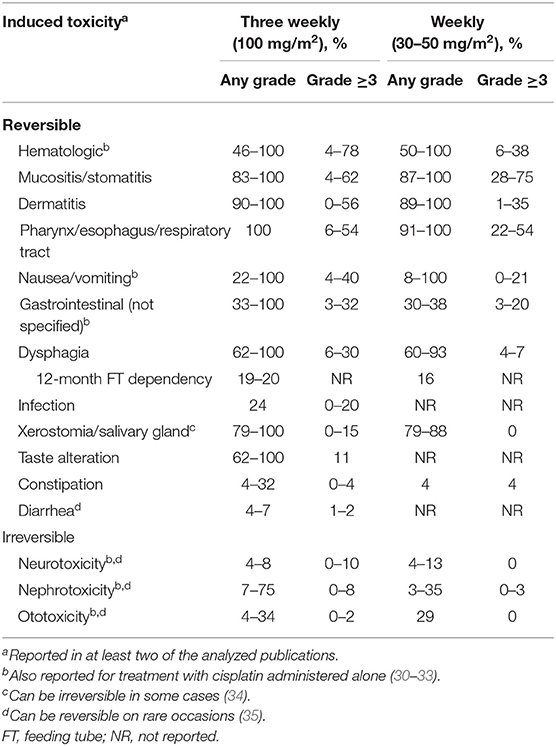
Table 1. Cisplatin chemoradiotherapy–associated acute toxicities in head and neck cancer (9–11, 13–29).
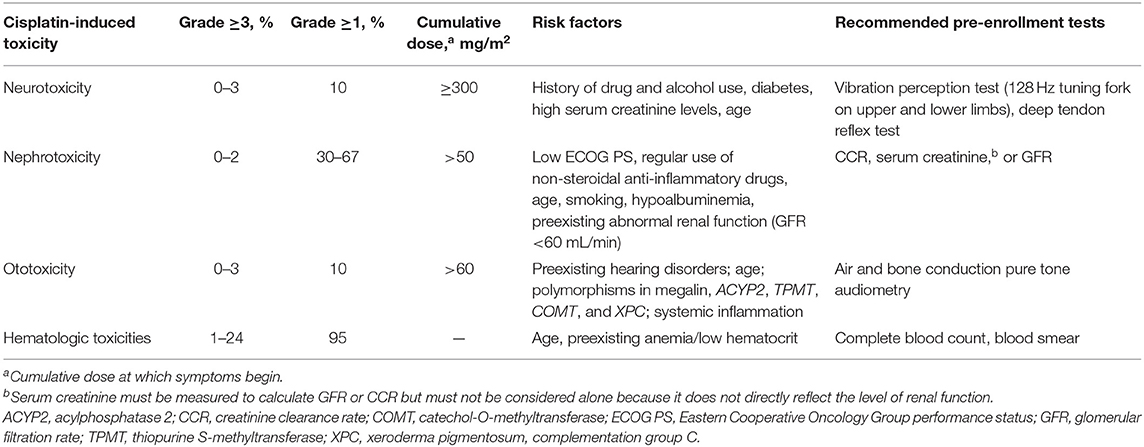
Table 2. Selected cisplatin chemoradiotherapy–associated late toxicities in head and neck cancer (10, 11, 13, 14, 35, 37–44).
Cisplatin-induced neurotoxicity, experienced at grade ≥3 (by investigator choice of version of National Cancer Institute Common Terminology Criteria for Adverse Events) by ≤10% of patients (Table 1), affects mainly peripheral neurons—most likely via DNA damage–induced apoptosis of dorsal root ganglion neurons (45, 46)—and presents as sensory symptoms in the extremities (47, 48). Neurotoxicity resulting from peripheral nerve damage is irreversible in 30% to 50% of cases and progresses for ≤4 months after treatment (35, 49). Additionally, concurrent irradiation of the spinal cord, brain, brain stem, or cranial nerves can compound cisplatin-associated neurotoxicity and result in further functional deficit (50).
Ototoxicity is another highly distressing AE. Although its mechanism is not fully understood, ototoxicity arises predominantly from sensory hair cell death within the cochlea and is perpetuated by irradiation of and cisplatin-mediated damage to the cochlea (often neglected as an organ at risk) (38, 51, 52). Late ototoxicity is observed in up to two-thirds of cisplatin-treated patients, with ≤2% experiencing grade ≥3 events (equivalent to irreversible damage) (Table 1). Because some patients discontinue treatment due to hearing loss before it reaches grade ≥3 severity, the frequency and severity of ototoxicity vary and are likely underreported.
Cisplatin-induced nephrotoxicity is the result of a combination of factors. The kidney absorbs cisplatin at higher concentrations than other tissues (53, 54). In the kidney, cisplatin induces apoptosis via the activation of death receptors and tumor necrosis factor α-stimulated inflammatory response (39, 55). Nephrotoxicity cannot be completely prevented, even with adequate hydration regimens, and has been reported to occur as an acute AE in 7–75% of patients receiving the high-dose regimen (Table 1). Dehydration and electrolyte imbalance from chemotherapy can further contribute to cisplatin-associated late nephrotoxicity, leading to irreversible reduction in glomerular filtration rate (GFR) (40, 56, 57).
Acute gastrointestinal symptoms associated with cisplatin-based chemoradiotherapy include nausea, vomiting, mucositis/stomatitis, xerostomia, taste alteration, constipation, and diarrhea and have a remarkably high incidence (Table 1).
Cisplatin induces vomiting in >90% of patients within 24 h of treatment if not administered with adequate antiemetic prophylaxis (58–60). Even at a low dose (<50 mg/m2), cisplatin-induced vomiting occurs in 60–90% of patients (60). Nausea, vomiting, and mucositis further exacerbate dehydration, adding to the burden on patients' kidneys. Thus, physicians deem even low-grade (1/2) vomiting as unacceptable, especially in patients already experiencing dehydration.
Another compounding but poorly reported AE experienced by patients receiving platinum-based therapy is altered taste (typically metallic), which, combined with radiation-induced loss of taste, can lead to marked dysgeusia and consequently poor food intake and nutritional problems (61, 62). Additional radiotherapy-associated AEs such as dysphagia [which can cause feeding-tube dependence and ultimately aspiration pneumonia (63–65)], dry mouth, mucositis, and dermatitis can occur at high rates upon the addition of high-dose cisplatin to radiotherapy. A comprehensive list of toxicities associated with cisplatin and corresponding incidence rates is shown in Table 1.
Absolute Contraindications vs. Borderline Unsuitability for Cisplatin
Since cisplatin's introduction as a chemotherapy agent in the late 1970s, a strong need has emerged to clearly define the patient population that is able to tolerate this treatment. For this purpose, studies investigating the correlations between baseline characteristics of patients and cisplatin-induced AEs have led to a consensus of absolute contraindications for cisplatin, which can be used to guide the treatment decision-making process.
Although it is often clear whether patients are absolutely or not at all contraindicated for high-dose cisplatin-based treatment, many patients fall in an in-between category of “borderline” unsuitability, for which the optimal treatment decision is not self-evident and must be made based on a physician's clinical judgment. Patients with conditions that may be worsened by the high-dose cisplatin regimen may experience QOL detriment while not reaching the recommended cumulative dose due to treatment interruption or cessation. The level of risk of sustaining irreversible cisplatin-associated toxicities should therefore be weighed against the potential benefit on a patient-by-patient basis. In many cases, these toxicities can be avoided if borderline-unsuitable patients are identified before treatment and preferentially redirected to alternative treatment regimens.
Absolute contraindications are outlined in Table 3 and include hypersensitivity to platinum, pregnancy/lactation, ECOG PS of ≥3, GFR of <50 mL/min or—only if GFR cannot be assessed—creatinine clearance rate of <50 mL/min (estimated by the Cockcroft-Gault formula), marrow disorders (in certain cases), preexisting hearing loss, neurological impairment, Child-Pugh score of B or C, New York Heart Association class III or IV congestive heart failure, and a severe hematologic condition (Table 3) (35, 41, 66–71). Notably, in regard to GFR of 50 to <60 mL/min, consultation with a nephrologist should be considered. Some clinicians offer dose-reduced cisplatin in these patients; this is a matter of discussion with the individual patient.
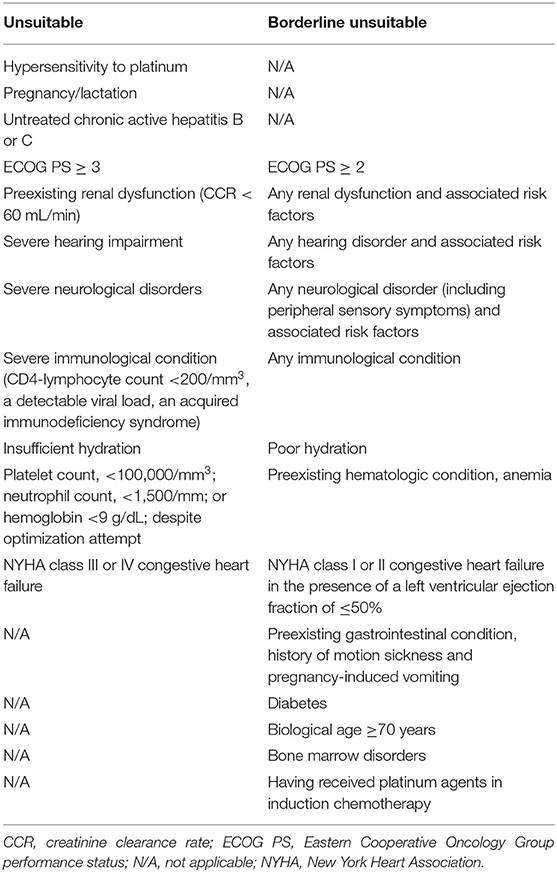
Table 3. Cisplatin unsuitability and borderline unsuitability criteria.
