Prevalence and correlates of severe under-5 child anthropometric failure measured by the composite index of severe anthropometric failure in Bangladesh
 Mohammad Rocky Khan Chowdhury1
Mohammad Rocky Khan Chowdhury1  Hafiz T. A. Khan2
Hafiz T. A. Khan2  Mamunur Rashid3*†
Mamunur Rashid3*†  Md. Nazrul Islam Mondal4 Farzana Akhter Bornee5 Baki Billah1
Md. Nazrul Islam Mondal4 Farzana Akhter Bornee5 Baki Billah1- 1Epidemiology and Preventive Medicine, School of Public Health and Preventive Medicine, Faculty of Medicine, Nursing and Health Sciences, Monash University, Melbourne, VIC, Australia
- 2Health Promotion and Public Health, College of Nursing, Midwifery and Healthcare, University of West London, London, United Kingdom
- 3Department of Public Health Science, Faculty of Occupational and Health Sciences, University of Gävle, Gävle, Sweden
- 4Population Science and Human Resource Development, University of Rajshahi, Rajshahi, Bangladesh
- 5Department of Pediatrics, Bangabandhu Sheikh Mujib Medical University, Dhaka, Bangladesh
Background: Although Bangladesh has made noticeable progress in reducing the prevalence of stunting, wasting, and being underweight among under-5 children, it has not been very successful in reducing overall severe anthropometric failure (SAF) among them. Therefore, the study aims to identify the prevalence and risk factors of SAF measured by the Composite Index of Severe Anthropometric Failure (CISAF) among under-5 children in Bangladesh.
Methods: Data was drawn from a cross-sectional Bangladesh Demographic Health Survey (BDHS) conducted in 2017–2018. A bivariate analysis (Chi-square test) and logistic regression analysis were used to estimate the unadjusted, and age and sex-adjusted prevalence of SAF. Odds ratio (OR) and confidence interval (CI) were assessed using logistic regression analysis to identify the various risk factor of SAF.
Results: The overall adjusted prevalence of under-5 child SAF was 11.3% (95% CI: 10.6–12.0) and it was highly prevalent among children of uneducated mothers (adjusted, 22%, 95% CI: 17.3–26.8). The key factors associated with SAF were children in the age group 24–35 months (OR: 2.43, 95% CI: 1.83–3.23), children born with low birth weight (OR: 3.14, 95% CI: 2.24–4.97), children of underweight mothers (OR: 1.82, 95% CI: 1.44–2.29), children of parents with no formal education (OR: 2.28, 95% CI: 1.56–3.31) and children from lower socio-economic status (OR: 2.25, 95% CI: 1.55–3.26).
Conclusion: Prioritizing and ensuring context-specific interventions addressing individual, community, public policy, and environment level risk factors from policy level to implementation to reduce structural and intermediary determinants of under-5 SAF.
Introduction
Anthropometric failure (AF) in children shows itself in the form of stunting, wasting, and being underweight and remains one of the biggest health problems in low- and middle-income countries, including Bangladesh (1). Globally, around 195 million children under-5 suffer from some form of AF (2). Further, ~3 million children under-5 die from AF (2). Reduced dietary intakes of macro- and/or micronutrients and increased losses or enhanced requirements are some established causes of AF among under-5 children (3). Children with AF are physically, emotionally, and intellectually less productive than well-nourished children due to incompatible growth and development (4). In addition, short and long-term adverse health consequences including a degree of cognitive impairment, weak thymus development, a decreased peripheral lymphocyte count, an increased susceptibility to infections, and a poor immune system are all directly related to the severity of AF and often lead to death of a child have multiple exposures of these health consequences (5). Nearly 20 million children globally suffer from severe wasting (6), resulting in 1 million deaths per year by increasing susceptibility to death from severe infection (7). Children having severe wasting are usually 12 times more likely to die than a non-wasted or stunted child. On the other hand, a child having severe stunting also carries five times high risk of death than a non-wasted or stunted child (8).
Bangladesh has been identified as having a high burden of AF in its under-5 with a more than 40% prevalence rate (9). Although the country has made significant improvements in addressing the Millennium Development Goals (MDG) 1 (eradication of extreme poverty and hunger) and MDG-4 (child mortality), it has not been very successful in reducing AF in children particularly in its severest form (10). In Bangladesh, around 20% of children with severe anthropometric failure (SAF) were identified in 2014 (9). Further, factors, including poor maternal education, poor household economic status, low birth weight, poor infant and young child feeding practices, frequent infections, and inadequate access to health care, unsafe water and sanitation complexly interacted with severe stunting, severe wasting and being severe underweight in low and middle income countries including Bangladesh (9, 11, 12). These studies, however, only identified the risk factors for single form or multiple concurrent forms of severe stunting, severe wasting and being severely underweight that partly overlap, thus not providing a convincing estimate of the proportion of AF among children in the population.
