 Mohammad Abumayyaleh1,2*
Mohammad Abumayyaleh1,2* Iván J. Núñez Gil3
Iván J. Núñez Gil3 María C. Viana-LLamas4
María C. Viana-LLamas4 Sergio Raposeiras Roubin5
Sergio Raposeiras Roubin5 Rodolfo Romero6
Rodolfo Romero6 Emilio Alfonso-Rodríguez7
Emilio Alfonso-Rodríguez7 Aitor Uribarri8,9
Aitor Uribarri8,9 Gisela Feltes10
Gisela Feltes10 Víctor Manuel Becerra-Muñoz11
Víctor Manuel Becerra-Muñoz11 Francesco Santoro12
Francesco Santoro12 Martino Pepe13
Martino Pepe13 Alex Fernando Castro Mejía14Jaime Signes-Costa15
Alex Fernando Castro Mejía14Jaime Signes-Costa15 Adelina Gonzalez16
Adelina Gonzalez16 Francisco Marín17Javier López-País18Edoardo Manzone19
Francisco Marín17Javier López-País18Edoardo Manzone19 Olalla Vazquez Cancela20Carolina Espejo Paeres21Alvaro López Masjuan22Lazar Velicki23,24
Olalla Vazquez Cancela20Carolina Espejo Paeres21Alvaro López Masjuan22Lazar Velicki23,24 Christel Weiß25
Christel Weiß25 David Chipayo3Antonio Fernandez-Ortiz3
David Chipayo3Antonio Fernandez-Ortiz3 Ibrahim El-Battrawy1,2,26Ibrahim Akin1,2 HOPE COVID-19 investigators
Ibrahim El-Battrawy1,2,26Ibrahim Akin1,2 HOPE COVID-19 investigators- 1Department of Cardiology, Angiology, Haemostaseology and Medical Intensive Care, University Medical Center Mannheim, Medical Faculty Mannheim, Heidelberg University, Mannheim, Germany
- 2European Center for AngioScience (ECAS) and German Center for Cardiovascular Research (DZHK) partner site Heidelberg/Mannheim, Mannheim, Germany
- 3Hospital Clínico San Carlos, Universidad Complutense de Madrid, Instituto de Investigación, Sanitaria del Hospital Clínico San Carlos (IdISSC), Madrid, Spain
- 4Hospital Universitario Guadalajara, Guadalajara, Spain
- 5University Hospital Álvaro Cunqueiro, Vigo, Spain
- 6Hospital Universitario Getafe, Getafe, Universidad Europea, Madrid, Spain
- 7Hospital University of Bellvitge, Barcelona, Spain
- 8Cardiology Department, Vall d’Hebron University Hospital and Research Institute, Universitat Autonoma de Barcelona, Barcelona, Spain
- 9Centro de Investigacion Biomedica en Red para Enfermedades Cardiovasculares (CIBERCV), Madrid, Spain
- 10Hospital Nuestra Señora de América, Madrid, Spain
- 11Hospital Clinico Universitario Virgen de la Victoria, Malaga, Spain
- 12Department of Medical and Surgical Sciences, University of Foggia, Foggia, Italy
- 13Azienda Ospedaliero-Universitaria Consorziale Policlinico di Bari, Bari, Italy
- 14Hospital General del norte de Guayaquil IESS Los Ceibos, Guayaquil, Ecuador
- 15Hospital Clínico de Valencia, INCLIVA, Valencia, Spain
- 16Hospital Universitario Infanta Sofia, Madrid, Spain
- 17Hospital Clínico Universitario Virgen de la Arrixaca, Murcia, Spain
- 18Complejo Hospitalario Universitario de Ourense, Ourense, Spain
- 19Hospital del Sureste, Madrid, Spain
- 20Complejo Hospitalario Universitario de Santiago de Compostela, Santiago, Spain
- 21Hospital Universitario Príncipe de Asturias, Madrid, Spain
- 22Hospital Universitario Juan Ramón Jimenez, Huelva, Spain
- 23Faculty of Medicine, University of Novi Sad, Novi Sad, Serbia
- 24Institute of Cardiovascular Diseases Vojvodina, Sremska Kamenica, Serbia
- 25Department for Statistical Analysis, University Heidelberg, Mannheim, Germany
- 26Department of Cardiology and Angiology, Bergmannsheil University Hospitals, Ruhr University of Bochum, Bochum, Germany
Background: Diabetes mellitus (DM) is one of the most frequent comorbidities in patients suffering from severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) with a higher rate of severe course of coronavirus disease (COVID-19). However, data about post-COVID-19 syndrome (PCS) in patients with DM are limited.
Methods: This multicenter, propensity score-matched study compared long-term follow-up data about cardiovascular, neuropsychiatric, respiratory, gastrointestinal, and other symptoms in 8,719 patients with DM to those without DM. The 1:1 propensity score matching (PSM) according to age and sex resulted in 1,548 matched pairs.
Results: Diabetics and nondiabetics had a mean age of 72.6 ± 12.7 years old. At follow-up, cardiovascular symptoms such as dyspnea and increased resting heart rate occurred less in patients with DM (13.2% vs. 16.4%; p = 0.01) than those without DM (2.8% vs. 5.6%; p = 0.05), respectively. The incidence of newly diagnosed arterial hypertension was slightly lower in DM patients as compared to non-DM patients (0.5% vs. 1.6%; p = 0.18). Abnormal spirometry was observed more in patients with DM than those without DM (18.8% vs. 13; p = 0.24). Paranoia was diagnosed more frequently in patients with DM than in non-DM patients at follow-up time (4% vs. 1.2%; p = 0.009). The incidence of newly diagnosed renal insufficiency was higher in patients suffering from DM as compared to patients without DM (4.8% vs. 2.6%; p = 0.09). The rate of readmission was comparable in patients with and without DM (19.7% vs. 18.3%; p = 0.61). The reinfection rate with COVID-19 was comparable in both groups (2.9% in diabetics vs. 2.3% in nondiabetics; p = 0.55). Long-term mortality was higher in DM patients than in non-DM patients (33.9% vs. 29.1%; p = 0.005).
