 Peng-Fei Wang1†
Peng-Fei Wang1† Yang Chen1,2†
Yang Chen1,2† Si-Ying Song3Ting-Jian Wang1Wen-Jun Ji4Shou-Wei Li1Ning Liu1*
Si-Ying Song3Ting-Jian Wang1Wen-Jun Ji4Shou-Wei Li1Ning Liu1* Chang-Xiang Yan1*
Chang-Xiang Yan1*- 1Department of Neurosurgery, Sanbo Brain Hospital, Capital Medical University, Beijing, China
- 2State Key Laboratory of Cardiovascular Disease, Department of Cardiology, Fuwai Hospital, National Center for Cardiovascular Diseases, Chinese Academy of Medical Sciences and Peking Union Medical College, Beijing, China
- 3Department of Clinical Medicine, Capital Medical University, Beijing, China
- 4Key Laboratory, Department of Neurosurgery, The Second Hospital of Yulin, Xi'an Jiaotong University, Xi'an, China
Background: Treatment of cancers with programmed cell death protein 1 (PD-1) pathway inhibitors can lead to immune-related adverse events (irAEs), which could be serious and even fetal. Therefore, clinicians should be aware of the characteristics of irAEs associated with the use of such drugs.
Methods: The MEDLINE, EMBASE, and Cochrane databases were searched to find potential studies using the following strategies: anti-PD-1/PD-L1 treatment; irAEs; and cancer. R© package Meta was used to pool incidence.
Results: Forty-six studies representing 12,808 oncologic patients treated with anti-PD-1/PD-L1 agents were included in the meta-analysis. The anti-PD-1/PD-L1 agents included nivolumab, pembrolizumab, atezolizumab, durvalumab, avelumab, and BMS-936559. The tumor types were melanomas, Hodgkin lymphomas, urothelial carcinomas, breast cancers, non-small cell lung cancers, renal cell carcinomas (RCC), colorectal cancers, and others. We described irAEs according to organ systems, namely, the skin (pruritus, rash, maculopapular rash, vitiligo, and dermatitis), endocrine system (hypothyroidism, hyperthyroidism, hypophysitis, thyroiditis, and adrenal insufficiency), digestive system (colitis, diarrhea, pancreatitis, and increased AST/ALT/bilirubin), respiratory system (pneumonitis, lung infiltration, and interstitial lung disease), and urinary system (increased creatinine, nephritis, and renal failure). In patients treated with the PD-1 signaling inhibitors, the overall incidence of irAEs was 26.82% (95% CI, 21.73–32.61; I2, 92.80) in any grade and 6.10% (95% CI, 4.85–7.64; I2, 52.00) in severe grade, respectively. The development of irAEs was unrelated to the dose of anti-PD-1/PD-L1 agents. The incidence of particular irAEs varied when different cancers were treated with different drugs. The incidence of death due to irAEs was around 0.17%.
Conclusion: The occurrence of irAEs was organ-specific and related to drug and tumor types.
Introduction
Passive immunotherapy for cancer, which involves the transfer of tumor-targeted mono-antibodies and donor T cells, has demonstrated clinical benefits against a variety of solid and hematological malignancies. In contrast to passive immunity techniques, active immunotherapy strategies aim to augment self/anti-tumor responses (Mellman et al., 2011; Callahan et al., 2016; Michot et al., 2016). However, cancer cells always evolve to exploit multiple pathways to resist immune attack. These immunosuppressive pathways are referred to as “immune checkpoints,” which terminate immune responses in the normal physiological state (Pardoll, 2012). Notably, blockade of these immune checkpoints is frequently reported to be superior to traditional treatments in improving survival of oncologic patients (Borghaei et al., 2015; Ribas et al., 2015; Fehrenbacher et al., 2016; Rittmeyer et al., 2017).
Cytotoxic T lymphocyte-associated antigen 4 (CTLA-4) is expressed exclusively in T cells, where it inhibits their activation (Leach et al., 1996). Antagonistic anti-CTLA-4 antibodies, such as ipilimumab and tremelimumab with proven clinical benefits, have been developed (Pardoll, 2012; Callahan et al., 2016). Ipilimumab has been approved by the FDA (Food and Drug Administration) for the treatment of advanced or recurrent melanomas. Programmed cell death protein 1 (PD-1) and its ligand PD-L1 are immune check points that physiologically limit autoimmunity during inflammatory responses (Leach et al., 1996). Monoclonal antibodies against PD-1 or PD-L1, such as nivolumab, pembrolizumab, atezolizumab, avelumab, and durvalumab, have been produced. These PD-1/PD-L1 inhibitors could result in a stable regression of malignancy (Borghaei et al., 2015; Brahmer et al., 2015; Motzer et al., 2015; Ribas et al., 2015; Weber et al., 2015; Fehrenbacher et al., 2016; Herbst et al., 2016; Rittmeyer et al., 2017). Currently, the FDA has approved the use of nivolumab for advanced melanoma, renal cell carcinoma (RCC), and non-small cell lung cancer (NSCLC), and pembrolizumab for advanced melanoma and NSCLC (Costa et al., 2017). Furthermore, combined blockade of CTLA-4 and PD-1/PD-L1 appears to achieve additional clinical benefits (Callahan et al., 2016).
Treatment with immune-checkpoint inhibitors could cause immune-related adverse events (irAEs) by unbalancing the immune system (Chen et al., 2015; Marrone et al., 2016; Kumar et al., 2017). The definition of irAEs is different from that of AEs and treatment-related AEs. AEs that occur potentially due to immunological effects were defined as irAEs. irAEs could be serious, requiring suspension of immunotherapy and possibly leading to death (Bertrand et al., 2015; Chen et al., 2015; Eigentler et al., 2016). Previous studies indicated that the occurrence of irAEs induced by anti PD-1/PD-L1 agents is related to tumor types and organs and is dose-independent (Michot et al., 2016). Additionally, there are reports of delayed occurrence of irAEs after treatment with anti PD-1/PD-L1 agents (Nishino et al., 2015). Therefore, there is a need to understand the characteristics of irAEs associated with anti PD-1/PD-L1 treatments to help us manage them appropriately.
In this study, we present a systematic review and meta-analysis and aim to assess the incidence and characteristics of irAEs in malignancies treated with anti-PD-1/PD-L1 agents.