The Composite Index of Anthropometric Failure (CIAF) uses conventional nutritional and growth indicators (stunting, wasting and underweight) to provide six different measurements, and the overall burden of AF was estimated by aggregating the values of conventional nutritional and growth indicators (13). The CIAF therefore, widely estimate the proportion of children with AF in the population (13). The Composite Index of Severe Anthropometric Failure (CISAF) followed by the methodological approach of CIAF that provides a comprehensive view of the overall burden of SAF in poor-resource settings (14). However, in Bangladesh, some socio-demographic factors were identified as risk factors of AF measured by the CIAF (15), no previous study used the CISAF to explore the national prevalence and complex interplay between individual, community, public policy and environment level risk factors and under-5 child SAF in Bangladesh. However, this study has considered already known etiology to identify the associated factors of SAF, investigating the change of direction of these factors using more recent data, especially in the context of SAF as per the CISAF, might be helpful for revising important policy decision-making. Therefore, we aim to explore the prevalence and risk factors of SAF by the CISAF in Bangladesh to help provide important insights for developing appropriate policy initiatives to address the severe adverse nutritional and growth outcome of under-5 children in the country.
Methods
Data source and study design
This study used data drawn from the 2017–2018 Bangladesh Demographic Health Surveys (BDHS) that showing around 99% response rate. In BDHS 2017–2018, enumeration areas (EAs) or primary sampling units (PSUs) and households were selected using multistage stratified sampling techniques to collect data from of adults (male and female) and children residing in non-institutional dwellings. The data collection was started on 24 October 2017 and ended on 15 March 2018. At the first stage, 675 PSUs (250 PSU from urban and 425 PSU from rural) were randomly selected from 293,579 PSUs (clusters) of the last census survey 2011 designed by the Bangladesh Bureau of Statistics using probability proportional to size technique. At the second stage, a systematic sample of 30 households from each PSU were selected using an equal probability systematic sampling technique. This multistage sampling technique, including its sampling weight, helps reduce potential sampling bias. In addition, all ever-married women aged 15–49 years from the pre-selected households were interviewed without replacement and change in the implementing stage to prevent selection bias (16). Informed consent was obtained verbally from each participant to collect information about them and their children before enrolling in the study. A significant number of the study sample was illiterate, so verbal consent was considered the most suitable option to confirm participation (16). The BDHS samples include socio-demographic data, health and nutritional indicators from Bangladeshi adults using a standard questionnaire. In 2017-18 survey, 8,759 under-5 children were found eligible for anthropometric measurement of which 7,776 were found credible for analysis (Figure 1). Further details of BDHS 2017-18 can be found elsewhere (16).
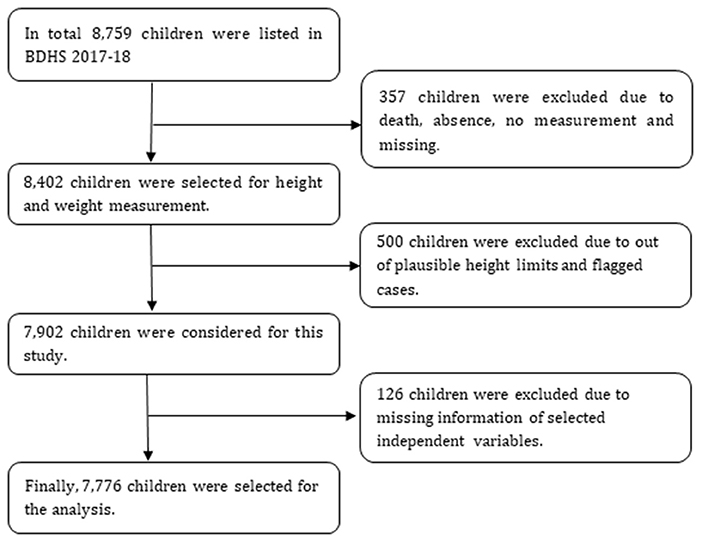
Figure 1. Schematic presentation of sample size selection.
Outcome variable
Severe nutritional and growth indicators for under-5 children were categorized into seven groups: (A) no severe failure; (B) severe wasting only; (C) severe stunting only; (D) severe underweight only; (E) severe wasting and severe underweight; (F) severe stunting and severe underweight; (G) severe wasting and severe stunting; (H) severe wasting, severe stunting and severe underweight (Table 1). A child is considered to have SAF if she/he has a severe form of any one out of three SAF's indicators (B, C and D) or their combinations from E to H (Figure 2).
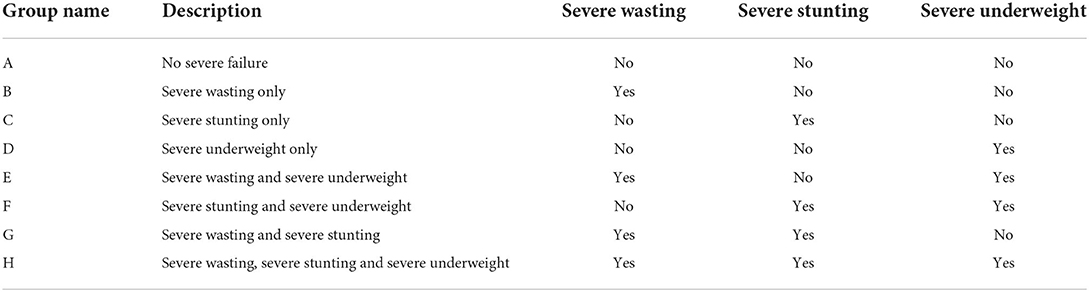
Table 1. Classification of children with severe anthropometric failure.
