 ChuanNan Zhai1,2Rui Li3Kai Hou1,2JingYi Chen1Mohammad Alzogool1YueCheng Hu2JingXia Zhang2YingYi Zhang2Le Wang2Rui Zhang2
ChuanNan Zhai1,2Rui Li3Kai Hou1,2JingYi Chen1Mohammad Alzogool1YueCheng Hu2JingXia Zhang2YingYi Zhang2Le Wang2Rui Zhang2 HongLiang Cong1,2*
HongLiang Cong1,2*- 1School of Medicine, NanKai University, Tianjin, China
- 2Department of Cardiology, Tianjin Chest Hospital, Tianjin, China
- 3Tianjin GongAn Hospital, Tianjin, China
Background: Recent studies have shown that blood-based miRNAs are dysregulated in patients with acute myocardial infarction (AMI) and are therefore a potential tool for the diagnosis of AMI. Therefore, this study summarized and evaluated studies focused on microRNAs as novel biomarkers for the diagnosis of AMI from the last ten years.
Methods: MEDLINE, the Cochrane Central database, and EMBASE were searched between January 2010 and December 2019. Studies that assessed the diagnostic accuracy of circulating microRNAs in AMI were chosen. The pooled sensitivity, specificity, positive likelihood ratio, negative likelihood ratio, diagnostic odds ratio, and area under the curve (AUC) were used to assess the test performance of miRNAs.
Results: A total of 58 studies that included 8,206 participants assessed the diagnostic accuracy of circulating miRNAs in AMI. The main results of the meta-analyses are as follows: (1) Total miRNAs: the overall pooled sensitivity and specificity were 0.82 (95% CI: 0.79–0.85) and 0.87 (95% CI: 0.84–0.90), respectively. The AUC value was 0.91 (95% CI: 0.88–0.93) in the overall summary receiver operator characteristic (SROC) curve. (2) The panel of two miRNAs: sensitivity: 0.88 (95% CI: 0.77–0.94), specificity: 0.84 (95% CI: 0.72–0.91), AUC: 0.92 (95% CI: 0.90–0.94). (3) The panel of three miRNAs: sensitivity: 0.91 (95% CI: 0.85–0.94), specificity: 0.87 (95% CI: 0.77–0.92), AUC: 0.92 (95% CI: 0.89–0.94). (4) Results by types of miRNAs: miRNA-1: sensitivity: 0.78 (95% CI: 0.71–0.84), specificity: 0.86 (95% CI: 0.77–0.91), AUC: 0.88 (95% CI: 0.85–0.90); miRNA-133a: sensitivity: 0.85 (95% CI: 0.69–0.94), specificity: 0.92 (95% CI: 0.61–0.99), AUC: 0.93 (95% CI: 0.91–0.95); miRNA-208b: sensitivity: 0.80 (95% CI: 0.69–0.88), specificity: 0.96 (95% CI: 0.77–0.99), AUC: 0.91 (95% CI: 0.88–0.93); miRNA-499: sensitivity: 0.85 (95% CI: 0.77–0.91), specificity: 0.95 (95% CI: 0.89–0.98), AUC: 0.96 (95% CI: 0.94–0.97).
Conclusion: miRNAs may be used as potential biomarkers for the detection of AMI. For single, stand-alone miRNAs, miRNA-499 may have better diagnostic accuracy compared to other miRNAs. We propose that a panel of multiple miRNAs with high sensitivity and specificity should be tested.
Introduction
Although advanced clinical medications have recently been developed for the diagnosis and prevention of coronary heart disease (CAD), acute myocardial infarction (AMI), which includes ST-elevation myocardial infarction (STEMI) and non-STEMI (NSTEMI), is still considered a primary public health threat, with high morbidity and mortality worldwide (Moss et al., 1996; GBD 2013 Mortality and Causes of Death Collaborators, 2015). Acute-phase reaction during ischemic damage is a crucial pathogenesis of ischemia myocardial issue (Hoffmeister et al., 2003). Dependent on accurate recognition and diagnosis, early effective revascularization treatment is an important strategy to repair ischemic myocardium and can significantly reduce the mortality of AMI patients (Hung et al., 2013). Currently, the most widely used biomarkers of myocardial injury during clinical practice are cardiac troponin and creatine kinase-MB (CK-MB), which may provide effective benefits for patients with revascularization therapy (Dohi et al., 2015; Anand et al., 2019). However, the elevation of cardiac troponin may be involved in serious, non-cardiac disease such as neuromuscular disorders, severe sepsis, and chronic renal insufficiency (Lamb et al., 2006; Finsterer et al., 2007; Vallabhajosyula et al., 2017). High levels of cardiac troponin have also been detected in patients with heart failure (Myhre et al., 2018). Therefore, early diagnostic biomarkers and improvement of the accuracy of approaches for the early prediction of AMI are still warranted.
Potential novel genetic and molecular biomarkers are currently being explored (Lorenzano et al., 2019). MicroRNAs (miRNAs/miRs) are endogenous, non-coding RNAs ~19–25nt that play crucial post-regulatory roles in animals and plants by targeting mRNAs for translational or cleavage repression (Bartel, 2004). MiRNAs can inhibit or reduce target gene expression, subsequently affecting protein expression (Saxena et al., 2018). Thus, miRNAs play important regulatory roles in cell growth, development, and differentiation (Gabisonia et al., 2019). Further, miRNAs have been identified in extracellular fluid and can be extremely stable despite the presence of endogenous RNase (Chevillet et al., 2014). In recent years, a number of studies have reported that miRNAs are dysregulated in CAD, and that specific circulating miRNA signatures might be useful as biomarkers for the diagnosis of AMI and as therapeutic targets (Jakob et al., 2017). However, the results of previous studies were significantly different, potentially due to sample size, specimen types, and different detection technologies. Therefore, the purpose of this systematic review and meta-analysis was to summarize the diagnostic values of blood-based miRNA levels from published articles from the last 10 years and to appraise the accuracy of results to determine whether miRNAs may be used as novel biomarkers for the diagnosis of AMI.
Materials and Methods
This study was conducted according to the Preferred Reporting Items for Systematic Reviews and Meta-analysis guidelines (Hutton et al., 2015; Moher et al., 2015). Two reviewers (CN Zhai, R Li) were independently involved with study selection, data extraction, and quality assessment.
Study Selection
An electronic search of MEDLINE (including PubMed), the Cochrane Central database, and EMBASE was performed to identify relevant articles published between January 2010 and December 2019. The following medical subject heading terms were used: (“plasma” OR “serum” OR “circulating”) AND (“microRNA” OR “miRNAs” OR “miR*”) AND (“myocardial infarction” OR “AMI” OR “coronary heart disease” OR “coronary artery disease” OR “coronary syndrome” OR “ischemic heart disease”). No language restrictions were imposed. All relevant review articles were retrieved, and duplicates were removed by manually searching. Based on the title and abstract, manuscripts of interest were obtained for full-text review. Only full-text references were included.
Inclusion and Exclusion Criteria
Inclusion and exclusion criteria were developed by the investigative team. The inclusion criteria were: (1) human studies, (2) studies related to circulating miRNAs levels and AMI, and (3) studies that contained enough data to evaluate the diagnostic value of miRNAs in AMI. Exclusion criteria were based on the following: (1) studies evaluating tissue miRNA or miRNA in other body fluids; (2) case reports, conference abstracts, and reviews; and (3) non-human studies.
Data Extraction, Meta-Analysis, and Quality Assessment
Each manuscript was assessed independently by two researchers (CN Zhai and K Hou). Disagreements among reviewers were resolved by consensus. Data extracted included the following: authors, publication year, country, type of blood-based fluid (serum or plasma), characteristics of the study population (both case and control), study design (qRT-PCR detection method), whether miRNA screening was performed, number of miRNAs assessed, listing of the specific dysregulated miRNAs in AMI patients compared with controls, and outcome of statistical analyses including details of miRNA analysis, such as type of reference miRNA utilized. Studies reporting on single miRNA were included in the meta-analysis and were evaluated according to the Quality Assessment of Diagnostic Accuracy Studies 2 (QUADAS-2) checklist (Whiting et al., 2011), which is designed to assess the risk of bias and the applicability of studies of diagnostic accuracy. The following four key domains were included: patient selection, the index test, the reference standard, and flow and timing. Each was assessed with respect to the risk of bias, and the first three domains were assessed with respect to applicability.
Statistical Analysis
Analysis was based on the accuracy of the identified miRNAs for diagnosing the presence of AMI, as determined using Receiver Operator Characteristic (ROC) curves via the Area Under the Curve (AUC) value, and sensitivity and specificity where available (Carter et al., 2016). We calculated the pooled sensitivity, specificity, positive likelihood ratio (PLR), negative likelihood ratio (NLR), and diagnostic odds ratio (DOR), generated the bivariate summary receiver operator characteristic (SROC) curve, and calculated the area under the curve (AUC) to assess the overall diagnostic accuracy of miRNAs in distinguishing AMI patients from controls. Forest plots were constructed using STATA (15.0 StataCorp LP, College, Station, TX, USA). Due to the presumed heterogeneity of studies, a random-effects model (DerSimonian–Laird method) was used (Mahid et al., 2006). The heterogeneity of included studies was assessed using I2, and the P-value was considered significant if I2 was >50% or P < 0.05. Subgroup analyses were performed to explore the potential source of heterogeneity as follows: (1) based on the type of blood sample (plasma or serum), (2) the method of qRT-PCR detection (SYBR Green or TaqMan), (3) the type of reference control used for normalization (RNU or Cel-miRNA), (4) sample size (Sample size ≥ 100 or Sample size <100), and (5) different populations (Caucasian or East Asian). To assess the publication bias of the included studies, we performed Deeks' test of funnel plot asymmetry (Deeks et al., 2005).
Results
Literature Search Results and Characteristics of the Included Studies
The PRISMA flow diagram of the literature search and inclusion of relevant studies are shown in Figure 1. Overall, 79 full-text articles were deemed relevant for a more detailed evaluation. Of these articles, 21 were excluded for the following reasons: review article (n = 4), not about AMI (n = 14), and not a diagnostic study (n = 3). Finally, 58 studies investigating plasma, serum, or peripheral venous blood miRNAs in the diagnosis of AMI were identified as eligible for inclusion in this systematic review (Adachi et al., 2010; Ai et al., 2010; Cheng et al., 2010; Corsten et al., 2010; D'Alessandra et al., 2010; Wang et al., 2010, 2011, 2013, 2014, 2016, 2019; Gidlöf et al., 2011, 2013; Meder et al., 2011; Zile et al., 2011; Devaux et al., 2012, 2015; Long et al., 2012a,b; Li C. et al., 2013; Li Y. Q. et al., 2013; Lu et al., 2013; Olivieri et al., 2013; He et al., 2014; Hsu et al., 2014; Huang et al., 2014; Li L. M. et al., 2014; Li Z. et al., 2014; Peng et al., 2014; Xiao et al., 2014; Białek et al., 2015; Chen et al., 2015; Gao et al., 2015; Han et al., 2015; Ji et al., 2015; Li et al., 2015; Liu et al., 2015, 2018; Yao et al., 2015; Zhang L. et al., 2015; Zhang R. et al., 2015; Zhao et al., 2015; Ke-Gang et al., 2016; Shalaby et al., 2016; Yang et al., 2016, 2017; Zhang et al., 2016, 2018; Zhu et al., 2016; Guo et al., 2017; Agiannitopoulos et al., 2018; Fawzy et al., 2018; Yi and An, 2018; Bukauskas et al., 2019; Li H. et al., 2019; Li P. et al., 2019; Xue et al., 2019a,b). These studies were performed in 12 countries; most of the subjects involved were East Asian, with Caucasian as the second most common population investigated. The major clinical characteristics of the included studies are shown in Table 1. In total, 8,206 patients were included in the study: 4,526 AMI patients and 3,680 healthy/non-AMI subjects (1,975 health controls, 1,705 non-AMI patients). Ten studies were relevant to the evaluation of patients with STEMI, three studies only included NSTEMI patients, and the other 45 articles included both types of myocardial infarction. The population demographics of our study are shown in Table 1. In total, 2,692 men and 1,834 women were included among AMI groups, and 2,066 men and 1,614 women were included in the control groups.
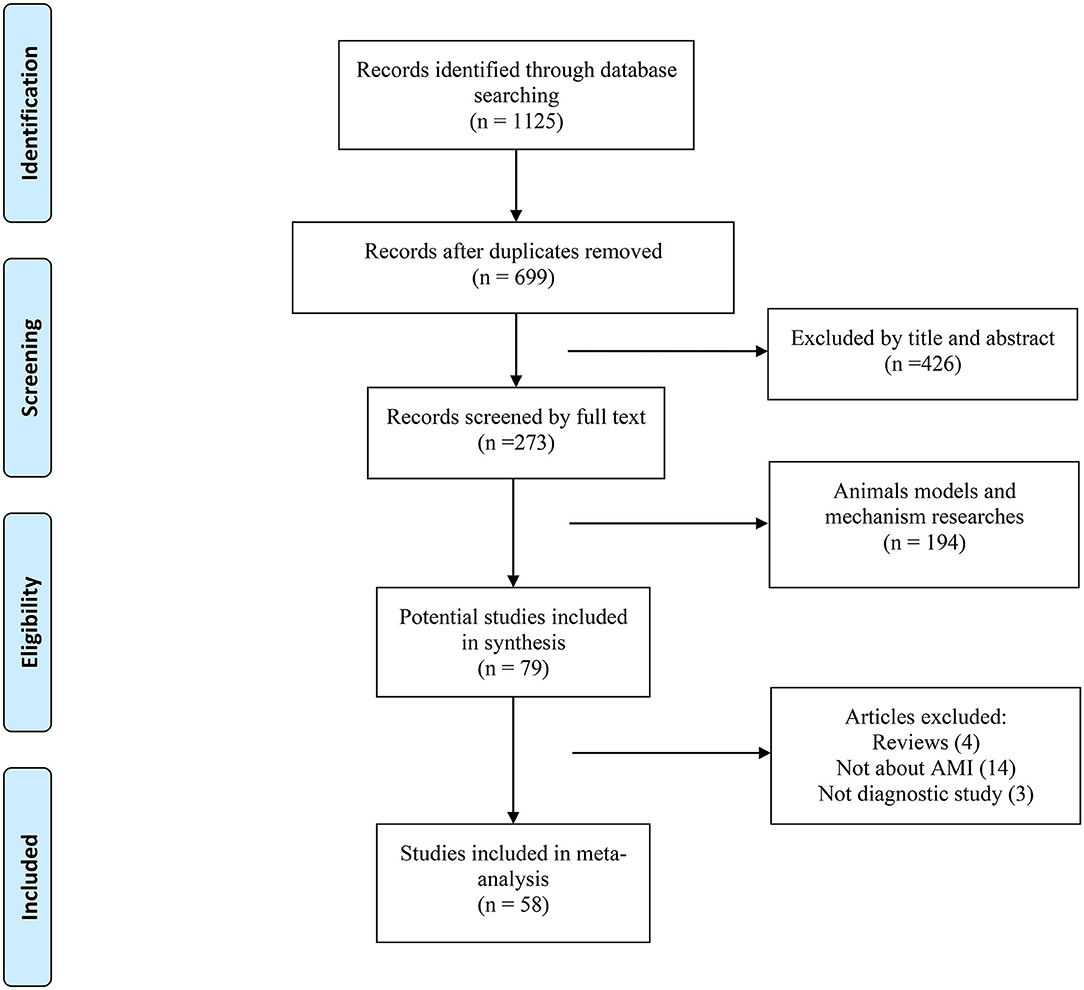
Figure 1. Flow diagram of the literature search process and study inclusion.
