 Yoon-Hee Cha
Yoon-Hee Cha Yong Yan Cui
Yong Yan Cui Robert W. Baloh4
Robert W. Baloh4
- 1Laureate Institute for Brain Research, Tulsa, OK, United States
- 2School of Community Medicine, University of Tulsa, Tulsa, OK, United States
- 3Department of Internal Medicine, Columbia Medical Center, New York, NY, United States
- 4Department of Neurology, David Geffen School of Medicine, University of California, Los Angeles, Los Angeles, CA, United States
Background: There has been increasing awareness that post-motion triggered rocking self-vertigo can last for months or years, a disorder known as Mal de Debarquement Syndrome (MdDS). A similar feeling of oscillating self-motion can occur without a motion trigger in some individuals, leading to controversy about whether motion triggered (MT) and non-motion triggered (non-MT) symptoms ultimately represent the same disorder. Recognizing the similarities and differences between MT and non-MT MdDS can prevent unnecessary diagnostic testing and lead to earlier and more effective treatments.
Methods: Standardized questionnaire assessment and follow-up interviews of individuals with persistent MT or non-MT MdDS (>1 month) examined at a University Dizziness Clinic.
Findings: Questionnaires were available on 80 individuals with persistent MT MdDS and 42 with non-MT MdDS. Sex distribution (81% female) and age of onset (mean 43.4 ± 12.2 years MT; 42.1 ± 15.2 years non-MT) were comparable between MT and non-MT MdDS (p > 0.05). Mean duration of illness was significantly longer in the non-MT group (82.8 ± 64.2 months) than the MT group (35.4 ± 46.4 months) (p < 0.001). There was no correlation between trigger type and age of onset or duration of illness for MT MdDS. Improvement with re-exposure to motion (driving) was typical for both (MT = 89%, non-MT = 64%), but non-MT individuals more frequently had symptoms exacerbated with motion (MT = 0%; non-MT = 10%). Peri-menstrual and menstrual worsening of symptoms was typical in both MT and non-MT MdDS (each 71%). Both MT and non-MT MdDS exhibited a higher population baseline prevalence of migraine (23% and 38%, respectively). Benzodiazepines and SSRI/SNRIs were helpful in both subtypes of MdDS (>50% individuals with a positive response). Physical therapy was modestly helpful in the MT (56%) subtype but not in non-MT (15%). Vestibular therapy made as many individuals worse as better in MT and none improved in the non-MT group.
Conclusion: General demographic characteristics and exacerbating factors are similar in MT and non-MT MdDS, but there are differences in the duration of illness, effect of motion on symptoms, and response to therapy. Recognizing clinical features of MdDS subtypes may allow for better tailoring of therapy and potentially serve as classification criteria for new clinical designations.
Introduction
Historical references to the phenomenon of landsickness date back to the seventeenth century, but recognition of a clinical entity characterized by prolonged landsickness, “Mal de Debarquement Syndrome,” (MdDS), has only occurred in the second half of the twentieth century (1–5). The post-motion triggered feeling of “rocking” as if one was “still on the boat,” that follows sea, air, or land-based motion is a common experience in otherwise healthy individuals, occurring with a prevalence of about 70% (6–10). These short bouts of motion triggered (MT) symptoms last for two or fewer days and are referred to as “landsickness.” In some cases, however, the symptoms can persist for months or years, putting the syndrome into the category of MdDS (11, 12).
The International Classification of Vestibular Disorders defined vertigo as the “sensation of self-motion when no self-motion is occurring or the sensation of distorted self-motion during an otherwise normal head movement.” In this broad sense, the experience of MdDS is a form of vertigo (13). However, it is not vertigo in the intuitive sense of a perception of rotation. MdDS vertigo is oscillating or periodic and is present at rest without head movement. It is described as a rocking, bobbing, or swaying sensation and never as spinning (3, 14).
Recognition of MdDS as a clinical entity appears to be limited. A typical patient with MdDS sees over a dozen health care providers before arriving at a diagnosis (12, 15). The burden of illness of MdDS has been measured as being comparable to multiple sclerosis and as expensive as migraine (15). There are no clinical tests like brain imaging or vestibular function testing that can diagnose MdDS, as these are overwhelmingly normal (11, 16). MdDS has typically been diagnosed by the appropriate clinical history of oscillating vertigo, i.e., rocking, bobbing, swaying, that starts after a motion trigger has ended. Most cases are reported to improve temporarily with re-exposure to passive motion, such as driving a car or getting back on the boat. In this regard, it should not be confused with motion sickness in which the predominant symptom is nausea which occurs during the motion exposure itself (17, 18).
Caring for patients with MdDS represents a challenge for both primary care providers and vestibular specialists because of limited awareness of the spectrum of clinical features that comprise this syndrome as well as the paucity of treatment options. Dizziness and vertigo in general are such common symptoms that clinically distinct though less prevalent disorders such as MdDS might be unrecognized or be considered as “atypical” variants of more common entities such as Meniere’s disease or benign paroxysmal positional vertigo (BPPV) (19–22). Therefore, recognition of the core clinical features of MdDS is critical for diagnosis. When the classical history of rocking vertigo that starts after exposure to passive motion is encountered in a patient, the need for extensive structural brain and inner ear testing is of low yield (16, 21). Moreover, efficient diagnosis and treatment can be critical in reducing the development of co-morbid mood or anxiety disorders and social stigma in MdDS (23).
Over the course of many years of seeing patients with MdDS and performing clinical trials in MdDS, a database of patients and research participants in MdDS studies was created at the University of California, Los Angeles. We had first sampled this database to report on clinical features of MdDS in 2008 and again in 2013 with respect to the association between MdDS and migraine (16, 24). Since then, we have added additional participants as well as obtained data on more nuanced features of the disorder, such as the effect of hormonal cycles, body position, past psychiatric illness diagnoses, circumstances surrounding the onset of MdDS, and effect on employment. These clinical features are provided in this study along with additional data on the efficacy of therapies that individuals with MdDS had tried in the course of their clinical care.
