 Patricia Borges dos Santos*
Patricia Borges dos Santos* Larissa Nascimento Gertrudes
Larissa Nascimento Gertrudes Flavia Lucia ConceiçãoBruno Moulin de AndradeDenise Pires de Carvalho
Flavia Lucia ConceiçãoBruno Moulin de AndradeDenise Pires de Carvalho Mario Vaisman
Mario Vaisman Patricia de Fatima dos Santos Teixeira
Patricia de Fatima dos Santos Teixeira- Post Graduation Program in Endocrinology, Medicine School, Federal University of Rio de Janeiro, Rio de Janeiro, Brazil
Objectives: To evaluate the impact of metformin (MTF) use on TSH levels, thyroid volume and volume of benign thyroid nodules (TNs). Additionally, to study if iodine status influences the outcomes.
Methods: A total of 23 euthyroid patients (42 TNs) with benign thyroid nodules, diagnosed by fine needle aspiration biopsy, were randomly assigned to MTF or placebo (P) use for 6 months. Serum TSH, homeostatic model assessment for insulin resistance (HOMA-IR), and urinary iodine concentrations (UIC) were assessed. Ultrasound was used to evaluate TNs and thyroid volumes (TV) and their variations throughout the study. Diabetic patients, those undergoing levothyroxine replacement, and/or using thyroid- or insulin level-influencing drugs were excluded.
Results: The sample consisted predominantly of patients without IR. Both intervention groups were similar regarding several confounding variables and showed a comparable median UIC. Serum TSH decreased significantly after MTF (−0.21 vs. 0.09 mUI/L in the P group; p = 0.015). At 6 months, no significant variations were found between groups with respect to TN volumes, TV, HOMA-IR, or body mass index (BMI). However, a tendency toward enlargement of TV with placebo (16.0%; p = 0.09) and a protective effect of MTF on growing TN (OR: 0.25; CI 0.05–1.20) was detected after excluding patients with IR (a lower UIC subgroup). The reduction on TSH levels with MTF maintained in the population without iodine insufficiency (−0.24 vs. +0.07 in the P group; p = 0.046) and was accentuated in those with excessive or more than adequate UIC (−0.69; p = 0.043). A protective effect of MTF on growing TN was suggested (OR: 0.11; IC: 0.02–0.84) in those with higher UIC.
Conclusions: This study demonstrated that MTF caused a reduction in TSH levels in benign nodular goiter. This effect was more accentuated in patients with higher levels of UIC and was accompanied by a suggested protective effect on TN enlargement.
Introduction
Thyroid nodules (TNs) are routinely found in worldwide clinical practices and are detected in up to 50 to 60% of subjects (1). However, even though fine needle aspiration biopsy (FNAB) confirms it's benign diagnosis in up to 75% of cases, a subgroup that might grow over time and sometimes requiring thyroidectomy (1). Identifying which type of benign TNs are at risk of developing this outcome and discovering the possibility of non-surgical strategies or drugs that could stop this evolution has been the subject of worldwide research.
Insulin is one of the hallmarks in the pathogenesis of thyroid growth since it stimulates thyrocyte proliferation similar to thyroid-stimulating hormone (TSH). It has been demonstrated that patients with insulin resistance (IR) and high serum levels of insulin might have large thyroid volumes and a higher prevalence of thyroid nodules (2, 3). An association between IR and differentiated thyroid carcinoma has already been demonstrated (4, 5).
Metformin (MTF), which improves peripheral insulin sensitivity and is commonly used to treat type 2 diabetes, has been studied with respect to decreasing thyroid volume and nodule size in subjects with IR (6–10) and might be a potential antitumor drug (11) The mechanism of its action can be attributed to its growth-inhibitory effect via insulin/insulin-like growth factor (IGF) signaling and AMP-activated protein kinase/mammalian target of rapamycin (AMPK/mTOR) pathway (11). A meta-analysis confirmed that MTF can also be associated with low levels of serum TSH in IR patients (12). The exact mechanism has not been completely elucidated, but it might involve inhibitory effects on the AMPK system in the hypothalamus (12).
Over recent years, various publications have focused on the effects of MTF on nodular volume and TSH levels in patients with IR (6–10, 12–19). However, there are insufficient data in the literature evaluating whether these effects can also be observed in patients without IR. Furthermore, no study has evaluated whether or not the presence of other goitrogenic factors influences, such as iodine insufficiency, the response to MTF on nodular goiter volume or serum TSH.
In the present study, we hypothesized that metformin use can exert some influence over enlargement of thyroid volume (TV) and of benign TNs over time and also reduces serum TSH levels. We evaluated the relationships between iodine status and metformin treatment on variations of TV and benign TN volumes.
