 Qiuxia Lin
Qiuxia Lin Menglu Wu
Menglu Wu Hanbing Yu
Hanbing Yu Xiaojiong Jia
Xiaojiong Jia Hua Zou
Hua Zou Deyu Ma
Deyu Ma Siqiang Niu
Siqiang Niu Shifeng Huang
Shifeng Huang- 1Department of Clinical Laboratory Medicine, The First Affiliated Hospital of Chongqing Medical University, Chongqing, China
- 2Department of Clinical Laboratory, Qingdao Women and Children’s Hospital, Qingdao, China
- 3Department of Clinical Laboratory Medicine, Chongqing Health Center for Women and Children, Chongqing, China
Aim: We aim to depict the clinicoepidemiological and molecular information of carbapenem-resistant Enterobacteriales (CRE) in Chongqing, China.
Methods: We performed a prospective, observational cohort study, recruiting inpatients diagnosed with CRE infections from June 1, 2018, to December 31, 2019. We carried out strain identification and molecular characterization of CRE. eBURST analysis was conducted to assess the relationships among the different isolates on the basis of their sequence types (STs) and associated epidemiological data using PHYLOViZ. Clinical parameters were compared between the carbapenemase-producing Enterobacteriales (CPE) and non-CPE group.
Findings: 128 unique CRE isolates from 128 patients were collected during the study period: 69 (53.9%) CPE and 59 (46.1%) non-CPE. The majority of CPE isolates were blaKPC-2 (56.5%), followed by blaNDM (39.1%) and blaIMP (5.8%). Klebsiella pneumoniae carbapenemase (KPC)–producing clonal group 11 Klebsiella pneumoniae (K. pneumoniae) was the most common CPE. Antibiotic resistance was more frequent in the CPE group than in the non-CPE group. Independent predictors for CPE infection were ICU admission and hepatobiliary system diseases. Although, there was no significant difference in desirability of outcome ranking (DOOR) outcomes between the two groups. At 30 days after index culture, 35 (27.3% ) of these patients had died.
Conclusion: CRE infections were related to high mortality and poor outcomes, regardless of CRE subgroups. CPE were associated with prolonged ICU stays and had different clinical and microbiological characteristics than non-CPE. The identification of CPE/non-CPE and CRE resistance mechanisms is essential for better guidance of the clinical administration of patients with CRE infections.
Introduction
Antimicrobial resistance (AMR) poses a serious threat to global health, economics, and medical practice, and the resistance to last-line antibiotics (i.e., carbapenems) is of most concern (World Bank Group (2017); WHO Antimicrobial resistance, 2014). Moreover, CRE belong to the top three multidrug-resistant (MDR) bacteria on the priority list of the WHO (Tacconelli et al., 2018). According to the definition of the United States Centers for Disease Control and Prevention (CDC), Enterobacteriales with resistance to a carbapenem are defined as CRE (CRE, 2015). Generally, CRE are divided into carbapenemase-producing Enterobacteriales (CPE) and non-CPE groups. In virtue of the quick spread of CPE in health-care settings and high mortality rates, CPE infections have attracted high clinical and public health attention (Haverkate et al., 2015).
Carbapenem resistance within Enterobacteriales derives from two main mechanisms: 1) acquisition of carbapenemase genes that encode enzymes capable of hydrolyzing carbapenems or 2) a decrease in the uptake of antibiotics by a qualitative or/and quantitative deficiency of porin expression in association with overexpression of β-lactamases that possess very weak affinity for carbapenems (Nordmann et al., 2012).Globally, the most important carbapenemases of carbapenem resistance within Enterobacteriales are classified into three categories: 1) class A serine enzymes, such as KPC-type enzymes; 2) class B metal enzymes, such as NDM, VIM, and IMP metallo-β-lactamases, and 3) class D serine enzymes, such as OXA-48–type enzymes (Nordmann et al., 2012). In some recent observational studies from Italy, Greece, Spain, and the United States, high mortality rates (40–60%) in patients with bacteremia caused by CPE were observed (Zarkotou et al., 2011; Qureshi et al., 2012; Tumbarello et al., 2012; Navarro-San Francisco et al., 2013; Daikos et al., 2014). In another observational study in 2013, the predominant species of CPE in the United States was K. pneumoniae (Satlin et al., 2017). Moreover, KPC is the most common carbapenemase in the United States (CDC, 2021). NDM-1 was widespread in India, Pakistan, and Bangladesh (Kumarasamy et al., 2010). OXA-48–like carbapenemases remain extremely rare in the United States; on the contrary, they are relatively commonly found in Europe, especially in Mediterranean countries (Poirel et al., 2012; Lyman et al., 2015). Carbapenemases have a worldwide distribution, but substantial variability in the distribution of carbapenemases exists on the continental, national, and regional levels. Most clinicoepidemiological information and its association with molecular characteristics have been reported for Western countries, including those in North America and/or Europe, and have focused on molecular types such as KPC or NDM. Awareness of the prevalence and incidence of the specific carbapenemases of CRE is essential for the prevention of their spread and selection of appropriate treatment options. To better assist the clinicians in administration of CRE infections, more detailed clinicoepidemiological information and its association with molecular characteristics are highly needed. In this prospective study, our research question was whether carbapenemase production in CRE is associated with adverse clinical outcomes, among CRE in China.