Conclusions: The mortality rate was higher in patients with DM type II as compared to those without DM. Readmission and reinfection rates with COVID-19 were comparable in both groups. The incidence of cardiovascular symptoms was higher in patients without DM.
Introduction
Coronavirus disease 2019 (COVID-19) is caused by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) and is associated with significant morbidity and mortality (1).
Among other related diseases such as arterial hypertension and obesity, diabetes mellitus (DM) is identified as a risk factor for the severe course of COVID-19, developing sepsis, and mortality (2–4).
In patients suffering from COVID-19, SARS-CoV-2 binds the angiotensin-converting enzyme 2 (ACE2) receptor and uses it as a potential target for viral interventions (5). In diabetic mice, the expression of ACE2 is increased as compared to mice without DM. In addition, patients who suffered from insufficient glycemic control showed worse outcomes, such as more complications and higher mortality rates (6). New-onset DM and metabolic complications in patients suffering from manifested DM with high doses of insulin have been revealed in COVID-19 (7, 8). Furthermore, uncontrolled glycemic levels in DM patients cause organ injury and may be exacerbated in patients suffering from COVID-19 (9).
The international Health Outcome Predictive Evaluation for COVID-19 (HOPE COVID-19) Registry was initiated to investigate comorbidity and mortality of COVID-19 (10). In the Health Outcome Predictive Evaluation for COVID-19 II (HOPE-II COVID-19) Registry, we investigated readmission, reinfection, vaccination rate, cardiovascular, neuropsychiatric, respiratory, gastrointestinal, and other symptoms in hospitalized patients suffering from COVID-19 and concomitant DM type II. Complications related to COVID-19 and long-term mortality were also systematically analyzed.
Material and methods
Study design and participants
HOPE-II COVID-19 (NCT04334291) is an international project at 55 international centers. It is designed as a retrospective and prospective cohort registry to investigate post-COVID-19 syndrome without any conflict of interest. We included hospitalized patients with a confirmed diagnosis of COVID-19. There are no exclusion criteria, except for the patient’s explicit refusal to participate. Initially, data on 8,828 hospitalized patients suffering from COVID-19 were collected until 30th September 2021. In this study, we excluded 56 patients due to age <18 and 53 patients with DM type I. Data from 8,719 consecutive patients with COVID-19 regarding their concomitant DM type II status were analyzed.
Ethics approval
This study was executed in compliance with the Declaration of Helsinki regarding human subjects, and the study was approved by the center ethics committee of Hospital Clinico San Carlos (Internal Code: 21/128-E) and, when needed, in all involved centers.
DM type II
DM type II was known and diagnosed by medical physicians. Data were collected from the patient’s medical records.
Post-COVID-19 syndrome
Patients suffering from post-COVID-19 syndrome describe new-onset symptoms following initial recovery from an acutely confirmed COVID-19 or ongoing from the initial illness. This condition occurs 3 months from the onset of COVID-19 with symptoms that last for at least 2 months and cannot be explained by an alternative diagnosis. Symptoms may also fluctuate or relapse over time (11).
Outcomes and follow-up
We described long-term mortality as a primary endpoint. Readmission, reinfection rate, respiratory complications, cardiovascular, neuropsychiatric, respiratory, gastrointestinal, and other symptoms as secondary endpoints were also evaluated. Follow-up for the overall population for mortality was 20 months (mean post-COVID-19; 2.6 ± 4.6).
Statistical analysis
Descriptive and comparative analyses were presented. Continuous variables were shown as mean ± standard deviation if the distribution was normal or median (min–max) if not. Categorical variables were presented as frequency rates and percentages. The Chi-square test was used for categorical variables for group comparisons. Quantitative variables were performed using the Mann–Whitney U test for nonparametric variables and the Student’s t-test for parametric variables, as verified by the Kolmogorov–Smirnov test. We applied a propensity score (PS)-based matching method to control for confounding baseline variables due to the nonrandomized nature of the study and the different participating centers. In a multivariable logistic regression test, hazard ratio (HR) with 95% confidence intervals (95% CI) was calculated for the determination of risk factors for the endpoint. Predictors of mortality were identified by univariate analysis. Predictors with p < 0.05 were analyzed by logistic multivariable regression. The multivariable regression test was used to investigate predictors of mortality, adjusting for all significant variables: age; male as sex; obesity; comorbidities such as arterial hypertension, dyslipidemia, DM type II, renal insufficiency, heart disease, cerebrovascular disease, liver disease, and cancer disease; immunosuppression; home oxygen therapy; premedication; symptomatic; clinical parameters such as peripheral oxygen saturation (SpO2) <92% and reduced blood pressure (systolic blood pressure <90 mmHg or diastolic blood pressure <60 mmHg); and laboratory parameters. p-value of <0.05 was recognized as statistically significant. Statistical analysis was performed with IBM SPSS Statistics version 27.