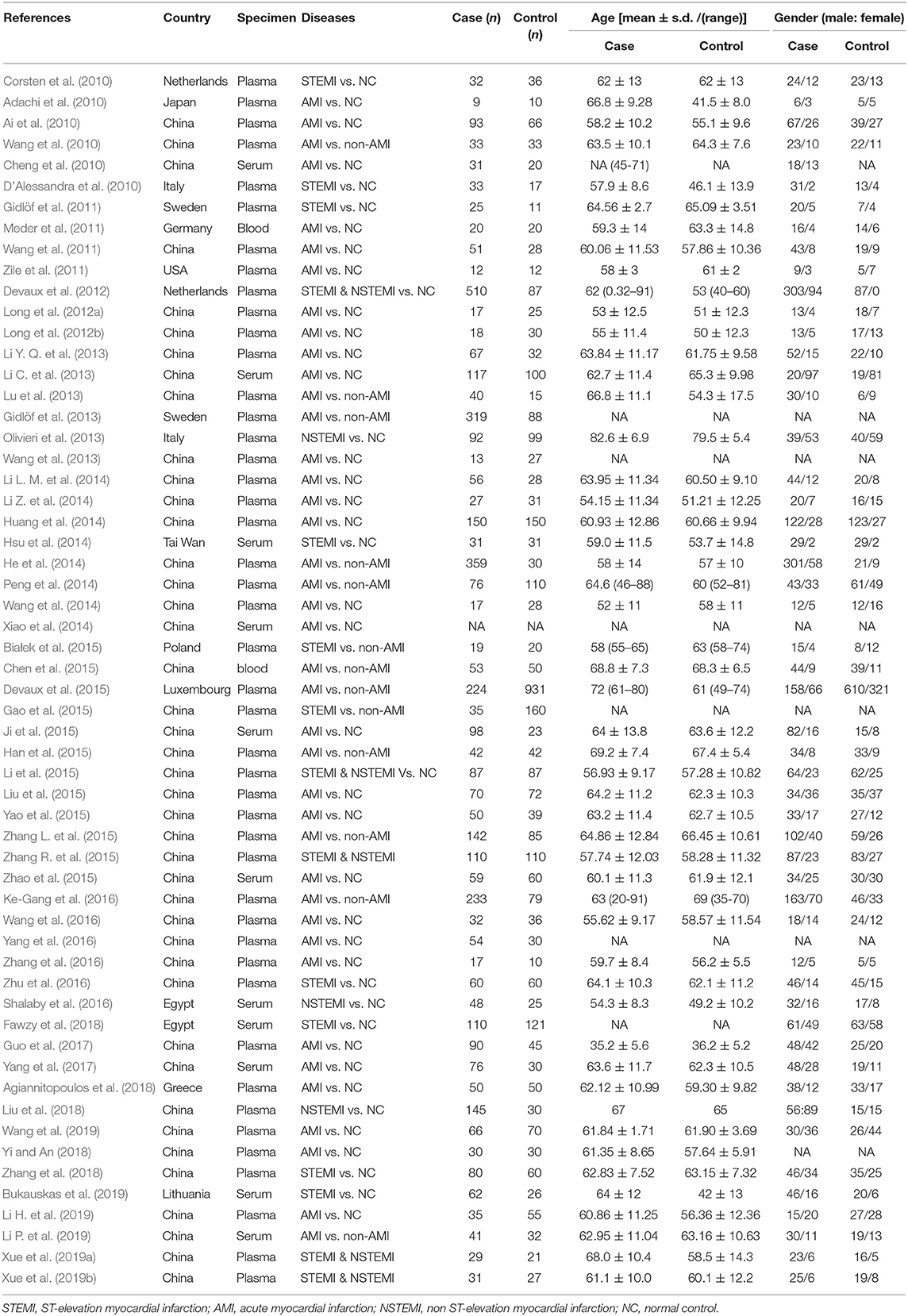
Table 1. Characteristics of studies included in the systematic review.
Identification of Dysregulated miRNAs in the Included Studies
All included studies used Quantitative reverse transcription polymerase chain reaction (qRT-PCR) to detect the expression levels of miRNAs. A summary of all study methods is provided in Table 2. Seven studies performed miRNA screening to compare blood-based miRNAs between AMI patients and control groups (Adachi et al., 2010; D'Alessandra et al., 2010; Meder et al., 2011; Li C. et al., 2013; Hsu et al., 2014; Huang et al., 2014; Li et al., 2015). Fifty-one articles identified miRNAs based on their own previous studies or based on the literature (Ai et al., 2010; Cheng et al., 2010; Corsten et al., 2010; Wang et al., 2010, 2011, 2013, 2014, 2016, 2019; Gidlöf et al., 2011, 2013; Zile et al., 2011; Devaux et al., 2012, 2015; Long et al., 2012a,b; Li Y. Q. et al., 2013; Lu et al., 2013; Olivieri et al., 2013; He et al., 2014; Li L. M. et al., 2014; Li Z. et al., 2014; Peng et al., 2014; Xiao et al., 2014; Białek et al., 2015; Chen et al., 2015; Gao et al., 2015; Han et al., 2015; Ji et al., 2015; Liu et al., 2015, 2018; Yao et al., 2015; Zhang L. et al., 2015; Zhang R. et al., 2015; Ke-Gang et al., 2016; Shalaby et al., 2016; Yang et al., 2016, 2017; Zhang et al., 2016, 2018; Zhu et al., 2016; Guo et al., 2017; Agiannitopoulos et al., 2018; Fawzy et al., 2018; Yi and An, 2018; Bukauskas et al., 2019; Li H. et al., 2019; Li P. et al., 2019; Xue et al., 2019a,b). The expression of 50 miRNAs were identified as either significantly higher or lower expression in AMI cases; specific details were shown in Table 3. Thirty-three miRNAs were upregulated (miRNA-1, miRNA-17-5p, miRNA-19b-3p, miRNA-21, miRNA-23b, miRNA-26a-1, miRNA-30a, miRNA-122-5p, miRNA-124, miRNA-126, miRNA-133a/b, miRNA-134, miRNA-145-3p, miRNA-146a, miRNA-150, miRNA-181a, miRNA-186, miRNA-195, miRNA-199a-1, miRNA-208a/b, miRNA-210, miRNA-223, miRNA-302b, miRNA-328, miRNA-361-5p, miRNA-423-5p, miRNA-486, miRNA-494, miRNA-497, miRNA-499, miRNA-663b, miRNA-1291, and miRNA-1303) (Adachi et al., 2010; Ai et al., 2010; Cheng et al., 2010; Corsten et al., 2010; D'Alessandra et al., 2010; Wang et al., 2010, 2011, 2013, 2014, 2016, 2019; Gidlöf et al., 2011, 2013; Meder et al., 2011; Zile et al., 2011; Devaux et al., 2012, 2015; Long et al., 2012a,b; Li C. et al., 2013; Li Y. Q. et al., 2013; Olivieri et al., 2013; He et al., 2014; Hsu et al., 2014; Li L. M. et al., 2014; Li Z. et al., 2014; Xiao et al., 2014; Białek et al., 2015; Chen et al., 2015; Han et al., 2015; Ji et al., 2015; Li et al., 2015; Liu et al., 2015, 2018; Yao et al., 2015; Zhang L. et al., 2015; Zhang R. et al., 2015; Ke-Gang et al., 2016; Shalaby et al., 2016; Zhang et al., 2016, 2018; Guo et al., 2017; Yang et al., 2017; Agiannitopoulos et al., 2018; Fawzy et al., 2018; Li P. et al., 2019; Xue et al., 2019a,b), and 17 miRNAs were downregulated (miRNA-22-5p, miRNA-23a-3p, miRNA-26a, miRNA-30d-5p, miRNA-99a, miRNA-125b, miRNA-126-3p, miRNA-132-5p, miRNA-145, miRNA-146a-5p, miRNA-191, miRNA-214, miRNA-320b, miRNA-375, miRNA-379, miRNA-519-5p, and miRNA-let-7d) (D'Alessandra et al., 2010; Meder et al., 2011; Long et al., 2012b; Lu et al., 2013; Hsu et al., 2014; Huang et al., 2014; Wang et al., 2014, 2019; Gao et al., 2015; Li et al., 2015; Yang et al., 2016; Yi and An, 2018; Bukauskas et al., 2019; Li H. et al., 2019). Thirteen upregulated miRNAs (miRNA-1, miRNA-19b-3p, miRNA-21, miRNA-122-5p, miRNA-126, miRNA-133a/b, miRNA-134, miRNA-150, miRNA-186, miRNA-208a/b, miRNA-486, miRNA-499, and miRNA-663b) (Adachi et al., 2010; Corsten et al., 2010; D'Alessandra et al., 2010; Wang et al., 2010, 2011, 2013, 2016, 2019; Gidlöf et al., 2011, 2013; Devaux et al., 2012, 2015; Li Y. Q. et al., 2013; Olivieri et al., 2013; He et al., 2014; Hsu et al., 2014; Peng et al., 2014; Xiao et al., 2014; Białek et al., 2015; Chen et al., 2015; Han et al., 2015; Ji et al., 2015; Li et al., 2015; Liu et al., 2015, 2018; Zhang L. et al., 2015; Zhang R. et al., 2015; Ke-Gang et al., 2016; Shalaby et al., 2016; Agiannitopoulos et al., 2018; Fawzy et al., 2018; Li H. et al., 2019; Li P. et al., 2019) and three downregulated miRNAs (miRNA-26a, miRNA-191, and miRNA-375) (D'Alessandra et al., 2010; Hsu et al., 2014; Li et al., 2015; Wang et al., 2019) were identified by more than one study. Among these articles, which included 22 original studies, miRNA-499 was the most frequently identified dysregulated miRNA in AMI patients (Adachi et al., 2010; Corsten et al., 2010; D'Alessandra et al., 2010; Wang et al., 2010; Gidlöf et al., 2011, 2013; Devaux et al., 2012, 2015; Li C. et al., 2013; Li Y. Q. et al., 2013; Olivieri et al., 2013; Xiao et al., 2014; Chen et al., 2015; Liu et al., 2015, 2018; Zhang L. et al., 2015; Zhang R. et al., 2015; Shalaby et al., 2016; Agiannitopoulos et al., 2018; Fawzy et al., 2018; Li P. et al., 2019). 16 studies focused on the miRNA-208 family (miRNA-208a/b) (Corsten et al., 2010; Wang et al., 2010; Gidlöf et al., 2011, 2013; Devaux et al., 2012, 2015; Li C. et al., 2013; Li Y. Q. et al., 2013; Xiao et al., 2014; Białek et al., 2015; Han et al., 2015; Li et al., 2015; Liu et al., 2015, 2018; Agiannitopoulos et al., 2018; Li P. et al., 2019), 14 studies focused on miRNA-1 (Ai et al., 2010; Cheng et al., 2010; Corsten et al., 2010; D'Alessandra et al., 2010; Wang et al., 2010; Gidlöf et al., 2011, 2013; Long et al., 2012a; Li C. et al., 2013; Li Y. Q. et al., 2013; Olivieri et al., 2013; Li L. M. et al., 2014; Liu et al., 2015, 2018), and 14 studies focused on the miRNA-133 family (miRNA-133a/b) (Corsten et al., 2010; D'Alessandra et al., 2010; Wang et al., 2010, 2011, 2013; Gidlöf et al., 2011; Li Y. Q. et al., 2013; Olivieri et al., 2013; Peng et al., 2014; Ji et al., 2015; Ke-Gang et al., 2016; Liu et al., 2018). Additionally, four studies identified a panel of two miRNAs (Hsu et al., 2014; Zhang R. et al., 2015; Shalaby et al., 2016; Wang et al., 2019), six studies identified a panel of three miRNAs (Long et al., 2012b; Wang et al., 2014, 2016; Li H. et al., 2019; Xue et al., 2019a,b), and one study identified a panel of more than four miRNAs that were elevated in AMI (Li C. et al., 2013).