Subjects and Methods
Patients with previous diagnosis of benign thyroid nodule (BTN) disease, confirmed by FNAB, were recruited from the outpatient clinic of Clementino Fraga Filho University Hospital of Federal University of Rio de Janeiro (UFRJ). All patients were >18 years and gave their written, informed consent to the researcher. The protocol was approved by the Institutional Ethical Committee (CAAE:35585214.0.0000.5257), and the study was registered at ClinicalTrial.gov (NCT03183752). An interview was conducted to assess inclusion and exclusion criteria before the patient was selected for the study. At the time of this interview, a new ultrasound was performed to reevaluate the specific ultrasound pattern of BTN since only those showing solid or predominantly solid formations were included in the study.
The exclusion criteria consisted of several parameters: (1) pregnancy; (2) diabetes (diagnosed before or during the study); (3) acromegaly; (4) hepatic or cardiac insufficiency; (5) creatinine levels >1.4 mg/dL: and (6) any previous use of MTF. We also excluded patients who were receiving levothyroxine, corticoids, or any weight loss medication in the past 6 months. Previous radioiodine treatment was also considered an exclusion criterion, as was MTF intolerance to doses <1.0 g/day during follow-up.
After initial evaluation and baseline assessment of studied parameters, the patients were randomized into two intervention groups. Randomization was done by blocks, comprising four patients each, in a double-blinded manner. Similar tablets containing MTF or placebo were precisely counted and given to each patient. All patients were instructed to initially take 1 MTF tablet/day (500 mg/tablet); however, patients were instructed to take MTF with a weekly increment until reaching 3 tablets/day. All patients returned after 2 months for biochemical assessments (creatinine levels) and evaluation of adherence to the study protocol. A physician not blinded and not enrolled in the ultrasound and clinical/laboratory evaluations, was responsible for this assessment. A blinded physician performed a new ultrasound after 6 months of follow-up (the same one who had assessed baseline ultrasound pattern). However, this researcher was also blinded to the first ultrasonography parameters and also to the intervention group to which the patient was allocated.
Throughout the study, patients who were already on drugs (corticoids, weight loss medications, diabetes drugs), which could influence serum insulin levels, were excluded. Patients not adhering to the filled criteria of the protocol were also excluded. No adherence to the protocol was assumed when there was a return of >20% of the total tablets for the period.
All participants underwent thyroid ultrasonography, specific anamnesis, and clinical and laboratory assessment in the first evaluation and after 6 months of follow-up.
Anthropometric Measurements
Participants were weighed and measured without shoes or cap. Waist circumference (WC) was measured with a folding tape at natural waistline (the level of the umbilical). Body mass index (BMI) was calculated by means of the following formula: BMI = weight/height2.
Thyroid Morphology
All ultrasonographic evaluations were performed by the same physician, using a high-frequency SIEMENS-AUSONX X300 multifrequency transducer (12 MHz). TV and TN volume were calculated by the formula: length × width × thickness ×0.52 of each lobe and the isthmus. A TN was considered to have growth if it showed an increase in its volume throughout the time by >10%. Additionally, a reduction of >10% was necessary to assume that a TN had shrunk. Variations in TV were also considered only when occurred by >10%.
Laboratory Assessments
Serum samples were obtained by venipuncture after 8 h fasting and included TSH, glucose, insulin for HOMA-IR calculation, lipid profile and thyroid peroxidase antibody (TPO-Ab).
Serum levels of TSH and anti-thyroid peroxidase antibodies (TPO-Ab) were determined by immunochemiluminesce (Immulite, Diagnostic Products, Los Angeles, CA). Reference ranges for TSH were 0.4–4.0 μUI/mL, and TPO-Ab >35 UI/mL was considered positive. The intra-assay coefficients of variation were 3.8–12.5% and 4.3–5.6% for TSH and TPO-Ab, respectively while the inter-assay coefficients of variation were 4.6–12.5% and 7.8–10.5%, respectively. Glucose was assayed by hexoquinase (ADVIA Chemistry, Siemens). The reference range for glucose was based on the guidelines of the American Diabetes Association (ADA) and the Brazilian Diabetes Society (SBD). Insulin levels were measured using the Chemiluminescence Imunoassay Kit (ADVIA Centauro, Siemens) with reference ranges 3.0–25 μU/ml. The intra- and inter-assay coefficients of variation were 3.2–4.6% and 2.6–5.9%, respectively. HOMA-IR was calculated with the formula (Fasting plasma insulin [IU/ml] × fasting plasma glucose [nmol/L])/22.5. IR was considered when HOMA-IR >2.7 (20).
Spot urine samples were obtained from each participant for assessing urinary iodine concentration (UIC) that was determined by Inductively Coupled Plasma Mass Spectrometry (ICP-MS-Spectroquant® Iodine Test–Merch KGaA, Germany). The manufacturer's reference range was 26 to 705 μg/L. The classification of adequate iodine status was made according to the World Health Organization (WHO) for adults (100 to 199 mcg/L) (21).
Statistical Analysis
SPSS software (version 21.0 for windows; SPSS Inc., Chicago, IL, USA) was used for statistical analysis. Continuous variables were expressed as medians (interquartile range [IQ]) or median (minimum–maximum values) and compared between two independent groups using the Mann-Whitney test. Categorical variables were described as frequencies and compared between groups using the chi-squared or Fisher's exact test. The Wilcoxon test was used for paired analysis in order to detect significant variations in each intervention group.