In contrast, the borderline-unsuitable population includes patients with any current organ system dysfunction, especially any history of hearing, neurological, renal, hepatic, or cardiovascular disorders; a compromised immune system (e.g., HIV infection/AIDS); ≥20% weight loss; or a history of having received platinum agents in addition to taxanes in the induction setting for LA SCCHN (the only category 1–level, post-induction regimen for these patients and for selected primary tumor sites is radiotherapy alone; Table 3) (4, 35, 40, 68). In addition, some guidelines have recommended that patients older than 70 years and those with an ECOG PS of ≥2 or without objective evidence of euvolemia should not be treated with cisplatin (35, 40, 68). Reports have shown, however, that biological age is far more important and that patients who are treated only in accordance with chronical age may therefore be undertreated (72–74).
Although there is consensus on the risk factors for cisplatin toxicity in different indications, the clinical cutoff for unsuitability criteria for other cancer types should also be considered when treating patients with SCCHN. For example, guidelines for lung and urothelial cancer define ECOG PS of ≥2, New York Heart Association class II to III heart failure, and creatinine clearance rate (or GFR) of <60 mL/min as absolute contraindications for cisplatin (66–69). Finally, the combination of multiple comorbidities can have an additive effect on the risk of cisplatin toxicity (75).
Risk Factors for Cisplatin-Induced Toxicities and Available Screening Methods
To assess whether a patient is contraindicated or borderline unsuitable for cisplatin, careful screening for comorbidities and evaluating the patient's current state of health and available psychosocial setting are necessary before prescribing cisplatin (35, 41).
Sensory symptoms in the extremities—such as weakness, tremor, numbness, paresthesia, and loss of position and vibration sense—are early predictors of severe cisplatin-induced neuropathy (47). Indeed, changes in vibration perception (assessable using a 128 Hz tuning fork on upper and lower limbs) and deep tendon reflex (assessable by standard deep tendon reflex test) have been shown to correlate with the severity of cisplatin-induced neuropathy (42). Furthermore, although known risk factors for chemotherapy-induced peripheral neurotoxicity such as history of drug and alcohol abuse, diabetes, high serum creatinine levels, and advancing age (Table 2) (76) have not been demonstrated to specifically and significantly increase the severity of cisplatin-induced toxicities (77), they should be considered when deciding on a treatment regimen for patients with LA SCCHN.
Key risk factors for cisplatin-induced ototoxicity are age and pre-existing hearing disorders (38). Because impaired hearing at baseline is not necessarily evident, it is not routinely or easily tested and thus should be evaluated by conduction audiometry before any cisplatin treatment (43).
Pre-existing renal disorders are the most important high-risk factors for cisplatin-induced nephrotoxicity and can be assessed by urinalysis and estimating GFR (10, 35, 38, 40). Measurement of creatinine clearance rate (see earlier recommendations) is not advised, because it has been shown to be dependent on body mass index and is often unreliable in practice due to faulty urine collection (78). Additional risk factors for cisplatin-induced nephrotoxicity are poor ECOG PS, regular use of non-steroidal anti-inflammatory drugs, advanced age, smoking, and diabetes (Table 2). Given that the risk of renal injury remains high despite all of these considerations, a model developed by Motwani et al. (79) to predict renal injury after the first cycle of cisplatin can be used.
Age is one of the most important risk factors for cisplatin-associated hematologic toxicities (80). A profound and prolonged decrease in neutrophil counts can be a serious issue and can lead to either a delay in cisplatin doses or failure to receive the total dose of 300 mg/m2. Low hematocrit (anemia) resulting from cisplatin treatment can increase the risk of severe hematologic AEs and should be measured in the blood (e.g., complete blood count or blood smear) before treatment. However, because anemia resulting from cisplatin therapy is rare and can be treated per ESMO guidelines (81), its risk should be weighed against the probability of cure.
Risk factors for chemotherapy-induced vomiting include age, sex (women are at higher risk), and history of motion sickness and/or pregnancy-induced vomiting (60). Patient age is a complex factor in the LA SCCHN treatment decision-making process and continues to be a topic of discussion. Specifically, although most young patients (≤55 years old) have good renal function and are thus optimal candidates for cisplatin treatment, their post-treatment QOL is of high consideration during the regimen selection process. To predict chemotherapy toxicity based on a patient's physiological age, a geriatric assessment can be performed using the scale developed by Extermann et al. (82).
Preventive Measures to Avoid Cisplatin-Induced Toxicities
In addition to the level of difficulty associated with managing cisplatin-induced late toxicities, limited preventive management options exist, and careful patient selection remains the most effective method to reduce overall risk. Because of the high incidence of toxicities, all available prophylactic measures should be applied when treating eligible patients with cisplatin, and patients should be closely monitored during and after therapy. Furthermore, patients with SCCHN should be managed by a multidisciplinary team (4, 5, 41).
Some studies suggest that accelerating the infusion time of cisplatin can exacerbate the severity of toxicities. A study comparing a 2 vs. 24 h infusion time, performed before the development of efficient antiemetic treatment, revealed significantly less emetic toxicity with the 24 h infusion of 50 or 100 mg/m2 and pretreatment hydration (83); hence, infusion times shorter than the recommended 6–8 h are not advisable. Furthermore, studies have suggested that lowering the dose of radiation to the pharyngeal constrictors and larynx to <50 Gy may reduce the risk of swallowing complications such as long-term dysphagia (84, 85); however, such a reduction is inadvisable because it may also lower the probability of tumor control.
Additionally, any concomitant neurotoxic, ototoxic, and nephrotoxic drugs should be strictly avoided (including aminoglycosides, furosemide, and non-steroidal anti-inflammatory drugs) (40, 86). Numerous studies have suggested that thiol compounds (e.g., glutathione), vitamin E, and anticonvulsants (e.g., gabapentin, pregabalin) can have a neuroprotective effect (87). Thiosulfates have also been used against ototoxicity (38). However, these strategies have failed to provide conclusive evidence of the prevention of neurotoxicity and ototoxicity secondary to cisplatin treatment and are not universally recommended (87). Although no effective measures are available to fully prevent cisplatin-associated ototoxicity, its occurrence can be reduced by administering reduced-dose radiotherapy directly to the cochlea; the threshold for ototoxicity was found to be 10 Gy (88).
Dehydration through nausea and vomiting is one of the most serious and unpleasant side effects of chemoradiotherapy with cisplatin, and keeping a patient sufficiently hydrated is an effective and widely used method to counteract associated nephrotoxicity (40). The recommended hydration regimen consists of a continuous infusion of a normal saline solution starting 12 h before cisplatin administration and ending ≥1 day after treatment (40). To avoid further nephrotoxicity and dehydration, triple or quadruple antiemetic therapy consisting of a 5-hydroxytryptamine-3 (serotonin) receptor antagonist, a neurokinin 1 receptor antagonist, and dexamethasone (with or without olanzapine)—per Multinational Association of Supportive Care in Cancer/ESMO and American Society of Clinical Oncology guidelines—and sufficient doses of magnesium (40–80 mmol/cycle), should always be administered concomitantly with cisplatin (40, 58, 59). Conversely, studies of the effectiveness of mannitol diuresis in preventing nephrotoxicity have shown contradictory results; hence, caution should be exercised when considering it as a protective measure (89–91).
Baseline Characteristics Dictating a Qol-Centric Approach
Recently, the long-term impact of treatment-related toxicities on the QOL of responders has come into focus in populations with a favorable prognosis. Specifically, overall, patients with HPV-positive OPC have a very good prognosis and tend to be younger and have little or no smoking history, fewer comorbidities, and improved locoregional control and OS compared with patients with HPV-negative tumors (92–94). Results from two phase III trials in patients with HPV-positive OPC suitable for cisplatin (RTOG 1016 and De-ESCALaTE) reinforced the high-dose cisplatin plus radiotherapy regimen as the standard of care for this patient population in terms of OS (95, 96). For the overall population, cetuximab plus radiotherapy remains a guideline-recommended treatment option, and has demonstrated a higher response rate, longer disease-free progression, and longer OS vs. radiotherapy alone (4, 5). The results of the TROG 12.01 study, which is comparing the combination of either cetuximab or weekly cisplatin with radiotherapy, are awaited (97). Finally, lowering the radiotherapy dose is being explored as a method of preventing detriment to QOL in patients with HPV-positive disease. It should be noted that the recently presented NRG-HN002 trial demonstrated that the addition of cisplatin to 60-Gy intensity-modulated radiation therapy in HPV-positive patients provided additional tumor control (98).