Materials and Methods
Study Settings and Participants
We performed a single-centre, prospective, observational cohort study at a tertiary-care, teaching hospital in Chongqing, China. Patients were eligible for inclusion if CRE was isolated in a clinical culture from any anatomical site during hospitalization. Institutional review board approval was obtained, and only the first qualifying culture episode during the first admission for each unique patient enrolled during the study period (June 1, 2018, to December 31, 2019) with CRE infection was included. There was no age exclusion. We excluded patients who had been involved in this study before and who refused treatment at the onset of infection. The study size was derived by inclusion of all eligible patients within the study period. Infections were defined by previously described standard criteria (Van Duin et al., 2014). A patient with a culture positive for CRE was deemed to have an infection if CRE was isolated from blood or any other sterile source. For patients with positive respiratory cultures, the criteria outlined by the American Thoracic Society and the Infectious Diseases Society of America were used (Pneumonia, 2005; Mandell et al., 2007). For patients with positive cultures from urine or surgical wounds, the CDC National Healthcare Safety Network criteria were applied (Horan et al., 2008). Patients with cultures from nonsurgical wounds were considered infected only if the treating physician documented infection in the medical record and evidence of systemic inflammation on the day the positive culture was documented; this was defined as an abnormal systemic white cell count (either > 10 × 103 or < 4 × 103 cells/μl) and/or an abnormal body temperature (either > 99.5°F or < 96°F). All of the other culture episodes were designated colonizations. According to CDC guidelines for clinical microbiology laboratories, CRE are defined as Enterobacteriales with resistance to any carbapenem (meropenem, imipenem, and/or ertapenem) and/or phenotypically carbapenemase producers (CRE, 2015). Follow-up time: from admission to discharge or death in hospital. Those discharged alive were followed up until 90 days after the first positive culture.
Clinical Data Collection
Clinical data, including demographics (age and sex), referral source (admission from another hospital, nursing home, long-term care facility, or home), isolation source of bacteria (e.g., blood and bronchial lavage fluid), severity of comorbid conditions (recorded by the Charlson comorbidity index (CCI) score (Charlson et al., 1987)), the Pitt bacteraemia score (Paterson et al., 2004) on the day of the first culture, exposure to antibiotic within 14 days before the first positive culture collection date of CRE, history of trauma and surgical procedures during 6 months before the CRE culture collection date, antibiotic usage of empirical therapy, antibiotic usage of definitive therapy, and outcomes, were collected from the patients’ electronic medical records system. Empirical therapy was defined as antibiotic usage before the antibiotic susceptibility report. Definitive therapy was antibiotics given after the antibiotic susceptibility report.
Microbiology
Standard identification and susceptibility testing of CRE were carried out and interpreted, according to the Clinical and Laboratory Standards Institute (CLSI) criteria of microbiology laboratories (Clinical Laboratory Standards Institute, 2018). Bacterial identification was conducted by using the VITEK MS or VITEK2 compact (BioMerieux, Hazelwood, MO, United States) automated system, and antimicrobial susceptibilities were determined in vitro using a VITEK 2 Compact AST-GN13 card (bioMérieux), which was used to test the antibiotic susceptibilities of all isolates to cefazolin (CFZ), ceftriaxone (CRO), ceftazidime (CAZ), cefepime (FEP), cefoxitin (FOX), aztreonam (ATM), ampicillin/sulbactam (SAM), piperacillin/tazobactam (TZP), ciprofloxacin (CIP), levofloxacin (LEV), minocycline (MH), and cefoperazone/sulbactam (CFPS). Four antibiotics, including imipenem (IMP), meropenem (MEM), ertapenem (ETP), and tigecycline (TGC), were tested by the broth microdilution method following the criteria of the CLSI (Clinical Laboratory Standards Institute, 2018). The minimal inhibitory concentrations (MICs) breakpoint for tigecycline was defined according to the European Committee on Antimicrobial Susceptibility Testing (EUCAST, 2021), while the others were interpreted according to CLSI protocols. Using the previously described primers (Tian et al., 2018), polymerase chain reaction (PCR) amplification of genomic DNA extracted from CRE isolates and subsequent PCR amplification product sequencing were performed to identify potential carbapenemase genes (i.e., blaKPC, blaNDM, blaIMP, blaVIM, and blaOXA-48) (Wang et al., 2018), extended spectrum-β-lactamases (ESBLs) genes (i.e., blaCTM, blaSHV, and blaTEM), and AmpC genes (i.e., blaACC, blaFOX, blaMOX, blaDHA, blaCIT, and blaEBC). Multilocus sequence typing (MLST) was conducted following the published protocol for K. pneumoniae (http://bigsdb.pasteur.fr/klebsiella/klebsiella.html). eBURST analysis was conducted to assess relationships between the different isolates on the basis of their sequence types (STs) and associated epidemiological data using PHYLOViZ.
Outcomes
After 30 days of the first positive culture, we evaluated the outcome. The primary outcome of this study was DOOR (Evans et al., 2015) analysis evaluating three harmful events (discharge failure, adverse events, and absence of clinical response, Supplementary Appendix). Death and being alive without harmful events were, respectively, defined as the worst and the best outcome. Between the two extremes, the three categories were alive with one, two, or three harmful events. There were five total categories of outcomes. The secondary outcomes of our study were in-hospital mortality, 30-day mortality, 90-day mortality, and 90-day readmission rates.
Statistical Analysis
Characteristics of patients with CPE infection were compared to those with non-CPE infection using Fisher’s exact tests or chi-square for categorical variables and Mann–Whitney U-tests for continuous variables as appropriate. Univariate analyses were performed for each variable. Variables with p value of ≤0.1 in the univariate analyses were included into the multivariate logistic regression model. All p values were two-sided, and p values ≤0.05 were considered statistically significant. All statistical analyses were conducted by IBM SPSS software version 25.0 (SPSS Inc., IL, United States).
Results
Summary of the Study Cohort
During the study period, a total of 128 isolates were collected from 128 patients (Supplementary Table S1). Carbapenemase genes were shown in 69 (53.9%) strains, referred to as CPE. On the other hand, 59 (46.1%) CRE resistant to at least one carbapenem, without any carbapenemase gene, were defined as non-CPE.