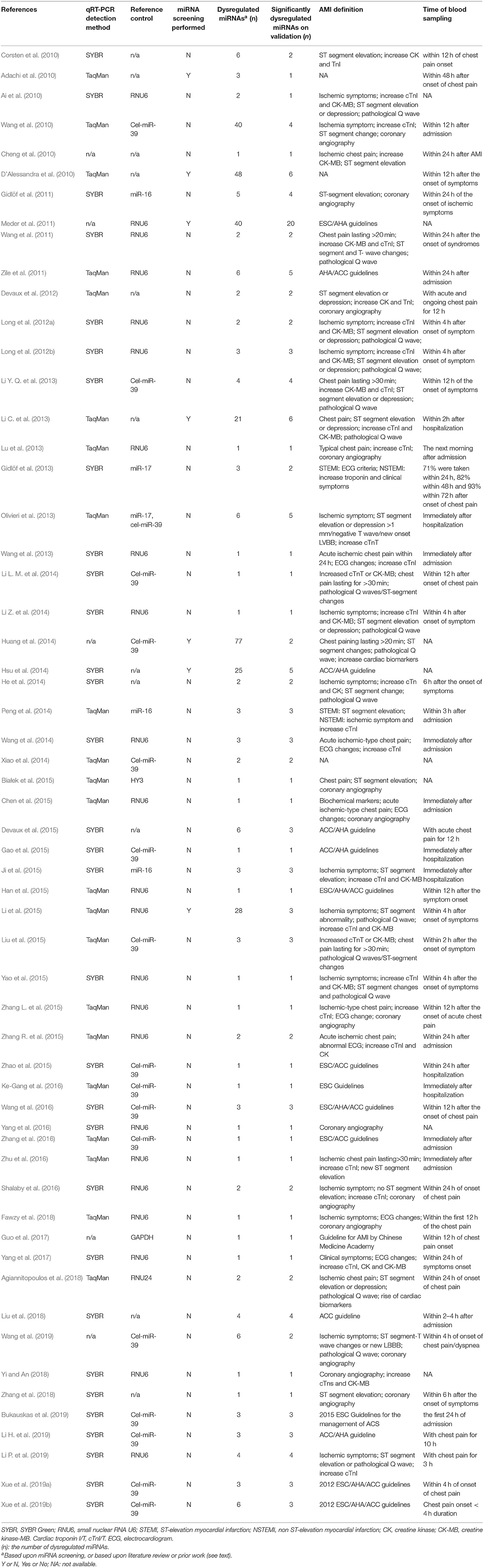
Table 2. Study methods and corresponding dysregulated miRNAs identified.
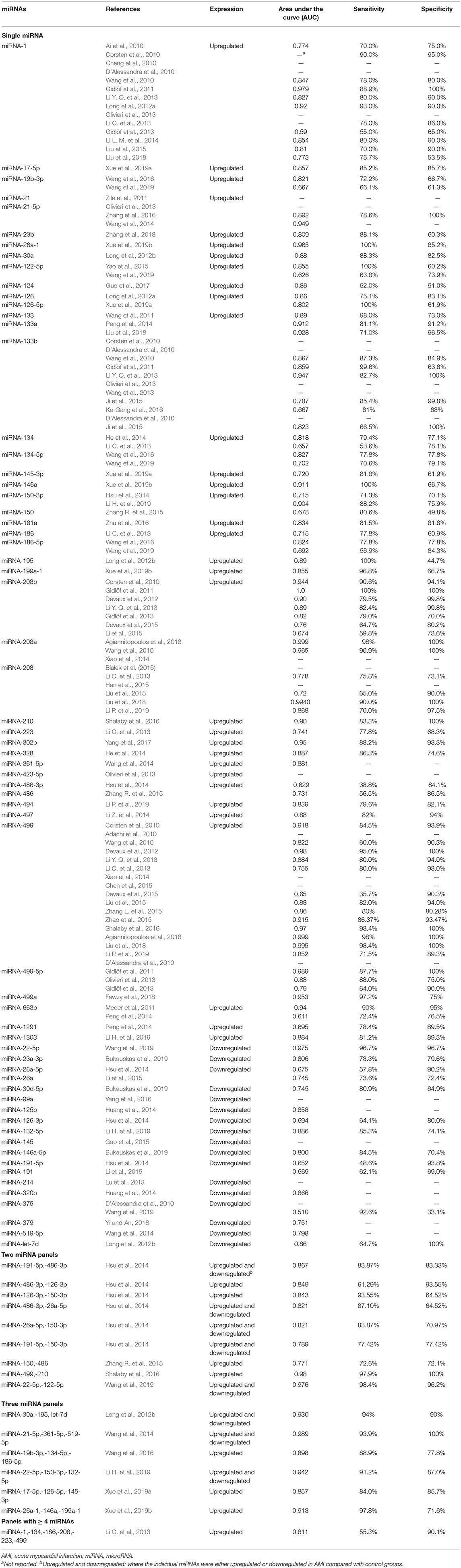
Table 3. Significantly dysregulated miRNAs of patients with AMI as compared with controls.
Sensitivity, Specificity, and Area Under the Curve
Among the included studies, the most common methods of assessing the diagnostic accuracy of dysregulated miRNAs were AUC and sensitivity and specificity, as determined from ROC curves. In the identified dysregulated miRNAs, AUC values ranged from 0.510 to 1.0, sensitivity ranged from 48.6% to 100%, and specificity from 33.1% to 100%. In the single identified miRNAs, the highest AUC sensitivity and specificity combination was reported for miRNA-208b (AUC 1.0, sensitivity 100%, specificity 100%) (Gidlöf et al., 2011). In the panel of two miRNAs, the highest value combination was reposted for miRNA-499 and miRNA-210 (AUC 0.98, sensitivity 97.9%, specificity 100%) (Shalaby et al., 2016). In the panel of three miRNAs, the highest value combination was reported for miRNA-21-5p, miRNA-361-5p, and miRNA-519-5p (AUC 0.989, sensitivity 93.9%, specificity 100%) (Wang et al., 2014). In the panel of ≥ 4 miRNAs, there was one study about AUC 0.811, which had sensitivity 55.3% and specificity 90.1% (Li C. et al., 2013).
Meta-Analysis Outcomes of Diagnostic Accuracy of miRNAs in AMI
The Quality Assessment of Included Studies
The pooled result of the meta-analysis for the diagnostic accuracy of blood-based miRNAs in AMI was pooled from 42 studies (Ai et al., 2010; Corsten et al., 2010; Wang et al., 2010, 2011, 2014, 2016, 2019; Gidlöf et al., 2011, 2013; Meder et al., 2011; Devaux et al., 2012, 2015; Long et al., 2012a,b; Li C. et al., 2013; Li Y. Q. et al., 2013; Olivieri et al., 2013; He et al., 2014; Hsu et al., 2014; Li L. M. et al., 2014; Li Z. et al., 2014; Peng et al., 2014; Ji et al., 2015; Li et al., 2015; Liu et al., 2015, 2018; Yao et al., 2015; Zhang L. et al., 2015; Zhang R. et al., 2015; Ke-Gang et al., 2016; Shalaby et al., 2016; Yang et al., 2016; Zhang et al., 2016, 2018; Zhu et al., 2016; Guo et al., 2017; Agiannitopoulos et al., 2018; Fawzy et al., 2018; Bukauskas et al., 2019; Li H. et al., 2019; Li P. et al., 2019; Xue et al., 2019a,b). Quality assessment results of the studies reporting on miRNAs included in the meta-analysis using the QUADAS-2 evaluation tool are shown in Supplementary Figure 1. Results are presented as percentages across the studies (Figure 2).
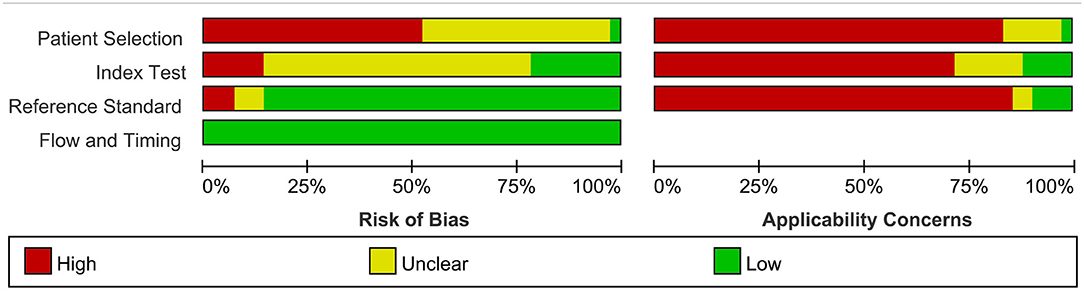
Figure 2. Bar graphs of the methodological quality assessment. Each risk-of-bias and applicability item is presented as percentages across included studies, which indicates the proportion of different levels for each item.
Total miRNAs
Dysregulated miRNAs in AMI patients compared with controls, the SROC curve with AUC, sensitivity, specificity, PLR, NLR, and DOR for miRNAs were included in our meta-analysis (Table 4). A random effect model was used for the meta-analysis due to significant heterogeneity (all I2 > 50%). Forty-four individual miRNAs were identified in 43 studies (Ai et al., 2010; Corsten et al., 2010; Wang et al., 2010, 2011, 2014, 2016, 2019; Gidlöf et al., 2011, 2013; Meder et al., 2011; Devaux et al., 2012, 2015; Long et al., 2012a,b; Li C. et al., 2013; Li Y. Q. et al., 2013; Olivieri et al., 2013; He et al., 2014; Hsu et al., 2014; Li L. M. et al., 2014; Li Z. et al., 2014; Peng et al., 2014; Ji et al., 2015; Li et al., 2015; Liu et al., 2015, 2018; Yao et al., 2015; Zhang L. et al., 2015; Zhang R. et al., 2015; Ke-Gang et al., 2016; Shalaby et al., 2016; Yang et al., 2016; Zhang et al., 2016, 2018; Zhu et al., 2016; Guo et al., 2017; Agiannitopoulos et al., 2018; Fawzy et al., 2018; Bukauskas et al., 2019; Li H. et al., 2019; Li P. et al., 2019; Xue et al., 2019a,b). The sensitivity, specificity, and the corresponding SROC value with 95% CIs (95% confidential intervals) of the total miRNAs in the diagnostic of AMI were 0.82 (95% CI: 0.79–0.85), 0.87 (95 %CI: 0.84–0.90), and 0.91 (95% CI: 0.88–0.93), respectively (Supplementary Figures 2A,B, 3A). The Deeks' funnel plot asymmetry test suggested a potential for publication bias in the total miRNAs (p-value = 0.00, Supplementary Figure 3B).
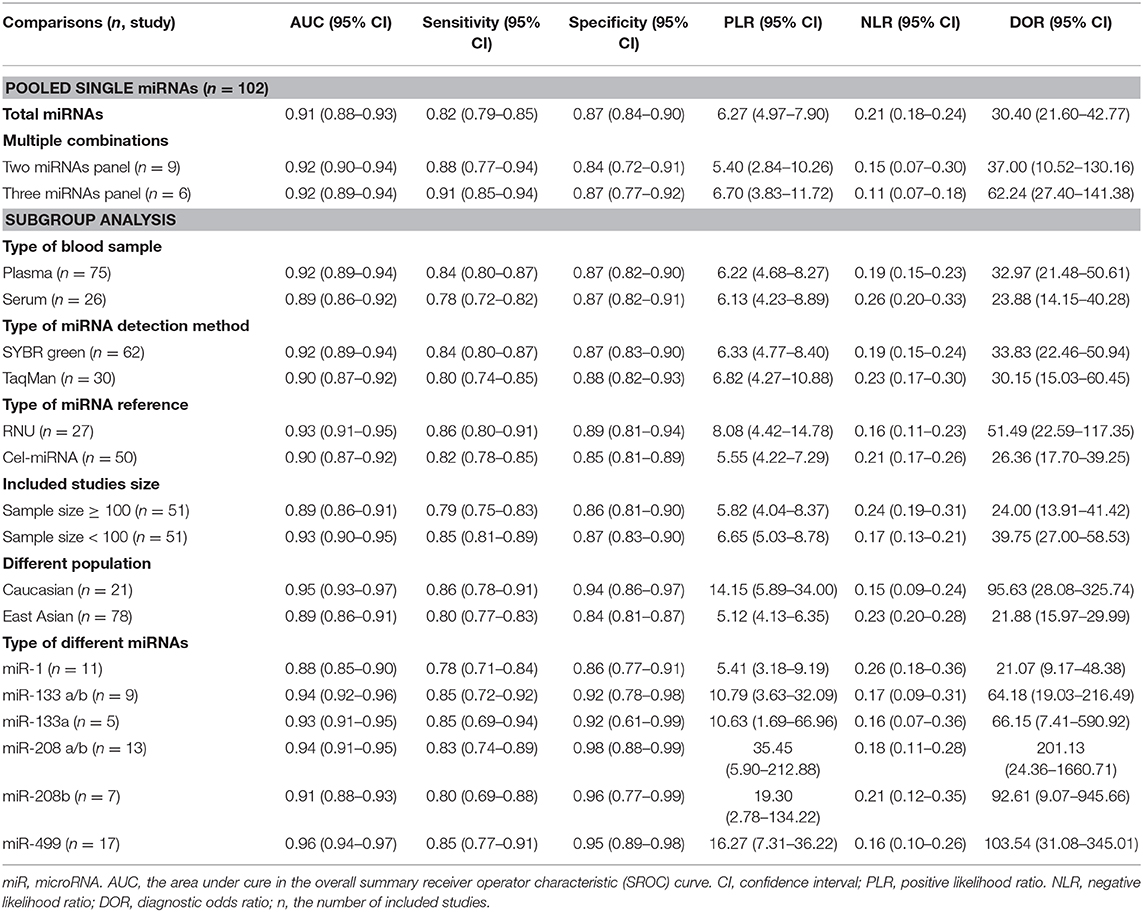
Table 4. The overall and subgroups meta-analysis results for comparison of diagnostic value of miRNAs.
Panels of Multiple miRNAs
As shown in Table 3, four studies (Hsu et al., 2014; Zhang R. et al., 2015; Shalaby et al., 2016; Wang et al., 2019) focused on the diagnostic value of a panel of two types of miRNAs, and the pooled sensitivity (Figure 3A) and specificity (Figure 3B) estimates were 0.88 (95% CI: 0.77–0.94) and 0.84 (95% CI: 0.72–0.91), respectively. The area under the SROC curve (Figure 3C) was 0.92 (95% CI: 0.90–0.94). The Deeks' test (Figure 3D) was performed to evaluate publication bias, and results suggested a low probability of publication bias.