Methods
The protocol of this meta-analysis was registered at PROSPERO, International Prospective Register of Systematic Reviews (crd.york.ac.uk/prospero, Identifier: 42016051745).
Literature Searches
MEDLINE, EMBASE, and Cochrane databases were searched to determine potentially eligible studies from database inception to March 1, 2017. We put no restriction on language. The following search terms were used: “safety OR security OR side effects OR adverse events AND (anti-PD-1 OR anti-PD-L1 OR nivolumab OR pembrolizumab OR BMS-936559 OR atezolizumab OR avelumab OR durvalumab)” in MEDLINE and EMBASE, and “anti-PD-1 OR anti-PD-L1 OR nivolumab OR pembrolizumab OR BMS-936559 OR atezolizumab OR avelumab OR durvalumab” in Cochrane databases. We also screened the references of included studies and relevant reviews to find potential studies. There were too many medical records reporting the side effects of anti-PD-1/PD-L1 agents, and it was difficult to check all conference abstracts in the 2 years prior to this study.
Selection Criteria
Eligible studies were required to meet the following criteria: (1) Prospective clinical trials that reported irAEs, which were clearly identified as “AEs of special interest,” “immune-mediated adverse events,” or “selected treatment-related adverse events of special interest,” but not “treatment-related AEs” or “drug-related AEs.” Additionally, every corresponding author of a potential irAE-related study was e-mailed and asked to provide more information about the irAEs and (2) patients were diagnosed with malignancies that were treated with anti-PD-1/PD-L1 agents. Oncologic therapy prior to anti-PD-1/PD-L1 treatment was acceptable.
The exclusion criteria were: (1) Non-oncologic patients (e.g., hepatitis C virus-related patients) treated with anti-PD-1/PD-L1 agents; (2) Oncologic patients treated with anti-PD-1/PD-L1 agents combined with other treatments simultaneously; (3) Retrospective studies, meeting abstracts, case reports, basic research, reviews, systematic reviews and meta-analysis, letters, editorials, and expert opinions; and (4) Duplicate publications or unpublished studies.
Data Extraction
The titles and abstracts of all studies retrieved were independently reviewed by two authors. Next, the full texts of all potentially eligible studies were assessed. A standardized, pre-piloted form was used to extract relevant information from the included studies.
The primary outcomes for this meta-analysis were incidence and risk ratio (RR) of irAEs and their grade (1–5; recorded according to Version 3 or 4 of the Common Terminology Criteria for Adverse Events of the National Cancer Institute). We considered that Grades ≥3 were evaluated as high grade or severe grade. The secondary outcome was incidence of death due to irAEs. Any discrepancies were solved by discussion. Missing data were requested from the principle investigator by e-mail.
Quality Assessment
Two independent investigators assessed the risk of bias for the included studies according to the Cochrane Handbook for Systematic Reviews of Interventions (Higgins et al., 2011). The following components were assessed: sequence generation, allocation concealment, blinding, completeness of outcome data, incomplete outcome data, and other sources of bias. Disagreements were resolved by discussion among investigators until a consensus was reached.
Statistical Analysis
The incidence and RR of irAEs were estimated for the included studies in this meta-analysis. We pooled the incidence of irAEs in malignancies treated with anti-PD/PD-L1 agents. Heterogeneity between studies was assessed by Q test and I2 statistics. If the I2 value was less than 50%, the meta-analysis was performed using the fixed-effects model. Otherwise, the random-effects model was adopted. Potential publication bias was examined by funnel plots and Egger's test. Incidence was calculated using R software [R version 3.3.2 (2016-10-31)] with package Meta and Metaprop function. RR was calculated using Review Manager 5.3 (Nordic Cochrane Centre, Copenhagen, Denmark).
Results
Literature Search
Our search strategy identified 1,991 potential articles. Five-hundred and 51 studies were excluded owing to duplicates. The remaining articles were screened for titles and abstracts, and 1080 articles were removed based on our inclusion or exclusion criteria. Furthermore, 314 studies were dropped because they did not contain our data of interest. Finally, 46 studies were included in our meta-analysis. The study selection is shown in Figure 1.
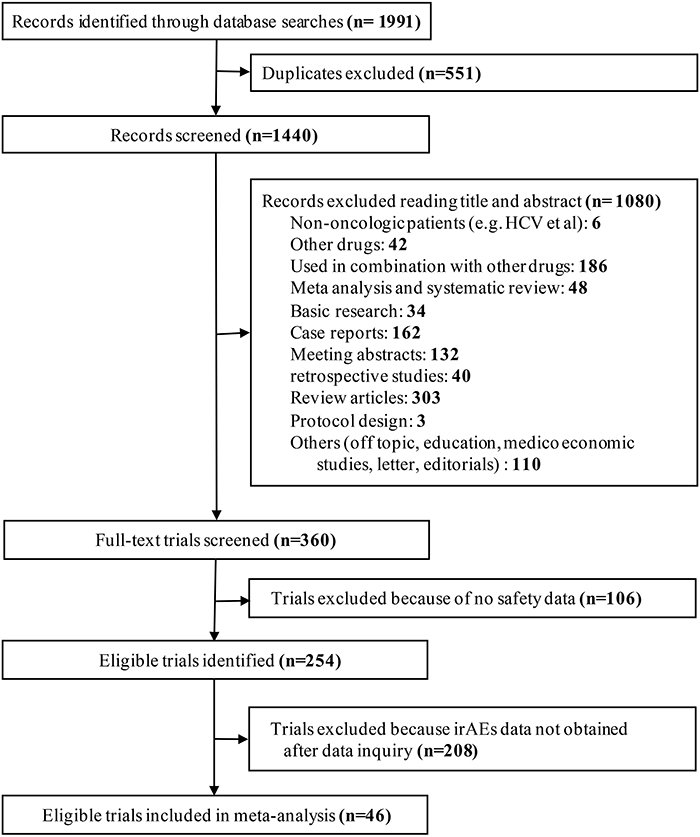
Figure 1. Flow diagram for identification and selection of studies included in the meta-analysis.