Bacterial Species and Isolation Sites
In Supplementary Table S1, bacterial species of CRE are summarized. CRE isolates included 69 (53.9%) K. pneumoniae, 24 (18.8%) Enterobacter spp., 20 (15.6%) Escherichia coli (E. coli), 7 (5.5%) Klebsiella aerogenes (K. aerogenes), 5 (3.9%) Citrobacter freundii (C. freundii), 2 (1.6%) Klebsiella oxytoca (K. oxytoca), and 1 (0.8%) Enterobacter kobei (E. kobei). For CPE isolates, the predominant genus and species were K. pneumoniae (60.7%), Enterobacter spp. (20.3%), and E. coli (11.6%); there were two (2.9%) C. freundii and one (1.4%) isolate of K. aerogenes, K. oxytoca, and E. kobei. For non-CPE, the genus and species distribution was largely similar but slightly reverse: K. pneumoniae (45.8%), E. coli (20.3%), Enterobacter spp. (16.9%), K. aerogenes (10.2%), C. freundii (5.1%), and K. oxytoca (1.7%).
In Supplementary Table S2, isolation sites of CRE are summarized. CPE were most commonly isolated from sputum (n = 27, 39.1%), followed by urine (n = 16, 23.2%), blood (n = 11, 15.9%), drainage (n = 6, 8.7%), wound secretion (n = 4, 5.8%), bile (n = 2, 2.9%), and others (n = 1, 1.4%). Non-CPE were most commonly isolated from urine (n = 18, 30.5%), followed by sputum (n = 13, 22.0%), drainage (n = 8, 13.6%), wound secretion (n = 7, 11.9%), blood (n = 5, 8.5%), and catheter (n = 4, 6.8%), bile (n = 3, 5.1%), intra-abdominal samples (n = 2, 2.9%), and others (n = 1, 1.7%).
Antimicrobial Susceptibility Profiles
Among non-β-lactam antibiotics, levofloxacin had significantly higher susceptibility rates in non-CPE [18 (30.5%)] than in CPE [8 (11.6%)], p = 0.008 in Supplementary Table S3. Similarly, among β-lactams, imipenem [non-CPE/CPE: 27(45.8%)/2(2.9%)], meropenem [30(50.9%)/3(4.3%)], piperacillin/tazobactam [10(16.9%)/0], cefepime [7(11.9%)/0], and cefoperazone/sulbactam [7(11.9%)/0] had significantly higher susceptibility rates in non-CPE than in CPE. Overall, CPE had higher resistant rates in those agents.
Prevalence of Carbapenemase, ESBLs, and AmpC Among CRE
Detected carbapenemase genes included blaKPC-2 (39 [56.5%] of 69), blaNDM-1 (19 [27.5%]), blaNDM-5 (8 [11.6%]), and blaIMP-4(4 [5.8%]); ESBL genes shown in CPE included blaCTX-M (13 [18.8%] of 69) and blaSHV (3 [4.3%]). Non-CPE showed similar blaCTX-M (14 [23.7%] of 59) and blaSHV (3 [5.1%] of 59) distribution characteristics. There are no differences in AmpC expression between CPE (5 [7.2%] of 69) and non-CPE (3 [5.1%] of 59). Notably, a K. aerogenes isolate simultaneously coproduced blaNDM-1, blaKPC-2, and blaCTX-M (Table 1). 42 (60.9%) of the 69 carbapenem-resistant K. pneumoniae isolates were CPE, compared with 14 (58.3%) of 24 for Enterobacter spp. and 8 (40.0%) of 20 for E. coli. Among 69 CR-KP isolates, blaKPC-2 was the most commonly identified carbapenemase-encoding gene; it was present in 37 CR-KP isolates. BlaIMP-4 was shown in 3 CR-KP isolates and blaNDM-5 in 2 CR-KP isolates. Among 14 carbapenemase-producing Enterobacter spp. isolates, all carbapenemase-encoding genes were blaNDM-1. However, various metallo-β-lactamase genes were identified in 8 carbapenemase-producing E. coli, including blaNDM-1 (1 of 8), blaNDM-5 (6 of 8), and blaIMP-4 (1 of 8) (Supplementary Table S4).
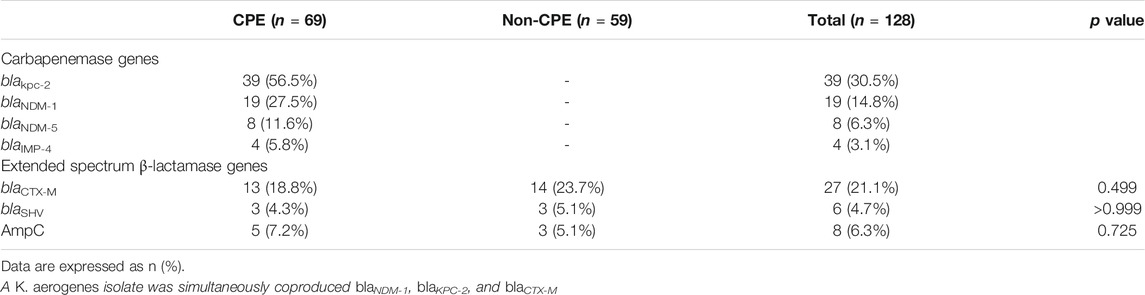
TABLE 1. Prevalence of carbapenemase, ESBL, and AmpC among CRE.
MLST of K. pneumoniae Isolates
In total, 69 K. pneumoniae isolates were subjected to MLST. We have identified 16 K. pneumoniae STs. The most common ST of K. pneumoniae was ST11 (43/69, 62.3%). The most frequent carbapenemase type and ST in K. pneumoniae was ST11-KPC-2 K. pneumoniae(33/69, 47.8%), followed by ST15-KPC-2 K. pneumoniae and ST307-IMP-4 K. pneumoniae (two of each type). eBURST diagrams based on the STs obtained for K. pneumoniae are shown by carbapenemase(Figure 1). 48 isolates belonged to clonal complex 11, including ST11, ST15, ST709, and ST5029. Three isolates belonged to clonal complex 307, including ST307. Three isolates belonged to clonal complex 147, including ST147 and ST273. Nine STs were uniquely represented by one isolate. In addition, the ST of remaining 6 K. pneumoniae isolates was not identified (Table 2).