Results
Twenty-eight individuals with benign TNs agreed to participate in this prospective study. Most patients had more than one TN; therefore, a total of 47 TNs were initially evaluated at the beginning of the prospective study. Patients were randomized into two groups: (1) 14 patients (24 TNs) receiving placebo (P) and (2) 14 patients (23 TNs) receiving metformin (MTF). Five patients were excluded because of lack adherence to the protocol or for not attending the 6 month evaluation: 1 patient from the P group (1 TN) and 4 patients from MTF group (4 TNs). Figure 1 shows the flowchart of the study participants.
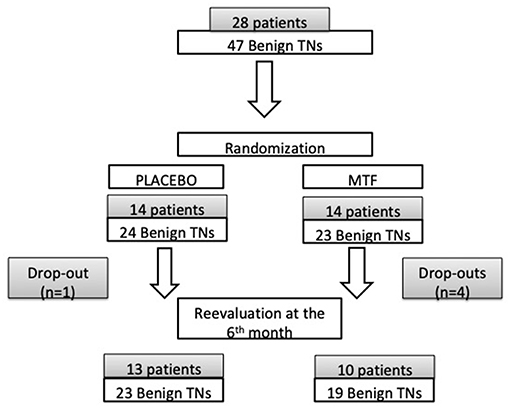
Figure 1. Flowchart of participants in the study.
A total of 42 nodules were monitored for 6 months (23 in P group and 19 in MTF group). Comparisons of baseline characteristics between groups showed that the two groups were similar at the moment of randomization and maintained this similarity at the end of the study with respect to the studied variables of interest (Table 1). The median UIC also did not differ between groups and showed a high frequency of excessive or more than adequate iodine status among participants, according to the WHO criteria (21) as shown in Table 1. Finally, the majority did not have any metabolic syndrome according to National Cholesterol Education Program (NCEP) criteria (22) or IR according to the Brazilian Metabolic Syndrome Study (BRAMS) (20).
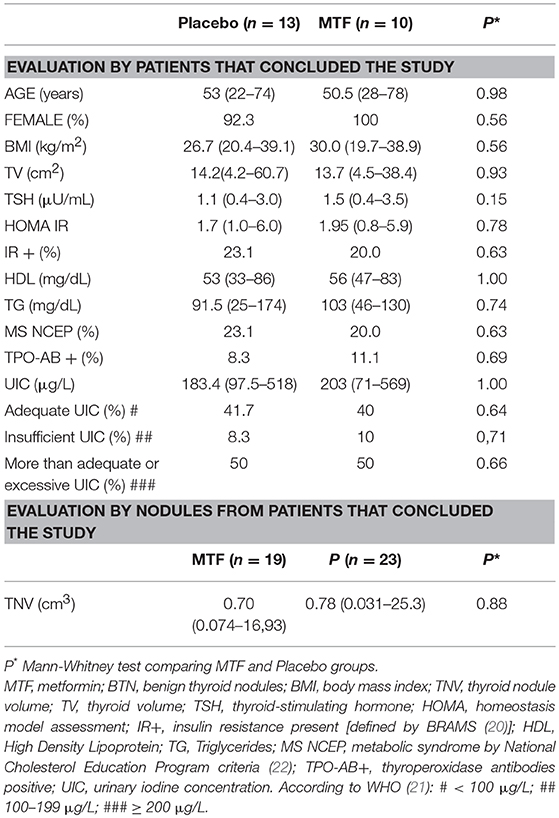
Table 1. Baseline characteristics of interesting variables between the studied groups.
After 6 months, serum TSH was significantly reduced in patients using MTF (−0.21 vs. 0.09 mUI/L in the P group; p = 0.015) as shown in Table 2. This pattern of reduction of serum TSH with MTF also occurred after excluding those five patients with IR; however, a borderline statistical significance (−0.21 vs. 0.10; p = 0.10) as shown in Table 2 was noted. Considering the outcomes of the entire group, there were no statistically significant variations in TN volume, TV, HOMA-IR, or BMI in each intervention group. Moreover, there were no significant differences in the variations between groups. However, tendencies for enlargement of benign nodular goiter (BNG) with placebo (16% from baseline TV; p = 0.093) and for a protective effect of MTF on growing TNs (OR: 0.25; IC:0.05–1.20) when those patients with IR were excluded from analysis were detected as shown in Table 2.