Results
Baseline characteristics and in-hospital complications
Data from 8,719 consecutive hospitalized patients (n = 1,578 with DM; n = 7,141 with non-DM) with confirmed COVID-19 were collected. The 1:1 propensity score matching (PSM) according to age and sex resulted in 1,548 matched pairs. The mean age of matched pairs was 72.6 ± 12.7 years old. Even more, the male sex was 63.5% in both groups. Diabetics suffered from more chronic conditions such as arterial hypertension (77.5% vs. 58.5%; p < 0.0001), renal insufficiency (13.6% vs. 8.1%; p < 0.0001), and liver disease (5.7% vs. 3.4%; p = 0.002). In-hospital complications were observed more in diabetics as compared to nondiabetics, for example, respiratory insufficiency (62.1% vs. 56.3%; p = 0.001), acute kidney injury (26.6% vs. 19.8%; p < 0.0001), and sepsis (15.4% vs. 12.8%, p = 0.04). Other baseline characteristics, immunosuppression, home oxygen therapy, premedication, symptomatic, clinical, and laboratory parameters, in-hospital complications, and intervention procedures during hospitalization are presented in Table 1.
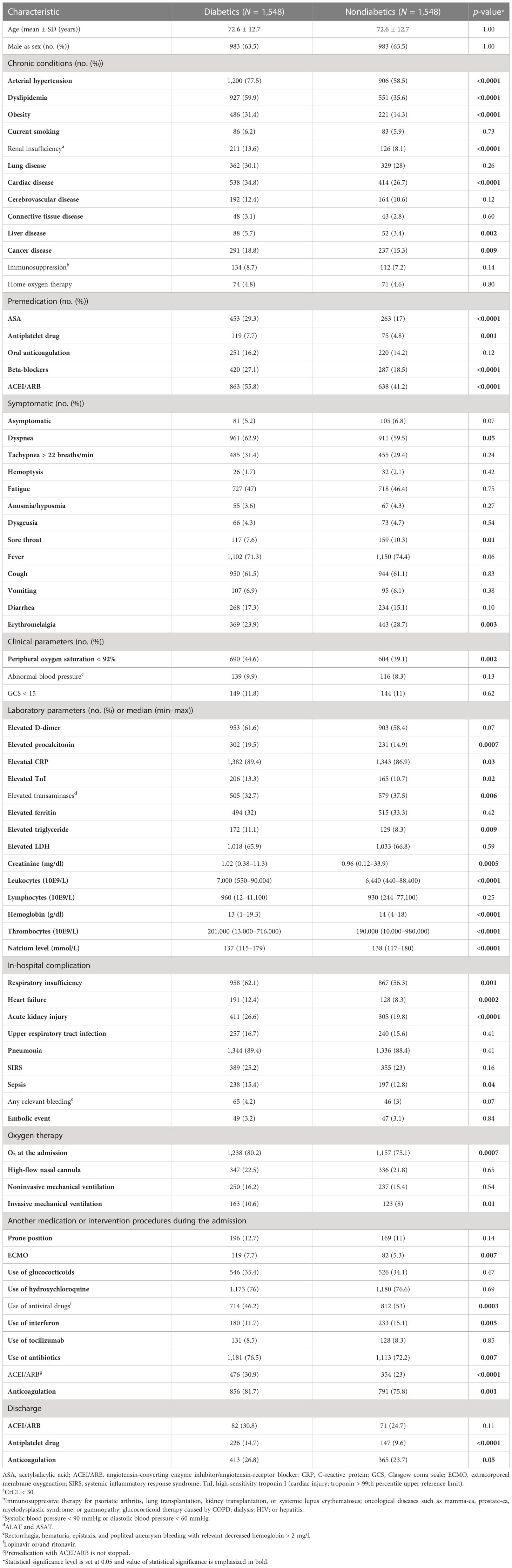
Table 1 Patients with diabetes mellitus type II as compared to patients without DM II, baseline characteristics, laboratory and radiographic findings, complications, and clinical outcomes.
Clinical outcomes at long-term follow-up
Mean follow-up (2.6 ± 4.6 months) data were available for 412 diabetics and 443 nondiabetics. The readmission rate due to any cause was similar in diabetics and nondiabetics, respectively (19.7% vs. 18.3%; p = 0.61). The reinfection rate with COVID-19 was also comparable in patients with DM than those without DM (2.9% vs. 2.3%; p = 0.55). Additionally, diabetics were vaccinated more than nondiabetics at follow-up with the same time to vaccination (11.9 ± 3.1 months in diabetics vs. 12.2 ± 2.9 months in nondiabetics) (57.3% vs. 51.7%; p = 0.10). At follow-up, cardiovascular symptoms such as dyspnea and an increase in resting heart rate after discharge occurred less frequently in patients suffering from DM (13.2% vs. 16.4%; p = 0.01) than those without DM (2.8% vs. 5.6%; p = 0.05), respectively. In addition, the mortality rate at the 20-month follow-up was significantly higher in DM than in non-DM patients (33.9% vs. 29.1%; p = 0.005). Cardiovascular, neuropsychiatric, respiratory, gastrointestinal, and other symptoms are presented in Table 2.