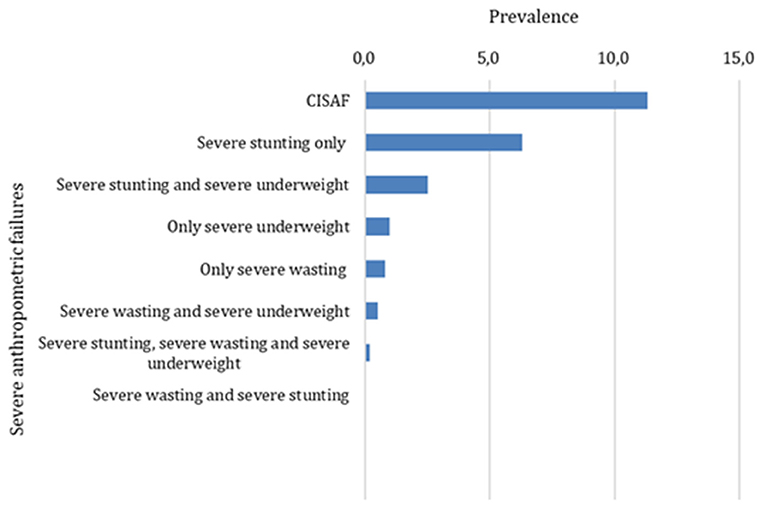
Figure 2. Prevalence of under-5 SAF.
The primary outcome measure was under-5 SAF using the CISAF (14). A child was considered to be, respectively, severely stunted (stature too short for age), severely wasted (extremely thin) and severely underweight (very low weight for age) if the height-for-age, weight-for-height, and weight-for-age indices were three Standard Deviations (SDs) or more below the respective median of the World Health Organization (WHO) reference population (17).
Independent variables
The literature indicates that a number of independent variables are important, and this study uses these variables to aid further investigation (9, 18, 19). The selected variables include maternal characteristics such as education of parents (both parents uneducated, only father uneducated—when mother educated, only mother uneducated—when father educated, both parents educated), mother's income-earning activities (currently not working, currently working), mother's BMI (≥ 18.5 kg/m2, <18.5 kg/m2), mothers received antenatal care (no, yes), mothers received postnatal care (no, yes), mother's attitude toward wife-beating (not justified, justified), mother's decision-making autonomy (not practiced, practiced) and number of living children (<3 children, three children and above); reproductive health related factors included unwanted child (no, yes), place of delivery (non-institutional, institutional), ever had terminated pregnancy (no, yes), last birth a cesarean section (no, yes) and sign of pregnancy complication (no, yes); children characteristics were children's age in months (0–11, 12–23, 24–35, 36–47, 48–59), sex of child (male, female), birth order (first, second third, fourth and above), low birth weight (no, yes) and currently had illness (no, yes); environmental characteristics included source of drinking water (improved, unimproved), solid fuel used in cooking (clean, solid) and type of toilet facility (improved, unimproved); household characteristics included mass media exposure through television, radio and newspaper/magazine (no, yes), and wealth index (poorest, poorer, middle, richer, richest); and contextual factor was place of residence (urban, rural) (16). Details explanations were provided in Appendix 1.
Statistical analysis
The background characteristics of the children were calculated using descriptive statistics. A Bivariate analysis and logistic regression were used for assessing the unadjusted and adjusted prevalence of SAF based on the CISAF. In all analyses, the significance level was set at p < 0.25 (Chi-square test) to include variables found important (20–22). Adjusted model was developed to analyze the appropriate binary value for SAF as per the CISAF. All independent variables found to be significant in the bivariate analysis (Chi-square test) were simultaneously entered into the multiple regression models for adjustment. Odds ratio (OR), risk difference (RD) and confidence interval (CI) were assessed to identify the factors associated with SAF where p < 0.05. The most influential factors were assessed using Wald statistics. The data were analyzed by controlling cluster (PSU) and stratum (urban area: city corporation area and other than city corporation area and rural area) with sampling weights that represent the whole country, both urban and rural areas, to ensure the precision of the estimates. Multicollinearity was checked by examining the standard errors (SEs) of regression coefficients in the logistic regression analyses. An SE >2.0 indicates multicollinearity among the independent variables (23). The SEs for the independent variables in the adjusted models for each outcome were <1, indicating an absence of multicollinearity. Stata version 14.2 (StataCorp LP, College Station, Texas) was used for all analyses to take account of the complex nature of the sampling weight of the BDHS 2017-18. To adjust sampling weight in the analysis, the Stata command “svyset” was used.
Results
Most of the women (around 35.0%) were from the age group 20–24 years. Mothers of ~7.0% of children had no formal education (both parents uneducated: 3.9% and only mothers were uneducated when fathers were educated: 3.2), fathers of around 11.3% of children had no formal education when mothers were educated, around 8% of mothers did not receive antenatal care and around 50% of birth delivery was non-institutional. More than two fifth (42.0%) of the children were <2 years of age and 52.0% of these were male. Around 42.0% of children were from low socio-economically and 68.0% of them were from rural areas (Table 2).

Table 2. Background characteristics of the respondents.
Prevalence of SAF based on the CISAF
The prevalence of overall severe stunting, severe wasting and severe underweight were, respectively, 9.1%, 4.2% and 1.8% (see Supplementary Figure 1). The adjusted prevalence of under-5 SAF based on the CISAF was 11.3%. The prevalence of only single form (only severe stunting, severe wasting or severe underweight) of SAF was 7.9% and multiple concurrent forms (severe stunting and severe underweight, severe wasting and severe underweight, and severe stunting, severe wasting and severe underweight) of SAF was (3.4%) (Figure 1). The adjusted prevalence of SAF was significantly higher consecutively among children of parents with (22.0%), children born with low birth weight (~19.0%), mothers that did not receive antenatal care (18.0%), children of underweight mothers (17.0%), children in fourth and above birth order (17.0%) and among children in the poorest section of the society (16.0%) (Table 3).