Study Characteristics
The detailed information of the clinical trials is presented in Table 1. Overall, 46 trials comprising 12,808 oncologic patients treated with anti-PD-1/PD-L1 agents were included in this meta-analysis (Table 1) (Brahmer et al., 2010, 2012, 2015; Topalian et al., 2012, 2014; Robert et al., 2014, 2015a,b; Borghaei et al., 2015; Garon et al., 2015; Gettinger et al., 2015, 2016; Hamanishi et al., 2015; Larkin et al., 2015; McDermott et al., 2015, 2016; Motzer et al., 2015; Patnaik et al., 2015; Ribas et al., 2015, 2016; Rizvi et al., 2015; Weber et al., 2015, 2016; Balar et al., 2016; Chatterjee et al., 2016; Choueiri et al., 2016; Fehrenbacher et al., 2016; Ferris et al., 2016; Herbst et al., 2016; Hua et al., 2016; Kaufman et al., 2016; Lesokhin et al., 2016; Massard et al., 2016; Muro et al., 2016; Nanda et al., 2016; Reck et al., 2016; Rosenberg et al., 2016; Seiwert et al., 2016; Shimizu et al., 2016; Younes et al., 2016; Bellmunt et al., 2017; Hui et al., 2017; Morris et al., 2017; Plimack et al., 2017; Sharma et al., 2017). Among these studies, there were 35 phase I/II clinical trials and 11 phase III clinical trials. Nine percent (4/46) of the studies were blind and 13% (6/46) were single-arm. There were 23 randomized trials and 18 multicentric studies. There were 21 studies involving nivolumab treatment (4,856 patients), 17 studies involving pembrolizumab treatment (5,581 patients), 5 trials involving atezolizumab treatment (2,015 patients), one trial involving durvalumab treatment (61 patients), and one trial involving avelumab treatment (88 patients).
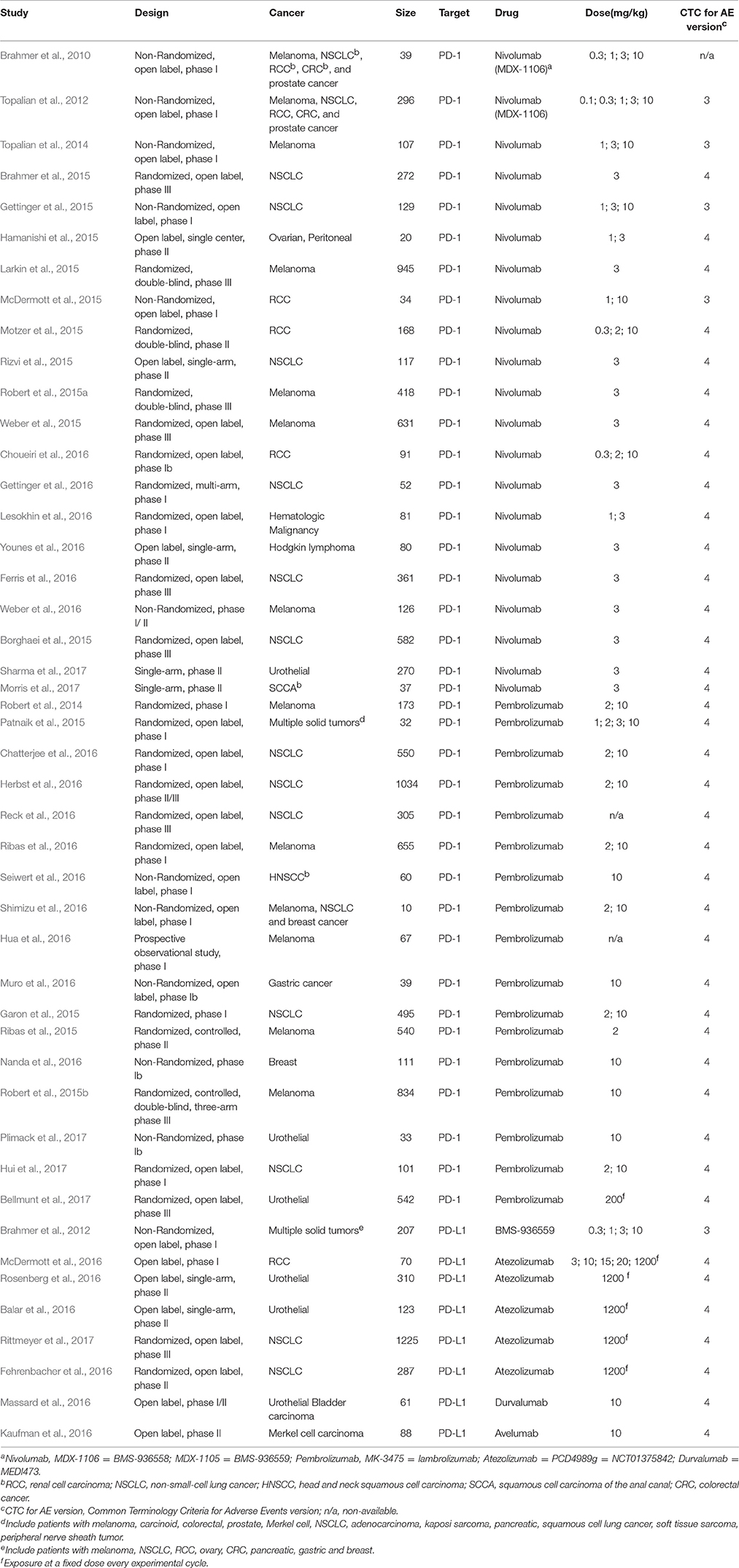
Table 1. Characteristics of studies included for meta-analysis.
Global Incidence of irAEs
The global incidence of irAEs of any grade and severe grade in patients treated with anti-PD-1/PD-L1 agents was 26.82% (95% CI, 21.73–32.61; I2, 92.80) and 6.10% (95% CI, 4.85–7.64; I2, 52.00), respectively (Figure S1). The incidence of any grade of irAEs was 18.50% (95% CI, 15.41–22.06; I2, 77.00) with pembrolizumab and 16.67% (95% CI, 4.75–44.50; I2, 96.00) with atezolizumab, which was lower than the incidence of irAEs with nivolumab (48.00%, 95% CI, 40.13–55.98; I2, 78.50). However, there were only slight differences in the incidence of severe grade irAEs, which was 8.25% (95% CI, 5.27–12.69; I2, 66.40) with nivolumab, 5.10% (95% CI, 3.58–7.22; I2, 48.40) with pembrolizumab, and 5.28% (95% CI, 3.62–7.64; I2, 0.00) with atezolizumab (Figure 2).