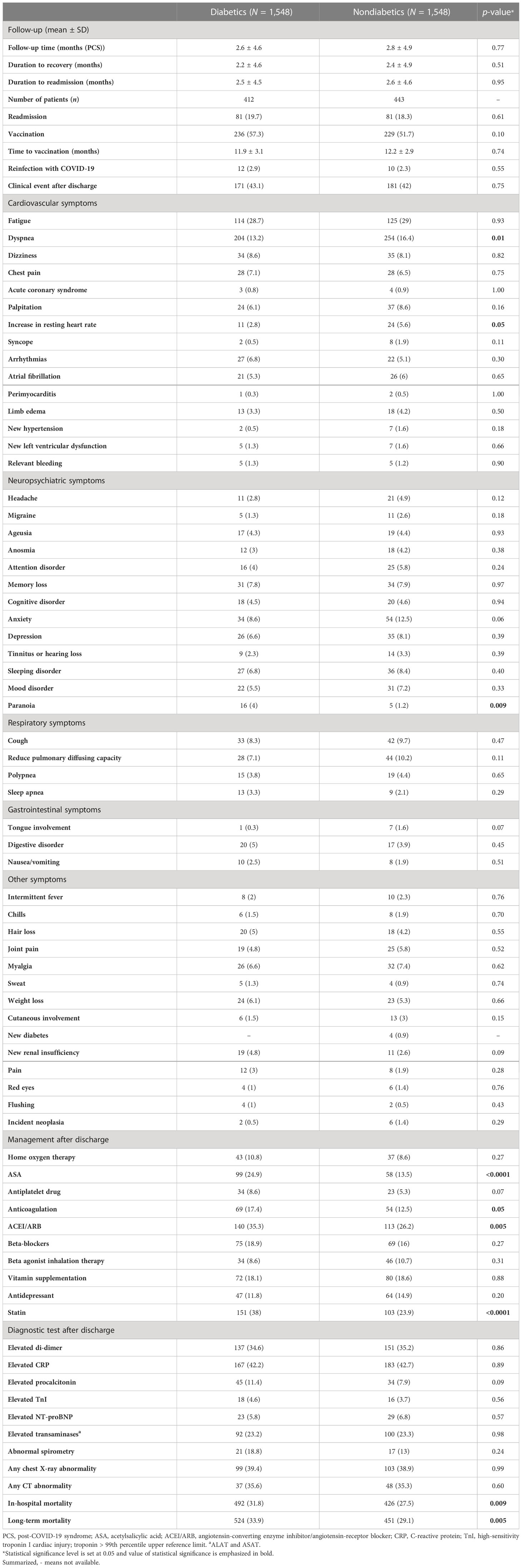
Table 2 Follow-up in patients suffering from DM type II as compared to those without DM.
PSM and predictors of mortality
The mortality rate at long-term follow-up was significantly higher in patients with DM than those without, in the overall cohort and in the matched cohort, respectively (p < 0.0001 and p = 0.005). The Kaplan–Meier curve with landmark analysis is displayed in Figure 1. In the multivariable analysis for mortality, age, and male sex were determined as predictors for mortality, respectively (HR: 2.34; p < 0.0001) (HRK 1.23; p = 0.008). Other predictors are performed in Table 3. Clinical outcomes before PSM are presented in the Supplementary Appendix.
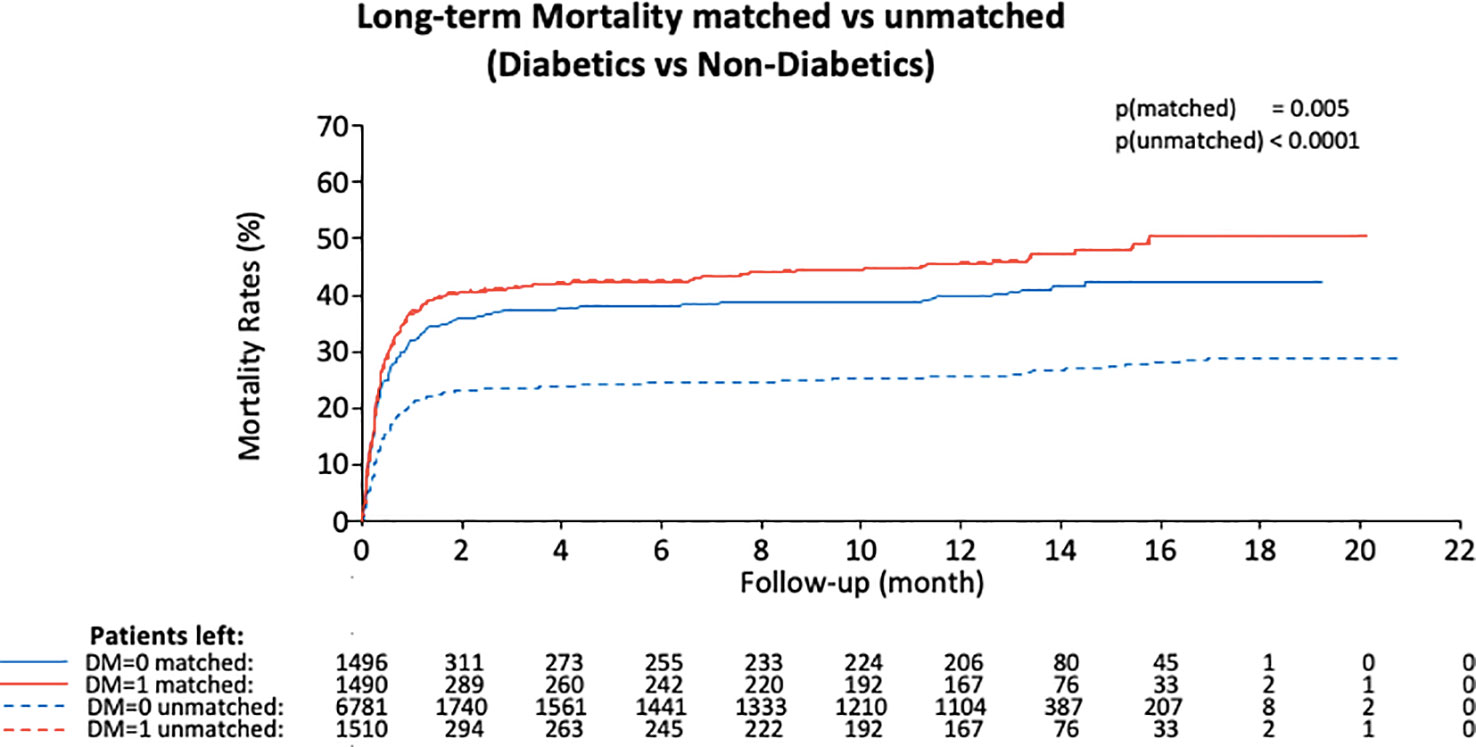
Figure 1 Kaplan–Meier curve for long-term mortality divided by diabetics vs. nondiabetics in the overall population and matched cohort. In both comparisons, a worse outcome in diabetics was detected.