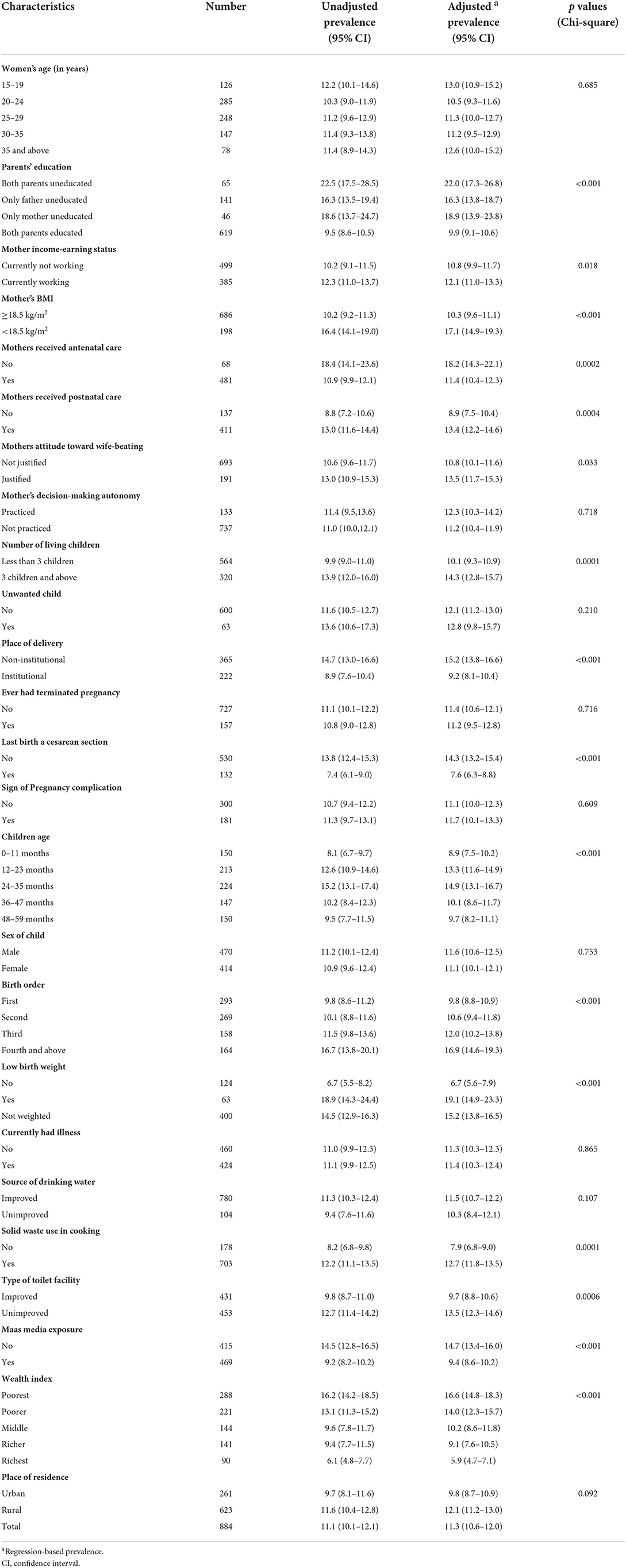
Table 3. Prevalence of SAF based on the CISAF among children under-5.
Factors associated with SAF
The most influential factors (based on Wald statistics) associated with under-5 SAF measured by the CISAF were children of age group 24–35 months (OR: 2.43, 95% CI: 1.83, 3.23, p < 0.001, Wald statistics: 6.13) (vs. youngest children), children born with low birth weight (OR: 3.33, 95% CI: 2.24, 4.97, p < 0.001, Wald statistics: 5.94) (vs. healthy weight children), children of underweight mothers (OR: 1.82, 95% CI: 1.44, 2.29, p < 0.001, Wald statistics: 5.09) (vs. healthy mothers), children of parents with no formal education (OR: 2.28, 95% CI: 1.56, 3.31, p < 0.001, Wald statistics: 4.31) (vs. children with educated parents), children from lower socio-economic quintile (OR: 2.25, 95% CI: 1.55, 3.26, p < 0.001, Wald statistics: 4.25) (vs. highest socio-economic quintile), children born by non-cesarean (OR: 1.56, 95% CI: 1.09, 2.22, p = 0.010, Wald statistics: 2.45) (vs. cesarean delivery) and children of mothers who did not receive antenatal care (OR: 1.54, 95% CI: 1.08, 2.20, p = 0.020, Wald statistics: 2.38) (vs. mothers received antenatal care) (Table 4).