We use two designations for MdDS in this study. Classical motion triggered MdDS, which we refer to as “MT” here, will be defined by the onset of rocking vertigo within 48-h of disembarking from a moving vessel, be it water, air, or land-based motion. Rocking vertigo can start without a motion trigger, however. These patients have presented a unique challenge, since they share nearly all of the features of classical MdDS from the patients’ experience standpoint, but present without an identified motion trigger. In the past, these individuals have been referred to as “mixed” MdDS, since they often have a prior history of MT MdDS, or as “spontaneous” MdDS to denote the non-motion triggered (non-MT) onset (12, 16). Whether non-MT rocking vertigo, which we refer to as “non-MT,” is fundamentally different from MT feelings of rocking vertigo is not known. However, there have been suggestions that the association with migraine and response to certain therapeutic maneuvers may be different in the two entities (16, 24, 25). Therefore, the designation of non-MT MdDS appears to be due to factors other than simple recall bias of a triggering event.
In our current assessment of individuals with MdDS, we have included both MT and non-MT variants in order to present a spectrum of how rocking vertigo may present to either the primary care physician or specialist. Detailed clinical features that may serve as risk factor identification or that may lead to disease sub-typing are presented. Greater recognition of the spectrum of MdDS may guide initial treatment and referral decisions.
Materials and Methods
The study was carried out in accordance with the approval and recommendations of the UCLA School of Medicine Medical IRB #3. Participants gave written informed consent in accordance with the Declaration of Helsinki (26). Outpatient visits to the neurotology clinic that had been tabulated in a clinical database since 1985 were reviewed for patients with a diagnosis of MdDS.
Criteria for the diagnosis of MdDS included the following: In the case of MT MdDS, criteria included the experience of persistent rocking vertigo that started within 48-h of disembarking from a water, air, or land-based vessel and that lasted at least 1-month. In the case of non-MT MdDS, symptoms had to start without any significant travel within the month before the onset. Significant travel was defined as passive motion exposure lasting at least 2 h. This duration was chosen because it is a length of time that is outside of normal exposures that would likely be experienced by the participant during their daily activities.
Since we were examining the clinical spectrum of rocking vertigo, we did not make restrictions on alleviating or exacerbating factors, such as the effect on re-exposure to passive motion. MT and non-MT were designated strictly on the identification of a proximate motion trigger. All participants in this study had been previously diagnosed with MdDS by an experienced neurotologist (RWB or YHC), without any other cause for symptoms determined after appropriate testing for peripheral or central vestibular dysfunction.
A standardized questionnaire packet and consent form was mailed to the most recent address on file for the participant with a stamped return envelope included. If no response was received within 2 months, a second packet was sent. Each packet contained a consent form to be returned with the questionnaire as well as a “do not wish to participate” card that could be returned to stop any future contact from the study. Therefore, all data tabulated in this study were from individuals who provided written informed consent.
Individuals who had consented to participate were contacted by phone if any answer on a questionnaire was ambiguous. However, not all participants with incomplete data could be contacted. Responses were scored if they were clear and unambiguous, so different numbers of responses were available for each set of questions. All percentages were rounded to the nearest whole number.
Statistics
The following statistical analyses were performed: (1) for continuous variables, such as age, a two sample t-test of means with a two-tailed p-value threshold of 0.05 for significance; (2) for categorical variables with more than five counts, a Chi-squared test; (3) for categorical variables with less than five counts, a Fisher’s exact test; (4) for age of onset and duration for MT MdDS, a one-way ANOVA with a post hoc correction for significance; and (5) for the effect of activities on symptoms, we converted responses of “better,” “same,” and “worse” into percentages, and assigned “better” as +1, “same” as 0, and “worse” as −1, and performed ordered logistic regression to determine the odds of favoring one category vs. another.
Results
A total of 283 questionnaires were mailed to patients diagnosed with MdDS. A total of 135 questionnaires/consent forms were returned. Twenty-two additional packets were returned by the post office because the individuals were no longer at the address on file. Eleven “do not wish to participate” cards were returned resulting in an approximately 52% response rate. Of the 135 returned packets, 132 were complete enough for analysis; an additional 10 were removed after secondary review because the respondents did not have an MdDS episode lasting at least 1 month. Data from the resulting 122 participants were analyzed. If a participant had experienced both MT and non-MT episodes, they were categorized according to their last episode, yielding 80 MT and 42 non-MT designations.
Basic demographic features, such as sex, age of onset, handedness, race, and duration of illness are provided in Table 1.
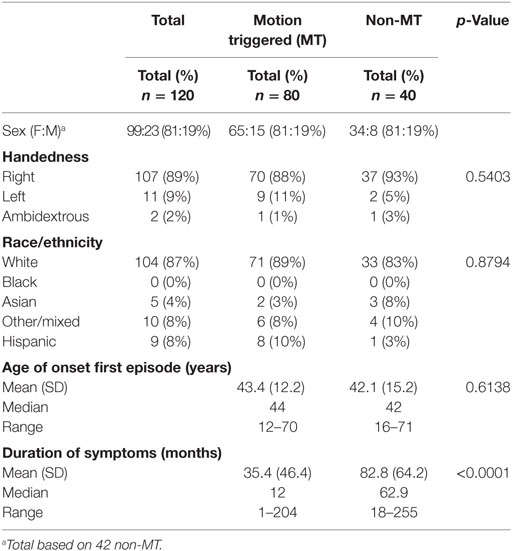
Table 1. Basic demographic characteristics.