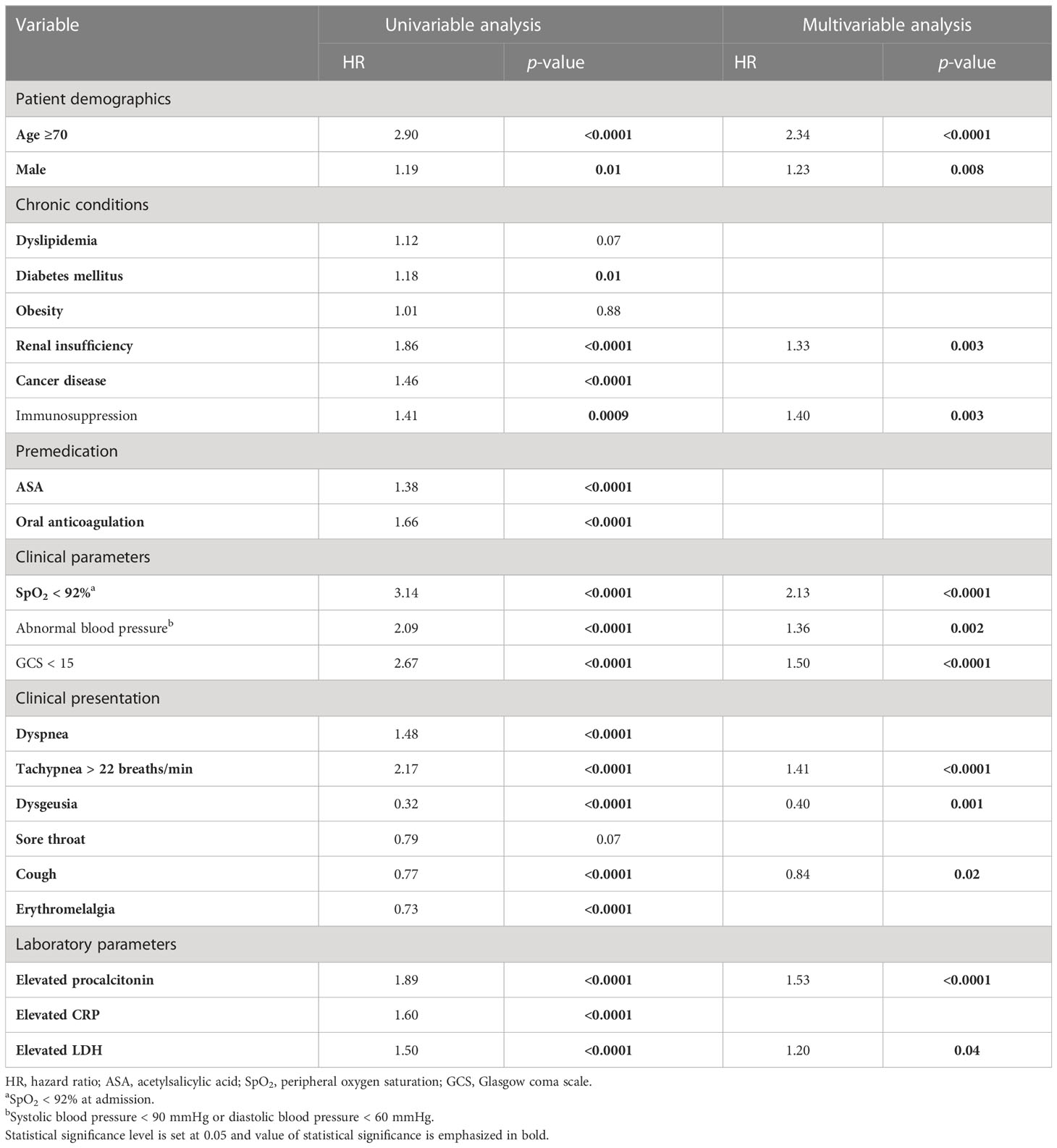
Table 3 Predictors of mortality, multivariable analysis.
Discussion
This study presents characteristics of PCS in patients suffering from DM as compared to those without DM. The main findings of this study are as follows: (1) readmission rate for any cause was similar in diabetics than nondiabetics at follow-up; (2) reinfection rate with COVID-19 was similar in both groups; (3) symptoms such as dyspnea and an increase of resting heart rate occurred less in diabetics as compared to nondiabetics; (4) The incidence of newly diagnosed arterial hypertension was less in diabetics than nondiabetics without statistical significance; (5) respiratory complications were revealed in diabetics and nondiabetics; and (5) long-term mortality was higher in patients suffering from DM as compared to those without DM.
Recently, it has been reported that the progression of type II DM is associated with increased insulin resistance accompanied by chronic inflammation and endothelial and ß-cell dysfunction (12). On the other hand, the inflammatory response in infected patients with SARS-CoV-2 may worsen insulin resistance and endothelial dysfunction (13). The existence of both diseases may further enhance the inflammation and decrease interferon levels, neutrophil chemotaxis, and T lymphocyte-mediated immune response with impairment of cytokine production (14–16). That is associated with a severe course of COVID-19 in DM patients. Furthermore, ACE2 expression increases insulin resistance. This receptor and dipeptidyl peptidase 4 (DPP4), which may be a factor in the severity of COVID-19 infection, are present in several physiological processes and are modulated by hyperglycemia and pharmacological therapies that are common in DM patients (17). In addition, chronic hyperglycemia leads to chronic vascular and kidney disease. Other comorbidities, such as obesity and hypertension, are present in concurrent DM. These diabetes-related comorbidities may negatively impact outcomes in DM patients with COVID-19 (18, 19).