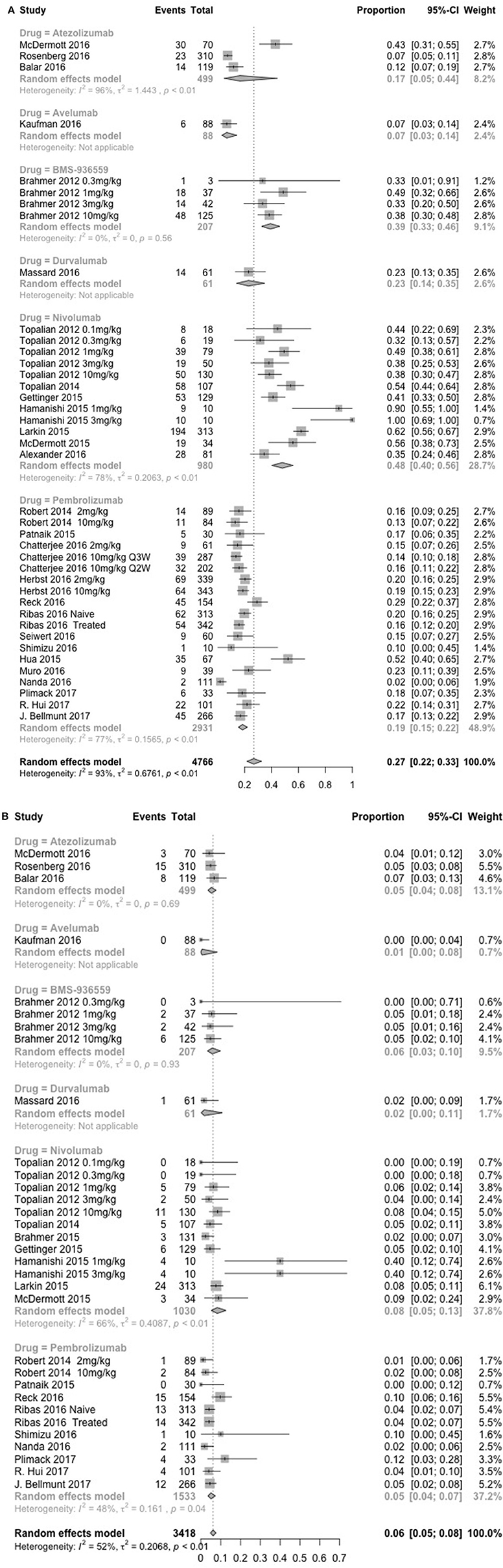
Figure 2. Incidence of global immune-related adverse events (irAEs) with nivolumab (1 and 3 mg/kg), pembrolizumab (2 mg/kg, 10 mg/kg, 200 mg), atezolizumab (1,200 mg) at all dosage, any grade (A), and severe grade (B).
Organ-Specific irAEs
We analyzed the incidence of irAEs associated with PD-1 blockade involving the skin, endocrine system, gastrointestinal tract, liver, kidney, and lung. The most common irAEs of all grades caused by nivolumab involved the skin, followed by the gastrointestinal tract, endocrine system, liver, lung, and kidney. The severe grade irAEs caused by nivolumab mostly occurred in the gastrointestinal tract and liver. However, we found it difficult to draw robust conclusions owing to limited data on pembrolizumab. The detailed information of organ-specific irAEs is presented in Tables S3–S8.
Skin
The most frequent irAEs during treatment with nivolumab were pruritus and rash, with an incidence of approximately 13%. However, pembrolizumab tended to have a lower incidence, less than 5% of any cutaneous irAEs of all grade. Notably, severe grade incidence of any irAEs was ~2% with nivolumab, pembrolizumab, and BMS-936559 (Table S9).
Endocrine System
The most common endocrine disorder associated with PD-1 blockade with nivolumab and pembrolizumab was hypothyroidism. PD-L1 blockade was associated with nearly the same incidence of irAEs for every endocrine disease. For all the drugs, the incidence of severe grade irAEs occurring in the endocrine system was ≤2% (Table S10).
Gastrointestinal Tract
Diarrhea was the most frequent irAEs in patients treated with nivolumab or BMS-936559, and its incidence was approximately 10–13%. Pembrolizumab was likely to have a relatively low risk of diarrhea of any grade, and its incidence was less than 4%. In addition, the incidence of high-grade colitis was ~1% regardless of the treatment type. Pancreatitis was rare, with an incidence of less than 1% for either all grade or severe grade across all drug types (Table S11).
Liver
The incidence of increased aspartate aminotransferase (AST) or alanine aminotransferase (ALT) levels ranged from 4 to 5% with nivolumab treatment. This incidence of increased AST or ALT levels was around 2% in patients treated with pembrolizumab or atezolizumab. However, the incidence of elevated AST/ALT/blood bilirubin and hepatitis was ≤2% regardless of treatment type (Table S12).
Pulmonary
Pneumonitis was the most common irAE related to the lung. The incidence of pneumonitis of any grade was approximately 3% and that of severe grade was approximately 1% during treatment with nivolumab or pembrolizumab. Treatment with atezolizumab was less likely to be associated with pneumonitis, with an incidence of ~1% for any grade and <1% for severe grade (Table S13).
Kidney
The incidence of any grade of nephritis was very low (less than 1%) regardless of the treatment type. There were reports of acute renal failure and renal failure only with nivolumab treatment, although the incidence was only ~2% for all grade and ~1% for severe grade (Table S14).
Tumor-Specific irAEs
We analyzed the incidence of irAEs with regard to the tumor being treated, including melanomas, NSCLCs, RCCs, and urothelial tumors. The highest incidence of any irAE associated with nivolumab and pembrolizumab occurred during the treatment of melanomas and NSCLCs, respectively. In contrast, the most frequent severe grade irAEs occurred with nivolumab treatment of melanomas.
Melanoma
The global incidence of all grade irAEs was 59.06% (95% CI, 51.53–66.18; I2, 50.00) with nivolumab and 21.33% (95% CI, 12.94–33.10; I2, 90.80) with pembrolizumab. The incidence of severe grade irAEs was low, ranging from 6.94% (95% CI, 4.69–10.16; I2, 8.3) with nivolumab to 3.80% (95% CI, 2.67–5.39; I2, 0.0%) with pembrolizumab (Figure S2).