There was a similar distribution of women vs. men in the MT vs. non-MT groups with a strong skew toward women (81% women vs. 19% men). The percentage of left-handed individuals was similar to population baselines (27). Of the respondents, the racial identification showed a higher proportion of self-identified whites, lower blacks, comparable Asians, and lower Hispanics compared to the latest general US census available from 2016 [76.9% whites, 13.3% black, 5.7% Asian, mixed 2.6%, and Hispanic 17.8%] (https://www.census.gov). Though both the mean and median age of onset of symptoms were earlier in the non-MT group, the difference was not significant. The main clear difference between the MT and non-MT groups was the longer duration of illness in the non-MT group [MT mean 35.4 (46.4), non-MT mean 82.8 (64.2), p < 0.0001]. Consistent with the difference in duration, 75% (60 out of 80) of MT MdDS and 90% (38 out of 42) of non-MT MdDS participants were continuing to experience symptoms at the time of the questionnaire.
The percentage of water, air, or land-based triggers, the age of onset of symptoms, and the duration of episodes experienced to date for each trigger were assessed for the MT MdDS group (Table 2). Since some episodes of MdDS were triggered by a combination of these exposures, the sum of the percentages was greater than 100%. Water-based triggers were the most common (69%), followed by air (33%), and then land (11%). One-way ANOVA with one factor (duration) and three levels (triggers), showed no significant effect of trigger type on duration (f ratio = 1.01, p = 0.367). Age of onset accounted for very little of the variance in duration of illness, R2 = 0.0257. Similarly, there was no significant difference between age of onset and trigger type (f ratio = 1.02, p = 0.364).

Table 2. Motion triggers for motion triggered Mal de Debarquement Syndrome.
Modulation of the rocking perception by re-exposure to passive motion, especially driving, or with walking, standing, lying down, or closing the eyes was evaluated on a basic scale of whether the rocking was better (decreased), stayed the same, or worsened (increased) in each of these body positions (Table 3).
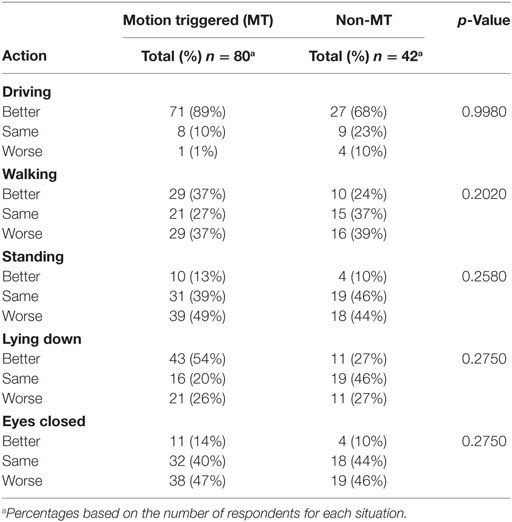
Table 3. Modulating feature of motion perception.
Respondents with MT MdDS were nearly always better when driving and rarely worse (89% better vs. 1% worse). The majority of individuals with non-MT MdDS also improved with driving, but not to as great an extent (64%), with a minority feeling worse (10%). In general, the effect of walking was as likely to make symptoms worse as better (both 37%) in the MT group. However, standing still was clearly more likely to worsen symptoms than to make them better (49% worse vs. 13% better). Lying down was more frequently reported as reducing the feeling of motion in MT MdDS than in non-MT MdDS (54 vs. 26%), but there was an important fraction of respondents in whom the rocking perception actually increased when recumbent (26%) in both groups. Removing vision was more likely to make symptoms worse than to make them better in both groups.
A history of migraine headaches, episodic vertigo, and any prior mental health diagnoses were specifically queried because of their known association with chronic dizziness (18, 28, 29) (Table 4). Respondents also reported about the context of their symptom onset, such as whether they were at a normal baseline or were experiencing any number of stressors at the onset of their symptoms (Table 4). Examples of physical stressors were concurrent medical illness or recent surgery. Mental health stressors included situations such as increased job or family stress or financial problems. Sleep deprivation was generally over a period of several weeks. Medication changes were of any variety, but the most important was rapid tapering of antidepressants. Hormone changes were typically abrupt switching of oral contraception. P-values reflect differences between the MT and non-MT group totals. There were no significant differences in past medical history or context of trigger between the MT and non-MT groups, but there was a trend toward a higher rater of baseline migraine in the non-MT group.
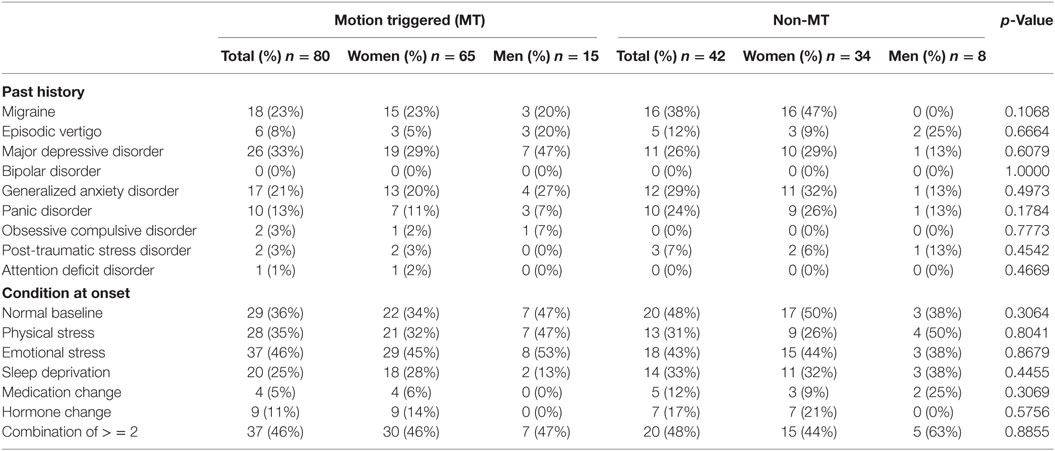
Table 4. Associated diagnoses and conditions.