DM as a risk factor for post-COVID-19 syndrome
Our DM cohort had more comorbidities such as arterial hypertension, renal insufficiency, liver disease, and cardiac disease than patients without DM. Furthermore, respiratory insufficiency requiring oxygen therapy and invasive mechanical ventilation (MV) was observed more in diabetics as compared to nondiabetics. During hospitalizations, sepsis and acute kidney injury occurred more often in diabetics than nondiabetics. A prospective study showed that the persistence of symptoms was associated with the severity of the disease at the beginning and that the intensive care unit (ICU) admission was an independent risk factor for PCS (20). In addition, the need for MV was determined as a predictor for the development of PCS (21). However, it has been reported that 60% of low-risk patients for mortality with COVID-19 suffered from severe PCS (22). In patients with DM, optimizing hyperglycemia therapy improve metabolic function which may be beneficial for the long-term management of patients with PCS (23). In this study, PCS was slightly comparable despite the different comorbidities and in-hospital complications in both groups.
Cardiovascular symptoms
In our study, dyspnea and an increase in resting heart rate occurred more significantly in nondiabetics as compared to diabetics. Additionally, newly diagnosed arterial hypertension was also revealed slightly more in nondiabetics than diabetics. Regarding that, the persistence of cardiovascular symptoms was recently reported (24). In one of the studies from Wuhan, Huang et al. showed that patients infected with SARS-CoV-2 suffered from acute cardiac injury (25). Subclinical myocarditis with an increased risk of arrhythmias may play a role in PCS (26). Data about the comparison between diabetics and nondiabetics are limited.
Neuropsychiatric symptoms
This study presented neuropsychiatric symptoms generally more common in nondiabetics as compared to diabetics without statistical significance, for example, headache, sleeping disorder, and anxiety. However, paranoia was observed significantly more in diabetics than nondiabetics at a 3-month follow-up. Studies reported that headache and other neuropsychiatric symptoms occurred after 3 months in patients infected with SARS-CoV-2 (27, 28). Guedj et al. reported that more areas in the brain showed hypometabolism in patients with PCS as compared to healthy subjects (29). Controlled, randomized studies are needed to investigate the neuropsychiatric symptoms in patients with DM as compared to those without DM.
Respiratory symptoms
Renal insufficiency and cardiac disease were observed more in patients with DM than non-DM, while the rate of lung diseases was similar in matched pairs. At follow-up, our data presented a similar rate of sleep apnea in diabetics and nondiabetics. Furthermore, computer tomography (CT) and chest X-ray abnormalities were revealed in both groups, but dyspnea occurred significantly more in nondiabetics as compared to diabetics at follow-up. In one retrospective study with 77 days of follow-up, spirometry (9.3%) and chest radiology (19%) abnormalities were detected in 277 patients, of whom 51% had PCS (30). In 22 patients after COVID-19-associated acute respiratory distress syndrome (ARDS), signs of lung fibrosis were detected in 55% of patients at 3-month follow-up (31). In patients with critical COVID-19, 9.5% of patients needed home oxygen therapy after discharge at a 1-year follow-up (32). Furthermore, DM was identified as a risk factor for the requirement of oxygen therapy in patients suffering from COVID-19 (33). In our multivariable analysis, DM was not identified as a predictor for mortality.
This study has some limitations. It has a retrospective character; not all laboratory tests were done on all patients. Furthermore, data on hemoglobin A1c (HbA1c), antihyperglycemic treatment including metformin and DPP-4 inhibitors, and statin therapy at baseline are missing. A strength of our study is the sample size of patients with COVID-19 and concomitant DM type II at 55 international centers. The results are therefore real-world evidence.
To summarize, PCS was observed in diabetics and nondiabetics. However, the mortality rate was higher in diabetics as compared to nondiabetics. DM was not determined as a risk factor for mortality at follow-up.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
This study was executed in compliance with the Declaration of Helsinki regarding in human subjects and the study was approved by the center Ethics Committee of Hospital Clinico San Carlos (Internal Code: 21/128-E) and, when needed, in all involved centers. Written informed consent for participation was not required for this study in accordance with the national legislation and the institutional requirements.
Author contributions
MA, IG, IE-B, and IA made substantial contributions to the study’s concept and design. All authors obtained ethical approval. Data were collected by MA, IG, MV-L, SR, RR, EA-R, AU, GF, VB-M, FS, MP, AM, JS-C, AG, FM, JL-P, EM, OC, CP, AM, LV, DC, AF-O, MA, and CW analyzed all the data. CW supported the descriptive statistics. IJNG and IA approved the statistical analysis. MA, IG, IE-B, and IA prepared the manuscript. All authors contributed to the article and approved the submission version.
Funding
Nonconditioned grant (Fundación Interhospitalaria para la Investigación cardiovascular, FIC, Madrid, Spain). This nonprofit institution had no role in the study design; collection, analysis, or interpretation of data; in the writing of the report; or in the decision to submit the paper for publication.