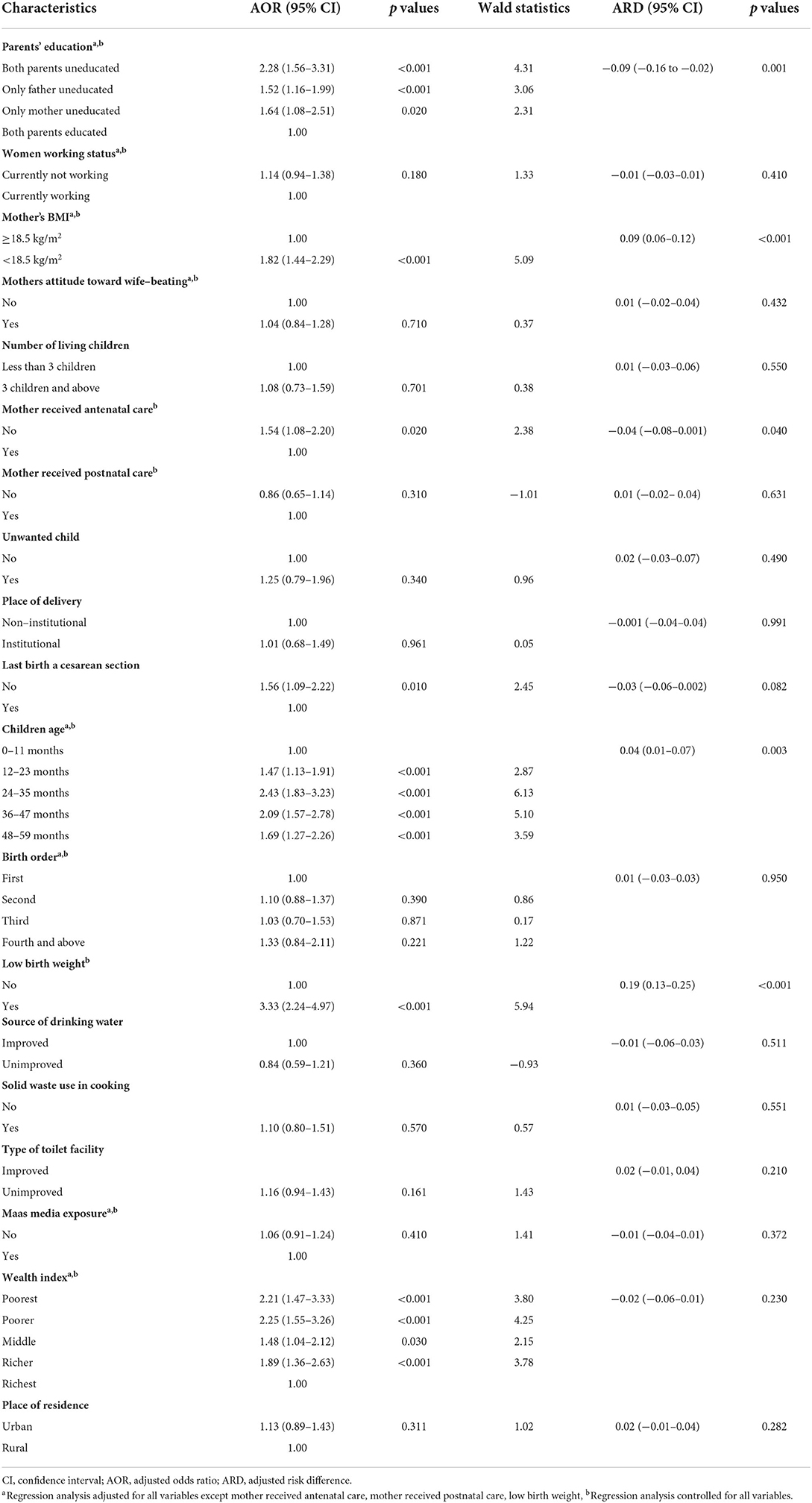
Table 4. Factors associated with SAF among under-5 children.
Significant adjusted risk differences (24) between no SAF and SAF were observed for indicators, such as, parents' education (ARD = −0.09), underweight mother (ARD = 0.09), mother received antenatal care (ARD = −0.04), children's age (ARD = 0.04) and low birth weight (ARD = 0.19) (Table 4).
Discussion
The prevalence of SAF among children under-5 in Bangladesh was 11.3%. In contrast, in the same population, the prevalence of severe stunting was 9% (16). Conventional indicators (i.e., severe stunting, severe wasting and severe underweight) can partly overlap, therefore may not provide a convincing estimate of the overall proportion of AF children in the population. On the other hand, CISAF uses conventional nutritional and growth indicators' aggregate values to estimate the overall proportion of SAF, thus provide a more convincing estimation of the overall proportion of AF children in the population (14). Previously no studies have widely addressed the overall proportion of SAF in Bangladesh based on the CISAF. Islam et al. recorded the prevalence of severe stunting (11.4%), severe wasting (3.1%) and severe underweight (7.7%) among children under-5 in Bangladesh using 2014 survey (25). In Nepal, Pravana et al. and Tiwari et al. revealed the prevalence of severe wasting (4.14%) and severe stunting (10.2%) respectively (26, 27). This study underlines that there are noticeable differences between the prevalence of SAF based on the CISAF and conventional disaggregated indicators in Bangladesh.
Most influential maternal characteristics associated with SAF were children of underweight mothers and children of parents with no formal education. Poor nutritional status of mothers is a potential risk factor of SAF (18, 25, 27). Mothers being underweight might affect the intrauterine growth of the fetus during the antenatal period, which in return affects the latter nutritional status of children (28). In addition, the poor nutritional status of women has been shown to be connected with poor distribution of inadequate food within the family along with food insecurity, poverty and micronutrient deficiencies that often tend to create macronutrient deficiencies in children (29). Again, parental education is another important associated factor of overall SAF has not been widely articulated apart from identifying association between parental educations and disaggregated conventional nutritional and growth indicators (i.e., stunting, wasting and underweight) (30, 31). Several studies have tried to introduce a link between mother's education and income by saying that increased schooling enables mothers to earn higher incomes and a similar argument can be made for paternal education that influences child's health (32, 33). However, it is difficult to assess the relative importance of income as a mediator for parental education effects. A comprehensive child SAF prevention package should include comprehensive health education and the use of nutritional interventions to enhance overall physical health and nutritional status of mothers and children (34).