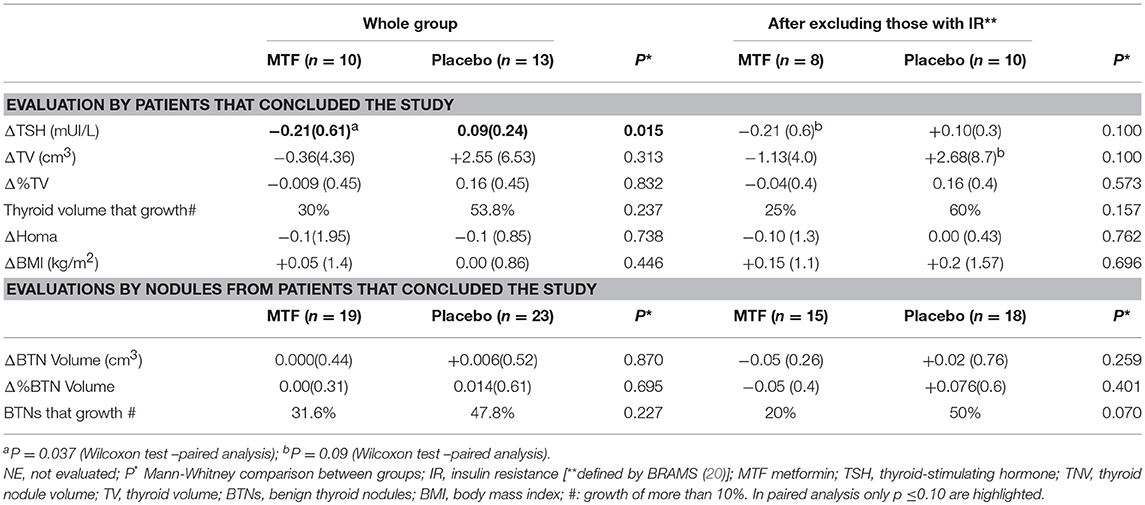
Table 2. Comparisons between outcome variables in MTF and Placebo groups during the study.
In this subgroup of nodules (with IR), a lower median UIC was observed compared to the remainder of the group (139 [119] vs. 207 [206]; p < 0.01) in addition to a higher frequency of iodine insufficiency (33.3 vs. 6.7%; p = 0.07).
A stratified analysis by iodine status showed that the reduction in serum TSH levels with MTF was maintained in the population without iodine insufficiency (−0.24 vs. +0.07 in the P group; p = 0.046) and was accentuated in those with excessive or more than adequate UIC (−0.69; p = 0.043) as demonstrated in Table 3. A protective effect of MTF on growing TN was also suggested (OR: 0.11; IC: 0.02–0.84) in those with higher UIC.
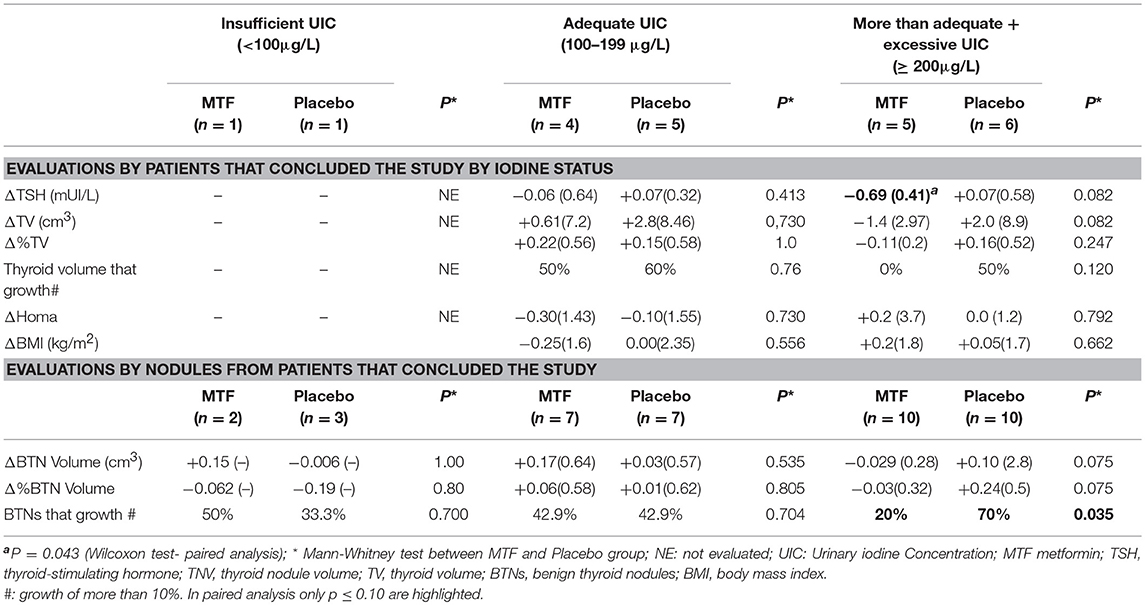
Table 3. Stratified analysis by iodine status: comparisons between outcome variables in MTF and Placebo groups during the study.
The median baseline TSH in the groups with adequate, insufficient, or excessive/more than adequate iodine status were similar (1.5, 1.8, and 1.4 μU/L, respectively; p = 0.764).