The most frequent irAEs in patients treated with nivolumab were pruritus, followed by diarrhea and rash. Pembrolizumab treatment was mostly associated with hypothyroidism. In patients treated with nivolumab, the most frequent severe irAE was AST/ALT increase, with an incidence of ~3%, while the other irAEs were rare (<1%). The severe irAEs associated with pembrolizumab administration were maculopapular rash, colitis, increased AST, and hepatitis, occurring at 1–2% (Tables S15–S20).
NSCLC
The most common irAEs associated with nivolumab were rash and diarrhea, and those associated with pembrolizumab were hypothyroidism and hyperthyroidism. The incidence of any grade of irAEs with pembrolizumab was higher than that with nivolumab. Severe grade irAEs were rare (Tables S21–S26).
RCC
Diarrhea and colitis were the most frequent any grade irAEs and severe grade irAEs, respectively, associated with nivolumab treatment (Tables S27–S32).
Urothelial Carcinomas
The global incidence of any grade irAEs in urothelial cancers treated with pembrolizumab and atezolizumab was 17.06% (95% CI, 13.21; 21.76; I2, 0.00) and 9.09% (95% CI, 5, 75; 14.09; I2, 50.60), respectively. The number of studies providing statistics on organ-specific irAEs in patients with urothelial cancer was relatively small. From the limited cases, we found that the incidence of all grade irAEs and severe grade irAEs in specific organs were very rare, with incidence of ≤ 1–3% (Table S33).
Dose-Dependent Analysis
The incidence of all grade irAEs in patients treated with 3 mg/kg nivolumab was 58.08% (95% CI, 34.05–78.81; I2, 84.80), while that in patients treated with 1 mg/kg nivolumab was 70.00% (95% CI, 21.76–95.14; I2, 76.50). This dose-dependent effect was also observed in severe grade irAEs, with incidence of 7.84% (95% CI, 2.62–21.22; I2, 81.30) at 3 mg/kg and 16.88% (95% CI, 2.11–65.64; I2, 88.00) at 1 mg/kg (Table S1). Owing to limited data, we could not calculate the RR for nivolumab. However, we hypothesized that dose would not affect the development of irAEs as the 95% CI overlapped greatly.
In the treatment with pembrolizumab, the incidence of all grade irAEs was 18.93% (95% CI, 15.69–22.67; I2, 0.00) at 2 mg/kg, while that at 10 mg/kg was 15.16% (95% CI, 11.85–19.20; I2, 56.00). It was also observed that the incidence of severe grade irAEs was 1.12% (95% CI, 0.16–7.54) with 2 mg/kg pembrolizumab and 4.07% (95% CI, 1.10–13.91; I2, 69.70) with 10 mg/kg pembrolizumab (Table S2). The RR of developing any grade of global irAEs with pembrolizumab at 10 mg/kg vs. that at 2 mg/kg was not statistically different [RR, 0.91 (0.70, 1.17); P = 0.46; Figure S3].
Death Related to irAEs
Deaths due to irAEs were reported in 33 studies comprising 5,090 patients. Death occurred in nine of 5,090 patients, with an incidence of 0.74 (95% CI, 00.44; 1.25; I2, 38.20). Four patients died owing to pembrolizumab treatment, with an incidence of 0.89 (95 % CI, 00.49; 1.62; I2, 0.00). Five patients died following nivolumab treatment, and four of the deaths were due to pneumonitis. The incidence of deaths following nivolumab treatment was 0.77 (95% CI, 00.32; 1.87; I2, 56.20). Drug/treatment-related deaths and studies not reporting deaths were not included in this meta-analysis.
Quality Assessment and Publication Bias
Risk of bias graphs and risk of bias summaries from Review Manager 5.3 were used to evaluate the methodological qualities of the studies. Blinding of participants and personnel was evaluated as a low risk item because many studies were dose-escalation and single-arm trials. The overall risk of bias was evaluated as low risk. Therefore, the quality of the studies was satisfactory (Figure S4).
The funnel plot and Egger's test for publication bias showed a symmetric distribution of trials on either side of the funnel. The Begg's test and Egger's test (P = 0.7355) also indicated that no significant publication bias existed in this meta-analysis (Figure S5).
Discussion
In the present study, we systematically characterized the occurrence of irAEs in oncologic patients treated with anti-PD-1/PD-L1 agents according to different targets, drug types, drug dose, organ-specificity, and the tumor type treated. Although immune-check point inhibitors improved clinical outcomes in oncology, their irAEs should not be neglected (Bertrand et al., 2015; Michot et al., 2016; Costa et al., 2017; Tie et al., 2017). A previous meta-analysis indicated a high risk of irAEs with anti-CTLA-4 treatment, with incidence of 72% (95% CI, 65–79%) for all grade irAEs and 24% (95% CI, 18–30%) for high grade irAEs, and the occurrence of irAEs following anti-CTLA-4 treatment was dose-dependent (Bertrand et al., 2015). However, we found a much lower incidence of irAEs in patients treated with any of the anti-PD-1/PD-L1 agents, regardless of the drug type or dose. This indicates better tolerance of PD-1/PD-L1 inhibitors in cancer patients. Moreover, severe grade irAEs caused by any anti-PD-1/PD-L1 agent had a very low incidence, ranging from 5 to 8%. This helped in maximizing patient safety and treatment duration, because serious irAEs may result in the discontinuation of anti-PD-1/PD-L1 treatment in patients (Kumar et al., 2017).