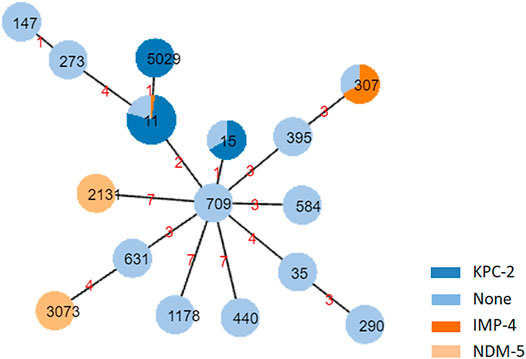
FIGURE 1. eBURST diagrams of Klebsiella pneumoniae isolates showing the relationship among isolates on the basis of their multilocus sequence typing and carbapenemase. Each node within the tree represents a single ST. The size of the nodes is proportional to the number of isolates represented by the said node. Within each node, the area of dark blue, dark orange, light orange, and light blue represents the number of KPC-2, IMP-4, NDM-5 and no carbapenemase. Nodes are labeled with corresponding ST. ST, sequence type. Links are labeled with absolute distance.
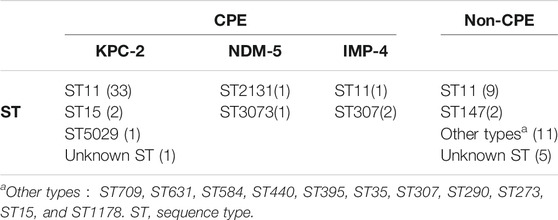
TABLE 2. The MLST analysis of 69 CR-KP.
Comparison of Clinical Characteristics and Outcomes of CPE and Non-CPE
Table 3 showed the results of the univariate analysis of the comparison between patients with CPE infections and those with non-CPE infections. For the univariate analyses, there were no significant differences in demographic information and most preexisting medical conditions between the two groups. 50 (39.1%) of the 128 patients showed a history of intensive care unit (ICU) admission. As compared with patients with non-CPE infections (16 [27.1%] of 59), patients with CPE infections (34 [49.3%] of 69) were more likely to be with the history of ICU admission. Moreover, patients with CPE infections tended to have longer ICU stay and hepatobiliary system disease than patients with non-CPE infections. Among the patients with CRE infections, patients with CPE infections represented a greater likelihood of having respiratory tract infections (27 [39.1%] of 69; p = 0.038) and lower likelihood of having catheter-related infections (0 of 69; p = 0.028) rather than patients with non-CPE infections (respiratory 13 [22.0%] of 59; catheter-related 4 [6.8%] of 59; for overall distribution, p = 0.042). Multivariate analysis for matched data showed that admission to ICU (OR, 5.55; 95% CI, 2.25–13.74; p < 0.001) and hepatobiliary system disease (OR, 2.91; 95% CI, 1.27–6.66; p = 0.011) were independent predictors for CPE isolation of patients with infection (Table 4).
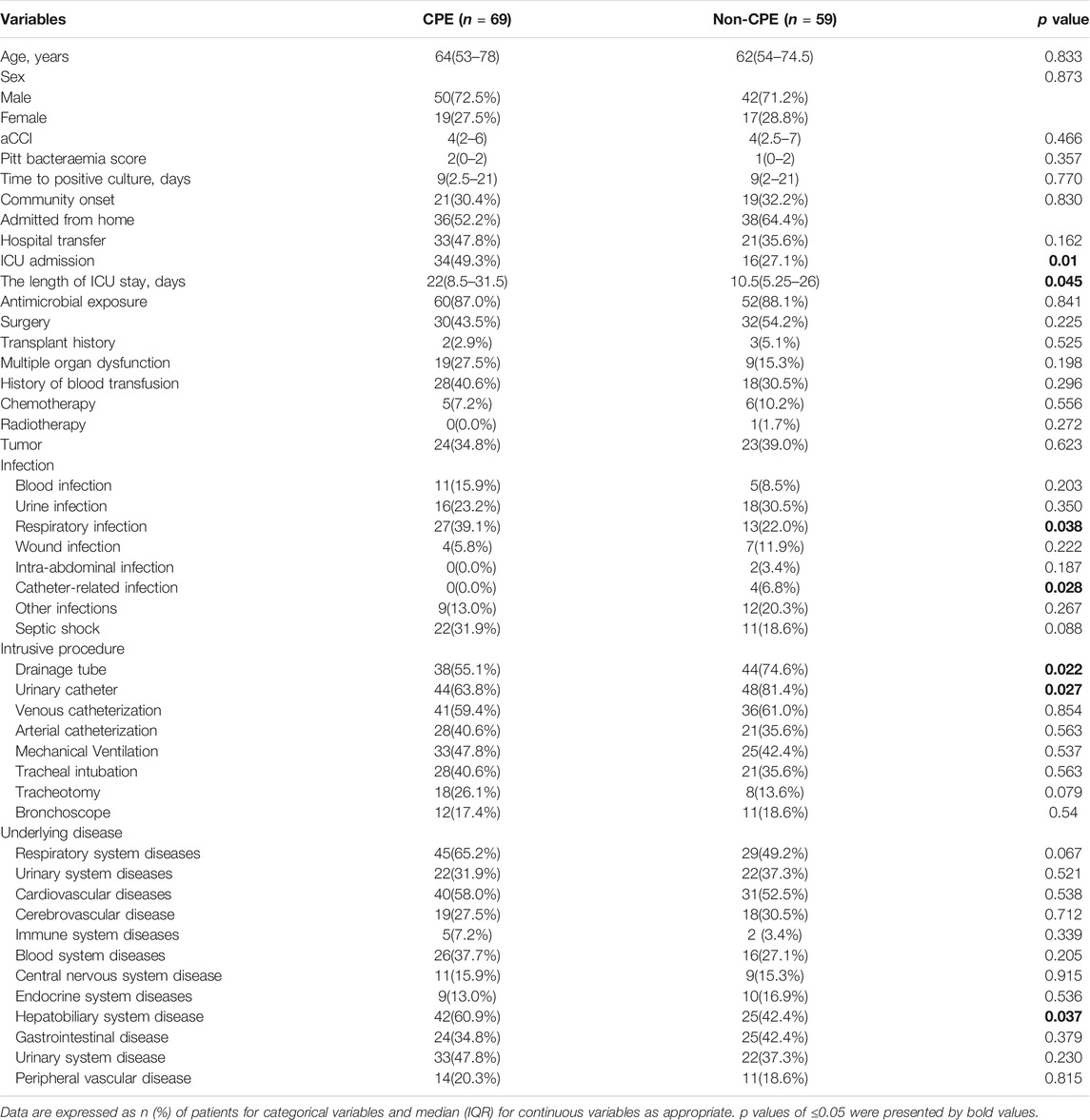
TABLE 3. Baseline characteristics of patients with CRE infection.