Discussion
In this study, 6 months of MTF therapy caused a reduction in TSH levels in euthyroid subjects without significant BMI reduction. These are significant data since it might be one of the diverse postulated mechanisms through which MTF could reduce thyroid and benign TN volumes. Some studies have already suggested that MTF therapy is associated with a reduction in TSH levels, but the majority of them evaluated patients with overt or subclinical hypothyroidism, and all of them evaluated only patients with diabetes or IR (7–10, 12–19). A meta-analysis, including seven studies in which changes in TSH levels in patients receiving MTF were evaluated, showed a reduction in TSH levels both in overt and in subclinical hypothyroidism but with no change in euthyroid patients (12). Moreover, in a double-blinded placebo-control clinical trial, MTF treatment was associated with a decrease in TSH levels only in patients with TSH >2.5 μU/mL (8). A preliminary study demonstrated that MTF administration in subjects with IR was associated with significant reduction in TSH levels and increase in levels of free tri-iodothyronine (FT3) with no change in free tetra-iodothyronine (FT4) (7). In a study with elderly people with type 2 diabetes, the patients with diabetes who were given MTF had lower TSH levels compared to non-diabetic patients in addition to patients treated with other antidiabetic agents (13).
Mechanisms by which MTF lowers TSH levels are still being debated. Some hypotheses mention a change in the affinity and/or quantity of thyroid receptors, an increase in central dopaminergic tone, or a direct effect on TSH regulation, thereby enhancing the effects of thyroid hormones in the pituitary gland (14, 15). The central effects of metformin on TRH/TSH regulation might involve the AMPK system. MTF decreases hepatic gluconeogenesis via AMPK activation; otherwise, its activity is inhibited in the hypothalamus and possibly enhances the inhibition of thyroid hormones on the pituitary gland (12).
It is well-known that TSH and insulin are involved in thyrocyte proliferation, and several studies have reported that patients with insulin resistance might have large thyroid volumes and a higher prevalence of TNs (2, 3). Therefore, the reduction of TSH and HOMA-IR after MTF treatment could be causative factors for TN volume reduction. However, contrary to previous studies, the current work revealed no impact of MTF on HOMA-IR. The principal hypothesis that has been suggested to explain these results is the small selected sample, which consisted of predominantly patients without IR. The low levels of baseline HOMA-IR make it difficult to find a significant decrease in this index throughout the study period. In summary, the effect of variations on this index caused by MTF might be weakened. Reanalyzing data after excluding patients with IR, an increase in BNG volume with placebo was detected; however with a borderline p-value. The evaluation of this small group with IR showed an association with iodine insufficiency that might blunt BNG volume response to MTF.
Iodine deficiency is a well-known risk factor for nodular thyroid disease. Additionally, lower UIC has been found among patients with diabetes and obesity compared to control subjects, and urinary iodine was shown to be negatively correlated with glucose, insulin levels, and HOMA-IR (23–26). Therefore, hypothesizing that iodine status could characterize a selection bias and could exert some influence on the effect of MTF on thyroid; we assessed UIC from the participants in our study. This was a differential approach, in comparison to studies from other researchers. Rezzónico et al. (6) and Karimifar et al. (8) did not assess UIC in their study; however, they reported previous studies that involved that participants residing in an iodine-sufficient area. Anil et al. (7) did not report UIC in their study participants. The median of UIC indicates that our sample did not have an insufficient or excessive iodine status according to WHO criteria (21); however, a high frequency of excessive/more than adequate UIC was found in accordance with previously reported studies from the same country (27, 28).
In the present study, the stratified analysis, by iodine status, showed that the MTF effects were more evident in the subgroup with higher UIC. We speculate that in this sample the reduction of serum TSH by MTF was important for preventing BNG growth since excessive UIC has been associated with higher levels of serum TSH and subclinical hypothyroidism in previous studies from the same region (28, 29). We could not prove this hypothesis since we did not demonstrate different TSH levels according to iodine status. Other possible hypothesis might be related to pro-inflammatory factors that were not measured in the present study but could be potentially associated with excessive iodine status; several studies have reported that high iodine intake is one of environmental factors implied in Hashimoto thyroiditis pathogenesis (30, 31).
MTF has diverse antitumor effects not solely related to reduction of insulin resistance. The insulin/insulin-like growth factor 1 (IGF-1) signaling pathway has long been known to promote cell proliferation and decrease apoptosis (32). Previous studies have shown the potential inhibitory effect of metformin on the growth of human thyroid cells (11). The potential antitumor effect of MTF is complex and multifactorial. Two distinct but not exclusive mechanisms can be implicated in this action. First, by decreasing insulinemia, MTF can exert an inhibitory effect via insulin/IGF-1 signaling (11). Second, MTF might also directly inhibit cell growth by multiple molecular pathways, including AMPK-dependent (mTOR) and AMPK-independent mechanisms (11, 33, 34). Other possible actions include an effect of MTF on tumor stem cells and the nuclear factor κB (NF-κB) pathway (33). Furthermore, a recent study reported that MTF could inhibit the secretion of CXCL8 stimulated by tumor necrosis factor-α (TNF-α) in primary cultures of normal thyroid cells and differentiated thyroid cancer cells (35).