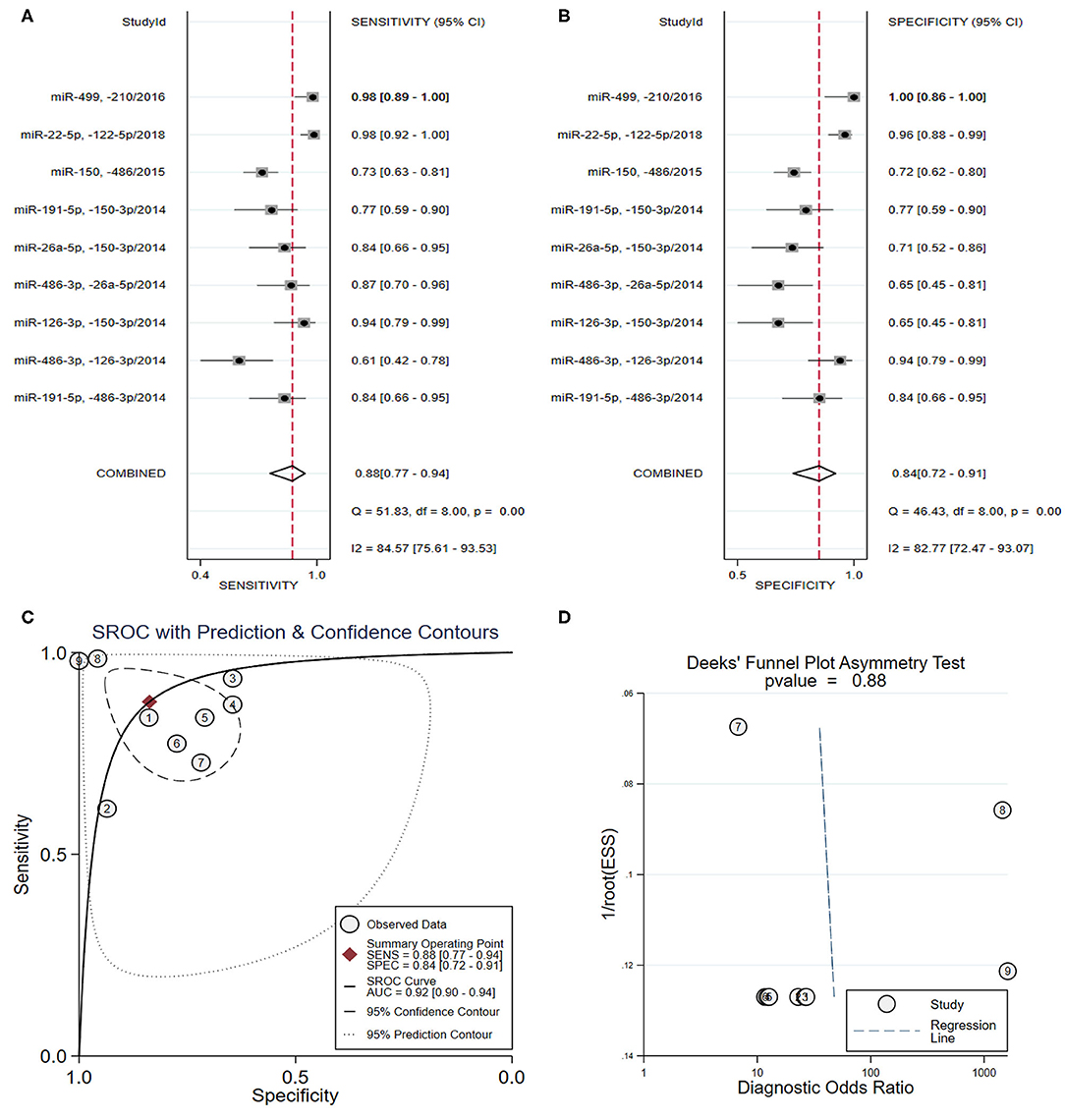
Figure 3. The sensitivity, specificity, summary receiver operator characteristic (SROC) curve with area under curve (AUC), and funnel graph of the combination of two miRNAs in the diagnosis of acute myocardial infarction. (A) Sensitivity. (B) Specificity. (C) SROC curve with AUC. (D) Funnel graph.
From the analysis of a panel of three types of miRNAs in six studies (Long et al., 2012b; Wang et al., 2014, 2016; Ke-Gang et al., 2016; Li H. et al., 2019; Xue et al., 2019a,b) (Table 3), the pooled sensitivity (Figure 4A) and specificity (Figure 4B) estimates were 0.91 (95% CI: 0.85–0.94) and 0.87 (95% CI: 0.77–0.92), respectively. The area under the SROC curve (Figure 4C) was 0.92 (95% CI: 0.89–0.94). The Deeks' test was performed and suggested that publication bias likely had a low effect on the summary estimates (Figure 4D).
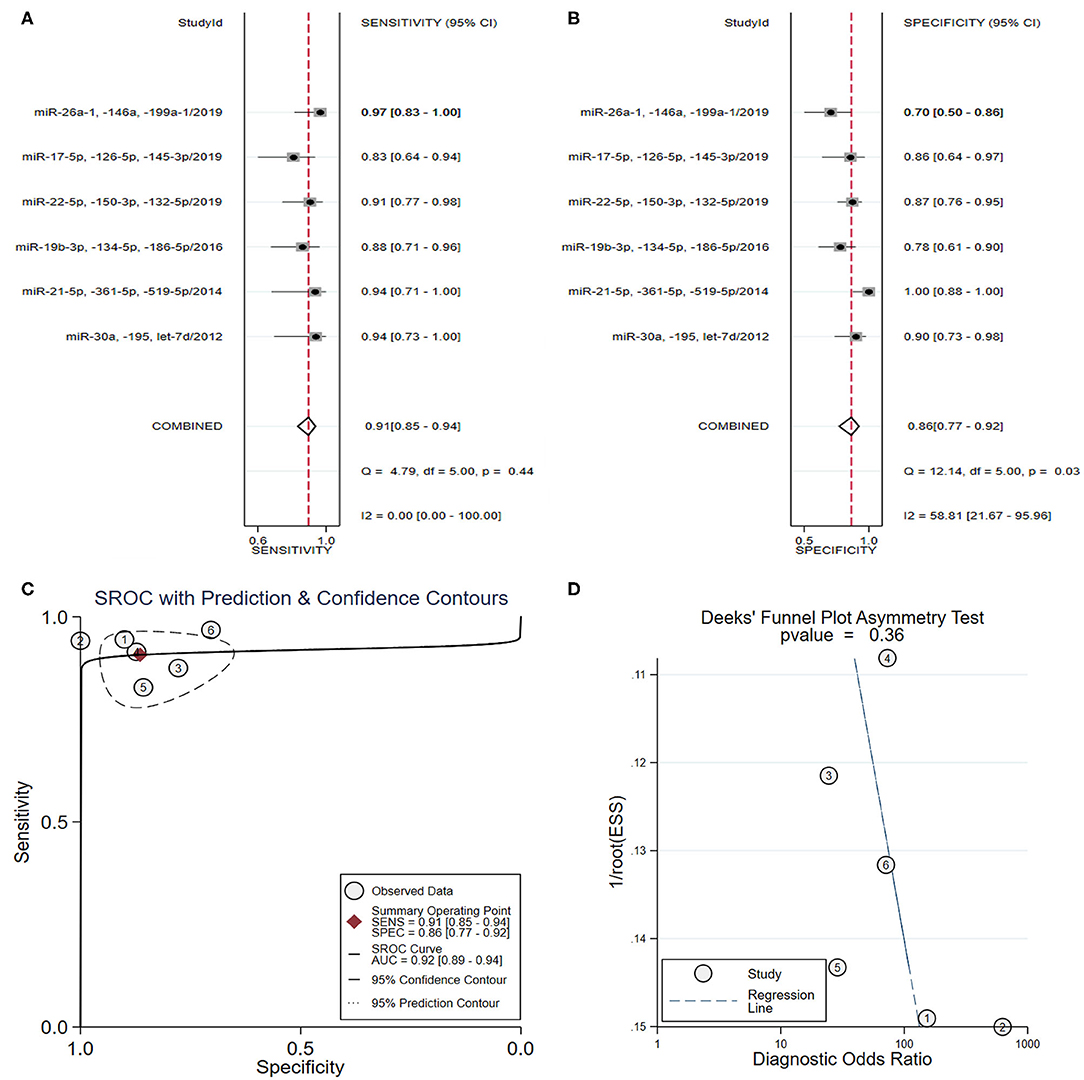
Figure 4. The sensitivity, specificity, summary receiver operator characteristic (SROC) curve with area under curve (AUC), and funnel graph of the combination of three miRNAs in the diagnosis of acute myocardial infarction. (A) Sensitivity. (B) Specificity. (C) SROC curve with AUC. (D) Funnel graph.
Sensitivity Analyses
Sensitivity analyses were performed on the included studies according to the following factors: (1) Type of patient blood sample (plasma vs. serum): the SROC values were 0.92 vs. 0.89, the pooled sensitivity and specificity were 0.84 vs. 0.78 and 0.87 vs. 0.87, respectively; (2) Type of miRNA detection method (SYBR green vs TaqMan): the SROC values were 0.92 vs. 0.90, the pooled sensitivity and specificity were 0.84 vs. 0.80 and 0.87 vs. 0.88, respectively; (3) Type of miRNA reference used for normalization (RNU or Cel-miRNA): the SROC values were 0.93 vs. 0.90, the pooled sensitivity and specificity were 0.86 vs. 0.82 and 0.89 vs. 0.85, respectively; (4) different study sizes (sample size ≥ 100 vs. sample size <100): the SROC values were 0.89 vs 0.93, the pooled sensitivity and specificity were 0.79 vs. 0.85 and 0.86 vs. 0.87, respectively; (5) Different populations (Caucasian vs. East Asian): the SROC values were 0.95 vs. 0.89, the pooled sensitivity and specificity were 0.86 vs. 0.80 and 0.94 vs. 0.84, respectively. A summary of the sensitivity analysis results is shown in Table 4. According to compared diagnostic values from each of the above groups, no major improvement or differences were found in the diagnostic accuracy values.
Meta-Analysis by Types of miRNAs
miRNA-1
In total, 11 studies identifying the diagnostic value of miRNA-1 in AMI were included in the meta-analysis (Ai et al., 2010; Corsten et al., 2010; Wang et al., 2010; Gidlöf et al., 2011, 2013; Long et al., 2012a; Li C. et al., 2013; Li Y. Q. et al., 2013; Li L. M. et al., 2014; Liu et al., 2015, 2018) (Table 3). As shown in Figures 5A,B, the pooled sensitivity and specificity estimates were 0.78 (95% CI: 0.71–0.84) and 0.86 (95% CI: 0.77–0.91), respectively. The area under the SROC curve for miRNA-1 was 0.88 (95% CI: 0.85–0.90) (Figure 5C). The pooled PLR was 5.41 (95% CI: 3.18–9.19), and the pooled NLR was 0.26 (95% CI: 0.18–0.36). The DOR was 21.07 (95% CI: 9.17–48.38). Additionally, the Deeks' test suggested that publication bias may have some effect on the summary estimates (p-value = 0.01) (Figure 5D). Representative results from the above analyses are shown in Table 4.
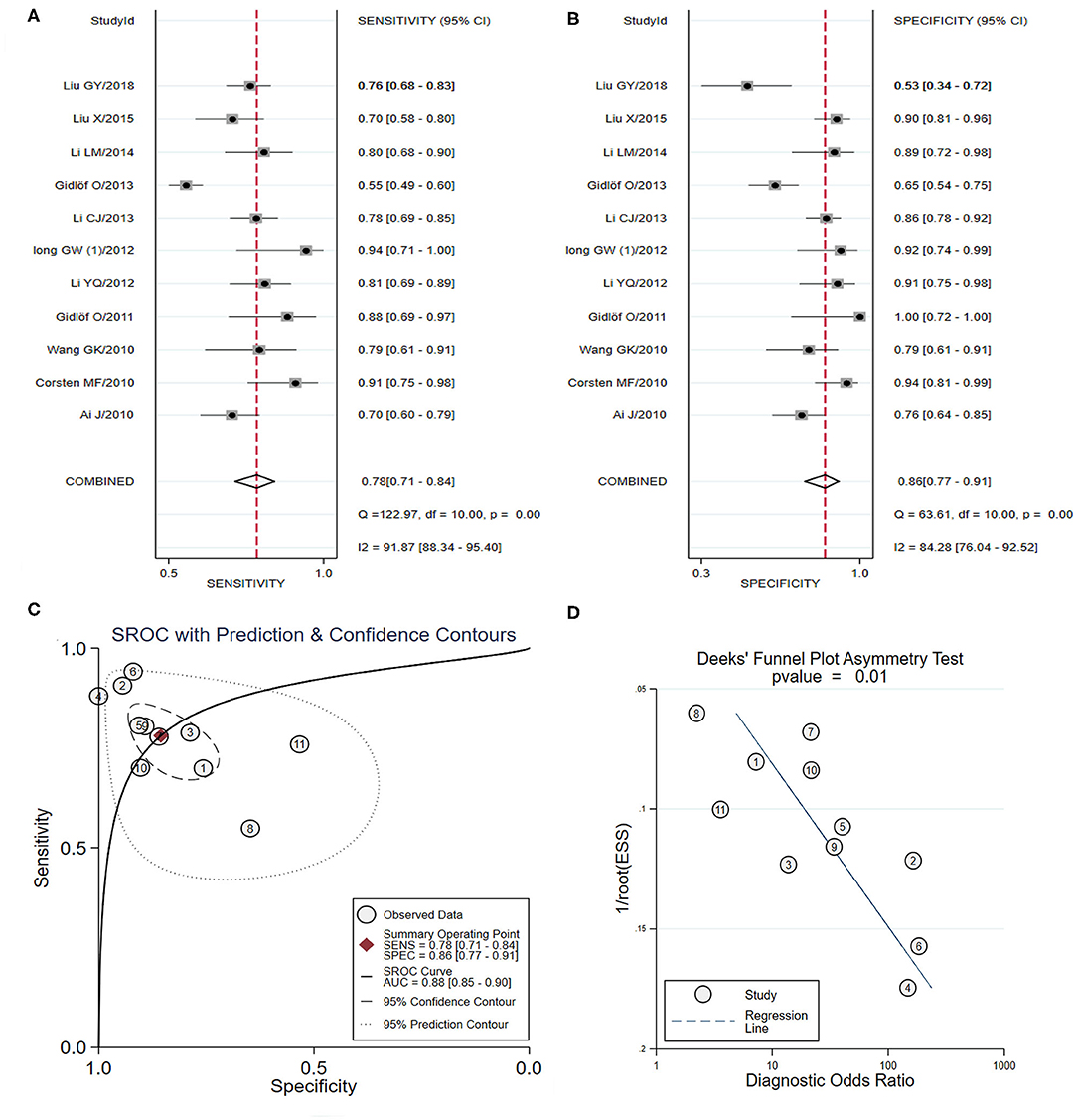
Figure 5. The sensitivity, specificity, summary receiver operator characteristic (SROC) curve with area under curve (AUC), and funnel graph of miRNA-1 in the diagnosis of acute myocardial infarction. (A) Sensitivity. (B) Specificity. (C) SROC curve with AUC. (D) Funnel graph.