A wide spectrum of irAEs was induced by all anti-PD-1/PD-L1 agents, including those involving the skin, gastrointestinal tract, lung, kidney, and liver. Michot et al. suggested that irAEs of grade I-II mainly affected the skin and gastrointestinal tract, and severe grade irAEs mostly occurred within the digestive system (Michot et al., 2016). We also found organ-specific irAEs associated with PD-1/PD-L1 blockade; however, our results indicated that these organ-specific characteristics were related to drug types. During nivolumab treatment, the most common irAEs of all grades were skin- (e.g., pruritus, rash) and gastrointestinal tract-related (e.g., diarrhea), with an incidence of approximately 13%. In contrast, during pembrolizumab treatment, the irAE with the highest incidence (~8%) was hypothyroidism (Tables S3–14). Additionally, the incidence of irAEs caused by PD-1 blockade was tumor-specific. Pneumonitis of all grades more frequently occurred during NSCLC and RCC treatment than during melanoma treatment. We also found a higher incidence of pneumonitis during NSCLC (4.15%, 95% CI, 3.36–5.12%) and RCC (7.19%, 95% CI, 4.54–11.21%) treatments than during melanoma treatment (2.18%, 95% CI, 1.67–2.84%; Tables S19, S25, and S31). Moreover, the incidence of all grade pruritus and diarrhea was lower in NSCLC than in melanoma and RCC during nivolumab treatment (Tables S15, S17, S21, S23, S27, and S29), confirming that the irAEs were tumor-specific. Our results correspond well with those published previously (Nishino et al., 2016) and are arguably more convincing owing to the larger number of studies involved.
In addition to the irAEs caused by anti-PD-1/PD-L1 agents, the response rate of this immunotherapy was another concern (Gibney et al., 2016; Topalian et al., 2016). Fortunately, genomic sequencing, RNA sequencing, and whole exome sequencing were of great importance in identifying predictive biomarkers for anti-PD-1/PD-L1 agent responses Gibney et al., 2016; Topalian et al., 2016; Hugo et al., 2017. Similarly, we could utilize the methods above to identify the genes associated with a higher risk of irAEs, especially with severe grade irAEs, which can sometimes be fatal. We conclude that the pattern of irAE occurrence was dependent on drug type, tumor type, irAE grades, target organ, and the particular irAE. However, the dataset in our analysis could ideally have been larger. As there are many ongoing studies on anti-PD-1/PD-L1 agents, we recommend that the factors related to irAEs be recorded in these clinical trials.
Limitations
There were some limitations in our study. First, the variability of clinical settings was high. Adopting the random-effects model was an important step to control variability. In addition, the main source of variability was significantly reduced when subgroup analysis was performed based on irAE grades, organs, drug types, and tumor types. These results provide clinical value for physicians to be wary about the occurrence of irAEs when treating specific tumors with different drugs. Second, the number of studies and patients were limited in the subgroup analysis performed based on drug type, organ-specific irAEs, particular irAEs, and tumor type. Third, some of the included studies were not random clinical trials, introducing some bias in our analysis. Last, the incidence of irAEs was not clear in patients with preexisting autoimmune diseases according to our analysis. Because all the included studies excluded patients with active autoimmune disease or a documented history of autoimmune disease or syndrome that requires systemic steroids or immunosuppressive agents, except vitiligo or resolved childhood asthma/atopy. Therefore, the safety of PD-1 inhibitors in patients with pre-existing autoimmune diseases needed to be assessed further in experimental or clinical studies.
Conclusion
In conclusion, our meta-analysis provided a statistical overview of irAEs in oncologic patients treated with anti-PD-1/PD-L1 agents. The pattern of irAE occurrence was organ-specific and related to the drug and tumor types.
Author Contributions
Conception and design: CY and NL; Collection and assembly of data: PW and YC; Data analysis and interpretation: All authors; Manuscript writing: All authors; Final approval of manuscript: All authors; Accountable for all aspects of the work: All authors.
Conflict of Interest Statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Supplementary Material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fphar.2017.00730/full#supplementary-material
References
Balar, A. V., Galsky, M. D., Rosenberg, J. E., Powles, T., Petrylak, D. P., Bellmunt, J., et al. (2016). Atezolizumab as first-line treatment in cisplatin-ineligible patients with locally advanced and metastatic urothelial carcinoma: a single-arm, multicentre, phase 2 trial. Lancet 389, 67–76. doi: 10.1016/S0140-6736(16)32455-2
Bellmunt, J., de Wit, R., Vaughn, D. J., Fradet, Y., Lee, J. L., Fong, L., et al. (2017). Pembrolizumab as second-line therapy for advanced urothelial carcinoma. N. Engl. J. Med. 376, 1015–1026. doi: 10.1056/NEJMoa1613683
Bertrand, A., Kostine, M., Barnetche, T., Truchetet, M. E., and Schaeverbeke, T. (2015). Immune related adverse events associated with anti-CTLA-4 antibodies: systematic review and meta-analysis. BMC Med. 13:211. doi: 10.1186/s12916-015-0455-8
Borghaei, H., Paz-Ares, L., Horn, L., Spigel, D., Steins, M., Ready, N., et al. (2015). Nivolumab versus docetaxel in advanced nonsquamous non-small-cell lung cancer. N. Eng. J. Med. 373, 1627–1639. doi: 10.1056/NEJMoa1507643