Alternative Treatment Options for Cisplatin-Unsuitable and Borderline-Unsuitable Patients
Patients with LA SCCHN who are strictly contraindicated to receive cisplatin depend on alternative treatments and/or future advances in this field, and those who are either cisplatin borderline unsuitable or have favorable prognoses may strongly benefit from them. To find the optimal regimen for each patient, the benefits and disadvantages of alternative regimens need to be carefully balanced. Despite the lack of phase III trials demonstrating the efficacy of alternative treatments vs. high-dose cisplatin–based chemoradiotherapy in the overall LA SCCHN population, several non-cisplatin regimens are currently recommended by international guidelines, of which only two do not include a platinum agent: radiotherapy plus either 5-fluorouracil [5-FU] and hydroxyurea or cetuximab (4, 5).
Data from a recent meta-analysis by the Meta-Analysis of Radiotherapy in Squamous Cell Carcinomas of Head and Neck (MARCH) Group demonstrated that concomitant chemoradiation is significantly superior to altered fractionation radiotherapy alone in terms of OS (99). Although no direct comparison between hyperfractionation (which seemed superior to other altered fractionation methods) and concomitant chemoradiation has been made, these results indicate that patients with LA SCCHN should not be treated with conventionally fractionated radiation alone (99).
Low-Dose Weekly Cisplatin Plus Radiotherapy
Because of the high incidence of AEs associated with high-dose cisplatin, clinical practice has focused on splitting the dose of 100 mg/m2 every 3 weeks into weekly doses of 20–50 mg/m2, which also allows the physician to monitor the patient weekly and hence potentiates supportive care. Weekly cisplatin 40 mg/m2, the most commonly used weekly regimen, has not been evaluated in a large randomized study vs. concurrent high-dose cisplatin chemoradiotherapy or radiotherapy alone and is currently supported by a category 2B level of evidence in international guidelines (4). A retrospective analysis suggested a potentially reduced efficacy with this regimen (median OS, 1.9 vs. 4.3 years for weekly 40 mg/m2 vs. high-dose cisplatin, respectively) (11). An evaluation of single-dose administration of 100 mg/m2 of cisplatin compared with a split dose of 50 mg/m2 per day on two consecutive days found no significant difference in OS between these two regimens in patients with SCCHN (100). Reported compliance rates with cisplatin 40 mg/m2 weekly are contradictory: one study (14) showed similar compliance with both regimens, whereas three studies (including COMPLY in the real-world setting) showed better compliance with high-dose than with weekly cisplatin (8, 15, 16).
Weekly cisplatin doses of <40 mg/m2 have failed to show superiority or non-inferiority to radiotherapy alone or to high-dose cisplatin in terms of efficacy and treatment compliance in multiple trials (8, 101, 102). For example, a phase III study conducted by the Head and Neck Intergroup (102) reported a median OS of 11.8 months with weekly cisplatin 20 mg/m2 plus radiotherapy and of 13.3 months with radiotherapy alone. In the real-world, retrospective, observational study COMPLY, compliance was lower with cisplatin 30 mg/m2 weekly than with high-dose cisplatin; toxicity was comparable (8).
Overall, weekly cisplatin treatment is precluded by the same contraindication panel as the high-dose schedule. Furthermore, because the level of toxicity risk with weekly cisplatin regimens has not been investigated in patients who are considered borderline unsuitable for high-dose cisplatin, this treatment cannot be said to circumvent any of the detriments of the high-dose schedule in this patient population.
Alternative Chemotherapy Agents in Combination With Radiotherapy
Efforts made to find less-toxic chemotherapeutic agents resulted in the development of carboplatin—a second-generation platinum-based drug with a mechanism of action similar to that of cisplatin but with a different chemical structure and a somewhat milder toxicity profile. Indeed, a meta-analysis (103) of 12 studies—published between 1995 and 2013—in patients (n = 1,165) with LA SCCHN showed improved 5-year OS with cisplatin. Toxicity profiles of the two agents were similar, although fewer gastrointestinal and renal toxicities but more frequent hematologic toxicities were observed with carboplatin. Because of the lack of randomized phase III trials, however, treatment of LA SCCHN with carboplatin and concurrent radiotherapy is not currently considered an evidence-based option in LA SCCHN (104). Carboplatin in combination with 5-FU and radiotherapy (predominantly used in France) has demonstrated improved OS and locoregional control compared with radiotherapy alone in two phase III trials (105, 106) and is recommended with a category 1 level of evidence (4). The most frequent grade 3 treatment-related AE with carboplatin and 5-FU is mucositis; other grade ≥3 toxicities include fever, renal toxicity, skin reaction, and altered liver enzyme function (107). As with cisplatin, patients need to be fit to receive carboplatin plus 5-FU; this regimen is thus an alternative option for patients with contraindications to cisplatin specifically (e.g., reduced renal or hearing function) who have a good PS. Therefore, non-platinum-based anticancer agents in combination with radiotherapy are needed for the treatment of LA SCCHN. A phase III trial comparing 5-FU + mitomycin C + hyperfractionated accelerated radiation therapy (HART) with cisplatin + mitomycin C + HART demonstrated no significant differences in OS, progression-free survival (PFS), or locoregional control. Chemoradiation with weekly cisplatin + 5-FU or mitomycin C + 5-FU showed excellent adherence rates and can easily compete with other concurrent chemoradiation schedules, including induction with docetaxel + cisplatin + 5-FU followed by radiation (108).
Targeted Therapies in Combination With Radiotherapy
A major recent advance in the LA SCCHN field was the development of cetuximab, an immunoglobulin G1 monoclonal antibody targeting the epidermal growth factor receptor. The effects of adding cetuximab to radiotherapy were studied in a randomized phase III trial by Bonner et al. (109), who reported a significant increase in median PFS (17.1 vs. 12.4 months), median OS (49.0 vs. 29.3 months), and median duration of locoregional control (24.4 vs. 14.9 months) in the cetuximab plus radiotherapy arm vs. radiotherapy alone. The 5-year survival rate was also considerably higher with cetuximab plus radiotherapy (45.6 vs. 36.4%) (110). On the basis of these results, cetuximab became the first targeted therapy approved by the US Food and Drug Administration for LA SCCHN in 2006 (111) and is now recommended by international guidelines (4, 5).
In contrast with cisplatin, no exacerbation of in-field mucositis and dysphagia and no evidence of ototoxicity, neurotoxicity, or nephrotoxicity were observed with the addition of cetuximab to radiotherapy at the end of the trial (Table 4) (109); hence, no reduction in the cetuximab dose is needed in patients with preexisting reduced renal function (111). Also unlike cisplatin, cetuximab does not significantly aggravate radiation dermatitis (109). However, when cetuximab is combined with radiotherapy, different aspects of the skin rash (e.g., crusting) can appear, which have been referred to as bioradiation dermatitis (114, 115). Furthermore, cetuximab is also associated with acneiform rash, a distinct skin rash characteristic of epidermal growth factor receptor inhibition that is severe in only ≤17% of patients. Acneiform rash can be prophylactically treated, resolves within weeks, and correlates with improved OS (109, 110). Randomized phase III data indicate that QOL is not affected by the addition of cetuximab to radiotherapy, despite the associated dermatologic AEs (116). Furthermore, the addition of cetuximab to radiotherapy does not appear to significantly increase the incidence of common radiotherapy-associated toxicities, including mucositis, xerostomia, dysphagia, pain, weight loss, and performance status deterioration (116). Notably, toxicity profiles of cisplatin in combination with radiotherapy and cetuximab in combination with radiotherapy have been shown to differ. Hematologic, renal, and gastrointestinal toxicities appear to occur more frequently with cisplatin combined with radiotherapy, and cutaneous toxicity and the need for nutritional support occur more frequently with cetuximab combined with radiotherapy (17). Differences in the toxicity profile of cisplatin vs. cetuximab in combination with radiotherapy were also confirmed in the RTOG 1016 study in patients with HPV-positive OPC (95), which showed a similar overall rate of grade ≥3 AEs but increased rates of nephrotoxicity, ototoxicity, and bone marrow suppression with cisplatin plus radiotherapy (95). As expected, rash was more frequent with cetuximab treatment (95). Similarly, in the De-ESCALaTE study in patients with low-risk HPV-positive OPC, the cisplatin arm showed comparable rates of all- and high-grade AEs and long-term dysphagia and no difference in QOL, but significantly more serious AEs per patient were observed (96). The tolerability of these regimens may be different in HPV-negative patients, who are older and tend to have more comorbidities (92–94).