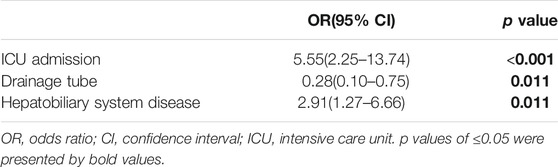
TABLE 4. Logistic regression analysis of predictors factors for CPE.
Antibiotic treatment history is displayed in Supplementary Table S5. 61 (47.5%) of 128 patients received empirical therapy with a carbapenem, while 57 (44.5%) of the 128 patients received definitive therapy with a carbapenem. In empirical therapy, 18 patients received monotherapy with a carbapenem. Also, in definitive therapy, 8 patients received monotherapy with a carbapenem. There were no significant differences between two groups in most agents of empiric and directed antibiotic regimens. Patients with CPE infection received more cefoperazone-sulbactam (29.0% vs. 11.9%, p = 0.018), less aminoglycoside (29.0% vs. 45.8%, p = 0.050), and more tigecycline (36.2% vs. 18.6%, p = 0.027) than patients with non-CPE infection in definitive therapy.
According to DOOR outcomes shown in Table 5, 37 (28.9%) patients with CRE infections were alive without events, 31 (24.2%) with one event, 19 (14.8%) with two events, 6 (4.7%) with three events, and 35 (27.3%) were dead. Between patients with CPE infections and with non-CPE infections groups, there was no significant difference of DOOR outcomes. In patients with CRE infections, 30-day mortality and 90-day mortality were, respectively, 27.3% (35 of 128) and 32.8% (42 of 128). Between the CPE and non-CPE groups, 30-day mortality and 90-day mortality rates were similar 25 (19.5%) were readmitted within 90 days. There were no significant differences between the two groups.
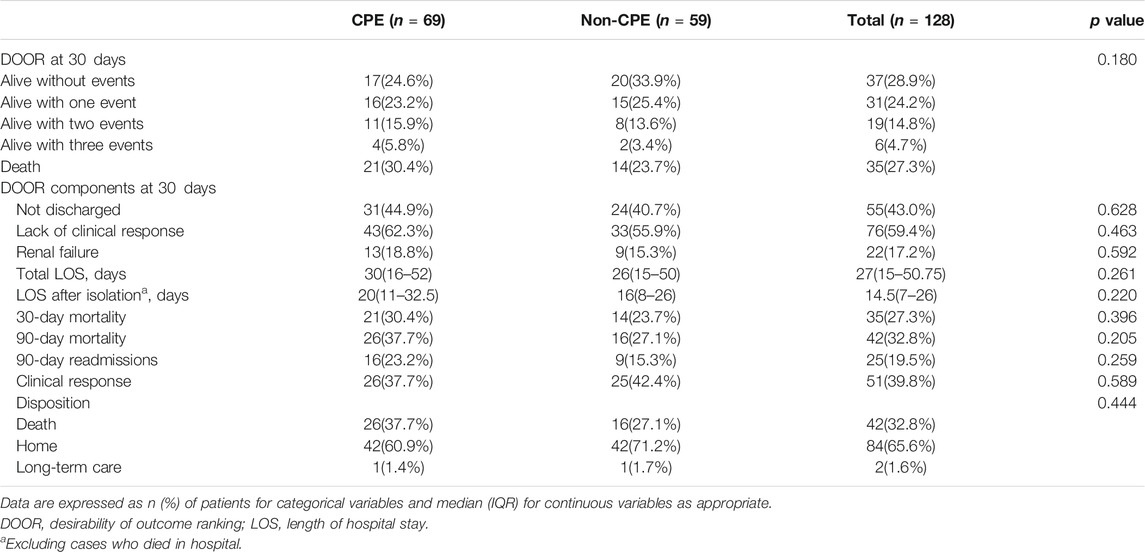
TABLE 5. Outcomes in patients with CRE infections.
Discussion
We aim to depict the clinicoepidemiological and molecular information of CRE in China. In this study, CRE were divided into two clinically and molecularly distinct groups (CPE and non-CPE groups). While CPE are Enterobacteriales that are resistant to carbapenem and express carbapenemase, non-CPE are CRE without any carbapenemase genes. In general, CPE are considered to be of the most epidemiological significance due to their ability to spread rapidly throughout health-care settings and their association with adverse outcomes. Nevertheless, in our cohort, 46.1% of the isolates did not carry carbapenemase genes. Resources dedicated to stopping the spread of CPE isolates might, therefore, be assigned to non-CPE of lesser public health concern. Therefore, correct identification of CPE is essential for the management of CRE infections. This study provided important information including the molecular microbiological characteristics of CPE and non-CPE groups, as well as clinical epidemiology and the differences between the two groups and predictors for CPE isolation and outcomes.