miRNA-133
Nine studies that focused on the diagnostic accuracy of miRNA-133 (including miRNA-133a/b) in AMI were included in the meta-analysis (Corsten et al., 2010; D'Alessandra et al., 2010; Wang et al., 2010, 2011, 2013; Gidlöf et al., 2011; Li Y. Q. et al., 2013; Olivieri et al., 2013; Peng et al., 2014; Ji et al., 2015; Ke-Gang et al., 2016; Liu et al., 2018) (Table 3). As shown in Figures 6A,B, the pooled sensitivity and specificity estimates with 95% CI were 0.85 (95% CI: 0.72–0.92) and 0.92 (95% CI: 0.78–0.98), respectively. The area under the SROC curve for miRNA-133 was 0.94 (95% CI: 0.92–0.96) (Figure 6C). The pooled PLR was 10.79 (95% CI: 3.63–32.09) and the pooled NLR was 0.17 (95% CI: 0.09–0.31). The DOR was 64.18 (95% CI: 19.03–216.49). The Deeks' test suggested a potential publication bias (p-value = 0.01) (Figure 6D). Further subgroup analysis was conducted on miRNA-133a in the diagnosis of AMI and the SROC value, the pooled sensitivity, specificity, and DOR in the five studies (Wang et al., 2010; Gidlöf et al., 2011; Li Y. Q. et al., 2013; Ji et al., 2015; Ke-Gang et al., 2016) were 0.93 (95% CI: 0.91–0.95), 0.85 (95% CI: 0.69–0.94), 0.92 (95% CI: 0.61–0.99), and 66.15 (95% CI: 7.41–590.92). Representative results from the above analyses are shown in Table 4.
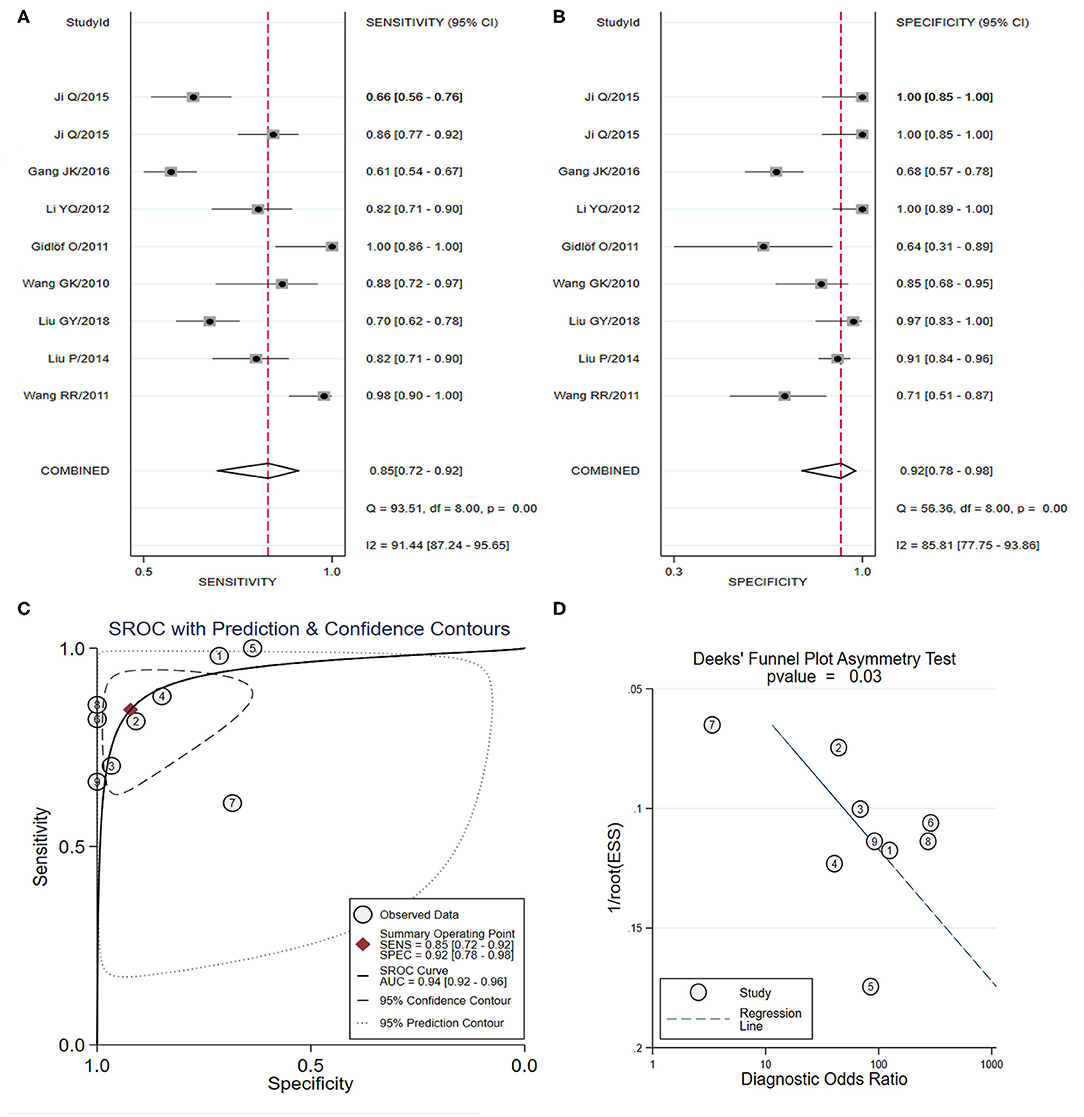
Figure 6. The sensitivity, specificity, summary receiver operator characteristic (SROC) curve with area under curve (AUC), and funnel graph of the miRNA-133 family in the diagnosis of acute myocardial infarction. (A) Sensitivity. (B) Specificity. (C) SROC curve with AUC. (D) Funnel graph.
miRNA-208
Thirteen studies evaluated the diagnostic value of miRNA-208 (including miRNA-208a/b) in AMI and were included in the meta-analysis (Corsten et al., 2010; Wang et al., 2010; Gidlöf et al., 2011, 2013; Devaux et al., 2012, 2015; Li C. et al., 2013; Li Y. Q. et al., 2013; Li et al., 2015; Liu et al., 2015, 2018; Agiannitopoulos et al., 2018; Li P. et al., 2019) (Table 3). As shown in Figures 7A,B, the pooled sensitivity and specificity estimates with 95% CI were 0.83 (95% CI: 0.74–0.89) and 0.98 (95% CI: 0.88–0.99), respectively. The area under the SROC curve for miRNA-208 was 0.94 (95% CI: 0.91–0.95) (Figure 7C). The pooled PLR was 35.45 (95% CI: 5.90–212.88), and the pooled NLR was 0.18 (95% CI: 0.11–0.28). The DOR was 201.13 (95% CI: 24.36–1660.71). The Deeks' test suggested a possible publication bias (p-value = 0.04) (Figure 7D). In the subgroup analysis of miRNA-208b in the diagnosis of AMI, the SROC value, the pooled sensitivity, specificity, and DOR in the seven studies (Corsten et al., 2010; Gidlöf et al., 2011, 2013; Devaux et al., 2012, 2015; Li Y. Q. et al., 2013; Li et al., 2015) were 0.91 (95% CI: 0.88–0.93), 0.80 (95% CI: 0.69–0.88), 0.96 (95% CI: 0.77–0.99), 92.61 (95% CI: 9.07–945.66). Representative results from the above analyses are shown in Table 4.
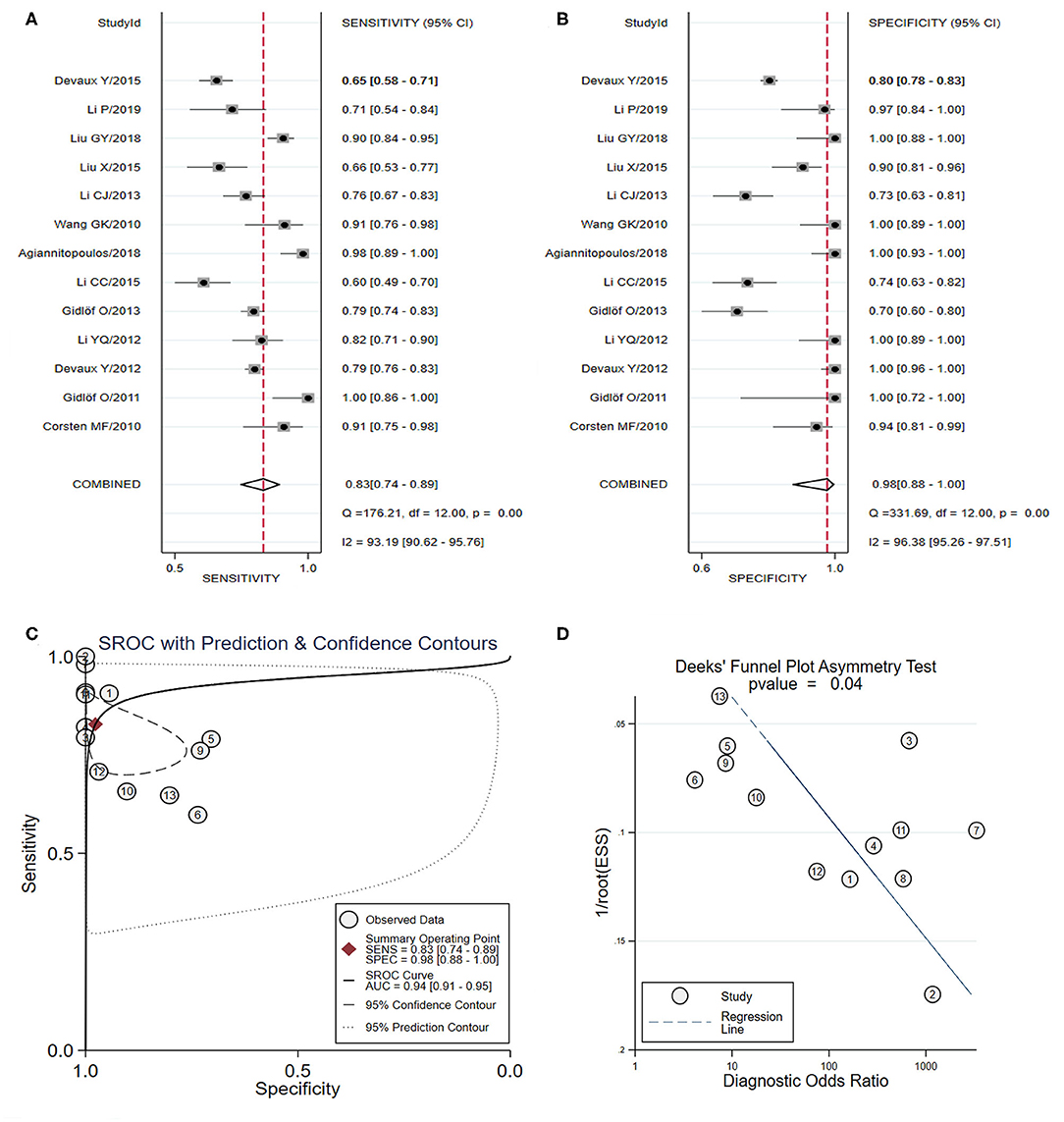
Figure 7. The sensitivity, specificity, summary receiver operator characteristic (SROC) curve with area under curve (AUC), and funnel graph of the miRNA-208 family in the diagnosis of acute myocardial infarction. (A) Sensitivity. (B) Specificity. (C) SROC curve with AUC. (D) Funnel graph.
miRNA-499
Seventeen studies involving 3,976 individuals investigated the diagnostic accuracy of miRNA-499 as a novel biomarkers for AMI (Corsten et al., 2010; Wang et al., 2010; Gidlöf et al., 2011, 2013; Devaux et al., 2012, 2015; Li C. et al., 2013; Li Y. Q. et al., 2013; Olivieri et al., 2013; Liu et al., 2015, 2018; Zhang L. et al., 2015; Zhang R. et al., 2015; Shalaby et al., 2016; Agiannitopoulos et al., 2018; Fawzy et al., 2018; Li P. et al., 2019) (Table 3). As shown in Figures 8A,B, the pooled sensitivity and specificity estimates with 95%CI were 0.85 (95% CI: 0.77–0.91) and 0.95 (95% CI: 0.89–0.98), respectively. The area under the SROC curve for miRNA-499 was 0.96 (95% CI: 0.94–0.97) (Figure 8C). The pooled PLR was 16.27 (95% CI: 7.31–36.22), and the pooled NLR was 0.16 (95% CI: 0.10–0.26). The DOR was 103.54 (95% CI: 31.08–345.01). The Deeks' test suggested a low possibility of publication bias (p-value = 0.12) (Figure 8D). Representative results from the above analyses are shown in Table 4.