Some studies have demonstrated that MTF, an insulin sensitizer, could help reduce TN volume. Rezzónico et al. (6) reported the effect of MTF on reduction in nodular size in patients with small benign TN and IR after 6 months of follow-up. Recently, two meta-analysis demonstrated a significant decrease in TN volume after MTF therapy by pooling the results of smaller studies (9, 10). Miao et al. (9) included seven studies with a total of 240 subjects and He et al. (10) included five studies with a total of 189 subjects. The time of follow-up in these studies ranged from 3 to 12 months. Anil et al. found that MTF therapy caused a significant decrease in TV and nodule size in patients with IR (7) although, the population of the study had obesity and had a significantly decreased BMI after diet and exercise was prescribed. Diet and exercise could have contributed to the reduction in HOMA-IR and thyroid and nodule volumes.
The present study has certain limitations. Our sample was small, which might have limited the statistical power of the analysis; however, this was also a limitation for other randomized controlled trials included in the meta-analysis (9, 10). Rezzónico et al. (6) evaluated 14 patients in MTF group (19 TNs), and Karimifar et al. (8) included 43 subjects in the MTF group (35 TNs). Our sample also had a few patients with IR, but to the best of our knowledge, it is the first time that the effect of MTF in TSH and TN volume was evaluated in patients without IR. Free thyroxine (FT4) was not assessed to evaluate if the reduction in TSH was accompanied by an increase in FT4. The follow-up time (6 months) might have been insufficient to observe a reduction in nodular goiter size; however, the follow-up period in the majority of studies included in the meta-analysis was 6 months. Only one study had a 1 year follow-up time (9, 10).
In conclusion, this study demonstrated that MTF caused a reduction in TSH levels in patients with BNG. This effect was more accentuated in patients with higher levels of UIC and was accompanied by a suggested protective effect on TN enlargement. Future studies with larger samples are necessary in order to evaluate the effect of MTF in benign thyroid nodules in a more detailed and conclusive manner.
Data Availability
The datasets generated for this study are available on request to the corresponding author.
Ethics Statement
This study was carried out in accordance with the recommendations of Ethical Committe of Clementino Fraga Filho University Hospital with written informed consent from all subjects. All subjects gave written informed consent in accordance with the Declaration of Helsinki. The protocol was approved by the Ethical Committe of Clementino Fraga Filho University Hospital (CAAE:35585214.0.0000.5257).
Author Contributions
PdS, PT, FC, MV, BdA, and DdC designed the study and discussed the results as well as providing contributions on writing and revising the manuscript. PT and PdS participated on final submission of the paper. BdA and LG organized the database. PdS, PT, and LG conducted the clinical trial and evaluated all patients during the study, collecting data, performing the ultrasounds and assessing laboratory data. PT and PdS analyzed and wrote the results.
Funding
This study was supported by Fundação Carlos Chagas Filho de Amparo à Pesquisa do Estado do Rio de Janeiro (FAPERJ) [grant n° E-26/203.286/2016] and Conselho Nacional de Pesquisa (CNPq) [grant universal n° 425031/2016-0 and productive in research n° 311761/2015-1].
Conflict of Interest Statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Acknowledgments
The authors would like to thank the Fundação Carlos Chagas Filho de Amparo à Pesquisa do Estado do Rio de Janeiro (FAPERJ) and Conselho Nacional de Pesquisa (CNPq), which encouraged this work.
Abbreviations
IR, insulin resistance; MTF, metformin; TN, thyroid nodule; TSH, thyroid stimulating hormone; TV, thyroid volume; AMPK, adenosine monophosphate-activated protein kinase; mTOR, mammalian target of rapamycin BTN, benign thyroid volume; BMI, body mass index; TPO-Ab, thyroid peroxidase antibody; UIC, Urinary Iodine Concentration; P, placebo; WHO, World Health Organization; BNG, benign nodular goiter; NF-κB, nuclear factor κB; TNF-α, tumor necrosis factor-α; FT4, tetra-iodothyronine.