Among 128 CRE isolates, CR-KP was the most dominant species (53.9%), followed by Enterobacter spp. (18.8%) and E. coli (15.6%). blaKPC-2 was the most commonly identified carbapenemase-encoding gene. Among 69 CR-KP, most isolates belonged to clonal complex 11, including ST11, ST15, ST709, and ST5029. ST11 was the most common ST type of CR-KP in our study, consistent with a multicenter study in China (Wang et al., 2018). In another study, the dominant ST of CR-KP was, and still is, ST258, which has become prevalent in many places around the world since it was first discovered in the United States (Kitchel et al., 2009; Munoz-Price et al., 2013). The most frequent carbapenemase type and ST in CR-KP was ST11-KPC-2 K. pneumoniae. Due to multidrug resistance, and high transmission, ST11-KPC-2 K. pneumoniae poses a substantial threat to human health. There were two novel clone groups, ST307 and ST147. ST307 was endemic in Colombia, the United States (Texas), Italy, and South Africa, while ST147 was endemic in India, Greece, Italy, and certain North African countries (Peirano et al., 2020). Due to their ability to cause serious infections, worldwide distribution, and association with AMR, including panresistance, ST307 and ST147 have the ability to become major threats to public health (Peirano et al., 2020), calling for public concern.
Asian countries are the hotbed of NDM producers. This study demonstrated that carrying blaNDM genes was the primary mechanism of carbapenem resistance in Enterobacter spp. and E. coli in southwestern China. Most carbapenemase-producing E. coli isolates harbored blaNDM-5 with high-level carbapenem resistances. All carbapenemase-producing Enterobacter spp. strains carried blaNDM-1 and showed simultaneous resistance to ertapenem, imipenem, and meropenem.
ICU admission and hepatobiliary system disease were identified as independent predictors of CPE infections rather than non-CPE infections. Patients with hepatobiliary system disease might be invaded more frequently by CPE than the non-CPE group. Patients with ICU admission associated with rapidly fatal diseases were at higher risk of acquiring CPE.
In this study, we found that CPE isolates were more resistant to levofloxacin, cefepime, piperacillin/tazobactam, cefoperazone/sulbactam, imipenem, and meropenem than non-CPE isolates. Concerning empiric therapy of patients with CRE infections, there was no significant difference between patients in the CPE group and those in the non-CPE group. About half of the patients with CRE received a carbapenem as a part of the treatment regimen. Generally, clinicians had preferred carbapenem for patients with severe infections. Among definitive therapy of patients with CRE infections, patients with CPE infections received more treament with cefoperazone-sulbactam and/or tigecycline than patients with non-CPE infections. However, CPE isolates were more resistant to cefoperazone-sulbactam than non-CPE isolates. With a tag of CRE infection, patients might receive more advanced but toxic drugs. Therefore, correct identification of CPE or non-CPE is essential for clinical drug selection.
In our study, clinical outcomes were not significantly different between groups with CPE or non-CPE infections. As most CPE isolates were ST11 K. pneumonia with blaKPC-2 genes, this comparison is principally between ST11-KPC-2 K. pneumonia and a more genetically diverse group of various Enterobacteriales. There are some explanations for this finding. First, regardless of the potential carbapenem resistance mechanisms of CRE, CDC standards might identify patients with infections that are associated with poor outcomes. Second, patients attached a label to CRE might receive overtreatment with more toxic drugs that might narrow the difference between the two groups (van Duin et al., 2020). Third, more effective treatment for CPE infections might have weakened the difference in clinical outcomes compared with that of the patients with non-CPE infections. In an observational study, patients with CPE bacteremia demonstrated a more than four times 14-day mortality rate when compared with non-CP-CRE bacteremic patients (aOR 4.92; 95% CI 1.01–24.81) (Tamma et al., 2017). Their study only included cases of CRE bacteraemia. In our study, not only bacteremia but also infections of the respiratory, urinary, catheter, wound, and intra-abdominal sites were included. Patients with CPE infections have a longer ICU stay than the non-CPE group. The reason for the longer ICU stay in the CPE group was unknown. However, this was an important finding suggesting that the identification of a CPE-affected patient indicated outcomes to a greater extent than the identification of a non-CPE patient in our cohort of CRE infection.
There are several limitations in this study. First, due to the small numbers of K. aerogenes, C. freundii, K. oxytoca, E.kobe, E. coli, and E.cloacae, we only performed an MLST of the most abundant K. pneumoniae isolates. Second, our data and isolates were collected from a single centre, where the distribution of carbapenemase genes may differ from the distribution of those in the rest of the world. Third, in any observational study, the analysis of antibiotic treatment regimens was under the influence of confounding biases. Nevertheless, no significant difference of the primary outcome DOOR was observed between the two groups. In China, the most common CPE is ST11-KPC-2 K. pneumoniae.
In conclusion, CRE infections were highly associated with poor outcomes, regardless of the CRE subgroup. Patients with CPE infections were associated with prolonged ICU stays and showed different clinical and microbiological characteristics as compared with those with non-CPE infections. Both CPE/non-CPE identification and CRE resistance mechanism determination are essential for better guidance of the clinical administration of patients with CRE infections, especially in those with the history of ICU admission and hepatobiliary system disease.
Data Availability Statement
The original contributions presented in the study are included in the article/Supplementary Material; further inquiries can be directed to the corresponding authors.
Ethics
The data and isolates analyzed in the study were obtained in accordance with the standards and approved by the Chongqing Medical University Institutional Review Board and Biomedical Ethics Committee (Ethical review batch number: 2020-644). For this study, isolates were collected at the microbiology laboratory of our hospital, with no contact with the patients. There was no patient identification performed during data collection. Therefore, the ethics committee determined that informed consent was not required
Author Contributions
SN and SH designed the study; QL, MW, HZ, DM, XJ, and HY performed the experiments and analyzed data; QL, SN, and SH wrote this article. All authors read and approved the final article.