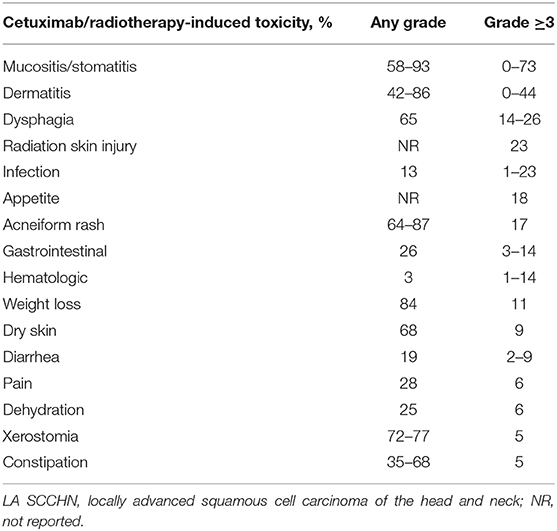
Table 4. Frequency of cetuximab bioradiotherapy–associated acute toxicities in LA SCCHN (17, 109, 112, 113).
Cetuximab in combination with radiotherapy is an efficacious treatment option in LA SCCHN and can be used as an alternative in patients who are unsuitable to receive high-dose cisplatin plus radiotherapy. The randomized phase III trial by Bonner et al. that is discussed above included a large number of patients who would be considered fit and cisplatin eligible. There are no phase III data showing benefit of cetuximab in combination with radiotherapy in the non–platinum-eligible population. Notably, combinations of cetuximab with non-cisplatin chemoradiotherapy agents, such as carboplatin plus paclitaxel or 5-FU, are currently being investigated and have thus far shown promising results (117–119). A recent study demonstrated that the addition of concurrent carboplatin and fluorouracil to cetuximab (three cycles) + radiotherapy resulted in improved PFS and locoregional control. However, the gain in OS was not significant (119).
Emerging Immunotherapy Agents Plus Radiotherapy
Immune checkpoint inhibitors are hypothesized to synergize well with radiotherapy (120). Immune checkpoint inhibitors (e.g., avelumab, nivolumab, pembrolizumab) are under investigation in combination with radiotherapy, chemoradiotherapy, or cetuximab/radiotherapy for LA SCCHN (36, 120–124), and any resulting chemotherapy-sparing regimens could be useful in cisplatin-ineligible patients. For example, avelumab plus cetuximab plus radiotherapy is being evaluated in patients with LA SCCHN in the ongoing phase III REACH study (125). Because no mature results are available for immune checkpoint inhibitors in LA SCCHN, these agents should not yet be used outside of the clinical trial setting.
Conclusions
High-dose cisplatin-based concurrent chemoradiotherapy is the preferred treatment for fit patients with LA SCCHN. Because high-dose cisplatin is associated with a considerable number of toxicities, it is not recommended for patients aged >70 years or with an ECOG PS of ≥2 (35). Preexisting comorbidities, such as neurological disorders, renal impairment, and hearing loss, can be exacerbated irreversibly by cisplatin treatment and are tentative or absolute contraindications for cisplatin treatment. In addition to absolute cisplatin-unsuitable patients, patients with a high risk of treatment non-adherence for concurrent high-dose cisplatin chemoradiotherapy are defined herein as borderline unsuitable.
Alternative chemotherapy regimens and administration schedules, targeted agents, and emerging immunotherapies provide possible treatment options for cisplatin-contraindicated or borderline-unsuitable patients with LA SCCHN. HART alone could also be a reasonable alternative for cisplatin-contraindicated patients (126). However, few of the previously-mentioned options have been tested for non-inferiority vs. high-dose cisplatin in randomized, phase III trials in the overall LA SCCHN population. Cetuximab is an approved non-platinum agent that is recommended for combination with radiotherapy in the treatment of LA SCCHN. This regimen has demonstrated good locoregional control and survival outcomes in patients with this tumor type and is thus a suitable treatment alternative for patients who are unlikely to tolerate high-dose cisplatin.
The reference tools provided in this review should facilitate the treatment decision-making process in LA SCCHN for oncologists and healthcare professionals before prescribing high-dose cisplatin chemoradiotherapy for their patients.
Author Contributions
SP, FS, MA, SS, AC, VL-V, and LL contributed equally to manuscript development in terms of manuscript preparation, manuscript review, and final approval.
Conflict of Interest
SS discloses employment with Merck KGaA, Darmstadt Germany.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Acknowledgments
Medical writing assistance was provided by ClinicalThinking, Inc., Hamilton, NJ, USA, and funded by Merck KGaA, Darmstadt, Germany, in accordance with Good Publication Practice guidelines (http://www.ismpp.org/gpp3).
References
1. Bray F, Ferlay J, Soerjomataram I, Siegel RL, Torre LA, Jemal A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. (2018) 68:394–424. doi: 10.3322/caac.21492
2. Blanchard P, Landais C, Petit C, Zhang Q, Grégoire V, Tobias J, et al. Meta-analysis of chemotherapy in head and neck cancer (MACH-NC): an update on 100 randomized trials and 19,248 patients, on behalf of MACH-NC Group. Ann Oncol. (2016) 27(Suppl 6):950O. doi: 10.1093/annonc/mdw376.02
3. Sacco AG, Cohen EE. Current treatment options for recurrent or metastatic head and neck squamous cell carcinoma. J Clin Oncol. (2015) 33:3305–13. doi: 10.1200/JCO.2015.62.0963
4. NCCN Clinical Practice Guidelines in Oncology. Head and Neck Cancers V1. (2019). Available online at: http://www.nccn.org/professionals/physician_gls/pdf/head-and-neck.pdf (accessed July 18, 2019).
5. Grégoire V, Lefebvre JL, Licitra L, Felip E EHNS-ESMO-ESTRO Guidelines Working Group. Squamous cell carcinoma of the head and neck: EHNS-ESMO-ESTRO clinical practice guidelines for diagnosis, treatment and follow-up. Ann Oncol. (2010) 21(Suppl 5): v184–6. doi: 10.1093/annonc/mdq185
6. Nguyen-Tan PF, Zhang Q, Ang KK, Weber RS, Rosenthal DI, Soulieres D, et al. Randomized phase III trial to test accelerated versus standard fractionation in combination with concurrent cisplatin for head and neck carcinomas in the Radiation Therapy Oncology Group 0129 trial: long-term report of efficacy and toxicity. J Clin Oncol. (2014) 32:3858–66. doi: 10.1200/JCO.2014.55.3925
7. Spreafico A, Huang SH, Xu W, Granata R, Liu CS, Waldron JN, et al. Impact of cisplatin dose intensity on human papillomavirus-related and -unrelated locally advanced head and neck squamous cell carcinoma. Eur J Cancer. (2016) 67:174–82. doi: 10.1016/j.ejca.2016.08.013
8. Dunst J, Hildebrandt G, Becker-Schiebe M, Kuhnt T, Weykamp F, Richetti A, et al. Assessment of therapeutic COMpliance of patients treated with cisPLatin plus radiotherapY in locally advanced squamous cell carcinoma of the head and neck—first results of the retrospective, anonymized, observational, European, multicenter COMPLY trial. Presented at: 6th Trends in Head and Neck Oncology. Nice (2017).