In addition, the presence of current anxiety or depression was determined by completion of the hospital anxiety and depression scale (HADS) (Table 5). The HADS is a well-validated self-reported scale of seven items that query anxiety and seven items that query depression symptoms (30). Higher scores indicate more severe symptoms.
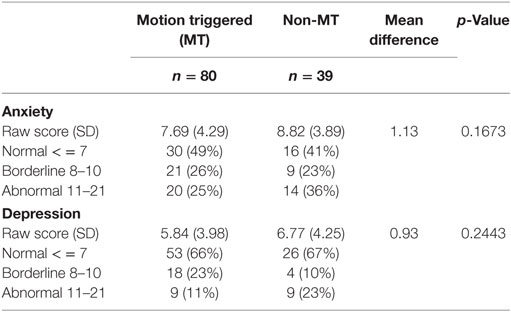
Table 5. Hospital anxiety and depression scale.
There were more individuals in the non-MT group whose scores were within the abnormal range for both anxiety (36 vs. 25%) and depression (23 vs. 11%) compared to the MT group, but the mean scores were not different between the two groups statistically.
Since the majority of affected individuals with MdDS were women, the relationship between MdDS and the effect of hormone transitions was queried (Table 6). Ages of onset of menarche, menopause, and MdDS showed no statistically significant differences between the MT and non-MT groups. Peri-menstrual worsening of symptoms was typical (71%) in both groups. Of MdDS occurring during hormonal transitions, only contraception change was significantly more common in the non-MT group.
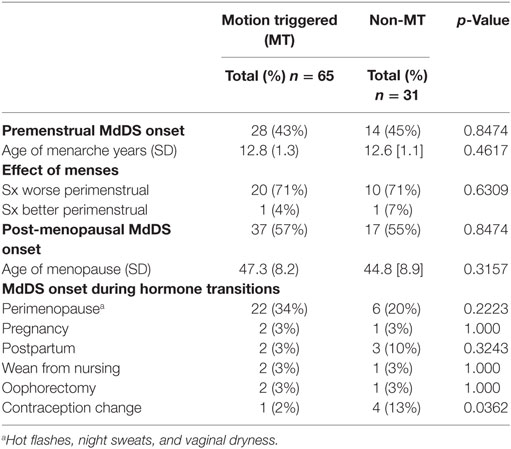
Table 6. Hormone status at onset of Mal de Debarquement Syndrome (MdDS).
Symptom severity was assessed on a 10-point scale in which 1 represented no rocking and 10 represented symptoms so severe that standing was not possible (Appendix). Since women and men could experience MdDS symptoms differently, scores were analyzed separately for women and men as well as for all MT and all non-MT respondents. The median rating of symptom severity by women was 0.5 higher in the MT group and 1 point higher in the non-MT group compared to men (Table 7).
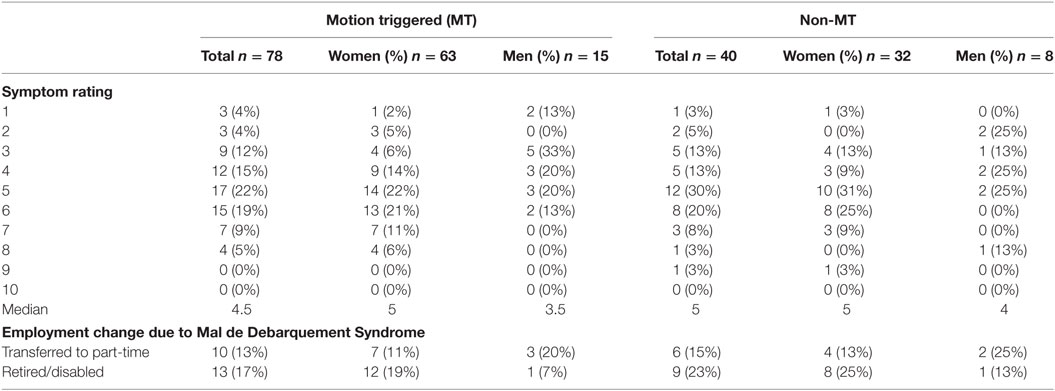
Table 7. Symptom severity and effect on employment.
Additionally, the effect of MdDS symptoms on transitions to part-time work if the individual was originally working full-time, or to early retirement or disability due to MdDS, was determined separately for women and men. 30% of MT and 38% of non-MT participants reported making a job status change because of their symptoms (Table 7).
Finally, we determined how treatments available to patients with MdDS at the time of the survey were scored. Though some experimental therapies have been investigated for MdDS to date, only therapies that were available through standard medical care were assessed for this study (25, 31–35).
Scores were made on a 1–6 scale with the following descriptors: 1 = greatly relieved symptoms; 2 = moderately improved symptoms; 3 = small but noticeable improvement; 4 = minimal improvement, if any; 5 = no improvement at all; and 6 = made symptoms worse.
Treatments that were tried by at least 10 individuals are listed in Table 8. Treatments that were rated at 1, 2, and 3 represented those that provided unambiguous positive responses and were combined under a single “Response” percentage.