Funding
This work was sponsored by Natural Science Foundation of Chognqing, China (Grant No. cstc2020jcyj-msxmX0519), the Science and Technology Research Program of the Chongqing Municipal Education Commission (Grant Nos. KJ1500235 and KJ1702022), and the Medical Research Program of the Chongqing Health and Family Planning Commission (Nos. 2018MSXM009 and 2016MSXM001)
Publisher’s Note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors, and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Supplementary Material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fphar.2021.716324/full#supplementary-material
References
CDC (2021). Prevention, C. For D.C. and Tracking CRE in the United States. Available online: wwww.cdc.gov/hai/organisms/cre/trackingcre.html (accessed on Apr 3, 2021).
Charlson, M., Pompei, P., Ales, K. L., and Mackenzie, C. (1987). A New Method of Classifying Prognostic Comorbidity in Longitudinal Studies: Development and Validation. J Chronic Dis40: 373-383. J. Chronic Dis. 40, 373–383. doi:10.1016/0021-9681(87)90171-8
Clinical Laboratory Standards Institute (2018). Clinical Laboratory Standards Institute Methods for Dilution Antimicrobial Susceptibility Tests for Bacteria that Grow Aerobically ; Approved Standard — Ninth Edition. CLSI Document M07-A9. Wayne, PA: CLSI.
CRE (2015). Centers for Diasease Control and Prevention Facility Guidance for Control of Carbapenem-Resistant Enterobacteriaceae (CRE) November 2015 Update - CRE Toolkit. Atlanta: CDC.
Daikos, G. L., Tsaousi, S., Tzouvelekis, L. S., Anyfantis, I., Psichogiou, M., Argyropoulou, A., et al. (2014). Carbapenemase-producing Klebsiella pneumoniae Bloodstream Infections: Lowering Mortality by Antibiotic Combination Schemes and the Role of Carbapenems. Antimicrob. Agents Chemother. 58, 2322–2328. doi:10.1128/AAC.02166-13
Evans, S. R., Rubin, D., Follmann, D., Pennello, G., Huskins, W. C., Powers, J. H., et al. (2015). Desirability of Outcome Ranking (DOOR) and Response Adjusted for Duration of Antibiotic Risk (RADAR). Clin. Infect. Dis. 61, 800–806. doi:10.1093/cid/civ495
Haverkate, M. R., Bootsma, M. C. J., Weiner, S., Blom, D., Lin, M. Y., Lolans, K., et al. (2015). Modeling Spread of KPC-Producing Bacteria in Long-Term Acute Care Hospitals in the Chicago Region, USA. Infect. Control. Hosp. Epidemiol. 36, 1148–1154. doi:10.1017/ice.2015.163
Horan, T. C., Andrus, M., and Dudeck, M. A. (2008). CDC/NHSN Surveillance Definition of Health Care-Associated Infection and Criteria for Specific Types of Infections in the Acute Care Setting. Am. J. Infect. Control. 36, 309–332. doi:10.1016/j.ajic.2008.03.002
Kitchel, B., Rasheed, J. K., Patel, J. B., Srinivasan, A., Navon-Venezia, S., Carmeli, Y., et al. (2009). Molecular Epidemiology of KPC-Producing Klebsiella pneumoniae Isolates in the United States: Clonal Expansion of Multilocus Sequence Type 258. Antimicrob. Agents Chemother. 53, 3365–3370. doi:10.1128/AAC.00126-09
Kumarasamy, K. K., Toleman, M. A., Walsh, T. R., Bagaria, J., Butt, F., Balakrishnan, R., et al. (2010). Emergence of a New Antibiotic Resistance Mechanism in India, Pakistan, and the UK: A Molecular, Biological, and Epidemiological Study. Lancet Infect. Dis doi:10.1016/S1473-3099(10)70143-2
Lyman, M., Walters, M., Lonsway, D., Rasheed, K., Limbago, B., and Kallen, A. (2015). Notes from the Field: Carbapenem-Resistant Enterobacteriaceae Producing OXA-48-like Carbapenemases - United States, 2010-2015. MMWR Morb. Mortal. Wkly. Rep. 64, 1315–1316. doi:10.15585/mmwr.mm6447a3
Mandell, L. A., Wunderink, R. G., Anzueto, A., Bartlett, J. G., Campbell, G. D., Dean, N. C., et al. (2007). Infectious Diseases Society of America/American Thoracic Society Consensus Guidelines on the Management of Community-Acquired Pneumonia in Adults. Clin. Infect. Dis. 44 Suppl 2, S27–S72. doi:10.1086/511159
Munoz-Price, L. S., Poirel, L., Bonomo, R. A., Schwaber, M. J., Daikos, G. L., Cormican, M., et al. (2013). Clinical Epidemiology of the Global Expansion of Klebsiella pneumoniae Carbapenemases. Lancet Infect. Dis. 13, 785–96. doi:10.1016/s1473-3099(13)70190-7
Navarro-San Francisco, C., Mora-Rillo, M., Romero-Gómez, M. P., Moreno-Ramos, F., Rico-Nieto, A., Ruiz-Carrascoso, G., et al. (2013). Bacteraemia Due to OXA-48-Carbapenemase-Producing Enterobacteriaceae: A Major Clinical challenge. Clin. Microbiol. Infect. 19, E72–E79. doi:10.1111/1469-0691.12091
Nordmann, P., Dortet, L., and Poirel, L. (2012). Carbapenem Resistance in Enterobacteriaceae: Here Is the Storm!. Trends Mol. Med. 18, 263–72. doi:10.1016/j.molmed.2012.03.003
Paterson, D. L., Ko, W. C., Von Gottberg, A., Mohapatra, S., Casellas, J. M., Goossens, H., et al. (2004). International Prospective Study of Klebsiella pneumoniae Bacteremia: Implications of Extended-Spectrum β-Lactamase Production in Nosocomial Infections. Ann. Intern. Med. 140, 26. doi:10.7326/0003-4819-140-1-200401060-00008