9. Forastiere AA, Goepfert H, Maor M, Pajak TF, Weber R, Morrison W, et al. Concurrent chemotherapy and radiotherapy for organ preservation in advanced laryngeal cancer. N Engl J Med. (2003) 349:2091–8. doi: 10.1056/NEJMoa031317
10. Cooper JS, Pajak TF, Forastiere AA, Jacobs J, Campbell BH, Saxman SB, et al. Postoperative concurrent radiotherapy and chemotherapy for high-risk squamous-cell carcinoma of the head and neck. N Engl J Med. (2004) 350:1937–44. doi: 10.1056/NEJMoa032646
11. Espeli V, Zucca E, Ghielmini M, Giannini O, Salatino A, Martucii F, et al. Weekly and 3-weekly cisplatin concurrent with intensity-modulated radiotherapy in locally advanced head and neck squamous cell cancer. Oral Oncol. (2012) 48:266–71. doi: 10.1016/j.oraloncology.2011.10.005
12. Wuthrick EJ, Zhang Q, Machtay M, Rosenthal DI, Nguyen-Tan PF, Fortin A, et al. Institutional clinical trial accrual volume and survival of patients with head and neck cancer. J Clin Oncol. (2015) 33:156–64. doi: 10.1200/JCO.2014.56.5218
13. Kiyota N, Tahara M, Okano S, Kawashima M, Matsuura K, Onozawa Y, et al. Phase II feasibility trial of adjuvant chemoradiotherapy with 3-weekly cisplatin for Japanese patients with post-operative high-risk squamous cell carcinoma of the head and neck. Jpn J Clin Oncol. (2012) 42:927–33. doi: 10.1093/jjco/hys128
14. Mitra D, Choudhury K, Rashid MA. Concurrent chemotherapy in advanced head and neck carcinoma—a prospective randomized trial. Bangaladesh J Otorhinolaryngol. (2011) 17:88–95. doi: 10.3329/bjo.v17i2.8847
15. Geeta SN, Padmanabhan TK, Samuel J, Pavithran K, Iyer S, Kuriakose MA. Comparison of acute toxicities of two chemotherapy schedules for head and neck cancers. J Cancer Res Ther. (2006) 2:100–4. doi: 10.4103/0973-1482.27584
16. Tsan DL, Lin CY, Kang CJ, Huang SF, Fan KH, Liao CT, et al. The comparison between weekly and three-weekly cisplatin delivered concurrently with radiotherapy for patients with postoperative high-risk squamous cell carcinoma of the oral cavity. Radiat Oncol. (2012) 7:215. doi: 10.1186/1748-717X-7-215
17. Magrini SM, Buglione M, Corvò R, Pirtoli L, Paiar F, Ponticelli P, et al. Cetuximab and radiotherapy versus cisplatin and radiotherapy for locally advanced head and neck cancer: a randomized phase II trial. J Clin Oncol. (2016) 34:427–35. doi: 10.1200/JCO.2015.63.1671
18. Liang H, Xia W-X, Lv X, Sun R, Zeng Q, Li S-W, et al. Comparison of concurrent chemoradiotherapy with 3-weekly versus weekly cisplatin in patients with local-regionally advanced nasopharyngeal carcinoma: a phase 3 multicentre randomised controlled trial (ChiCTR-TRC-12001979). J Clin Oncol. (2017) 35(Suppl):6006. doi: 10.1200/JCO.2017.35.15_suppl.6006
19. Ho KF, Swindell R, Brammer CV. Dose intensity comparison between weekly and 3-weekly cisplatin delivered concurrently with radical radiotherapy for head and neck cancer: a retrospective comparison from New Cross Hospital, Wolverhampton, UK. Acta Oncol. (2008) 47:1513–8. doi: 10.1080/02841860701846160
20. Kose F, Besen A, Sumbul T, Sezer A, Karadeniz C, Disel U, et al. Weekly cisplatin versus standard three-weekly cisplatin in concurrent chemoradiotherapy of head and neck cancer: the Baskent University experience. Asian Pac J Cancer Prev. (2011) 12:1185–8. doi: 10.1200/jco.2011.29.15_suppl.e16001
21. Oosting SF, Chen TWW, Huang SH, Wang L, Waldron J, Gilbert R, et al. A comparison of weekly versus 3-weekly cisplatin during adjuvant radiotherapy for high-risk head and neck cancer. Oral Oncol. (2016) 59:43–49. doi: 10.1016/j.oraloncology.2016.05.016
22. Sahoo TK, Samanta DR, Senapati SN, Parida K. A comparative study on weekly versus three weekly cisplatinum based chemoradiation in locally advanced head and neck cancers. J Clin Diagn Res. (2017) 11:XC07–11. doi: 10.7860/JCDR/2017/24765.9293
23. Tao CJ, Lin L, Zhou GQ, Tang LL, Chen L, Mao YP, et al. Comparison of long-term survival and toxicity of cisplatin delivered weekly versus every three weeks concurrently with intensity-modulated radiotherapy in nasopharyngeal carcinoma. PLoS ONE. (2014) 9:e110765. doi: 10.1371/journal.pone.0110765
24. Zenda S, Onozawa Y, Tahara M, Kawashima M, Shikama N, Sasaki S, et al. Feasibility study of single agent cisplatin and concurrent radiotherapy in Japanese patients with squamous cell carcinoma of the head and neck: preliminary results. Jpn J Clin Oncol. (2007) 37:725–9. doi: 10.1093/jjco/hym106
25. Gupta T, Agarwal JP, Ghosh-Laskar S, Parikh PM, D-Cruz AK, Dinshaw KA. Radical radiotherapy with concurrent weekly cisplatin in loco-regionally advanced squamous cell carcinoma of the head and neck: a single-institution experience. Head Neck Oncol. (2009) 1:17. doi: 10.1186/1758-3284-1-17
26. Al-Sarraf M, Pajak TF, Marcial VA, Mowry P, Cooper JS, Stetz J, et al. Concurrent radiotherapy and chemotherapy with cisplatin in inoperable squamous cell carcinoma of the head and neck. An RTOG study. Cancer. (1987) 59:259–65. doi: 10.1002/1097-0142(19870115)59:2<259::AID-CNCR2820590214>3.0.CO;2-1
27. Fountzilas G, Skarlos D, Kosmidis P, Samantas E, Kalogera-Fountzila A, Papaspyrou S, et al. Radiation therapy and concurrent cisplatin administration in locally advanced head and neck cancer. A Hellenic Co-operative Oncology Group study. Acta Oncol. (1994) 33:825–30. doi: 10.3109/02841869409083955
28. Homma A, Inamura N, Oridate N, Suzuki S, Hatakeyama H, Mizumachi T, et al. Concomitant weekly cisplatin and radiotherapy for head and neck cancer. Jpn J Clin Oncol. (2011) 41:980–6. doi: 10.1093/jjco/hyr086
29. Osman N, Elamin YY, Rafee S, O'Brien C, Stassen LF, Timon C, et al. Weekly cisplatin concurrently with radiotherapy in head and neck squamous cell cancer: a retrospective analysis of a tertiary institute experience. Eur Arch Otorhinolaryngol. (2014) 271:2253–9. doi: 10.1007/s00405-013-2749-9
30. Jacobs C, Bertino JR, Goffinet DR, Fee WE, Goode RL. 24-hour infusion of cis-platinum in head and neck cancers. Cancer. (1978) 42:2135–40. doi: 10.1002/1097-0142(197811)42:5<2135::AID-CNCR2820420508>3.0.CO;2-W
31. Creagan ET, O'Fallon JR, Woods JE, Ingle JN, Schutt AJ, Nichols WC. Cis-diamminedichloroplatinum (II) administered by 24-hour infusion in the treatment of patients with advanced upper aerodigestive cancer. Cancer. (1983) 51:2020–23. doi: 10.1002/1097-0142(19830601)51:11<2020::AID-CNCR2820511110>3.0.CO;2-X
32. Veronesi A, Zagonel V, Tirelli U, Galligioni E, Tumolo S, Barzan L, et al. High-dose versus low-dose cisplatin in advanced head and neck squamous carcinoma: a randomized study. J Clin Oncol. (1985) 3:1105–8. doi: 10.1200/JCO.1985.3.8.1105
33. Sako K, Razack MS, Kalnins I. Chemotherapy for advanced and recurrent squamous cell carcinoma of the head and neck with high and low dose cis-diamminedichloroplatinum. Am J Surg. (1978) 136:529–33. doi: 10.1016/0002-9610(78)90276-3
34. De la Cal C, Fernandez-Solari J, Mohn C, Prestifilippo J, Pugnaloni A, Medina V, et al. Radiation produces irreversible chronic dysfunction in the submandibular glands of the rat. Open Dent J. (2012) 6:8–13. doi: 10.2174/1874210601206010008
35. Ahn MJ, D'Cruz A, Vermorken JB, Chen JP, Chitapanarux I, Dang HQ, et al. Clinical recommendations for defining platinum unsuitable head and neck cancer patient populations on chemoradiotherapy: a literature review. Oral Oncol. (2016) 53:10–6. doi: 10.1016/j.oraloncology.2015.11.019
36. DeVita VT, Lawrence TS, Rosenberg SA. Cancer: Principles & Practice of Oncology. 11th edn. Philadelphia, PA: Wolters Kluwer 2018.