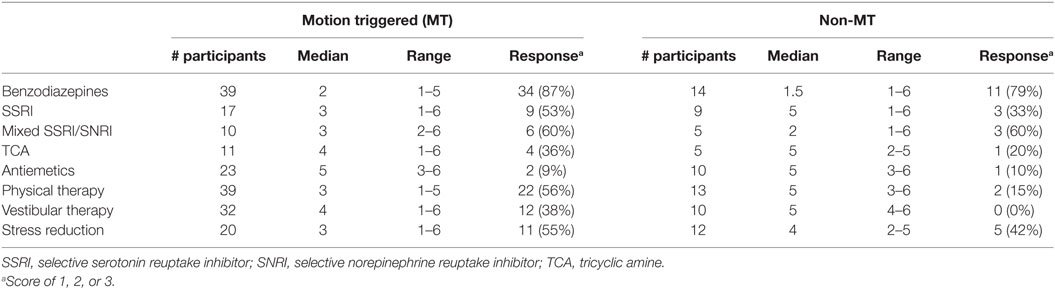
Table 8. Therapeutic responses.
Median responses to benzodiazepines and mixed SSRI/SNRIs were clearly on the favorable side in the majority of MT and non-MT participants. SSRIs, stress reduction, and physical therapy were reported to be somewhat helpful in the MT group, but less so in the non-MT group. Vestibular therapy could be somewhat helpful in the MT group, but was not helpful in the non-MT group. The median response rate was lower for the non-MT group for all categories of treatment other than benzodiazepines and SSRI/SNRIs. Other treatments tried by fewer than 10 individuals included: acetazolamide, other diuretics, low salt diet, beta-blockers, calcium channel blockers, and anticonvulsants. None were reported to confer any improvement, however.
Discussion
We report detailed clinical features of MdDS in order to elucidate the spectrum of historical features that may aid in recognizing, diagnosing, and treating individuals who present with rocking vertigo. New information provided through this study include a broad range of demographic data, such as sex, handedness, race, age, and triggers, as well as potentially contributing factors to the onset of symptoms, such as a past history of migraine or homeostatic altering factors, such as stress, medication changes, and sleep deprivation (Tables 1, 2, and 4). We also provide a measure of symptom severity, showing differences between women and men as well as the effect symptoms on employment status (Table 7).
Exacerbating and mitigating effects of body position, motion, and vision are reported. Our study shows that at least a quarter of individuals with MdDS may actually feel worse when they lie down (Table 3). This may be considered unusual for a balance disorder in which an intuitive assumption might be that getting off of one’s feet would be preferred. However, these individuals report that lying still and flat increases the internal motion perception, similar to how a very quiet room enhances the perception of tinnitus. This should not be confused with BPPV, however, which can be triggered by the motion of lying down. The vertigo of BPPV is specifically triggered by vertical head motion, lasts less than 1-min, and resolves once the head stops moving (36). Unlike BPPV, the motion perception of MdDS is persistent and not specifically head movement triggered.
Re-exposure to motion in the context of driving improved symptoms in the majority of participants, but there were more instances of driving worsening the rocking in the non-MT (10%) group compared to the MT group (1%). While 89% of MT MdDS individuals felt specifically better with driving, the percentage was lower (68%) in the non-MT group. Though this was not a statistically significant difference, it does suggest that there may be some underlying pathophysiological differences between the two groups (Table 3).
Though most individuals with MdDS did not meet current criteria for a depression or anxiety, the percentage of abnormal scores on both depression and anxiety subscores of the HADS was higher in the non-MT vs. the MT group. Whether this was simply due to their longer duration of illness is not clear, however (Table 5). There was a relatively high percentage of participants who had had a prior diagnosis of major depressive disorder (overall 33% for MT and 26% for non-MT), which is much higher than the reported population prevalence of 6–15% for depression (37). Similarly, the percentage of participants diagnosed with generalized anxiety disorder was also high at 21% for MT and 29% for non-MT, which is 2–3 times the prevalence of generalized anxiety disorder in the population (38). Since these assessments were of pre-existing mood and anxiety disorders, it is possible that they may have been premorbid risk factors for the development of MdDS. However, recall bias may potentially skew reporting, since current mood and anxiety symptoms may also affect recollection of past diagnoses.
The prevalence of migraine in MdDS patients at 23% MT and 38% non-MT revealed in this study is higher than the US population baseline of roughly 18% in women and 9% in men (Table 4) (39). A more specific evaluation of the association between migraine and MdDS was reported in an earlier study of this database (24). This prior study reported that though the general prevalence of migraine was similar in the two groups, the non-MT group generally began experiencing migraines before the onset of MdDS, while the MT group more frequently developed migraine along with the onset MdDS symptoms (24). Additionally, headache frequency and severity generally increased in both groups with the onset of MdDS symptoms.
An evolving issue is whether MdDS should be considered a form of vestibular migraine. Sensory hypersensitivities can develop as a function of MdDS itself and many of these symptoms overlap with migraine symptoms. For example, chronic nausea can develop in MdDS (16). On this baseline, any moderately severe headache that is worse with movement would automatically meet the criteria for migraine, creating a low bar for diagnosing migraine in an individual who has already developed MdDS (40). This subtlety should be considered when attempting to treat MdDS as a form of vestibular migraine.
Vestibular migraine has been conceptualized as an episodic disorder in which discrete vestibular events occur in the context of a history of migraine, but in which vestibular symptoms do not exceed 72 h (41). Therefore, MdDS would not be considered a form of vestibular migraine under current diagnostic criteria due to its chronicity. However, the pathophysiology could be related and there may be some support for treating MdDS with lifestyle modifications typically used to treat vestibular migraine (42). However, an argument against MdDS as specifically being a form of migraine is that SSRIs are generally much more effective than tricyclic amines in reducing MdDS symptoms (Table 8), while this pattern is exactly opposite the treatment pathway for migraine headaches in which SSRIs have not shown evidence of efficacy greater than placebo or tricyclic amines (43, 44).