Children of age group 24–35 months and born with low birth weight were more likely to suffer SAF. However, children born with low birthweight was previously identified as key factor associated with severe stunting in some developing countries like Pakistan, Nepal, Malawi, Mexico and Iran; Children of age group 24–35 months found insignificant in Nepal and Nigeria (18, 26, 35–38). After the 2nd year of life, children in Bangladesh tend to have the same diet as the family and only have access to inadequate amounts of solid food that can lead to a poor nutritional and growth status (39). Parents should offer healthy foods to the children age >2 years to avoid SAF. Exclusive breastfeeding is still not satisfactory in Bangladesh and this might have minimized the risk of AF in future (16). On the other hand, children with low birth weight experience faltered growth during early childhood that can lead to an increased risk of complications in later life (40). Children with synchronized conditions of AF and low birth weight have an increased susceptibility to infection such as diarrhea plus lower respiratory infections, sleep apnea, jaundice, anemia, chronic lung disorders, fatigue and loss of appetite (4). Appropriate initiation of complementary feeding might reduce the risk of SAF in later stage (41).
The odds of being SAF increased among children from less wealthy households, as also evidenced by various previous studies (6, 25, 42, 43). One fifth of the children living in socio-economically poorest households experienced SAF. Parents of having such status often cannot afford minimum diet and quality health care for their children (28, 44).
The findings indicate that Bangladesh has not yet achieved sustainable improvement in child nutrition and growth. Concerted efforts to enable strong collaboration among multiple sectors such as government, non-government, social, cultural, and religious institutions in order to improve nutritional and growth status are essential, particularly to address the severe adverse nutritional and growth outcomes. SAF can be reduced by taking measures to strengthen action around social determinants of health, such as, increasing the participation of women and girls in education, reducing socio-economic inequality by enhancing income generating sectors and establishing specific health and nutrition programmes. Further, empirical education and quality health care should be made available and accessible to all women will confer many benefits, for example, improve caregiver practices, enhance health and environmental knowledge; increase educated and skill work force; to live in better neighborhoods, reduce gender-based violence; reduces child marriage and early childbearing; reduces maternal death rates for the betterment of nutritional status and child development (45).
This study has several strengths. Firstly, a wide range of parental, household and child characteristics have been used to explain the SAF based on the CISAF among children under-5 living in Bangladesh. Secondly, the sample size is representative of that country and, based on the complex nature of the data, sophisticated statistical analyses have been used in order to meet the main objective of the study. There were limitations, however. For example, the cross-sectional nature of the study means that it was not possible to establish a causal relationship between risk factors and SAF. Diet practice, ethnicity and parental behavioral factors were not controlled in this study due to the unavailability of a large amount of necessary information covering these areas. Another limitation is recall bias or information bias that can occur from information collected by self-reporting such as age, education, occupation, and household assets etc. Overall, CISAF used seven measurements of nutritional and growth status provided a credible estimate of the overall proportion of under-5 SAF and the complex interplay between individual, community, public policy and environment level risk factors. Although the composite index is a more convincing estimate to represent the overall burden of SAF among under-5 children, it is not popular among pediatricians and public health researchers. Because this method has not been widely studied and validated, more research in this area is recommended.
Conclusion
The overall prevalence of under-5 child SAF was greater than conventional nutritional and growth indicators. One in 10 children experiences SAF in Bangladesh. Children born with low birth weight, those living in socio-economically poorest households, children of age group 24–35 months, children of underweight mothers and children in fourth and above birth order are important key factors associated with SAF. Prioritizing and ensuring context-specific interventions addressing individual, community, public policy and environment level risk factors from policy level to implementation to reduce structural and intermediary determinants of under-5 SAF.
Data availability statement
The datasets presented in this study can be found in online repositories. The names of the repository/repositories and accession number(s) can be found at: https://dhsprogram.com/data/available-datasets.cfm.
Ethics statement
Ethical approval for using the data was obtained from ICF International Rockville, Maryland, USA. Since the data was collected from secondary sources, ethical approval and written consent for participation were not required in this research.
Author contributions
MC designed the study plan. MC and HK performed statistical analyses. MC and FB prepared figures and tables. MC, FB, and MR drafted the manuscript. MM and BB edited it. All authors approved the study and the final manuscript.
Acknowledgments
The authors thank the MEASURE DHS project for their support and free access to the original data. The authors are thankful to the Oxford Institute of Population Aging, University of Oxford, UK for academic support, and would also like to acknowledge the support of the University of Gävle, Sweden, for open access permission for the article.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fped.2022.978568/full#supplementary-material
References
1. WHO/UNICEF. The Extension of the 2025 Maternal, Infant and Young Child Nutrition Targets to 2030. World Health Organization. (2019). Available online at: https://data.unicef.org/resources/who-unicef-discussion-paper-nutrition-targets/
2. UNICEF. Malnutrition Prevalence Remains Alarming: Stunting Is Declining Too Slowly While Wasting Still Impacts the Lives of Far too Many Young Children. (2020).