37. Garden AS, Harris J, Vokes EE, Forastiere AA, Ridge JA, Jones C, et al. Preliminary results of Radiation Therapy Oncology Group 97-03: a randomized phase II trial of concurrent radiation and chemotherapy for advanced squamous cell carcinomas of the head and neck. J Clin Oncol. (2004) 22:2856–64. doi: 10.1200/JCO.2004.12.012
38. Karasawa T, Steyger PS. An integrated view of cisplatin-induced nephrotoxicity and ototoxicity. Toxicol Lett. (2015) 237:219–27. doi: 10.1016/j.toxlet.2015.06.012
39. Miller RP, Tadagavadi RK, Ramesh G, Reeves WB. Mechanisms of cisplatin nephrotoxicity. Toxins. (2010) 2:2490–518. doi: 10.3390/toxins2112490
40. Launay-Vacher V, Rey JB, Isnard-Bagnis C, Deray G, Daouphars M, European Society of Clinical Pharmacy Special Interest Group on Cancer Care. Prevention of cisplatin nephrotoxicity: state of the art and recommendations from the European Society of Clinical Pharmacy Special Interest Group on Cancer Care. Cancer Chemother Pharmacol. (2008) 61:903–9. doi: 10.1007/s00280-008-0711-0
41. de Castro G, Alves GV, Castro AF, Chaves ALF, De Marchi P, de Oliveira TB, et al. Criteria for eligibility to cisplatin in the curative treatment of head and neck cancer: consensus opinion from a panel of experts. Crit Rev Oncol Hematol. (2018) 131:30–4. doi: 10.1016/j.critrevonc.2018.08.009
42. Cavaletti G, Bogliun G, Marzorati L, Zincone A, Piatti M, Colombo N, et al. Early predictors of peripheral neurotoxicity in cisplatin and paclitaxel combination chemotherapy. Ann Oncol. (2004) 15:1439–42. doi: 10.1093/annonc/mdh348
43. Paken J, Govender CD, Pillay M, Sewram V. Cisplatin-associated ototoxicity: a review for the health professional. J Toxicol. (2016) 2016:1809394. doi: 10.1155/2016/1809394
44. Rademaker-Lakhai JM, Crul M, Zuur L, Baas P, Beijnen JH, Simis YJ, et al. Relationship between cisplatin administration and the development of ototoxicity. J Clin Oncol. (2006) 24:918–24. doi: 10.1200/JCO.2006.10.077
45. Kanat O, Ertas H, Caner B. Platinum-induced neurotoxicity: a review of possible mechanisms. World J Clin Oncol. (2017) 8:329–35. doi: 10.5306/wjco.v8.i4.329
46. McWhinney SR, Goldberg RM, McLeod HL. Platinum neurotoxicity pharmacogenetics. Mol Cancer Ther. (2009) 8:10–6. doi: 10.1158/1535-7163.MCT-08-0840
47. Argyriou AA, Bruna J, Marmiroli P, Cavaletti G. Chemotherapy-induced peripheral neurotoxicity (CIPN): an update. Crit Rev Oncol Hematol. (2012) 82:51–77. doi: 10.1016/j.critrevonc.2011.04.012
48. Thompson SW, Davis LE, Kornfeld M, Hilgers RD, Standefer JC. Cisplatin neuropathy. Clinical, electrophysiologic, morphologic, and toxicologic studies. Cancer. (1984) 54:1269–75. doi: 10.1002/1097-0142(19841001)54:7<1269::AID-CNCR2820540707>3.0.CO;2-9
49. von Schlippe M, Fowler CJ, Harland SJ. Cisplatin neurotoxicity in the treatment of metastatic germ cell tumour: time course and prognosis. Br J Cancer. (2001) 85:823–6. doi: 10.1054/bjoc.2001.2006
50. Ko C, Citrin D. Radiotherapy for the management of locally advanced squamous cell carcinoma of the head and neck. Oral Dis. (2009) 15:121–32. doi: 10.1111/j.1601-0825.2008.01495.x
51. Rybak LP, Whitworth CA, Mukherjea D, Ramkumar V. Mechanisms of cisplatin-induced ototoxicity and prevention. Hear Res. (2007) 226:157–67. doi: 10.1016/j.heares.2006.09.015
52. Sun Y, Yu X-L, Luo W, Lee AW, Wee JT, Lee N, et al. Recommendation for a contouring method and atlas of organs at risk in nasopharyngeal carcinoma patients receiving intensity-modulated radiotherapy. Radiother Oncol. (2014) 110:390–7. doi: 10.1016/j.radonc.2013.10.035
53. Filipski KK, Mathijssen RH, Mikkelsen TS, Schinkel AH, Sparreboom A. Contribution of organic cation transporter 2 (OCT2) to cisplatin-induced nephrotoxicity. Clin Pharmacol Ther. (2009) 86:396–402. doi: 10.1038/clpt.2009.139
54. Pabla N, Murphy RF, Liu K, Dong Z. The copper transporter Ctr1 contributes to cisplatin uptake by renal tubular cells during cisplatin nephrotoxicity. Am J Physiol Renal Physiol. (2009) 296:F505–11. doi: 10.1152/ajprenal.90545.2008
55. Zhang B, Ramesh G, Norbury CC, Reeves WB. Cisplatin-induced nephrotoxicity is mediated by tumor necrosis factor-α produced by renal parenchymal cells. Kidney Int. (2007) 72:37–44. doi: 10.1038/sj.ki.5002242
56. Roncal-Jimenez C, Lanaspa MA, Jensen T, Sanchez-Lozada LG, Johnson RJ. Mechanisms by which dehydration may lead to chronic kidney disease. Ann Nutr Metab. (2015) 66(Suppl 66):10–3. doi: 10.1159/000381239
57. Oronsky B, Caroen S, Oronsky A, Dobalian A, Oronsky N, Lybeck M, et al. Electrolyte disorders with platinum-based chemotherapy: mechanisms, manifestations and management. Cancer Chemother Pharmacol. (2017) 80:895–907. doi: 10.1007/s00280-017-3392-8
58. Roila F, Molassiotis A, Herrstedt J, Aapro M, Gralla RJ, Bruera E, et al. 2016 MASCC and ESMO guideline update for the prevention of chemotherapy- and radiotherapy-induced nausea and vomiting and of nausea and vomiting in advanced cancer patients. Ann Oncol. (2016) 27(Suppl 27):v119–33. doi: 10.1093/annonc/mdw270
59. Hesketh PJ, Kris MG, Basch E, Bohlke K, Barbour SY, Clark-Snow RA, et al. Antiemetics: American Society of Clinical Oncology clinical practice guideline update. J Clin Oncol. (2017) 35:3240–61. doi: 10.1200/JCO.2017.74.4789
60. Schnell FM. Chemotherapy-induced nausea and vomiting: the importance of acute antiemetic control. Oncologist. (2003) 8:187–98. doi: 10.1634/theoncologist.8-2-187
61. Nelms M, Sucher KP. Nutrition therapy. In Nelms M, Sucher KP, Lacey K, et al. (eds). Nutrition Therapy and Pathophysiology, 3rd edn. Boston, MA: Cengage Learning (2016), p. 698–706.
62. IJpma I, Timmermans ER, Renken RJ, Ter Horst GJ, Reyners AK. Metallic taste in cancer patients treated with systemic therapy: a questionnaire-based study. Nutr Cancer. (2017) 69:140–5. doi: 10.1080/01635581.2017.1250922
63. Mortensen HR, Jensen K, Grau C. Aspiration pneumonia in patients treated with radiotherapy for head and neck cancer. Acta Oncol. (2013) 52:270–6. doi: 10.3109/0284186X.2012.742205
64. Nguyen NP, Moltz CC, Frank C, Vos P, Smith HJ, Karlsson U, et al. Dysphagia following chemoradiation for locally advanced head and neck cancer. Ann Oncol. (2004) 15:383–8. doi: 10.1093/annonc/mdh101
65. Caudell JJ, Schaner PE, Meredith RF, Locher JL, Nabell LM, Carroll WR, et al. Factors associated with long-term dysphagia after definitive radiotherapy for locally advanced head-and-neck cancer. Int J Radiat Oncol Biol Phys. (2009) 73:410–5. doi: 10.1016/j.ijrobp.2008.04.048
66. Bellmunt J, Orsola A, Leow JJ, Wiegel T, De Santis M, Horwich A, ESMO Guidelines Working Group. Bladder cancer: ESMO practice guidelines for diagnosis, treatment and follow-up. Ann Oncol. (2014) 25(Suppl 25):iii40–8. doi: 10.1093/annonc/mdu223
67. Besse B, Adjei A, Baas P, Meldgaard P, Nicolson M, Paz-Ares L, et al. 2nd ESMO Consensus Conference on Lung Cancer: non-small-cell lung cancer first-line/second and further lines of treatment in advanced disease. Ann Oncol. (2014) 25:1475–84. doi: 10.1093/annonc/mdu123
68. De Marinis F, Bria E, Baas P, Tiseo M, Camerini A, Favaretto AG, et al. Treatment of unfit patients with advanced non-small-cell lung cancer: definition criteria according an expert panel. Clin Lung Cancer. (2015) 16:399–405. doi: 10.1016/j.cllc.2015.04.008
69. Galsky MD, Hahn NM, Rosenberg J, Sonpavde G, Hutson T, Oh WK, et al. Treatment of patients with metastatic urothelial cancer “unfit” for cisplatin-based chemotherapy. J Clin Oncol. (2011) 29:2432–8. doi: 10.1200/JCO.2011.34.8433
70. Galsky MD, Hahn NM, Rosenberg J, Sonpavde G, Hutson T, Oh WK, et al. A consensus definition of patients with metastatic urothelial carcinoma who are unfit for cisplatin-based chemotherapy. Lancet Oncol. (2011) 12:211–4. doi: 10.1016/S1470-2045(10)70275-8
71. Base de Données Publique de Médicaments. CISPLATINE TEVA 1 mg/1 mL, Solution pour Perfusion—Résumé des Caractéristiques du Produit [CISPLATIN TEVA 1 mg/mL, Solution for Infusion - Summary of Product Characteristics]. Available online at: http://base-donnees-publique.medicaments.gouv.fr/affichageDoc.php?specid=68377552&typedoc=R (accessed October 8, 2018).
72. Müller von der Grün J, Martin D, Stöver T, Ghanaati S, Rödel C, Balermpas P. Chemoradiotherapy as definitive treatment for elderly patients with head and neck cancer. Biomed Res Int. (2018) 2018:3508795. doi: 10.1155/2018/3508795
73. Moye VA, Chandramouleeswaran S, Zhao N, Muss HB, Weissler MC, Hayes DN, et al. Elderly patients with squamous cell carcinoma of the head and neck and the benefit of multimodality therapy. Oncologist. (2015) 20:159–65. doi: 10.1634/theoncologist.2013-0325
74. Szturz P, Vermorken JB. Treatment of elderly patients with squamous cell carcinoma of the head and neck. Front Oncol. (2016) 6:199. doi: 10.3389/fonc.2016.00199
75. Quoix E. Therapeutic options in older patients with metastatic non-small cell lung cancer. Ther Adv Med Oncol. (2012) 4:247–54. doi: 10.1177/1758834012455838
76. National Institute of Neurological Disorders and Stroke. Peripheral Neuropathy Fact Sheet. Available online at: https://www.ninds.nih.gov/Disorders/Patient-Caregiver-Education/Fact-Sheets/Peripheral-Neuropathy-Fact-Sheet (accessed October 8, 2018).