Acknowledgments
The authors thank all HOPE-II researchers.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fendo.2023.1167087/full#supplementary-material
References
1. Nunez-Gil IJ, Fernandez-Perez C, Estrada V, Becerra-Munoz VM, El-Battrawy I, Uribarri A, et al. Mortality risk assessment in spain and italy, insights of the hope covid-19 registry. Intern Emerg Med (2021) 16(4):957–66. doi: 10.1007/s11739-020-02543-5
2. El-Battrawy I, Nunez-Gil IJ, Abumayyaleh M, Estrada V, Manuel Becerra-Munoz V, Uribarri A, et al. Covid-19 and the impact of arterial hypertension-an analysis of the international hope covid-19 registry (italy-spain-germany). Eur J Clin Invest (2021) 51(11):e13582. doi: 10.1111/eci.13582
3. Abumayyaleh M, Nunez-Gil IJ, El-Battrawy I, Estrada V, Becerra-Munoz VM, Uribarri A, et al. Sepsis of patients infected by sars-cov-2: real-world experience from the international hope-covid-19-registry and validation of hope sepsis score. Front Med (Lausanne) (2021) 8:728102. doi: 10.3389/fmed.2021.728102
4. Abumayyaleh M, Nunez Gil IJ, El-Battrawy I, Estrada V, Becerra-Munoz VM, Aparisi A, et al. Does there exist an obesity paradox in covid-19? insights of the international hope-covid-19-registry. Obes Res Clin Pract (2021) 15(3):275–80. doi: 10.1016/j.orcp.2021.02.008
5. Hoffmann M, Kleine-Weber H, Schroeder S, Kruger N, Herrler T, Erichsen S, et al. Sars-cov-2 cell entry depends on ace2 and tmprss2 and is blocked by a clinically proven protease inhibitor. Cell (2020) 181(2):271–280.e278. doi: 10.1016/j.cell.2020.02.052
6. Mader JK, Brix J, Aberer F, Vonbank A, Resl M, Pieber TR, et al. [hospital diabetes management (update 2019)]. Wien Klin Wochenschr (2019) 131(Suppl 1):200–11. doi: 10.1007/s00508-019-1447-z
7. Ren H, Yang Y, Wang F, Yan Y, Shi X, Dong K, et al. Association of the insulin resistance marker tyg index with the severity and mortality of covid-19. Cardiovasc Diabetol (2020) 19(1):58. doi: 10.1186/s12933-020-01035-2
8. Chee YJ, Ng SJH, Yeoh E. Diabetic ketoacidosis precipitated by covid-19 in a patient with newly diagnosed diabetes mellitus. Diabetes Res Clin Pract (2020) 164:108166. doi: 10.1016/j.diabres.2020.108166
9. Mrigpuri P, Sonal S, Spalgais S, Goel N, Menon B, Kumar R. Uncontrolled diabetes mellitus: a risk factor for post covid fibrosis. Monaldi Arch Chest Dis (2021) 91(1). doi: 10.4081/monaldi.2021.1607
10. Nunez-Gil IJ, Estrada V, Fernandez-Perez C, Feltes G, Vedia O, Vergara-Uzcategui CE, et al. Health outcome predictive evaluation for covid 19 international registry (hope covid-19), rationale and design. Contemp Clin Trials Commun (2020) 20:100654. doi: 10.1016/j.conctc.2020.100654
11. Soriano JB, Murthy S, Marshall JC, Relan P, Diaz and WHOCCDWGoP-C- Condition JV. A clinical case definition of post-covid-19 condition by a delphi consensus. Lancet Infect Dis (2022) 22(4):e102–7. doi: 10.1016/S1473-3099(21)00703-9
12. Schwarz PEH, Timpel P, Harst L, Greaves CJ, Ali MK, Lambert J, et al. Blood sugar regulation for cardiovascular health promotion and disease prevention: jacc health promotion series. J Am Coll Cardiol (2018) 72(15):1829–44. doi: 10.1016/j.jacc.2018.07.081
13. Bornstein SR, Rubino F, Ludwig B, Rietzsch H, Schwarz PEH, Rodionov RN, et al. Consequences of the covid-19 pandemic for patients with metabolic diseases. Nat Metab (2021) 3(3):289–92. doi: 10.1038/s42255-021-00358-y
14. Berbudi A, Rahmadika N, Tjahjadi and R Ruslami AI. Type 2 diabetes and its impact on the immune system. Curr Diabetes Rev (2020) 16(5):442–9.