4. Rahman MS, Howlader T, Masud MS, Rahman ML. Association of low-birth weight with malnutrition in children under five years in Bangladesh: do mother's education, socio-economic status, and birth interval matter? PLoS ONE. (2016) 11:e0157814. doi: 10.1371/journal.pone.0157814
5. Khattak UK, Iqbal SP, Ghazanfar H. The role of parents' literacy in malnutrition of children under the age of five years in a semi-urban community of Pakistan: a case-control study. Cureus. (2017) 9:e1316. doi: 10.7759/cureus.1316
6. Khanal V, Sauer K, Karkee R, Zhao Y. Factors associated with small size at birth in Nepal: further analysis of Nepal Demographic and Health Survey 2011. BMC Pregn Childbirth. (2014) 14:1–9. doi: 10.1186/1471-2393-14-32
7. Williams P, Berkley JA. Severe Acute Malnutrition Update: Current Whoguidelines and the Whoessential Medicine List for Children. Geneva: World Health Organization. (2016).
9. Chowdhury MRK, Khan HT, Mondal MNI, Kabir R. Socio-demographic risk factors for severe malnutrition in children aged under five among various birth cohorts in Bangladesh. J Biosoc Sci. (2021) 53:590–605. doi: 10.1017/S0021932020000425
10. Chowdhury MRK, Rahman MS, Khan MMH, Mondal MNI, Rahman MM, Billah B. Risk factors for child malnutrition in Bangladesh: a multilevel analysis of a nationwide population-based survey. J Pediatr. (2016) 172:194–201.e1. doi: 10.1016/j.jpeds.2016.01.023
11. Madhusudhan K, Rajeev P, Shireesha A, Ushashree G. Study of risk factors of severe acute malnutrition (SAM) in children 6 months to 5 years of age and evaluation of effect of micronutrient supplementation (WHO protocol) on serum zinc and magnesium levels: a case control study. Int J Contemp Pediatr. (2017) 4:1198–205. doi: 10.18203/2349-3291.ijcp20172112
12. Kamal S. Socio-economic determinants of severe and moderate stunting among under-five children of rural Bangladesh. Malaysian J Nutr. (2011) 17:1.
13. Nandy S, Irving M, Gordon D, Subramanian S, Smith GD. Poverty, child undernutrition and morbidity: new evidence from India. Bull World Health Organization. (2005) 83:210–6.
14. Vollmer S, Harttgen K, Kupka R, Subramanian S. Levels and trends of childhood undernutrition by wealth and education according to a Composite Index of Anthropometric Failure: evidence from 146 Demographic and Health Surveys from 39 countries. BMJ Global Health. (2017) 2:e000206. doi: 10.1136/bmjgh-2016-000206
15. Islam MS, Biswas T. Prevalence and correlates of the composite index of anthropometric failure among children under 5 years old in Bangladesh. Maternal Child Nutr. (2020) 16:e12930. doi: 10.1111/mcn.12930
16. NIPORT. Bangladesh Demographic and Health Survey 2017-18. National Institute of Population Research and Training (NIPORT), and ICF Dhaka, Bangladesh, and Rockville, Maryland, USA. (2020).
17. WHO. WHO Child Growth Standards: Length/Height-for-Age, Weight-for-Age, Weight-for-Length, Weight-for-Height and Body Mass Index-for-Age: Methods and Development. World Health Organization (2006).
18. Akombi BJ, Agho KE, Hall JJ, Merom D, Astell-Burt T, Renzaho A. Stunting and severe stunting among children under-5 years in Nigeria: A multilevel analysis. BMC Pediatrics. (2017) 17:1–16. doi: 10.1186/s12887-016-0770-z
19. Kumar R, Abbas F, Mahmood T, Somrongthong R. Prevalence and factors associated with underweight children: a population-based subnational analysis from Pakistan. BMJ Open. (2019) 9:e028972. doi: 10.1136/bmjopen-2019-028972
20. Bursac Z, Gauss CH, Williams DK, Hosmer DW. Purposeful selection of variables in logistic regression. Source Code Biol Med. (2008) 3:1–8. doi: 10.1186/1751-0473-3-17
21. Thiese MS, Ronna B, Ott U. P value interpretations and considerations. J Thoracic Dis. (2016) 8:E928. doi: 10.21037/jtd.2016.08.16
22. Kim J. How to Choose the Level of Significance: A Pedagogical Note. (2015). doi: 10.2139/ssrn.2652773
24. Trehan I, Goldbach HS, LaGrone LN, Meuli GJ, Wang RJ, Maleta KM, et al. Research Article (New England Journal of Medicine) Antibiotics as part of the management of severe acute malnutrition. Malawi Med J. (2016) 28:123–30. doi: 10.1056/NEJMoa1202851
25. Islam MR, Rahman MS, Rahman MM, Nomura S, De Silva A, Lanerolle P, et al. Reducing childhood malnutrition in Bangladesh: the importance of addressing socio-economic inequalities. Public Health Nutr. (2020) 23:72–82. doi: 10.1017/S136898001900140X
26. Tiwari R, Ausman LM, Agho KE. Determinants of stunting and severe stunting among under-fives: evidence from the 2011 Nepal Demographic and Health Survey. BMC Pediatrics. (2014) 14:1–15. doi: 10.1186/1471-2431-14-239