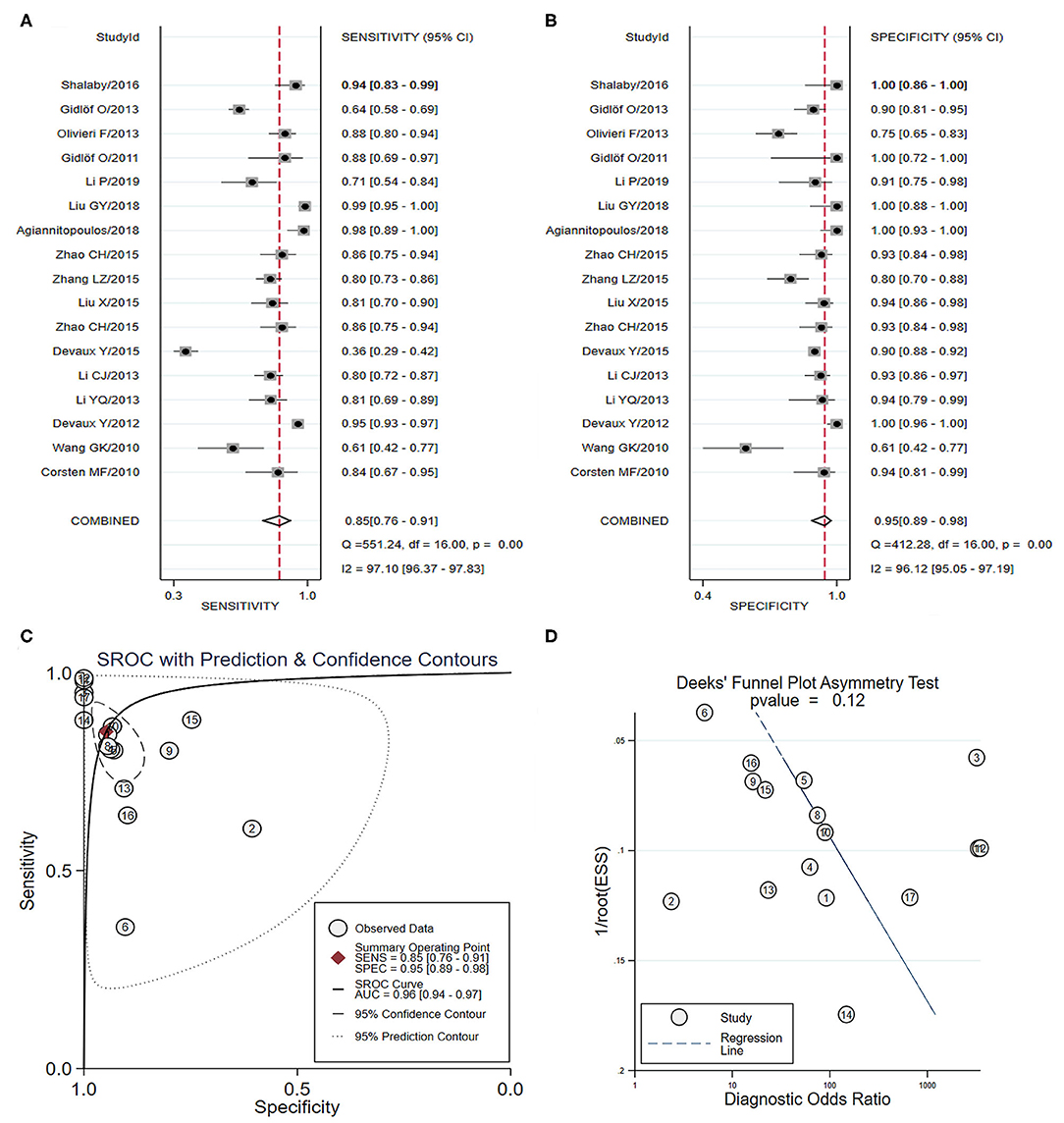
Figure 8. The sensitivity, specificity, summary receiver operator characteristic (SROC) curve with area under curve (AUC), and funnel graph of miRNA-499 in the diagnosis of acute myocardial infarction. (A) Sensitivity. (B) Specificity. (C) SROC curve with AUC. (D) Funnel graph.
Discussion
This systematic review and meta-analysis of 58 manuscripts that utilize blood circulating miRNAs (including plasma- or serum-based) in the diagnosis of AMI identified 51 significantly dysregulated miRNAs between AMI cases and controls. Additionally, this review assessed the feasibility of using these miRNAs as novel biomarkers for the diagnosis of AMI patients. Sixteen of the abnormally expressed miRNAs were investigated by more than one study, including thirteen upregulated miRNAs: miRNA-1, miRNA-19b-3p, miRNA-21, miRNA-122-5p, miRNA-126, miRNA-133a/b, miRNA-134, miRNA-150, miRNA-186, miRNA-208a/b, miRNA-486, miRNA-499, and miRNA-663b, and three downregulated miRNAs: miRNA-26a, miRNA-191, and miRNA-375. A further 34 dysregulated miRNAs were only reported by one study. The overall pooled diagnostic data of total miRNAs expression were as follows: SROC curve with AUC: 0.91, sensitivity: 0.82, specificity: 0.87, showing that circulating miRNAs might be suitable for use as potential biomarkers of AMI. Furthermore, the present meta-analysis was conducted via subgroup analyses based on type of miRNAs, including miRNA-1, miRNA-133a/b, miRNA-208a/b, and miRNA-499. MiRNA-499 had the highest diagnostic value (sensitivity: 0.85, specificity: 0.95, SROC curve with AUC: 0.96), followed by miRNA-133a (sensitivity: 0.85, specificity: 0.92, SROC curve with AUC: 0.93), and miRNA-208b had better specificity (0.96) than sensitivity (0.80). These results indicate a relatively high diagnostic accuracy for AMI based on significantly dysregulated miRNAs.
It is well-known that an early, accurate diagnosis and effective revascularization therapy play vital roles in reducing morbidity and mortality in patients with AMI (Yeh et al., 2010). At present, cardiac troponin, creatine kinase-MB (CK-MB), and myoglobin are the most widely used biomarkers in the diagnosis of AMI (de Winter et al., 1995). A good standard for the early diagnosis of AMI is an increase of cTn level (Celik et al., 2011). However, these markers are also likely to be elevated in patients with other diseases, whether or not CAD is also present (French and White, 2004). The detection of cTn has time constraints, as significant levels are reached 4–8 h following the onset of ischemia symptoms. Thus, novel genetic and molecular biomarkers of myocardial damage that have high sensitivity and specificity are still urgently needed.
Significant advances have occurred in the field of cardiovascular disease and miRNAs since their first discovery in the blood (Karakas et al., 2017). A growing number of studies indicate that the abnormal expression of miRNAs plays a critical role due to their various pathological functions in the presence of myocardial infarction (Gurha, 2016; Moghaddam et al., 2019). MiRNAs are steadily present in bodily fluids (including plasma, serum, urine, and saliva) due to protection from RNase via binding to argonaute proteins and the ability to be released from cells via microvesicles, exosomes, or bound to proteins (Meister, 2013). Moreover, recent studies have showed that cTn is more difficult to detect than miRNAs in patients with MI during the earlier acute stage, as it is usually below the cut-off value (Gidlöf et al., 2013; Zhang L. et al., 2015). This suggests a difference between these two types of biomarkers in the physiological process of myocardial infarction. Cardiac troponin releases into the blood during necrosis and during the pathological process of myocardial hypoxia and ischemia (Wu and Ford, 1999). However, miRNAs can be released in response to several forms of cellular stress occurring earlier then cell necrosis such as anoxia, lactic acidosis, and cellular edema (Edeleva and Shcherbata, 2013). Thus, experts may consider the expression levels of dysregulated miRNAs at an earlier stage of AMI, as they might be reliable candidate biomarkers for the diagnosis of AMI (Li C. et al., 2013).
In this study, the summary of single miRNAs showed that miRNA-1, miRNA-133, miRNA-208, and miRNA-499 are potential candidates for the detection of AMI, as they were most frequently detected in the previous studies. Among these individual miRNAs, circulating miRNA-499 might be an effective candidate biomarker of AMI. Some studies have demonstrated that miRNA-499 was specifically expressed in the myocardium and skeletal muscle of mammals (Xue et al., 2019a) and played a critical role in the recovery process following cardiac injury (Hosoda et al., 2011). Based on the present study, miRNA-499 has a higher sensitivity and specificity in identifying patients with AMI, and these results were similar to or better than previous studies (Cheng et al., 2014; Zhao et al., 2019). Previous studies were based on relatively small sample sizes and did not include studies published in recent years. Thus, the results of the present study are more reliable and convincing. Furthermore, we strictly considered the precise setting of specific miRNAs in the diagnosis of AMI and that assessing their diagnostic performance in combination with other biomarkers, especially highly sensitive troponin immunoassays, may be warranted. A study by Olivieri et al. showed a significant correlation between miRNA-499 and cTnT, and that the diagnosis value of this combination was superior to either one alone (Olivieri et al., 2013). However, another study reported that the diagnostic value of miRNA-499 and hs-cTnT combined was not better than either them alone (Devaux et al., 2012). Thus, due to the limited sample sizes of these studies, further research is required.
There are only a small number of high-quality studies with large sample sizes focused on the diagnostic value of miRNAs in AMI. To the best of our knowledge, this study has included the largest sample size of dysregulated miRNAs as novel biomarkers for AMI for summary and evaluation. Further high-quality studies should be performed to acquire more reliable data for use in formulating standard diagnostic criterion and to determine optimal cut-off values. Moreover, due to the different diagnostic values of miRNAs, our study demonstrated that a panel of 2 or 3 miRNAs might be superior for diagnostic accuracy. The combination of 3 miRNAs trended toward a higher sensitivity than others for use as biomarkers in the diagnosis of AMI. Therefore, to further improve the feasibility of clinical diagnosis, future research should explore the most effective combination of multiple miRNAs, especially those confirmed to have a higher utilization value in the single miRNA groups.
Aside from the many studies investigating miRNA profiles in the detection of AMI, researchers should pay closer attention to the search for the technology to detect miRNAs quickly and accurately. Methods of RNA detection tend to be time-consuming, expensive, require sophisticated techniques, and are difficult to implement for urgent testing, especially in some developing countries (Lippi et al., 2013). However, novel detection technologies developed in recent years may provide a solution to these tissues, which would also support the clinical application of miRNAs in the future. Examples of new technologies include isothermal reactions based on cleavage with DNAzyme and signal amplification, which can simultaneously amplify and detect RNA (Zhao et al., 2013). This method is thought to be immune to genomic DNA pollution and has a relatively reliable sensitivity and specificity. We believed that new, precise methods of diagnosis that can detect miRNAs very rapidly and inexpensively need to be continuously improved.
In addition, the heterogeneity of the results of this study were substantial and could not be completely resolved. We found that the sources of heterogeneity included the following: quality of included studies, age, gender proportion, regional and environmental factors, and sampling criteria. Despite the heterogeneity, we believe the results of this study are worthwhile and valuable. Results of the overall and stratified analysis of different subgroups trended toward satisfactory values of miRNAs as novel biomarkers in the diagnosis of AMI. Furthermore, it was remarkable that some publication bias was found in the present study and might imply that the potential negative results were less likely to be published.
Although this study had a satisfactory result regarding the use of miRNAs for AMI detection, conclusions should be drawn cautiously due to several limitations: (1) there was a lack of standardization due to different normalization procedures across the included studies; (2) the exclusion of non-English articles may have caused important studies to be overlooked and publication bias due to significant results being more easily published; (3) the combined analysis of multiple miRNAs for a panel were insufficient, and we were unable to conduct a meta-analysis based on the data from limited studies; and (4) the results may have been affected by the impact of inevitable clinical heterogeneity, including the general condition of the included individuals, effects of medication, and medical history.
Conclusion
The current systematic review identifies numerous miRNAs associated with AMI and suggested that miRNAs may be used as a potential biomarker for the detection of AMI. For single, stand-alone miRNAs, miRNA-499 had better diagnostic accuracy than other miRNAs. A panel of two or three miRNAs might be superior for diagnostic accuracy. To develop a diagnostic test for AMI diagnosis, we suggest that a panel of miRNAs with high sensitivity and specificity should be tested. For this purpose, large scale, high-quality studies are still required to validate the clinical application of miRNAs for AMI diagnostics, as well as to identify the precise setting of dysregulated miRNAs in patients with AMI.
Data Availability Statement
Publicly available datasets were analyzed in this study. Datasets are available through the corresponding author upon reasonable request.
Ethics Statement
All analyses were based on previous published studies; thus no ethical approval or patient consent were required. All previous published studies were approved by Ethics Committee, respectively.
Author Contributions
HC and CZ designed the study. CZ carried out the statistical analysis and participated in most of the study steps. CZ, RL, JC, KH, and MA prepared the manuscript and assisted in the study processes. YH, JZ, YZ, LW, and RZ assisted in the data collection and helped in the interpretation of the study. All authors read and approved the final manuscript.
Funding
The authors gratefully acknowledge the financial support by Tianjin Chest Hospital Labor Union (HL Cong's Model Worker Innovation Studio).
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Acknowledgments
We thank LetPub (https://www.letpub.com) for the linguistic assistance during the preparation of this manuscript. Additionally, we thank Tianjin Chest Hospital Labor Union.
Supplementary Material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fphys.2020.00691/full#supplementary-material
Supplementary Figure 1. Methodological quality of studies in the meta-analysis using the Quality Assessment of Diagnostic Accuracy Studies 2 score system, including risk of bias and applicability concerns. The items were scored with “yes,” “no,” or “unsure”.
Supplementary Figure 2. Forest plots of the total miRNAs in the diagnosis of acute myocardial infarction among the studies included in the meta-analysis. (A) Sensitivity. (B) Specificity.
Supplementary Figure 3. Summary receiver operator characteristic (SROC) curve with area under the curve (AUC) and funnel graph of the total miRNAs in the diagnosis of acute myocardial infarction. (A) SROC curve with AUC. (B) Funnel graph.