The most striking feature of MdDS may be the duration of illness considering that it develops out of what should have been an otherwise self-limiting disorder. The probability of symptoms resolving with or without treatment declines quite rapidly after the first month, with a flattening out of the response curve at 12 months (16). There is also a striking difference in the duration of illness between the MT and non-MT groups, which was consistent with an overall lower response to treatment in the non-MT group. Notably, while both groups reported a high response rate to benzodiazepines, and moderately high levels of response to SSRI/SNRIs, they differed in that both physical and vestibular therapy were rarely reported to be helpful in non-MT MdDS (Table 8). Latent comorbidities, such as migraine, a mood, or anxiety disorder, which were slightly higher in the non-MT group, may be factors that work against symptom resolution (Tables 4 and 5).
An additional consideration is that non-MT MdDS might be diagnosed later than MT MdDS, since there is no proximate event such as recent travel in MT MdDS to aid in diagnosis. Therefore, the longer duration of non-MT MdDS reported here might be influenced by a potentially longer time to diagnosis and treatment. This potential factor was not specifically assessed in this study, since many of the patients presented for second opinions. It should be noted, however, that the durations reported in this study are not related to the time to diagnosis. A participant may have been diagnosed at 3 months into the symptoms, but participated in the study after 18 months of symptoms and thus be tabulated with a duration of 18 months if they were continuing to experience symptoms.
A second concern is potential recall bias in that some individuals simply may not remember the relevant motion trigger and thus be misclassified as non-MT MdDS. In order to mitigate against this possibility, we chose 2 h of travel as the criteria for diagnosing non-MT MdDS, since this duration is generally outside the normal range for most people’s daily activities. For MT MdDS participants, the proximate motion trigger was clear, prolonged motion, which was outside their normal daily activities. The onset of non-MT MdDS, however, was usually not as discrete as MT MdDS, with symptoms often evolving over days or weeks. Therefore, though there is some risk to misattributing a particular participant, we do not suspect that this affected many individuals.
It is possible that both MT and non-MT MdDS represent a convergent physiologic state that has been entered by two different pathways. Prior functional imaging studies have shown enhanced metabolism in the left entorhinal cortex and amygdala in individuals with MT-MdDS along with greater functional connectivity between these limbic regions and posterior visual and vestibular areas compared to controls. These findings were in the setting of lower limbic connectivity with prefrontal cortex (45). Entrainment of these limbic regions through periodic sensorimotor and vestibular input may be the critical factor in the pathophysiology in MT cases, whereas reduced higher order regulation of spatially tuned limbic regions might be a greater factor in non-MT MdDS (5, 46, 47).
Some individuals who have been diagnosed with non-MT MdDS or “spontaneous” MdDS or might also meet the criteria of persistent postural perceptual dizziness (PPPD). The PPPD diagnosis was created to encompass the characteristics of chronic subjective dizziness, space, and motion discomfort, and visual vertigo (48, 49). Proposed diagnostic criteria for PPPD include chronic dizziness and unsteadiness of at least three months duration that is of a non-vertiginous (non-rotational) nature that is generally worse on upright stance and which persists throughout the day. Visual stimuli and either active or passive movements exacerbate PPPD. Since some descriptions of PPPD include sensations of rocking, it is not clear whether individuals with non-MT rocking sensations should fall under the umbrella of PPPD vs. MdDS, or how much clinical utility the distinction would afford. Though the effect of passive motion may appear to be a critical difference between PPPD and non-MT MdDS, we did note that 10% of the non-MT participants did report feeling worse with driving, indicating that these disorders fall within a large spectrum.
Conclusion
We have presented a large body of clinical information on individuals with MT and non-MT MdDS in order to provide a view of the spectrum of these disorders. Given limited treatment choices in MdDS and the need to develop better predictive models for who responds best to certain treatments, a clearer understanding of the basic clinical features and variability in MdDS will help to increase recognition of MdDS in general medical practice, guide therapeutic management, and contribute to more accurate disease categorization.
Ethics Statement
This study was carried out in accordance with the recommendations of the UCLA School of Medicine Medical IRB #3. The protocol was approved by Medical IRB #3. All subjects gave written informed consent in accordance with the Declaration of Helsinki (26).
Author Contributions
Conceptualization: Y-HC and RB. Data curation: Y-HC and YC. Analysis: Y-HC and YC. Writing the draft: Y-HC. Reviewing and editing the final draft: Y-HC, YC, and RB.
Conflict of Interest Statement
The authors report that there were no personal, professional, or financial conflicts of interest in the design and execution of this study.
Acknowledgments
We thank the many patients throughout the years who have participated in these studies.
Funding
This work was funded by MdDS Balance Disorders Foundation, Springbank Foundation, NIH-NIDCD R03-DC010451, NSF EPSCor RII Track-2 #1539068, and NIH-NIHGMS grant P20GM121312.
References
1. Whittle J. An Exact Diary of the Late Expedition of His Illustrious Highness the Prince of Orange. Bradford on Avon: Ex Libris Press (1689).
2. Irwin JA. The pathology of sea-sickness. Lancet (1881) 118(3039):907–9. doi:10.1016/S0140-6736(02)38129-7
3. Brown JJ, Baloh RW. Persistent Mal de Debarquement Syndrome: a motion-induced subjective disorder of balance. Am J Otolaryngol (1987) 8:219–22. doi:10.1016/S0196-0709(87)80007-8
4. Hain TC, Hanna PA, Rheinberger MA. Mal de Debarquement. Arch Otolaryngol Head Neck Surg (1999) 125:615–20. doi:10.1001/archotol.125.6.615
5. Cha YH. Mal de Debarquement Syndrome: new insights. Ann N Y Acad Sci (2015) 1343:63–8. doi:10.1111/nyas.12701
6. Cohen H. Mild Mal de Debarquement after sailing. Ann N Y Acad Sci (1996) 781:598–600. doi:10.1111/j.1749-6632.1996.tb15734.x
7. Gordon CR, Spitzer O, Doweck I, Melamed Y, Shupak A. Clinical features of mal de debarquement: Adaptation and habituation to sea conditions. Jrnl Vest Res (1995) 5:363–9.