27. Pravana NK, Piryani S, Chaurasiya SP, Kawan R, Thapa RK, Shrestha S. Determinants of severe acute malnutrition among children under 5 years of age in Nepal: a community-based case–control study. BMJ Open. (2017) 7:e017084. doi: 10.1136/bmjopen-2017-017084
28. Kasaye HK, Bobo FT, Yilma MT, Woldie M. Poor nutrition for under-five children from poor households in Ethiopia: Evidence from 2016 Demographic and Health Survey. PLoS ONE. (2019) 14:e0225996. doi: 10.1371/journal.pone.0225996
29. Sinha N, Deshmukh P, Garg B. Epidemiological correlates of nutritional anemia among children (6-35 months) in rural Wardha, Central India. Ind J Med Sci. (2008) 62:45–54. doi: 10.4103/0019-5359.39366
30. Mishra K, Kumar P, Basu S, Rai K, Aneja S. Risk factors for severe acute malnutrition in children below 5 y of age in India: a case-control study. Ind J Pediatrics. (2014) 81:762–5. doi: 10.1007/s12098-013-1127-3
31. Vollmer S, Bommer C, Krishna A, Harttgen K, Subramanian S. The association of parental education with childhood undernutrition in low-and middle-income countries: comparing the role of paternal and maternal education. Int J Epidemiol. (2017) 46:312–23. doi: 10.1093/ije/dyw133
32. Abuya B, Onsomu E, Kimani J, Moore D. Influence of maternal education on child immunization and stunting in Kenya. Mater Child Health J. (2011) 15:1389–99. doi: 10.1007/s10995-010-0670-z
33. Frost MB, Forste R, Haas DW. Maternal education and child nutritional status in Bolivia: finding the links. Soc Sci Med. (2005) 60:395–407. doi: 10.1016/j.socscimed.2004.05.010
34. WHO. Essential Nutrition Actions: Improving Maternal, Newborn, Infant and Young Child Health and Nutrition. World Health Organization (2013).
35. Ntenda PAM, Chuang Y-C. Analysis of individual-level and community-level effects on childhood undernutrition in Malawi. Pediatrics Neonatol. (2018) 59:380–9. doi: 10.1016/j.pedneo.2017.11.019
36. Saleemi M, Ashraf R, Mellander L, Zaman S. Determinants of stunting at 6, 12, 24 and 60 months and postnatal linear growth in Pakistani children. Acta Paediatrica. (2001) 90:1304–8. doi: 10.1111/j.1651-2227.2001.tb01580.x
37. Varela-Silva MI, Azcorra H, Dickinson F, Bogin B, Frisancho AR. Influence of maternal stature, pregnancy age, and infant birth weight on growth during childhood in Yucatan, Mexico: a test of the intergenerational effects hypothesis. Am J Human Biol. (2009) 21:657–63. doi: 10.1002/ajhb.20883
38. Jahanihashemi H, Noroozi M, Zavoshy R, Afkhamrezaei A, Jalilolghadr S, Esmailzadehha N. Malnutrition and birth related determinants among children in Qazvin, Iran. Eur J Public Health. (2017) 27:559–62. doi: 10.1093/eurpub/ckx043
39. Hong R, Banta JE, Betancourt JA. Relationship between household wealth inequality and chronic childhood under-nutrition in Bangladesh. Int J Equity Health. (2006) 5:1–10. doi: 10.1186/1475-9276-5-15
40. Ramakrishnan U. Nutrition and low birth weight: from research to practice. Am J Clin Nutr. (2004) 79:17–21. doi: 10.1093/ajcn/79.1.17
41. Khan JR, Awan N, Sheikh MT. A multilevel and spatial analysis of the infant and young child feeding practices and associated factors among the under-2 aged children in Bangladesh. Child Care Pract. (2022) 28:178–95. doi: 10.1080/13575279.2019.1680528
42. Urke HB, Bull T, Mittelmark MB. Socioeconomic status and chronic child malnutrition: wealth and maternal education matter more in the Peruvian Andes than nationally. Nutr Res. (2011) 31:741–7. doi: 10.1016/j.nutres.2011.09.007
43. Ikeda N, Irie Y, Shibuya K. Determinants of reduced child stunting in Cambodia: analysis of pooled data from three demographic and health surveys. Bull World Health Organization. (2013) 91:341–9. doi: 10.2471/BLT.12.113381
Keywords: Bangladesh, children, severe malnutrition, determinants, undernutrition
Citation: Chowdhury MRK, Khan HTA, Rashid M, Mondal MNI, Bornee FA and Billah B (2022) Prevalence and correlates of severe under-5 child anthropometric failure measured by the composite index of severe anthropometric failure in Bangladesh. Front. Pediatr. 10:978568. doi: 10.3389/fped.2022.978568
Received: 26 June 2022; Accepted: 23 August 2022;
Published: 14 September 2022.
Edited by:
Judie Arulappan, Sultan Qaboos University, OmanReviewed by:
Prakash Doke, Bharati Vidyapeeth Deemed University, IndiaMarta Cristina Sanabria, National University of Asunción, Paraguay
Copyright © 2022 Chowdhury, Khan, Rashid, Mondal, Bornee and Billah. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Mamunur Rashid, Mamunur.Rashid@hig.se
†ORCID: Mamunur Rashid orcid.org/0000-0001-7558-4168