15. Hodgson K, Morris J, Bridson T, Govan B, Rush and N Ketheesan C. Immunological mechanisms contributing to the double burden of diabetes and intracellular bacterial infections. Immunology (2015) 144(2):171–85. doi: 10.1111/imm.12394
16. Santos A, Magro DO, Evangelista-Poderoso and MJA Saad R. Diabetes, obesity, and insulin resistance in covid-19: molecular interrelationship and therapeutic implications. Diabetol Metab Syndr (2021) 13(1):23. doi: 10.1186/s13098-021-00639-2
17. Drucker DJ. Coronavirus infections and type 2 diabetes-shared pathways with therapeutic implications. Endocr Rev (2020) 41(3). doi: 10.1210/endrev/bnaa011
18. Yan Y, Yang Y, Wang F, Ren H, Zhang S, Shi X, et al. Clinical characteristics and outcomes of patients with severe covid-19 with diabetes. BMJ Open Diabetes Res Care (2020) 8(1). doi: 10.1136/bmjdrc-2020-001343
19. Zhu L, She ZG, Cheng X, Qin JJ, Zhang XJ, Cai J, et al. Association of blood glucose control and outcomes in patients with covid-19 and pre-existing type 2 diabetes. Cell Metab (2020) 31(6):1068–1077.e1063. doi: 10.1016/j.cmet.2020.04.021
20. Peghin M, Palese A, Venturini M, De Martino M, Gerussi V, Graziano E, et al. Post-covid-19 symptoms 6 months after acute infection among hospitalized and non-hospitalized patients. Clin Microbiol Infect (2021) 27(10):1507–13. doi: 10.1016/j.cmi.2021.05.033
21. Michelen M, Manoharan L, Elkheir N, Cheng V, Dagens A, Hastie C, et al. Characterising long covid: a living systematic review. BMJ Glob Health (2021) 6(9). doi: 10.1136/bmjgh-2021-005427
22. Dennis A, Wamil M, Alberts J, Oben J, Cuthbertson DJ, Wootton D, et al. Multiorgan impairment in low-risk individuals with post-covid-19 syndrome: a prospective, community-based study. BMJ Open (2021) 11(3):e048391. doi: 10.1136/bmjopen-2020-048391
23. Khunti K, Davies MJ, Kosiborod and MA Nauck MN. Long covid - metabolic risk factors and novel therapeutic management. Nat Rev Endocrinol (2021) 17(7):379–80. doi: 10.1038/s41574-021-00495-0
24. Carvalho-Schneider C, Laurent E, Lemaignen A, Beaufils E, Bourbao-Tournois C, Laribi S, et al. Follow-up of adults with noncritical covid-19 two months after symptom onset. Clin Microbiol Infect (2021) 27(2):258–63. doi: 10.1016/j.cmi.2020.09.052
25. Huang C, Wang Y, Li X, Ren L, Zhao J, Hu Y, et al. Clinical features of patients infected with 2019 novel coronavirus in wuhan, china. Lancet (2020) 395(10223):497–506. doi: 10.1016/S0140-6736(20)30183-5
26. Maron BJ, Udelson JE, Bonow RO, Nishimura RA, Ackerman MJ, Estes NA 3rd, et al. Eligibility and disqualification recommendations for competitive athletes with cardiovascular abnormalities: task force 3: hypertrophic cardiomyopathy, arrhythmogenic right ventricular cardiomyopathy and other cardiomyopathies, and myocarditis: a scientific statement from the american heart association and american college of cardiology. Circulation (2015) 132(22):e273–280. doi: 10.1161/CIR.0000000000000239
27. Goertz YMJ, Van Herck M, Delbressine JM, Vaes AW, Meys R, Machado FVC, et al. Persistent symptoms 3 months after a sars-cov-2 infection: the post-covid-19 syndrome? ERJ Open Res (2020) 6(4). doi: 10.1183/23120541.00542-2020
28. Wijeratne T, Crewther S. Post-covid 19 neurological syndrome (pcns); a novel syndrome with challenges for the global neurology community. J Neurol Sci (2020) 419:117179. doi: 10.1016/j.jns.2020.117179
29. Guedj E, Campion JY, Dudouet P, Kaphan E, Bregeon F, Tissot-Dupont H, et al. (18)f-fdg brain pet hypometabolism in patients with long covid. Eur J Nucl Med Mol Imaging (2021) 48(9):2823–33. doi: 10.1007/s00259-021-05215-4
30. Moreno-Perez O, Merino E, Leon-Ramirez JM, Andres M, Ramos JM, Arenas-Jimenez J, et al. Post-acute covid-19 syndrome. incidence and risk factors: a mediterranean cohort study. J Infect (2021) 82(3):378–83.
31. Truffaut L, Demey L, Bruyneel AV, Roman A, Alard S, De Vos N, et al. Post-discharge critical covid-19 lung function related to severity of radiologic lung involvement at admission. Respir Res (2021) 22(1):29. doi: 10.1186/s12931-021-01625-y
32. Gribensk A, Schneider A, Gallaher JR, Reid TS, Kindell DG, Charles AG, et al. Posthospitalization outcomes after extracorporeal membrane oxygenation (ecmo) for covid-19. Surgery (2022) 172(1):466–9. doi: 10.1016/j.surg.2022.01.044
Keywords: diabetes mellitus, post-COVID-19 syndrome, SARS-CoV-2, respiratory complications, reinfection, vaccination rate, long-term mortality
Citation: Abumayyaleh M, Núñez Gil IJ, Viana-LLamas MC, Raposeiras Roubin S, Romero R, Alfonso-Rodríguez E, Uribarri A, Feltes G, Becerra-Muñoz VM, Santoro F, Pepe M, Castro Mejía AF, Signes-Costa J, Gonzalez A, Marín F, López-País J, Manzone E, Vazquez Cancela O, Paeres CE, Masjuan AL, Velicki L, Weiß C, Chipayo D, Fernandez-Ortiz A, El-Battrawy I, Akin I and HOPE COVID-19 investigators (2023) Post-COVID-19 syndrome and diabetes mellitus: a propensity-matched analysis of the International HOPE-II COVID-19 Registry. Front. Endocrinol. 14:1167087. doi: 10.3389/fendo.2023.1167087
Received: 15 February 2023; Accepted: 27 April 2023;
Published: 16 May 2023.
Edited by:
Pranav Kumar Prabhakar, Lovely Professional University, IndiaReviewed by:
Sawai Singh Rathore, Dr. Sampurnanand Medical College, IndiaEvgeny Shlyakhto, Almazov National Medical Research Centre, Russia
Copyright © 2023 Abumayyaleh, Núñez Gil, Viana-LLamas, Raposeiras Roubin, Romero, Alfonso-Rodríguez, Uribarri, Feltes, Becerra-Muñoz, Santoro, Pepe, Castro Mejía, Signes-Costa, Gonzalez, Marín, López-País, Manzone, Vazquez Cancela, Paeres, Masjuan, Velicki, Weiß, Chipayo, Fernandez-Ortiz, El-Battrawy, Akin, HOPE COVID-19 investigators. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Mohammad Abumayyaleh, mohammad.abumayyaleh@medma.uni-heidelberg.de