References
Adachi, T., Nakanishi, M., Otsuka, Y., Nishimura, K., Hirokawa, G., Goto, Y., et al. (2010). Plasma microRNA 499 as a biomarker of acute myocardial infarction. Clin. Chem. 56, 1183–1185. doi: 10.1373/clinchem.2010.144121
Agiannitopoulos, K., Pavlopoulou, P., Tsamis, K., Bampali, K., Samara, P., Nasioulas, G., et al. (2018). Expression of miR-208b and miR-499 in Greek patients with acute myocardial infarction. In Vivo 32, 313–318. doi: 10.21873/invivo.11239
Ai, J., Zhang, R., Li, Y., Pu, J., Lu, Y., Jiao, J., et al. (2010). Circulating microRNA-1 as a potential novel biomarker for acute myocardial infarction. Biochem. Biophys. Res. Commun. 391, 73–77. doi: 10.1016/j.bbrc.2009.11.005
Anand, A., Shah, A. S. V. S., Beshiri, A., Jaffe, A. S., and Mills, N. L. (2019). Global adoption of high-sensitivity cardiac troponins and the universal definition of myocardial infarction. Clin. Chem. 65, 484–489. doi: 10.1373/clinchem.2018.298059
Bartel, D. P. (2004). MicroRNAs: genomics, biogenesis, mechanism, and function. Cell 116, 281–297. doi: 10.1016/s0092-8674(04)00045-5
Białek, S., Górko, D., Zajkowska, A., Kołtowski, Ł., Grabowski, M., Stachurska, A., et al. (2015). Release kinetics of circulating miRNA-208a in the early phase of myocardial infarction. Kardiol. Pol. 73, 613–619. doi: 10.5603/KP.a2015.0067
Bukauskas, T., Mickus, R., Cereskevicius, D., and Macas, A. (2019). Value of serum miR-23a, miR-30d, and miR-146a biomarkers in ST-elevation myocardial infarction. Med. Sci. Monit. 25, 3925–3932. doi: 10.12659/MSM.913743
Carter, J. V., Pan, J., Rai, S. N., and Galandiuk, S. (2016). ROC-ing along: evaluation and interpretation of receiver operating characteristic curves. Surgery 159, 1638–1645. doi: 10.1016/j.surg.2015.12.029
Celik, S., Giannitsis, E., Wollert, K. C., Schwöbel, K., Lossnitzer, D., Hilbel, T., et al. (2011). Cardiac troponin T concentrations above the 99th percentile value as measured by a new high-sensitivity assay predict long-term prognosis in patients with acute coronary syndromes undergoing routine early invasive strategy. Clin. Res. Cardiol. 100, 1077–1085. doi: 10.1007/s00392-011-0344-x
Chen, X., Zhang, L., Su, T., Li, H., Huang, Q., Wu, D., et al. (2015). Kinetics of plasma microRNA-499 expression in acute myocardial infarction. J. Thorac. Dis. 7, 890–896. doi: 10.3978/j.issn.2072-1439.2014.11.32
Cheng, C., Wang, Q., You, W., Chen, M., and Xia, J. (2014). MiRNAs as biomarkers of myocardial infarction: a meta-analysis. PLoS ONE 9:e88566. doi: 10.1371/journal.pone.0088566
Cheng, Y., Tan, N., Yang, J., Liu, X., Cao, X., He, P., et al. (2010). A translational study of circulating cell-free microRNA-1 in acute myocardial infarction. Clin. Sci. 119, 87–95. doi: 10.1042/CS20090645
Chevillet, J. R., Lee, I., Briggs, H. A., He, Y., and Wang, K. (2014). Issues and prospects of microRNA-based biomarkers in blood and other body fluids. Molecules 19, 6080–6105. doi: 10.3390/molecules19056080
Corsten, M. F., Dennert, R., Jochems, S., Kuznetsova, T., Devaux, Y., Hofstra, L., et al. (2010). Circulating MicroRNA-208b and MicroRNA-499 reflect myocardial damage in cardiovascular disease. Circ. Cardiovasc. Genet. 3, 499–506. doi: 10.1161/CIRCGENETICS.110.957415
D'Alessandra, Y., Devanna, P., Limana, F., Straino, S., Di, C. A., Brambilla, P. G., et al. (2010). Circulating microRNAs are new and sensitive biomarkers of myocardial infarction. Eur. Heart J. 31, 2765–2773. doi: 10.1093/eurheartj/ehq167
de Winter, R. J., Koster, R. W., Sturk, A., and Sanders, G. T. (1995). Value of myoglobin, troponin T, and CK-MBmass in ruling out an acute myocardial infarction in the emergency room. Circulation 92, 3401–3407. doi: 10.1161/01.cir.92.12.3401
Deeks, J. J., Macaskill, P., and Irwig, L. (2005). The performance of tests of publication bias and other sample size effects in systematic reviews of diagnostic test accuracy was assessed. J. Clin. Epidemiol. 58, 882–893. doi: 10.1016/j.jclinepi.2005.01.016
Devaux, Y., Mueller, M., Haaf, P., Goretti, E., Twerenbold, R., Zangrando, J., et al. (2015). Diagnostic and prognostic value of circulating microRNAs in patients with acute chest pain. J. Intern. Med. 277, 260–271. doi: 10.1111/joim.12183
Devaux, Y., Vausort, M., Goretti, E., Nazarov, P. V., Azuaje, F., Gilson, G., et al. (2012). Use of circulating microRNAs to diagnose acute myocardial infarction. Clin. Chem. 58, 559–567. doi: 10.1373/clinchem.2011.173823
Dohi, T., Maehara, A., Brener, S. J., Généreux, P., Gershlick, A. H., Mehran, R., et al. (2015). Utility of peak creatine kinase-MB measurements in predicting myocardial infarct size, left ventricular dysfunction, and outcome after first anterior wall acute myocardial infarction (from the INFUSE-AMI trial). Am. J. Cardiol. 115, 563–570. doi: 10.1016/j.amjcard.2014.12.008
Edeleva, E. V., and Shcherbata, H. R. (2013). Stress-induced ECM alteration modulates cellular microRNAs that feedback to readjust the extracellular environment and cell behavior. Front. Genet. 4:305. doi: 10.3389/fgene.2013.00305
Fawzy, M. S., Toraih, E. A., Hamed, E. O., Hussein, M. H., and Ismail, H. M. (2018). Association of MIR-499a expression and seed region variant (rs3746444) with cardiovascular disease in Egyptian patients. Acta Cardiol. 73, 131–140. doi: 10.1080/00015385.2017.1351243
Finsterer, J., Stöllberger, C., and Krugluger, W. (2007). Cardiac and noncardiac, particularly neuromuscular, disease with troponin-T positivity. Neth. J. Med. 65, 289–295.
French, J. K., and White, H. D. (2004). Clinical implications of the new definition of myocardial infarction. Heart 90, 99–106. doi: 10.1136/heart.90.1.99
Gabisonia, K., Prosdocimo, G., Aquaro, G. D., Carlucci, L., Zentilin, L., Secco, I., et al. (2019). MicroRNA therapy stimulates uncontrolled cardiac repair after myocardial infarction in pigs. Nature 569, 418–422. doi: 10.1038/s41586-019-1191-6
Gao, H., Guddeti, R. R., Matsuzawa, Y., Liu, L. P., Su, L. X., Guo, D., et al. (2015). Plasma levels of microRNA-145 are associated with severity of Coronary Artery Disease. PLoS ONE 10:e0123477. doi: 10.1371/journal.pone.0123477
GBD 2013 Mortality and Causes of Death Collaborators (2015). Global, regional, and national age-sex specific all-cause and cause-specific mortality for 240 causes of death, 1990-2013: a systematic analysis for the Global Burden of Disease Study 2013. Lancet 385, 117–171. doi: 10.1016/S0140-6736(14)61682-2
Gidlöf, O., Andersson, P., van der Pals, J., Götberg, M., and Erlinge, D. (2011). Cardiospecific microRNA plasma levels correlate with troponin and cardiac function in patients with ST elevation myocardial infarction, are selectively dependent on renal elimination, and can be detected in urine samples. Cardiology 118, 217–226. doi: 10.1159/000328869
Gidlöf, O., Smith, J. G., Miyazu, K., Gilje, P., Spencer, A., Blomquist, S., et al. (2013). Circulating cardio-enriched microRNAs are associated with long-term prognosis following myocardial infarction. BMC Cardiovasc. Disord. 13:12. doi: 10.1186/1471-2261-13-12
Guo, M. L., Guo, L. L., and Weng, Y. Q. (2017). Implication of peripheral blood miRNA-124 in predicting acute myocardial infarction. Eur. Rev. Med. Pharmacol. Sci. 21, 1054–1059.
Gurha, P. (2016). MicroRNAs in cardiovascular disease. Curr. Opin. Cardiol. 31, 249–254. doi: 10.1097/HCO.0000000000000280
Han, Z., Zhang, L., Yuan, L., Liu, X., Chen, X., Ye, X., et al. (2015). Change of plasma microRNA-208 level in acute myocardial infarction patients and its clinical significance. Ann. Transl. Med. 3:307. doi: 10.3978/j.issn.2305-5839.2015.10.25
He, F., Lv, P., Zhao, X., Wang, X., Ma, X., Meng, W., et al. (2014). Predictive value of circulating miR-328 and miR-134 for acute myocardial infarction. Mol. Cell. Biochem. 394, 137–144. doi: 10.1007/s11010-014-2089-0
Hoffmeister, H. M., Ehlers, R., Büttcher, E., Steinmetz, A., Kazmaier, S., Helber, U., et al. (2003). Relationship between minor myocardial damage and inflammatory acute-phase reaction in acute coronary syndromes. J. Thromb. Thrombolysis 15, 33–39. doi: 10.1023/a:1026140317777
Hosoda, T., Zheng, H., Cabral-da-Silva, M., Sanada, F., Ide-Iwata, N., Ogórek, B., et al. (2011). Human cardiac stem cell differentiation is regulated by a mircrine mechanism. Circulation 123, 1287–1296. doi: 10.1161/CIRCULATIONAHA.110.982918
Hsu, A., Chen, S. J., Chang, Y. S., Chen, H. C., and Chu, P. H. (2014). Systemic approach to identify serum microRNAs as potential biomarkers for acute myocardial infarction. Biomed. Res. Int. 2014:418628. doi: 10.1155/2014/418628
Huang, S., Chen, M., Li, L., He, M., Hu, D., Zhang, X., et al. (2014). Circulating MicroRNAs and the occurrence of acute myocardial infarction in Chinese populations. Circ. Cardiovasc. Genet. 7, 189–198. doi: 10.1161/CIRCGENETICS.113.000294
Hung, J., Teng, T. H., Finn, J., Knuiman, M., Briffa, T., Stewart, S., et al. (2013). Trends from 1996 to 2007 in incidence and mortality outcomes of heart failure after acute myocardial infarction: a population-based study of 20,812 patients with first acute myocardial infarction in Western Australia. J. Am. Heart Assoc. 2:e000172. doi: 10.1161/JAHA.113.000172
Hutton, B., Salanti, G., Caldwell, D. M., Chaimani, A., Schmid, C. H., Cameron, C., et al. (2015). The PRISMA extension statement for reporting of systematic reviews incorporating network meta-analyses of health care interventions: checklist and explanations. Ann. Intern. Med. 162, 777–784. doi: 10.7326/M14-2385
Jakob, P., Kacprowski, T., Briand-Schumacher, S., Heg, D., Klingenberg, R., Stähli, B. E., et al. (2017). Profiling and validation of circulating microRNAs for cardiovascular events in patients presenting with ST-segment elevation myocardial infarction. Eur. Heart J. 38, 511–515. doi: 10.1093/eurheartj/ehw563
Ji, Q., Jiang, Q., Yan, W., Li, X., Zhang, Y., Meng, P., et al. (2015). Expression of circulating microRNAs in patients with ST segment elevation acute myocardial infarction. Minerva Cardioangiol. 63, 397–402.