77. Grisold W, Cavaletti G, Windebank AJ. Peripheral neuropathies from chemotherapeutics and targeted agents: diagnosis, treatment, and prevention. Neuro Oncol. (2012) 14(Suppl 14):iv45–54. doi: 10.1093/neuonc/nos203
78. Gerchman F, Tong J, Utzschneider KM, Zraika S, Udayasankar J, McNeely MJ, et al. Body mass index is associated with increased creatinine clearance by a mechanism independent of body fat distribution. J Clin Endocrinol Metab. (2009) 94:3781–8. doi: 10.1210/jc.2008-2508
79. Motwani SS, McMahon GM, Humphreys BD, Partridge AH, Waikar SS, Curhan GC. Development and validation of a risk prediction model for acute kidney injury after the first course of cisplatin. J Clin Oncol. (2018) 36:682–8. doi: 10.1200/JCO.2017.75.7161
80. Argiris A, Li Y, Murphy BA, Langer CJ, Forastiere AA. Outcome of elderly patients with recurrent or metastatic head and neck cancer treated with cisplatin-based chemotherapy. J Clin Oncol. (2004) 22:262–8. doi: 10.1200/JCO.2004.08.039
81. Aapro M, Beguin Y, Bokemeyer C, Dicato M, Gascón P, Glaspy J. Management of anaemia and iron deficiency in patients with cancer: ESMO Clinical Practice Guidelines. Ann Oncol. (2018) 29(Suppl 29):iv271. doi: 10.1093/annonc/mdy323
82. Extermann M, Boler I, Reich RR, Lyman GH, Brown RH, DeFelice J, et al. Predicting the risk of chemotherapy toxicity in older patients: the Chemotherapy Risk Assessment Scale for High-Age Patients (CRASH) score. Cancer. (2012) 118:3377–86. doi: 10.1002/cncr.26646
83. Reece PA, Stafford I, Abbott RL, Anderson C, Denham J, Freeman S, et al. Two- versus 24-hour infusion of cisplatin: pharmacokinetic considerations. J Clin Oncol. (1989) 7:270–5. doi: 10.1200/JCO.1989.7.2.270
84. Rancati T, Schwarz M, Allen AM, Feng F, Popovtzer A, Mittal B, et al. Radiation dose-volume effects in the larynx and pharynx. Int J Radiat Oncol Biol Phys. (2010) 76(Suppl 76):S64–9. doi: 10.1016/j.ijrobp.2009.03.079
85. Popovtzer A, Cao Y, Feng FY, Eisbruch A. Anatomical changes in the pharyngeal constrictors after chemo-irradiation of head and neck cancer and their dose-effect relationships: MRI-based study. Radiother Oncol. (2009) 93:510–5. doi: 10.1016/j.radonc.2009.05.013
86. Merck Manual Professional Version. Drug-Induced Ototoxicity. Available online at: http://www.merckmanuals.com/professional/ear,-nose,-and-throat-disorders/inner-ear-disorders/drug-induced-ototoxicity (accessed October 8, 2018).
87. Amptoulach S, Tsavaris N. Neurotoxicity caused by the treatment with platinum analogues. Chemother Res Pract. (2011) 2011:843019. doi: 10.1155/2011/843019
88. Hitchcock YJ, Tward JD, Szabo A, Bentz BG, Shrieve DC. Relative contributions of radiation and cisplatin-based chemotherapy to sensorineural hearing loss in head-and-neck cancer patients. Int J Radiat Oncol Biol Phys. (2009) 73:779–88. doi: 10.1016/j.ijrobp.2008.05.040
89. Heidemann HT, Gerkens JF, Jackson EK, Branch RA. Attenuation of cisplatinum-induced nephrotoxicity in the rat by high salt diet, furosemide and acetazolamide. Naunyn Schmiedebergs Arch Pharmacol. (1985) 329:201–5. doi: 10.1007/BF00501213
90. Pera MF, Zook BC, Harder HC. Effects of mannitol or furosemide diuresis on the nephrotoxicity and physiological disposition of cis-dichlorodiammineplatinum-(II) in rats. Cancer Res. (1979) 39:1269–78.
91. Lehane D, Winston A, Gray R, Daskal Y. The effect of diuretic pre-treatment on clinical, morphological and ultrastructural cis-platinum induced nephrotoxicity. Int J Radiat Oncol Biol Phys. (1979) 5:1393–9. doi: 10.1016/0360-3016(79)90677-1
92. Hong AM, Martin A, Chatfield M, Jones D, Zhang M, Armstrong B, et al. Human papillomavirus, smoking status and outcomes in tonsillar squamous cell carcinoma. Int J Cancer. (2013) 132:2748–54. doi: 10.1002/ijc.27956
93. O'Sullivan B, Huang SH, Siu LL, Waldron J, Zhao H, Perez-Ordonez B, et al. Deintensification candidate subgroups in human papillomavirus-related oropharyngeal cancer according to minimal risk of distant metastasis. J Clin Oncol. (2013) 31:543–50. doi: 10.1200/JCO.2012.44.0164
94. Fakhry C, Westra WH, Li S, Cmelak A, Ridge JA, Pinto H, et al. Improved survival of patients with human papillomavirus-positive head and neck squamous cell carcinoma in a prospective clinical trial. J Natl Cancer Inst. (2008) 100:261–9. doi: 10.1093/jnci/djn011
95. Gillison ML, Trotti AM, Harris J, Eisbruch A, Harari PM, Adelstein DJ, et al. Radiotherapy plus cetuximab or cisplatin in human papillomavirus-positive oropharyngeal cancer (NRG Oncology RTOG 1016): a randomised, multicentre, non-inferiority trial. Lancet. (2019) 393:40–50. doi: 10.1016/S0140-6736(18)32779-X
96. Mehanna H, Robinson M, Hartley A, Kong A, Foran B, Fulton-Lieuw T, et al. Radiotherapy plus cisplatin or cetuximab in low-risk human papillomavirus-positive oropharyngeal cancer (De-ESCALaTE HPV): an open-label randomised controlled phase 3 trial. Lancet. (2019) 393:51–60. doi: 10.1016/S0140-6736(18)32752-1
97. ClinicalTrials.gov. Weekly Cetuximab/RT Versus Weekly Cisplatin/RT in HPV-Associated Oropharyngeal Squamous Cell Carcinoma (HPVOropharynx). Available online at: https://clinicaltrials.gov/ct2/show/NCT01855451 (accessed October 8, 2018).