References
1. Gharib H, Papini E, Garber JR, Duick DS, Harrell RM, Hegedüs L, et al. AACE/ACE/AME task force on thyroid nodules. American association of clinical endocrinologists, American college of endocrinology, and associazione medici endocrinologi medical guidelines for clinical practice for the diagnosis and management of thyroid nodules - 2016 Update. Endocr Pract. (2016) 22:622–39. doi: 10.4158/EP161208.GL
2. Rezzónico J, Rezzónico M, Pusiol E, Pitoia F, Niepomniszcze H. Introducing the thyroid gland as another victim of the insulin resistance syndrome. Thyroid. (2008) 18:461–64. doi: 10.1089/thy.2007.0223
3. Sousa PA, Vaiman M, Carneiro JR, Guimarães L, Freitas H, Pinheiro MF, et al. Prevalence of goiter and thyroid nodular disease in patients with class III obesity. Arq Bras Endocrinol Metabol. (2013) 57:120–5. doi: 10.1590/S0004-27302013000200004
4. Rezzónico JN, Rezzónico M, Pusiol E., Pitoia F, Niepomniszcze H. Increased prevalence of insulin resitance in patients with differentiated thyroid carcinoma. Metab Syndr Related Disord. (2009) 7:375–80. doi: 10.1089/met.2008.0062
5. Gursoy A. Rising thyroid cancer incidence in the world might be related to insulin resistance. Med Hypotheses. (2010) 74(1):35–6. doi: 10.1016/j.mehy.2009.08.021
6. Rezzónico J, Rezzónico M, Pusiol E, Pitoia F, Niepomniszcze H. Metformin treatment for small benign thyroid nodules in patients with insulin resistance. Metab Syndr Relat Disord. (2011) 9:69–75. doi: 10.1089/met.2010.0026
7. Anil C, Kut A, Atesagaoglu B, Nar A, Bascil Tutuncu N, Gursoy A. Metformin decreases thyroid volume and nodule size in subjects with insulin resistance: a preliminary study. Med Princ Pract. (2016) 25:233–6. doi: 10.1159/000442821
8. Karimifar M, Aminorroaya A, Amini M, Mirfendereski T, Iraj B, Feizi A, et al. Effect of metformin on thyroid stimulating hormone and thyroid volume in patients with prediabetes: a randomized placebo-controlled clinical trial. J Res Med Sci. (2014) 19:1019–26.
9. Miao S, Yuan Y, Huifeng Z, Hongjie D, Chao L, Yaofu F. Efficacy of Metformin for benign thyroid nodules in subjects with insulin resistance: a systematic review and meta-analysis. Front Endocrinol. (2018) 9: 494. doi: 10.3389/fendo.2018.00494
10. He X, Wu D, Hu C, Xu T, Liu Y, Liu C, et al. Role of Metformin in the treatment of patients with thyroid nodules and insulin resistance: a systematic review and metanalysis. Thyroid. (2019) 29:359–67. doi: 10.1089/thy.2017.0707
11. Chen G, Xu S, Renko K, Derwahl M. Metformin inhibits growth of thyroid carcinoma cells, suppresses self-renewal of derived cancer stem cells, and potentiates the effect of chemotherapeutic agents. J Clin Endocrinol Metab. (2012) 97:E510–20. doi: 10.1210/jc.2011-1754
12. Lupoli R, Di Minno A, Tortora A, Ambrosino P, Lupoli GA, Di Minno MN. Effects of treatment with metformin on TSH levels: a meta-analysis of literature studies. J Clin Endocrinol Metab. (2014) 99:E143–48. doi: 10.1210/jc.2013-2965
13. Fontes R, Teixeira Pde F, Vaisman M. Screening of undiagnosed hypothyroidism in elderey persons with diabetes according to age-specific reference intervals for serum thyroid stimulating hormone and the impact of antidiabetes drugs. J Diabetes Res. (2016) 2016: 1417408. doi: 10.1155/2016/1417408
14. Vigersky RA, Filmore-Nassar A, Glass AR: thyrotropin suppression by metformin. J Clin Endocrinol Metab. (2006) 9:225–7. doi: 10.1210/jc.2005-1210
15. Rotondi M, Cappelli C, Magri F, Botta R, Dionisio R, Iacobello C, et al. Thyroidal effect of metformin treatment in patients with polycystic ovary syndrome. Clin Endocrinol. (2011) 75:378–81. doi: 10.1111/j.1365-2265.2011.04042.x
16. Isidro ML, Penín MA, Nemiña R, Cordido F. Metformin reduces thyrotropin levels in obese, diabetic women with primary hypothyroidism on thyroxine replacement therapy. Endocrine. (2007) 32: 79–82. doi: 10.1007/s12020-007-9012-3
17. Cappelli C, Rotondi M, Pirola I, Agosti B, Gandossi E, Valentini U, et al. TSH-lowering effect of metformin in type 2 diabetic patients: differences between euthyroid, untreated hypothyroid, and euthyroid on L-T4 therapy patients. Diabetes Care. (2009) 32:1589–90. doi: 10.2337/dc09-0273
18. Morteza Taghavi S, Rokni H, Fatemi S. Metformin decreases thyrotropin in overweight women with polycystic ovarian syndrome and hypothyroidism. Diab Vasc Dis Res. (2011) 8:47–8. doi: 10.1177/1479164110391917
19. Cappelli C, Rotondi M, Pirola I, Agosti B, Formenti A, Zarra E, et al. Thyreotropin levels in diabetic patients on metformin treatment. Eur J Endocrinol. (2012) 167:261–5. doi: 10.1530/EJE-12-0225
20. Geloneze B, Vasques AC, Stabe CF, Pareja JC, Rosado LE, Queiroz EC, et al. HOMA1-IR and HOMA2-IR indexes in identifying insulin resistance and metabolic syndrome: Brazilian Metabolic Syndrome Study (BRAMS). Arq Bras Endocrinol Metab. (2009) 53:281–7. doi: 10.1590/S0004-27302009000200020
21. World Health Organization. Assessment of Iodine Deficiency Disorders and Monitoring Their Elimination: A Guide for Programme Managers, 3rd ed. Geneva: WHO Press (2007).
22. Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults. Executive summary of the third report of the national cholesterol education program (NCEP) expert panel on detection, evaluation, and treatment of high blood cholesterol in adults (adult treatment Panel III). JAMA. (2001) 285:2486–97. doi: 10.1001/jama.285.19.2486
23. Al-Attas OS, Al-Daghri NM, Alkharfy KM, Alokail MS, Al-Johani NJ, Abd-Alrahman SH, et al. Urinary iodine is associated with insulin resistance in subjects with diabetes mellitus type 2. Exp Clin Endocrinol Diabetes. (2012) 120:618–22. doi: 10.1055/s-0032-1323816
24. Eray E, Sari F, Ozdem S, Sari R. Relationship between thyroid volume and iodine, leptin, and adiponectin in obese women before and after weight loss. Med Princ Pract. (2011) 20:43–6. doi: 10.1159/000322075
25. Lecube A, Zafon C, Gromaz A, Fort JM, Caubet E, Baena JA, et al. Iodine deficiency is higher in morbid obesity in comparison with late after bariatric surgery and non-obese women. Obes Surg. (2015) 25:85–9. doi: 10.1007/s11695-014-1313-z
26. Malaguarnera R, Vella V, Nicolosi ML, Belfiore A. Insulin resistance: any role in the changing epidemiology of thyroid cancer? Front Endocrinol. (2017) 8:314. doi: 10.3389/fendo.2017.00314
27. Carvalho AL, Meirelles CJ, Oliveira LA, Costa TM, Navarro AM. Excessive iodine intake in schoolchildren. Eur J Nutr. (2012) 51:557–62. doi: 10.1007/s00394-011-0239-7
28. Corcino CM, Berbara TMBL, Saraiva DA, Morais NAOES, Schtscherbyna A, Gertrudes LN, et al. Variation of iodine status during pregnancy and its associations with thyroid function in women from Rio de Janeiro, Brazil. Public Health Nutr. (2019) 22:1232–40. doi: 10.1017/S1368980019000399
29. Camargo RY, Tominori EK, Neves SC, Rubio I, Galrão AL, Knobel M, et al. Thyroid and the environment: exposure to excessive nutritional iodine increases the prevalence of thyroid disorders in São Paulo, Brazil. Eur J Endocrinol. (2008) 159:293–9. doi: 10.1530/EJE-08-0192
30. Hu S, Rayman MP. Multiple nutritional factors and the risk of hashimoto's thyroiditis. Thyroid. (2017) 27:597–610. doi: 10.1089/thy.2016.0635
31. Duntas LH. Environmental factors and autoimmune thyroiditis. Nat Clin Pract Endocrinol Metabol. (2008) 4:454–60. doi: 10.1038/ncpendmet0896
32. Gong J, Kelekar G, Shen J, Shen J, Kaur S, Mita M. The expanding role of metformin in cancer: an update on antitumor mechanisms and clinical development. Target Oncol. (2016) 11:447–67. doi: 10.1007/s11523-016-0423-z
33. Coperchini F, Leporati P, Rotondi M, Chiovato L. Expanding the therapeutic spectrum of metformin: from diabetes to cancer. J Endocrinol Invest. (2015) 38:1047–55. doi: 10.1007/s40618-015-0370-z
34. Zhou G, Myers R, Li Y, Chen Y, Shen X, Fenyk-Melody J, et al. Role of AMP-activated protein kinase in mechanism of metformin action. J Clin Invest. (2001) 108:1167–74. doi: 10.1172/JCI13505
Keywords: benign thyroid nodule, thyroid nodules volume, thyroid volume, metformin, insulin resistance, TSH
Citation: dos Santos PB, Gertrudes LN, Conceição FL, de Andrade BM, Carvalho DP, Vaisman M and Teixeira PFS (2019) Effects of Metformin on TSH Levels and Benign Nodular Goiter Volume in Patients Without Insulin Resistance or Iodine Insufficiency. Front. Endocrinol. 10:465. doi: 10.3389/fendo.2019.00465
Received: 30 April 2019; Accepted: 26 June 2019;
Published: 17 July 2019.
Edited by:
Michele Marinò, University of Pisa, ItalyReviewed by:
Rosaria Maddalena Ruggeri, University of Messina, ItalyMario Rotondi, University of Pavia, Italy
Copyright © 2019 dos Santos, Gertrudes, Conceição, de Andrade, Carvalho, Vaisman and Teixeira. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Patricia Borges dos Santos, patriciaborges.endocrino@gmail.com