8. Stoffregen TA, Chen FC, Varlet M, Alcantara C, Bardy BG. Getting your sea legs. PLoS One (2013) 8:e66949. doi:10.1371/journal.pone.0066949
9. Nachum Z, Shupak A, Letichevsky V, Ben-David J, Tal D, Tamir A, et al. Mal de Debarquement and posture: reduced reliance on vestibular and visual cues. Laryngoscope (2004) 114:581–6. doi:10.1097/00005537-200403000-00036
10. Hain TC, Cherchi M. Mal de Débarquement Syndrome. Handb Clin Neurol (2016) 137:391–5. doi:10.1016/B978-0-444-63437-5.00028-5
12. Mucci V, Canceri JM, Brown R, Dai M, Yakushin S, Watson S, et al. Mal de Debarquement Syndrome: a survey on subtypes, misdiagnoses, onset and associated psychological features. J Neurol (2018) 265:486–99. doi:10.1007/s00415-017-8725-3
13. Bisdorff A, Von Brevern M, Lempert T, Newman-Toker DE. Classification of vestibular symptoms: towards an international classification of vestibular disorders. J Vestib Res (2009) 19:1–13. doi:10.3233/VES-2009-0343
14. Cha YH. Migraine-associated vertigo: diagnosis and treatment. Semin Neurol (2010) 30:167–74. doi:10.1055/s-0030-1249225
15. Macke A, Leporte A, Clark BC. Social, societal, and economic burden of Mal de Debarquement Syndrome. J Neurol (2012) 259:1326–30. doi:10.1007/s00415-011-6349-6
16. Cha YH, Brodsky J, Ishiyama G, Sabatti C, Baloh RW. Clinical features and associated syndromes of Mal de Debarquement. J Neurol (2008) 255:1038–44. doi:10.1007/s00415-008-0837-3
17. Golding JF. Motion sickness. Handb Clin Neurol (2016) 137:371–90. doi:10.1016/B978-0-444-63437-5.00027-3
18. Paillard AC, Quarck G, Paolino F, Denise P, Paolino M, Golding JF, et al. Motion sickness susceptibility in healthy subjects and vestibular patients: effects of gender, age and trait-anxiety. J Vestib Res (2013) 23:203–9. doi:10.3233/VES-130501
19. Best C, Tschan R, Eckhardt-Henn A, Dieterich M. Who is at risk for ongoing dizziness and psychological strain after a vestibular disorder? Neuroscience (2009) 164:1579–87. doi:10.1016/j.neuroscience.2009.09.034
20. Jönsson R, Sixt E, Landahl S, Rosenhall U. Prevalence of dizziness and vertigo in an urban elderly population. J Vestib Res (2004) 14:47–52.
21. Cha YH. Less common neuro-otologic disorders. Continuum (Minneap Minn) (2012) 18:1142–57. doi:10.1212/01.CON.0000421623.56525.11
22. Strupp M, Büttner U, Cohen B. Basic and clinical aspects of vertigo and dizziness. Ann N Y Acad Sci (2009) 1164:xi–xii. doi:10.1111/j.1749-6632.2009.04922.x
23. Arroll MA, Attree EA, Cha YH, Dancey CP. The relationship between symptom severity, stigma, illness intrusiveness and depression in Mal de Debarquement Syndrome (MdDS). J Health Psychol (2016) 21:1339–50. doi:10.1177/1359105314553046
24. Cha YH, Cui Y. Rocking dizziness and headache: a two-way street. Cephalalgia (2013) 33:1160–9. doi:10.1177/0333102413487999
25. Dai M, Cohen B, Cho C, Shin S, Yakushin SB. Treatment of the Mal de Debarquement Syndrome: a 1-year follow-up. Front Neurol (2017) 8:175. doi:10.3389/fneur.2017.00175
26. World Medical Association. World Medical Association Declaration of Helsinki. Ethical principles for medical research involving human subjects. Bull World Health Organ (2001) 79:373–4.