Peirano, G., Chen, L., Kreiswirth, B. N., and Pitout, J. D. D. (2020). Emerging Antimicrobial-Resistant High-Risk klebsiella Pneumoniae Clones ST307 and ST147. Antimicrob. Agents Chemother. 64, 64. doi:10.1128/AAC.01148-20
Pneumonia, H. (2005). Guidelines for the Management of Adults with Hospital-Acquired, Ventilator-Associated, and Healthcare-Associated Pneumonia. Am. J. Respir. Crit. Care Med. 171, 388–416. doi:10.1164/rccm.200405-644ST
Poirel, L., Potron, A., and Nordmann, P. (2012). OXA-48-like Carbapenemases: The Phantom Menace. J. Antimicrob. Chemother. 67, 1597–1606. doi:10.1093/jac/dks121
Qureshi, Z. A., Paterson, D. L., Potoski, B. A., Kilayko, M. C., Sandovsky, G., Sordillo, E., et al. (2012). Treatment Outcome of Bacteremia Due to KPC-Producing Klebsiella pneumoniae: Superiority of Combination Antimicrobial Regimens. Antimicrob. Agents Chemother. 56, 2108–2113. doi:10.1128/AAC.06268-11
Satlin, M. J., Chen, L., Patel, G., Gomez-Simmonds, A., Weston, G., Kim, A. C., et al. (2017). Multicenter Clinical and Molecular Epidemiological Analysis of Bacteremia Due to Carbapenem-Resistant Enterobacteriaceae (CRE) in the CRE Epicenter of the United States. Antimicrob. Agents Chemother. 61, e02349–16. doi:10.1128/AAC.02349-16
Tacconelli, E., Carrara, E., Savoldi, A., Harbarth, S., Mendelson, M., Monnet, D. L., et al. (2018). Discovery, Research, and Development of New Antibiotics: the WHO Priority List of Antibiotic-Resistant Bacteria and Tuberculosis. Lancet Infect. Dis. 18, 318–327. doi:10.1016/S1473-3099(17)30753-3
Tamma, P. D., Goodman, K. E., Harris, A. D., Tekle, T., Roberts, A., Taiwo, A., et al. (2017). Comparing the Outcomes of Patients with Carbapenemase-Producing and Non-carbapenemase-producing Carbapenem-Resistant Enterobacteriaceae Bacteremia. Clin. Infect. Dis. 64, 257–264. doi:10.1093/cid/ciw741
Tian, X., Sun, S., Jia, X., Zou, H., Li, S., and Zhang, L. (2018). Epidemiology of and Risk Factors for Infection with Extended-Spectrum β-lactamase-producing Carbapenem-Resistant Enterobacteriaceae: Results of a Double Case–Control Study. Idr 11, 1339–1346. doi:10.2147/IDR.S173456
Tumbarello, M., Viale, P., Viscoli, C., Trecarichi, E. M., Tumietto, F., Marchese, A., et al. (2012). Predictors of Mortality in Bloodstream Infections Caused by Klebsiella pneumoniae Carbapenemase-Producing K. pneumoniae: Importance of Combination Therapy. Clin. Infect. Dis. 55, 943–950. doi:10.1093/cid/cis588
Van Duin, D., Perez, F., Rudin, S. D., Cober, E., Hanrahan, J., Ziegler, J., et al. (2014). Surveillance of Carbapenem-Resistant Klebsiella pneumoniae: Tracking Molecular Epidemiology and Outcomes through a Regional Network. Antimicrob. Agents Chemother. 58, 4035–4041. doi:10.1128/AAC.02636-14
van Duin, D., Arias, C. A., Komarow, L., Chen, L., Hanson, B. M., Weston, G., et al. (2020). Molecular and Clinical Epidemiology of Carbapenem-Resistant Enterobacterales in the USA (CRACKLE-2): a Prospective Cohort Study. Lancet Infect. Dis. 20, 731–741. doi:10.1016/S1473-3099(19)30755-8
Wang, Q., Wang, X., Wang, J., Ouyang, P., Jin, C., Wang, R., et al. (2018). Phenotypic and Genotypic Characterization of Carbapenem-resistantEnterobacteriaceae: Data from a Longitudinal Large-Scale CRE Study in China (2012-2016). Clin. Infect. Dis. 67, S196–S205. doi:10.1093/cid/ciy660
WHO Antimicrobial resistance, (2014). Global Report on Surveillance. World Heal. Organ doi:10.1007/s13312-014-0374-3
World Bank Group (2017). Drug-resistant Infections: A Threat to Our Economic Future. Washington DC: World Bank.
Zarkotou, O., Pournaras, S., Tselioti, P., Dragoumanos, V., Pitiriga, V., Ranellou, K., et al. (2011). Predictors of Mortality in Patients with Bloodstream Infections Caused by KPC-Producing Klebsiella pneumoniae and Impact of Appropriate Antimicrobial Treatment. Clin. Microbiol. Infect. 17, 1798–1803. doi:10.1111/j.1469-0691.2011.03514.x
Keywords: mortality, carbapenemase-producing Klebsiella pneumoniae, carbapenemase-producing Enterobacteriales, multilocus sequence typing, molecular epidemiology
Citation: Lin Q, Wu M, Yu H, Jia X, Zou H, Ma D, Niu S and Huang S (2021) Clinical and Microbiological Characterization of Carbapenem-Resistant Enterobacteriales: A Prospective Cohort Study. Front. Pharmacol. 12:716324. doi: 10.3389/fphar.2021.716324
Received: 28 May 2021; Accepted: 24 August 2021;
Published: 08 October 2021.
Edited by:
Elisabetta Poluzzi, University of Bologna, ItalyReviewed by:
Milo Gatti, University of Bologna, ItalyFarzad Badmasti, Pasteur Institute of Iran, Iran
Copyright © 2021 Lin, Wu, Yu, Jia, Zou, Ma, Niu and Huang. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Siqiang Niu, siqiangniu@cqmu.edu.cn; Shifeng Huang, sfhuang@hospital.cqmu.edu.cn
†These authors have contributed equally to this work and share first authorship