Karakas, M., Schulte, C., Appelbaum, S., Ojeda, F., Lackner, K. J., Münzel, T., et al. (2017). Circulating microRNAs strongly predict cardiovascular death in patients with coronary artery disease-results from the large AtheroGene study. Eur. Heart J. 38, 516–523. doi: 10.1093/eurheartj/ehw250
Ke-Gang, J., Zhi-Wei, L., Xin, Z., Jing, W., Ping, S., Xue-Jing, H., et al. (2016). Evaluating diagnostic and prognostic value of plasma miRNA133a in acute chest pain patients undergoing coronary angiography. Medicine 95:e3412. doi: 10.1097/MD.0000000000003412
Lamb, E. J., Hall, E. M., and Fahie-Wilson, M. (2006). Cardiac troponins and chronic kidney disease. Kidney Int. 70, 1525–1526; author reply 1526. doi: 10.1038/sj.ki.5001802
Li, C., Chen, X., Huang, J., Sun, Q., and Wang, L. (2015). Clinical impact of circulating miR-26a, miR-191, and miR-208b in plasma of patients with acute myocardial infarction. Eur. J. Med. Res. 20:58. doi: 10.1186/s40001-015-0148-y
Li, C., Fang, Z., Jiang, T., Zhang, Q., Liu, C., Zhang, C., et al. (2013). Serum microRNAs profile from genome-wide serves as a fingerprint for diagnosis of acute myocardial infarction and angina pectoris. BMC Med. Genomics 6:16. doi: 10.1186/1755-8794-6-16
Li, H., Zhang, P., Li, F., Yuan, G., Wang, X., Zhang, A., et al. (2019). Plasma miR-22-5p, miR-132-5p, and miR-150-3p are associated with acute myocardial infarction. Biomed. Res. Int. 2019:5012648. doi: 10.1155/2019/5012648
Li, L. M., Cai, W. B., Ye, Q., Liu, J. M., Li, X., and Liao, X. X. (2014). Comparison of plasma microRNA-1 and cardiac troponin T in early diagnosis of patients with acute myocardial infarction. World J. Emerg. Med. 5, 182–186. doi: 10.5847/wjem.j.1920-8642.2014.03.004
Li, P., Li, S. Y., Liu, M., Ruan, J. W., Wang, Z. D., and Xie, W. C. (2019). Value of the expression of miR-208, miR-494, miR-499 and miR-1303 in early diagnosis of acute myocardial infarction. Life Sci. 232:116547. doi: 10.1016/j.lfs.2019.116547
Li, Y. Q., Zhang, M. F., Wen, H. Y., Hu, C. L., Liu, R., Wei, H. Y., et al. (2013). Comparing the diagnostic values of circulating microRNAs and cardiac troponin T in patients with acute myocardial infarction. Clinics 68, 75–80. doi: 10.6061/clinics/2013(01)oa12
Li, Z., Lu, J., Luo, Y., Li, S., and Chen, M. (2014). High association between human circulating microRNA-497 and acute myocardial infarction. Sci. World J. 2014:931845. doi: 10.1155/2014/931845
Lippi, G., Mattiuzzi, C., and Cervellin, G. (2013). Circulating microRNAs (miRs) for diagnosing acute myocardial infarction: meta-analysis of available studies. Int. J. Cardiol. 167, 277–278. doi: 10.1016/j.ijcard.2012.09.152
Liu, G., Niu, X., Meng, X., and Zhang, Z. (2018). Sensitive miRNA markers for the detection and management of NSTEMI acute myocardial infarction patients. J. Thorac. Dis. 10, 3206–3215. doi: 10.21037/jtd.2018.05.141
Liu, X., Fan, Z., Zhao, T., Cao, W., Zhang, L., Li, H., et al. (2015). Plasma miR-1, miR-208, miR-499 as potential predictive biomarkers for acute myocardial infarction: an independent study of Han population. Exp. Gerontol. 72, 230–238. doi: 10.1016/j.exger.2015.10.011
Long, G., Wang, F., Duan, Q., Chen, F., Yang, S., Gong, W., et al. (2012a). Human circulating microRNA-1 and microRNA-126 as potential novel indicators for acute myocardial infarction. Int. J. Biol. Sci. 8, 811–818. doi: 10.7150/ijbs.4439
Long, G., Wang, F., Duan, Q., Yang, S., Chen, F., Gong, W., et al. (2012b). Circulating miR-30a, miR-195 and let-7b associated with acute myocardial infarction. PLoS ONE 7:e50926. doi: 10.1371/journal.pone.0050926
Lorenzano, S., Rost, N. S., Khan, M., Li, H., Batista, L. M., Chutinet, A., et al. (2019). Early molecular oxidative stress biomarkers of ischemic penumbra in acute stroke. Neurology 93, e1288–e1298. doi: 10.1212/WNL.0000000000008158
Lu, H. Q., Liang, C., He, Z. Q., Fan, M., and Wu, Z. G. (2013). Circulating miR-214 is associated with the severity of coronary artery disease. J. Geriatr. Cardiol. 10, 34–38. doi: 10.3969/j.issn.1671-5411.2013.01.007
Mahid, S. S., Hornung, C. A., Minor, K. S., Turina, M., and Galandiuk, S. (2006). Systematic reviews and meta-analysis for the surgeon scientist. Br. J. Surg. 93, 1315–1324. doi: 10.1002/bjs.5596
Meder, B., Keller, A., Vogel, B., Haas, J., Sedaghat-Hamedani, F., Kayvanpour, E., et al. (2011). MicroRNA signatures in total peripheral blood as novel biomarkers for acute myocardial infarction. Basic Res. Cardiol. 106, 13–23. doi: 10.1007/s00395-010-0123-2
Meister, G. (2013). Argonaute proteins: functional insights and emerging roles. Nat. Rev. Genet. 14, 447–459. doi: 10.1038/nrg3462
Moghaddam, A. S., Afshari, J. T., Esmaeili, S. A., Saburi, E., Joneidi, Z., and Momtazi-Borojeni, A. A. (2019). Cardioprotective microRNAs: lessons from stem cell-derived exosomal microRNAs to treat cardiovascular disease. Atherosclerosis 285, 1–9. doi: 10.1016/j.atherosclerosis.2019.03.016
Moher, D., Shamseer, L., Clarke, M., Ghersi, D., Liberati, A., Petticrew, M., et al. (2015). Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015 statement. Syst. Rev. 4:1. doi: 10.1186/2046-4053-4-1
Moss, A. J., Hall, W. J., Cannom, D. S., Daubert, J. P., Higgins, S. L., Klein, H., et al. (1996). Improved survival with an implanted defibrillator in patients with coronary disease at high risk for ventricular arrhythmia. Multicenter automatic defibrillator implantation trial investigators. N. Engl. J. Med. 335, 1933–1940. doi: 10.1056/NEJM199612263352601
Myhre, P. L., O'Meara, E., Claggett, B. L., de Denus, S., Jarolim, P., Anand, I. S., et al. (2018). Cardiac troponin I and risk of cardiac events in patients with heart failure and preserved ejection fraction. Circ. Heart Fail. 11:e005312. doi: 10.1161/CIRCHEARTFAILURE.118.005312
Olivieri, F., Antonicelli, R., Lorenzi, M., D'Alessandra, Y., Lazzarini, R., Santini, G., et al. (2013). Diagnostic potential of circulating miR-499-5p in elderly patients with acute non ST-elevation myocardial infarction. Int. J. Cardiol. 167, 531–536. doi: 10.1016/j.ijcard.2012.01.075
Peng, L., Chun-guang, Q., Bei-fang, L., Xue-zhi, D., Zi-hao, W., Yun-fu, L., et al. (2014). Clinical impact of circulating miR-133, miR-1291 and miR-663b in plasma of patients with acute myocardial infarction. Diagn. Pathol. 9:89. doi: 10.1186/1746-1596-9-89
Saxena, S., Gupta, A., Shukla, V., and Rani, V. (2018). Functional annotation of differentially expressed fetal cardiac microRNA targets: implication for microRNA-based cardiovascular therapeutics. 3 Biotech 8:494. doi: 10.1007/s13205-018-1520-8
Shalaby, S. M., El-Shal, A. S., Shoukry, A., Khedr, M. H., and Abdelraheim, N. (2016). Serum miRNA-499 and miRNA-210: a potential role in early diagnosis of acute coronary syndrome. IUBMB Life 68, 673–682. doi: 10.1002/iub.1529
Vallabhajosyula, S., Sakhuja, A., Geske, J. B., Kumar, M., Poterucha, J. T., Kashyap, R., et al. (2017). Role of admission troponin-T and serial troponin-T testing in predicting outcomes in severe sepsis and septic shock. J. Am. Heart Assoc. 6:5930. doi: 10.1161/JAHA.117.005930
Wang, F., Long, G., Zhao, C., Li, H., Chaugai, S., Wang, Y., et al. (2013). Plasma microRNA-133a is a new marker for both acute myocardial infarction and underlying coronary artery stenosis. J. Transl. Med. 11:222. doi: 10.1186/1479-5876-11-222
Wang, F., Long, G., Zhao, C., Li, H., Chaugai, S., Wang, Y., et al. (2014). Atherosclerosis-related circulating miRNAs as novel and sensitive predictors for acute myocardial infarction. PLoS ONE 9:e105734. doi: 10.1371/journal.pone.0105734
Wang, G. K., Zhu, J. Q., Zhang, J. T., Li, Q., Li, Y., He, J., et al. (2010). Circulating microRNA: a novel potential biomarker for early diagnosis of acute myocardial infarction in humans. Eur. Heart J. 31, 659–666. doi: 10.1093/eurheartj/ehq013
Wang, K. J., Zhao, X., Liu, Y. Z., Zeng, Q. T., Mao, X. B., Li, S. N., et al. (2016). Circulating MiR-19b-3p, MiR-134-5p and MiR-186-5p are promising novel biomarkers for early diagnosis of acute myocardial infarction. Cell. Physiol. Biochem. 38, 1015–1029. doi: 10.1159/000443053
Wang, R., Li, N., Zhang, Y., Ran, Y., and Pu, J. (2011). Circulating microRNAs are promising novel biomarkers of acute myocardial infarction. Intern. Med. 50, 1789–1795. doi: 10.2169/internalmedicine.50.5129
Wang, Y., Chang, W., Zhang, Y., Zhang, L., Ding, H., Qi, H., et al. (2019). Circulating miR-22-5p and miR-122-5p are promising novel biomarkers for diagnosis of acute myocardial infarction. J. Cell. Physiol. 234, 4778–4786. doi: 10.1002/jcp.27274
Whiting, P. F., Rutjes, A. W., Westwood, M. E., Mallett, S., Deeks, J. J., Reitsma, J. B., et al. (2011). QUADAS-2: a revised tool for the quality assessment of diagnostic accuracy studies. Ann. Intern. Med. 155, 529–536. doi: 10.7326/0003-4819-155-8-201110180-00009
Wu, A. H., and Ford, L. (1999). Release of cardiac troponin in acute coronary syndromes: ischemia or necrosis. Clin. Chim. Acta 284, 161–174. doi: 10.1016/s0009-8981(99)00078-9
Xiao, J., Shen, B., Li, J., Lv, D., Zhao, Y., Wang, F., et al. (2014). Serum microRNA-499 and microRNA-208a as biomarkers of acute myocardial infarction. Int. J. Clin. Exp. Med. 7, 136–141.
Xue, S., Liu, D., Zhu, W., Su, Z., Zhang, L., Zhou, C., et al. (2019a). Circulating MiR-17-5p, MiR-126-5p and MiR-145-3p are novel biomarkers for diagnosis of acute myocardial infarction. Front. Physiol. 10:123. doi: 10.3389/fphys.2019.00123
Xue, S., Zhu, W., Liu, D., Su, Z., Zhang, L., Chang, Q., et al. (2019b). Circulating miR-26a-1, miR-146a and miR-199a-1 are potential candidate biomarkers for acute myocardial infarction. Mol. Med. 25:18. doi: 10.1186/s10020-019-0086-1
Yang, S., Fu, C., Xu, R., Xun, Z., Zhao, X., and Fang, R. (2017). Serum microRNA-302b: the novel biomarker for diagnosis of acute myocardial infarction. Br. J. Biomed. Sci. 74, 214–216. doi: 10.1080/09674845.2017.1333665
Yang, S. Y., Wang, Y. Q., Gao, H. M., Wang, B., and He, Q. (2016). The clinical value of circulating miR-99a in plasma of patients with acute myocardial infarction. Eur. Rev. Med. Pharmacol. Sci. 20, 5193–5197.
Yao, X. L., Lu, X. L., Yan, C. Y., Wan, Q. L., Cheng, G. C., and Li, Y. M. (2015). Circulating miR-122-5p as a potential novel biomarker for diagnosis of acute myocardial infarction. Int. J. Clin. Exp. Pathol. 8, 16014–16019.
Yeh, R. W., Sidney, S., Chandra, M., Sorel, M., Selby, J. V., and Go, A. S. (2010). Population trends in the incidence and outcomes of acute myocardial infarction. N. Engl. J. Med. 362, 2155–2165. doi: 10.1056/NEJMoa0908610
Yi, J., and An, Y. (2018). Circulating miR-379 as a potential novel biomarker for diagnosis of acute myocardial infarction. Eur. Rev. Med. Pharmacol. Sci. 22, 540–546. doi: 10.26355/eurrev_201801_14207
Zhang, J., Li, Y., and Zhao, Q. (2018). Circulating miR-23b as a novel biomarker for early risk stratification after st-elevation myocardial infarction. Med. Sci. Monit. 24, 1517–1523. doi: 10.12659/msm.908060
Zhang, L., Chen, X., Su, T., Li, H., Huang, Q., Wu, D., et al. (2015). Circulating miR-499 are novel and sensitive biomarker of acute myocardial infarction. J. Thorac. Dis. 7, 303–308. doi: 10.3978/j.issn.2072-1439.2015.02.05
Zhang, R., Lan, C., Pei, H., Duan, G., Huang, L., and Li, L. (2015). Expression of circulating miR-486 and miR-150 in patients with acute myocardial infarction. BMC Cardiovasc. Disord. 15:51. doi: 10.1186/s12872-015-0042-0
Zhang, Y., Liu, Y. J., Liu, T., Zhang, H., and Yang, S. J. (2016). Plasma microRNA-21 is a potential diagnostic biomarker of acute myocardial infarction. Eur. Rev. Med. Pharmacol. Sci. 20, 323–329.
Zhao, C. H., Cheng, G. C., He, R. L., Hong, Y., Wan, Q. L., Wang, Z. Z., et al. (2015). Analysis and clinical significance of microRNA-499 expression levels in serum of patients with acute myocardial infarction. Genet. Mol. Res. 14, 4027–4034. doi: 10.4238/2015.April.27.17
Zhao, J., Yu, H., Yan, P., Zhou, X., Wang, Y., and Yao, Y. (2019). Circulating MicroRNA-499 as a diagnostic biomarker for acute myocardial infarction: a meta-analysis. Dis. Markers 2019:6121696. doi: 10.1155/2019/6121696
Zhao, Y., Zhou, L., and Tang, Z. (2013). Cleavage-based signal amplification of RNA. Nat. Commun. 4:1493. doi: 10.1038/ncomms2492
Zhu, J., Yao, K., Wang, Q., Guo, J., Shi, H., Ma, L., et al. (2016). Circulating miR-181a as a potential novel biomarker for diagnosis of acute myocardial infarction. Cell. Physiol. Biochem. 40, 1591–1602. doi: 10.1159/000453209
Zile, M. R., Mehurg, S. M., Arroyo, J. E., Stroud, R. E., DeSantis, S. M., and Spinale, F. G. (2011). Relationship between the temporal profile of plasma microRNA and left ventricular remodeling in patients after myocardial infarction. Circ. Cardiovasc. Genet. 4, 614–619. doi: 10.1161/CIRCGENETICS.111.959841
Keywords: miRNAs, acute myocardial infarction, diagnosis, biomarker, meta-analysis
Citation: Zhai C, Li R, Hou K, Chen J, Alzogool M, Hu Y, Zhang J, Zhang Y, Wang L, Zhang R and Cong H (2020) Value of Blood-Based microRNAs in the Diagnosis of Acute Myocardial Infarction: A Systematic Review and Meta-Analysis. Front. Physiol. 11:691. doi: 10.3389/fphys.2020.00691
Received: 26 February 2020; Accepted: 27 May 2020;
Published: 14 August 2020.
Edited by:
Johannes Van Lieshout, University of Amsterdam, NetherlandsReviewed by:
Alessandro Capucci, Marche Polytechnic University, ItalyXu Yan, Victoria University, Australia
Copyright © 2020 Zhai, Li, Hou, Chen, Alzogool, Hu, Zhang, Zhang, Wang, Zhang and Cong. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: HongLiang Cong, hl_cong@126.com