27. McManus IC. The inheritance of left-handedness. Ciba Found Symp (1991) 162:251–67; discussion 267–81.
28. Balaban CD, Thayer JF. Neurological bases for balance-anxiety links. J Anxiety Disord (2001) 15:53–79. doi:10.1016/S0887-6185(00)00042-6
29. Furman JM, Balaban CD, Jacob RG, Marcus DA. Migraine-anxiety related dizziness (MARD): a new disorder? J Neurol Neurosurg Psychiatry (2005) 76:1–8. doi:10.1136/jnnp.2004.048926
30. Zigmond AS, Snaith RP. The hospital anxiety and depression scale. Acta Psychiatr Scand (1983) 67:361–70. doi:10.1111/j.1600-0447.1983.tb09716.x
31. Cha Y-H, Urbano D, Pariseau N. Randomized single blind sham controlled trial of adjunctive home-based tDCS after rTMS for Mal de Debarquement Syndrome: safety, efficacy, and participant satisfaction assessment. Brain Stimulat (2016) 9:537–44. doi:10.1016/j.brs.2016.03.016
32. Cha YH, Cui Y, Baloh RW. Repetitive transcranial magnetic stimulation for Mal de Debarquement Syndrome. Otol Neurotol (2013) 34:175–9. doi:10.1097/MAO.0b013e318278bf7c
33. Ding L, Shou G, Yuan H, Urbano D, Cha YH. Lasting modulation effects of rTMS on neural activity and connectivity as revealed by resting state EEG. IEEE Trans Biomed Eng (2014) 61:2070–80. doi:10.1109/TBME.2014.2313575
34. Yuan H, Shou G, Urbano D, Ding L, Cha YH. Resting state functional connectivity signature of treatment effects of rTMS in Mal de Debarquement Syndrome. Brain Connect (2017) 7:617–26. doi:10.1089/brain.2017.0514
35. Dai M, Cohen B, Smouha E, Cho C. Readaptation of the vestibulo-ocular reflex relieves the Mal de Debarquement Syndrome. Front Neurol (2014) 5:1–6. doi:10.3389/fneur.2014.00124
36. Fife TD, Iverson DJ, Lempert T, Furman JM, Baloh RW, Tusa RJ, et al. Practice parameter: therapies for benign paroxysmal positional vertigo (an evidence-based review): report of the Quality Standards Subcommittee of the American Academy of Neurology. Neurology (2008) 70:2067–74. doi:10.1212/01.wnl.0000313378.77444.ac
37. Richards D. Prevalence and clinical course of depression: a review. Clin Psychol Rev (2011) 31:1117–25. doi:10.1016/j.cpr.2011.07.004
38. Wittchen HU. Generalized anxiety disorder: prevalence, burden, and cost to society. Depress Anxiety (2002) 16:162–71. doi:10.1002/da.10065
39. Victor TW, Hu X, Campbell JC, Buse DC, Lipton RB. Migraine prevalence by age and sex in the United States: a life-span study. Cephalalgia (2010) 30:1065–72. doi:10.1177/0333102409355601
40. Headache Classification Committee of the International Headache Society (IHS). The International Classification of Headache Disorders, 3rd edition (beta version). Cephalalgia (2013) 33:629–808. doi:10.1177/0333102413485658
41. Lempert T, Olesen J, Furman J, Waterston J, Seemungal B, Carey J, et al. Vestibular migraine: diagnostic criteria. J Vestib Res (2012) 22:167–72. doi:10.3233/VES-2012-0453
42. Ghavami Y, Haidar YM, Ziai KN, Moshtaghi O, Bhatt J, Lin HW, et al. Management of Mal de Debarquement Syndrome as vestibular migraines. Laryngoscope (2017) 127:1670–5. doi:10.1002/lary.26299
43. Banzi R, Cusi C, Randazzo C, Sterzi R, Tedesco D, Moja L. Selective serotonin reuptake inhibitors (SSRIs) and serotonin-norepinephrine reuptake inhibitors (SNRIs) for the prevention of migraine in adults. Cochrane Database Syst Rev (2015) 4:CD002919. doi:10.1002/14651858.CD002919.pub3
44. Silberstein SD, Holland S, Freitag F, Dodick DW, Argoff C, Ashman E, et al. Evidence-based guideline update: pharmacologic treatment for episodic migraine prevention in adults: report of the Quality Standards Subcommittee of the American Academy of Neurology and the American Headache Society. Neurology (2012) 78:1337–45. doi:10.1212/WNL.0b013e3182535d20
45. Cha YH, Chakrapani S, Craig A, Baloh RW. Metabolic and functional connectivity changes in Mal de Debarquement Syndrome. PLoS One (2012) 7:e49560. doi:10.1371/journal.pone.0049560
46. Liao C, Feng Z, Zhou D, Dai Q, Xie B, Ji B, et al. Dysfunction of fronto-limbic brain circuitry in depression. Neuroscience (2012) 201:231–8. doi:10.1016/j.neuroscience.2011.10.053
47. Etkin A, Schatzberg AF. Common abnormalities and disorder-specific compensation during implicit regulation of emotional processing in generalized anxiety and major depressive disorders. Am J Psychiatry (2011) 168:968–78. doi:10.1176/appi.ajp.2011.10091290
48. Staab JP, Ruckenstein MJ. Expanding the differential diagnosis of chronic dizziness. Arch Otolaryngol Head Neck Surg (2007) 133:170–6. doi:10.1001/archotol.133.2.170
49. Dieterich M, Staab JP. Functional dizziness: from phobic postural vertigo and chronic subjective dizziness to persistent postural-perceptual dizziness. Curr Opin Neurol (2017) 30:107–13. doi:10.1097/WCO.0000000000000417
Appendix
Mal de Debarquement Syndrome Symptom Severity Scale
1. No rocking.
2. Barely noticeable rocking. Walking is normal.
3. Mild intermittent rocking that can be easily ignored. Walking is normal.
4. Mild persistent rocking, which is distracting.
5. Moderate intermittent rocking which requires extra attention to balance control. Walking is normal.
6. Moderate persistent rocking that leads to balance difficulty. May occasionally stumble.
7. Moderately severe, but intermittent rocking that impairs walking. Need occasional assistance to walk.
8. Moderately severe persistent rocking that leads to great balance difficulty. Need assistance to walk for greater distances or specific situations.
9. Severe rocking causing great difficulty with walking. Need constant gait assistance.
10. Severe rocking that prevents any walking.
Keywords: Mal de Debarquement Syndrome, rocking vertigo, persistent postural perceptual dizziness, clinical spectrum, therapeutics
Citation: Cha Y-H, Cui YY and Baloh RW (2018) Comprehensive Clinical Profile of Mal De Debarquement Syndrome. Front. Neurol. 9:261. doi: 10.3389/fneur.2018.00261
Received: 12 February 2018; Accepted: 04 April 2018;
Published: 07 May 2018
Edited by:
Michael E. Hoffer, University of Miami, United StatesReviewed by:
Sergei B. Yakushin, Icahn School of Medicine at Mount Sinai, United StatesMarcos Rossi-Izquierdo, Hospital Universitario Lucus Augusti, Spain
Copyright: © 2018 Cha, Cui and Baloh. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Yoon-Hee Cha, ycha@laureateinstitute.org