98. Yom SS, Torres-Saavedra P, Caudell JJ, Waldron JN, Gillison ML, Truong MT, et al. NRG-HN002: a randomized phase II trial for patients with p16-positive, non-smoking-associated, locoregionally advanced oropharyngeal cancer. Int J Radiat Oncol Biol Phys. (2019) 105:684–5. doi: 10.1016/j.ijrobp.2019.08.038
99. Lacas B, Bourhis J, Overgaard J, Zhang Q, Grégoire V, Nankivell M, et al. Role of radiotherapy fractionation in head and neck cancers (MARCH): an updated meta-analysis. Lancet Oncol. (2017) 18:1221–37. doi: 10.1016/S1470-2045(17)30458-8
100. Tchekmedyian V, Ho AL, Dunn L, Fetten JV, Pfister RG, Lobaugh S, et al. A retrospective analysis of cisplatin dosing strategies when used with radiation on outcomes in head and neck squamous cell carcinoma of the oropharynx. J Clin Oncol. (2019) 37(Suppl 37):6079. doi: 10.1200/JCO.2019.37.15_suppl.6079
101. Noronha V, Joshi A, Patil VM, Agarwal J, Ghosh-Laskar S, Budrukkar A, et al. Once-a-week versus once-every-3-weeks cisplatin chemoradiation for locally advanced head and neck cancer: a phase III randomized noninferiority trial. J Clin Oncol. (2017) 36:1064–72. doi: 10.1200/JCO.2017.35.15_suppl.6007
102. Quon H, Leong T, Haselow R, Leipzig B, Cooper J, Forastiere A, et al. Phase III study of radiation therapy with or without cis-platinum in patients with unresectable squamous or undifferentiated carcinoma of the head and neck: an intergroup trial of the Eastern Cooperative Oncology Group (E2382). Int J Radiat Oncol Biol Phys. (2011) 81:719–25. doi: 10.1016/j.ijrobp.2010.06.038
103. Guan J, Li Q, Zhang Y, Xiao N, Chen M, Zhang Y, et al. A meta-analysis comparing cisplatin-based to carboplatin-based chemotherapy in moderate to advanced squamous cell carcinoma of head and neck (SCCHN). Oncotarget. (2016) 7:7110–9. doi: 10.18632/oncotarget.6858
104. Porceddu SV, Bressel M, Poulsen MG, Stoneley A, Veness MJ, Kenny LM, et al. Postoperative concurrent chemoradiotherapy versus postoperative radiotherapy in high-risk cutaneous squamous cell carcinoma of the head and neck: the randomized phase III TROG 05.01 trial. J Clin Oncol. (2018) 36:1275–83. doi: 10.1200/JCO.2017.77.0941
105. Denis F, Garaud P, Bardet E, Alfonsi M, Sire C, Germain T, et al. Final results of the 94-01 French Head and Neck Oncology and Radiotherapy Group randomized trial comparing radiotherapy alone with concomitant radiochemotherapy in advanced-stage oropharynx carcinoma. J Clin Oncol. (2004) 22:69–76. doi: 10.1200/JCO.2004.08.021
106. Bourhis J, Sire C, Graff P, Grégoire V, Maingon P, Calais G, et al. Concomitant chemoradiotherapy versus acceleration of radiotherapy with or without concomitant chemotherapy in locally advanced head and neck carcinoma (GORTEC 99-02): an open-label phase 3 randomised trial. Lancet Oncol. (2012) 13:145–53. doi: 10.1016/S1470-2045(11)70346-1
107. Geoffrois L, Martin L, De Raucourt D, Sun XS, Tao Y, Maingon P, et al. Induction chemotherapy followed by cetuximab radiotherapy is not superior to concurrent chemoradiotherapy for head and neck carcinomas: results of the GORTEC 2007-02 phase III randomized trial. J Clin Oncol. (2018) 36:3077–83. doi: 10.1200/JCO.2017.76.2591
108. Budach V, Cho C-H, Sedlmaier B, Wittlinger M, Iro H, Engenhart-Cabillic R, et al. Five years' results of the German ARO 04-01 trial of concurrent 72 Gy hyperfractionated accelerated radiation therapy (HART) plus once weekly cisplatinum/5-FU versus mitomycin C/5-FU in stage IV head and neck cancer. J Clin Oncol. (2012) 30(Suppl 30):5512. doi: 10.1200/jco.2012.30.15_suppl.5512
109. Bonner JA, Harari PM, Giralt J, Azarnia N, Shin DM, Cohen RB, et al. Radiotherapy plus cetuximab for squamous-cell carcinoma of the head and neck. N Engl J Med. (2006) 354:567–78. doi: 10.1056/NEJMoa053422
110. Bonner JA, Harari PM, Giralt J, Cohen RB, Jones CU, Sur RK, et al. Radiotherapy plus cetuximab for locoregionally advanced head and neck cancer: 5-year survival data from a phase 3 randomised trial, and relation between cetuximab-induced rash and survival. Lancet Oncol. (2010) 11:21–8. doi: 10.1016/S1470-2045(09)70311-0
111. National Cancer Institute. Cetuximab. Available online at: https://www.cancer.gov/about-cancer/treatment/drugs/cetuximab (accessed October 8, 2018).
112. Dattatreya S, Goswami C. Cetuximab plus radiotherapy in patients with unresectable locally advanced squamous cell carcinoma of head and neck region—a open labelled single arm phase II study. Indian J Cancer. (2011) 48:154–7. doi: 10.4103/0019-509X.82873
113. Okano S, Yoshino T, Fujii M, Onozawa Y, Kodaira T, Fujii H, et al. Phase II study of cetuximab plus concomitant boost radiotherapy in Japanese patients with locally advanced squamous cell carcinoma of the head and neck. Jpn J Clin Oncol. (2013) 43:476–82. doi: 10.1093/jjco/hyt030
114. Bernier J, Russi EG, Homey B, Merlano MC, Mesía R, Peyrade F, et al. Management of radiation dermatitis in patients receiving cetuximab and radiotherapy for locally advanced squamous cell carcinoma of the head and neck: proposals for a revised grading system and consensus management guidelines. Ann Oncol. (2011) 22:2191–200. doi: 10.1093/annonc/mdr139
115. Russi EG, Bensadoun RJ, Merlano MC, Bourhis J, Ricardi U, Giralt J, et al. Bio-radiation dermatitis: the need of a new grading. Ann Oncol. (2013) 24:2463–5. doi: 10.1093/annonc/mdt281
116. Curran D, Giralt J, Harari PM, Ang KK, Cohen RB, Kies MS, et al. Quality of life in head and neck cancer patients after treatment with high-dose radiotherapy alone or in combination with cetuximab. J Clin Oncol. (2007) 25:2191–7. doi: 10.1200/JCO.2006.08.8005
117. Suntharalingam M, Kwok Y, Goloubeva O, Parekh A, Taylor R, Wolf J, et al. Phase II study evaluating the addition of cetuximab to the concurrent delivery of weekly carboplatin, paclitaxel, and daily radiotherapy for patients with locally advanced squamous cell carcinomas of the head and neck. Int J Radiat Oncol Biol Phys. (2012) 82:1845–50. doi: 10.1016/j.ijrobp.2011.02.062
118. Corry J, Bressel M, Fua T, Herschtal A, Solomon B, Porceddu SV, et al. Prospective study of cetuximab, carboplatin, and radiation therapy for patients with locally advanced head and neck squamous cell cancer unfit for cisplatin. Int J Radiat Oncol Biol Phys. (2017) 98:948–54. doi: 10.1016/j.ijrobp.2017.02.088
119. Tao Y, Auperin A, Sire C, Martin L, Khoury C, Maingon P, et al. Improved outcome by adding concurrent chemotherapy to cetuximab and radiotherapy for locally advanced head and neck carcinomas: results of the GORTEC 2007-01 phase III randomized trial. J Clin Oncol. (2018) 36:3084–90. doi: 10.1200/JCO.2017.76.2518
120. Lee NY, Ferris RL, Beck JT, Harrington K, Haddad RI, Bourhis J, et al. JAVELIN head and neck 100: a phase 3 trial of avelumab in combination with chemoradiotherapy (CRT) vs CRT for 1st-line treatment of locally advanced squamous cell carcinoma of the head and neck (LA SCCHN). J Clin Oncol. (2017) 35(Suppl 35):TPS6093. doi: 10.1200/JCO.2017.35.15_suppl.TPS6093
121. Powell SF, Gitau MM, Sumey CJ, Reynolds JT, Lohr M, McGraw S, et al. Safety of pembrolizumab with chemoradiation (CRT) in locally advanced squamous cell carcinoma of the head and neck (LA-SCCHN). J Clin Oncol. (2017) 35(Suppl 35):6011. doi: 10.1200/JCO.2017.35.15_suppl.6011
122. Machiels J-PH, Licitra L, Rischin D, Waldron J, Burtness B, Gregoire V, et al. KEYNOTE-412: pembrolizumab (pembro) in combination with chemoradiation versus chemoradiation alone in locally advanced head and neck squamous cell carcinoma (LA-HNSCC). J Clin Oncol. (2017) 35(Suppl 35):TPS6090. doi: 10.1200/JCO.2017.35.15_suppl.TPS6090
123. Sun XS, Sire C, Tao Y, Martin L, Alfonsi M, Prevost JB, et al. A phase II randomized trial of pembrolizumab versus cetuximab, concomitant with radiotherapy (RT) in locally advanced (LA) squamous cell carcinoma of the head and neck (SCCHN): first results of the GORTEC 2015-01 “PembroRad” trial. J Clin Oncol. (2018) 36(Suppl 36):6018. doi: 10.1200/JCO.2018.36.15_suppl.6018
124. Johnson JM, Bar Ad V, Lorber E, Luginbuhl A, Curry JM, Cognetti D, et al. Nivolumab and ipilimumab in combination with radiotherapy in patients with locally advanced head and neck cancer. Ann Oncol. (2018) 29(Suppl 29): viii372–99. doi: 10.1093/annonc/mdy287.082
125. Tao Y, Auperin A, Sun XS, Sire C, Martin L, Bera G, et al. Avelumab-cetuximab-radiotherapy (RT) versus standards of care (SoC) in locally advanced squamous cell carcinoma of the head and neck (SCCHN): safety phase of the randomized trial GORTEC 2017-01 (REACH). J Clin Oncol. (2018) 36(Suppl 36):6076. doi: 10.1200/JCO.2018.36.15_suppl.6076
Keywords: cisplatin, locally advanced squamous cell carcinoma of the head and neck, toxicity, cetuximab, radiotherapy, chemotherapy
Citation: Porceddu SV, Scotté F, Aapro M, Salmio S, Castro A, Launay-Vacher V and Licitra L (2020) Treating Patients With Locally Advanced Squamous Cell Carcinoma of the Head and Neck Unsuitable to Receive Cisplatin-Based Therapy. Front. Oncol. 9:1522. doi: 10.3389/fonc.2019.01522
Received: 23 August 2019; Accepted: 17 December 2019;
Published: 22 January 2020.
Edited by:
Jordi Giralt, Vall d'Hebron University Hospital, SpainReviewed by:
Panagiotis Balermpas, University Hospital Zürich, SwitzerlandNobuhiko Oridate, Yokohama City University, Japan
Copyright © 2020 Porceddu, Scotté, Aapro, Salmio, Castro, Launay-Vacher and Licitra. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Lisa Licitra, lisa.licitra@istitutotumori.mi.it