Brahmer, J. R., Drake, C. G., Wollner, I., Powderly, J. D., Picus, J., Sharfman, W. H., et al. (2010). Phase I study of single-agent anti-programmed death-1 (MDX-1106) in refractory solid tumors: safety, clinical activity, pharmacodynamics, and immunologic correlates. J. Clin. Oncol. 28, 3167–3175. doi: 10.1200/JCO.2009.26.7609
Brahmer, J., Reckamp, K., Baas, P., Crinò, L., Eberhardt, W., Poddubskaya, E., et al. (2015). Nivolumab versus docetaxel in advanced squamous-cell non-small-cell lung cancer. N. Eng. J. Med. 373, 123–135. doi: 10.1056/NEJMoa1504627
Brahmer, J. R., Tykodi, S. S., Chow, L. Q., Hwu, W. J., Topalian, S. L., Hwu, P., et al. (2012). Safety and activity of anti-PD-L1 antibody in patients with advanced cancer. N. Engl. J. Med. 366, 2455–2465. doi: 10.1056/NEJMoa1200694
Callahan, M. K., Postow, M. A., and Wolchok, J. D. (2016). Targeting T Cell co-receptors for cancer therapy. Immunity 44, 1069–1078. doi: 10.1016/j.immuni.2016.04.023
Chatterjee, M., Turner, D. C., Felip, E., Lena, H., Cappuzzo, F., Horn, L., et al. (2016). Systematic evaluation of pembrolizumab dosing in patients with advanced non-small-cell lung cancer. Ann. Oncol. 27, 1291–1298. doi: 10.1093/annonc/mdw174
Chen, T. W., Razak, A. R., Bedard, P. L., Siu, L. L., and Hansen, A. R. (2015). A systematic review of immune-related adverse event reporting in clinical trials of immune checkpoint inhibitors. Ann. Oncol. 26, 1824–1829. doi: 10.1093/annonc/mdv182
Choueiri, T. K., Fishman, M. N., Escudier, B., McDermott, D. F., Drake, C. G., Kluger, H., et al. (2016). Immunomodulatory activity of nivolumab in metastatic renal cell carcinoma. Clin. Cancer Res. 22, 5461–5471. doi: 10.1158/1078-0432.CCR-15-2839
Costa, R., Carneiro, B. A., Agulnik, M., Rademaker, A. W., Pai, S. G., Villaflor, V. M., et al. (2017). Toxicity profile of approved anti-PD-1 monoclonal antibodies in solid tumors: a systematic review and meta-analysis of randomized clinical trials. Oncotarget 8, 8910–8920. doi: 10.18632/oncotarget.13315
Eigentler, T. K., Hassel, J. C., Berking, C., Aberle, J., Bachmann, O., Grunwald, V., et al. (2016). Diagnosis, monitoring and management of immune-related adverse drug reactions of anti-PD-1 antibody therapy. Cancer Treat. Rev. 45, 7–18. doi: 10.1016/j.ctrv.2016.02.003
Fehrenbacher, L., Spira, A., Ballinger, M., Kowanetz, M., Vansteenkiste, J., Mazieres, J., et al. (2016). Atezolizumab versus docetaxel for patients with previously treated non-small-cell lung cancer (POPLAR): a multicentre, open-label, phase 2 randomised controlled trial. Lancet 387, 1837–1846. doi: 10.1016/S0140-6736(16)00587-0
Ferris, R. L., Blumenschein, G. Jr., Fayette, J., Guigay, J., Colevas, A. D., Licitra, L., et al. (2016). Nivolumab for recurrent squamous-cell carcinoma of the head and neck. N. Engl. J. Med. 375, 1856–1867. doi: 10.1056/NEJMoa1602252
Garon, E. B., Rizvi, N. A., Hui, R., Leighl, N., Balmanoukian, A. S., Eder, J. P., et al. (2015). Pembrolizumab for the treatment of non-small-cell lung cancer. N. Engl. J. Med. 372, 2018–2028. doi: 10.1056/NEJMoa1501824
Gettinger, S. N., Horn, L., Gandhi, L., Spigel, D. R., Antonia, S. J., Rizvi, N. A., et al. (2015). Overall survival and long-term safety of nivolumab (anti-programmed death 1 antibody, BMS-936558, ONO-4538) in patients with previously treated advanced non-small-cell lung cancer. J. Clin. Oncol. 33, 2004–2012. doi: 10.1200/JCO.2014.58.3708
Gettinger, S., Rizvi, N., Chow, L., Borghaei, H., Brahmer, J., Ready, N., et al. (2016). Nivolumab monotherapy for first-line treatment of advanced non-small-cell lung cancer. J. Clin. Oncol. 34, 2980–2987. doi: 10.1200/JCO.2016.66.9929
Gibney, G. T., Weiner, L. M., and Atkins, M. B. (2016). Predictive biomarkers for checkpoint inhibitor-based immunotherapy. Lancet Oncol. 17, e542–e551. doi: 10.1016/S1470-2045(16)30406-5
Hamanishi, J., Mandai, M., Ikeda, T., Minami, M., Kawaguchi, A., Murayama, T., et al. (2015). Safety and antitumor activity of anti-PD-1 antibody, nivolumab, in patients with platinum-resistant ovarian cancer. J. Clin. Oncol. 33, 4015–4022. doi: 10.1200/JCO.2015.62.3397
Herbst, R., Baas, P., Kim, D., Felip, E., Pérez-Gracia, J., Han, J., et al. (2016). Pembrolizumab versus docetaxel for previously treated, PD-L1-positive, advanced non-small-cell lung cancer (KEYNOTE-010): a randomised controlled trial. Lancet 387, 1540–1550. doi: 10.1016/S0140-6736(15)01281-7
Higgins, J. P., Altman, D. G., Gotzsche, P. C., Juni, P., Moher, D., Oxman, A. D., et al. (2011). The Cochrane Collaboration's tool for assessing risk of bias in randomised trials. BMJ 343:d5928. doi: 10.1136/bmj.d5928
Hua, C., Boussemart, L., Mateus, C., Routier, E., Boutros, C., Cazenave, H., et al. (2016). Association of vitiligo with tumor response in patients with metastatic melanoma treated with pembrolizumab. JAMA Dermatol. 152, 45–51. doi: 10.1001/jamadermatol.2015.2707
Hugo, W., Zaretsky, J. M., Sun, L., Song, C., Moreno, B. H., Hu-Lieskovan, S., et al. (2017). Genomic and transcriptomic features of response to Anti-PD-1 therapy in metastatic melanoma. Cell 168:542. doi: 10.1016/j.cell.2017.01.010
Hui, R., Garon, E. B., Goldman, J. W., Leighl, N. B., Hellmann, M. D., Patnaik, A., et al. (2017). Pembrolizumab as first-line therapy for patients with PD-L1-positive advanced non-small cell lung cancer: a phase 1 trial. Ann. Oncol. 28, 874–881. doi: 10.1093/annonc/mdx008
Kaufman, H. L., Russell, J., Hamid, O., Bhatia, S., Terheyden, P., D'Angelo, S. P., et al. (2016). Avelumab in patients with chemotherapy-refractory metastatic Merkel cell carcinoma: a multicentre, single-group, open-label, phase 2 trial. Lancet Oncol. 17, 1374–1385. doi: 10.1016/S1470-2045(16)30364-3
Kumar, V., Chaudhary, N., Garg, M., Floudas, C. S., Soni, P., and Chandra, A. B. (2017). Current diagnosis and management of immune related adverse events (irAEs) induced by immune checkpoint inhibitor therapy. Front. Pharmacol. 8:49. doi: 10.3389/fphar.2017.00049
Larkin, J., Chiarion-Sileni, V., Gonzalez, R., Grob, J., Cowey, C., Lao, C., et al. (2015). Combined nivolumab and ipilimumab or monotherapy in untreated melanoma. N. Eng. J. Med. 373, 23–34. doi: 10.1056/NEJMoa1504030
Leach, D. R., Krummel, M. F., and Allison, J. P. (1996). Enhancement of antitumor immunity by CTLA-4 blockade. Science 271, 1734–1736. doi: 10.1126/science.271.5256.1734
Lesokhin, A. M., Ansell, S. M., Armand, P., Scott, E. C., Halwani, A., Gutierrez, M., et al. (2016). Nivolumab in patients with relapsed or refractory hematologic malignancy: preliminary results of a Phase Ib study. J. Clin. Oncol. 34, 2698–2704. doi: 10.1200/JCO.2015.65.9789
Marrone, K. A., Ying, W., and Naidoo, J. (2016). Immune-related adverse events from immune checkpoint inhibitors. Clin. Pharmacol. Ther. 100, 242–251. doi: 10.1002/cpt.394
Massard, C., Gordon, M. S., Sharma, S., Rafii, S., Wainberg, Z. A., Luke, J., et al. (2016). Safety and efficacy of durvalumab (MEDI4736), an anti-programmed cell death ligand-1 immune checkpoint inhibitor, in patients with advanced urothelial bladder cancer. J. Clin. Oncol. 34, 3119–3125. doi: 10.1200/JCO.2016.67.9761
McDermott, D. F., Drake, C. G., Sznol, M., Choueiri, T. K., Powderly, J. D., Smith, D. C., et al. (2015). Survival, durable response, and long-term safety in patients with previously treated advanced renal cell carcinoma receiving nivolumab. J. Clin. Oncol. 33, 2013–2020. doi: 10.1200/JCO.2014.58.1041
McDermott, D. F., Sosman, J. A., Sznol, M., Massard, C., Gordon, M. S., Hamid, O., et al. (2016). Atezolizumab, an anti-programmed death-ligand 1 antibody, in metastatic renal cell carcinoma: long-term safety, clinical activity, and immune correlates from a phase ia study. J. Clin. Oncol. 34, 833–842. doi: 10.1200/JCO.2015.63.7421
Mellman, I., Coukos, G., and Dranoff, G. (2011). Cancer immunotherapy comes of age. Nat. Clin. Pract. Oncol. 2, 480–489. doi: 10.1038/nature10673
Michot, J. M., Bigenwald, C., Champiat, S., Collins, M., Carbonnel, F., Postel-Vinay, S., et al. (2016). Immune-related adverse events with immune checkpoint blockade: a comprehensive review. Eur. J. Cancer 54, 139–148. doi: 10.1016/j.ejca.2015.11.016
Morris, V. K., Salem, M. E., Nimeiri, H., Iqbal, S., Singh, P., Ciombor, K., et al. (2017). Nivolumab for previously treated unresectable metastatic anal cancer (NCI9673): a multicentre, single-arm, phase 2 study. Lancet Oncol. 18, 446–453. doi: 10.1016/S1470-2045(17)30104-3
Motzer, R. J., Escudier, B., McDermott, D. F., George, S., Hammers, H. J., Srinivas, S., et al. (2015). Nivolumab versus everolimus in advanced renal-cell carcinoma. N. Engl. J. Med. 373, 1803–1813. doi: 10.1056/NEJMoa1510665
Muro, K., Chung, H. C., Shankaran, V., Geva, R., Catenacci, D., Gupta, S., et al. (2016). Pembrolizumab for patients with PD-L1-positive advanced gastric cancer (KEYNOTE-012): a multicentre, open-label, phase 1b trial. Lancet Oncol. 17, 717–726. doi: 10.1016/S1470-2045(16)00175-3
Nanda, R., Chow, L. Q., Dees, E. C., Berger, R., Gupta, S., Geva, R., et al. (2016). Pembrolizumab in patients with advanced triple-negative breast cancer: Phase Ib KEYNOTE-012 study. J. Clin. Oncol. 34, 2460–2467. doi: 10.1200/JCO.2015.64.8931
Nishino, M., Giobbie-Hurder, A., Hatabu, H., Ramaiya, N. H., and Hodi, F. S. (2016). Incidence of programmed cell death 1 inhibitor-related pneumonitis in patients with advanced cancer: a systematic review and meta-analysis. JAMA Oncol. 2, 1607–1616. doi: 10.1001/jamaoncol.2016.2453
Nishino, M., Sholl, L. M., Hodi, F. S., Hatabu, H., and Ramaiya, N. H. (2015). Anti-PD-1-Related Pneumonitis during Cancer Immunotherapy. N. Engl. J. Med. 373, 288–290. doi: 10.1056/NEJMc1505197
Pardoll, D. M. (2012). The blockade of immune checkpoints in cancer immunotherapy. Nat. Rev. Cancer 12, 252–264. doi: 10.1038/nrc3239
Patnaik, A., Kang, S. P., Rasco, D., Papadopoulos, K. P., Elassaiss-Schaap, J., Beeram, M., et al. (2015). Phase I study of pembrolizumab (MK-3475; Anti-PD-1 monoclonal antibody) in patients with advanced solid tumors. Clin. Cancer Res. 21, 4286–4293. doi: 10.1158/1078-0432.CCR-14-2607
Plimack, E. R., Bellmunt, J., Gupta, S., Berger, R., Chow, L. Q., Juco, J., et al. (2017). Safety and activity of pembrolizumab in patients with locally advanced or metastatic urothelial cancer (KEYNOTE-012): a non-randomised, open-label, phase 1b study. Lancet Oncol. 18, 212–220. doi: 10.1016/S1470-2045(17)30007-4
Reck, M., Rodriguez-Abreu, D., Robinson, A. G., Hui, R., Csoszi, T., Fulop, A., et al. (2016). Pembrolizumab versus Chemotherapy for PD-L1-Positive Non-Small-Cell Lung Cancer. N. Engl. J. Med. 375, 1823–1833. doi: 10.1056/NEJMoa1606774
Ribas, A., Hamid, O., Daud, A., Hodi, F., Wolchok, J., Kefford, R., et al. (2016). Association of pembrolizumab with tumor response and survival among patients with advanced melanoma, JAMA 315, 1600–1609. doi: 10.1001/jama.2016.4059
Ribas, A., Puzanov, I., Dummer, R., Schadendorf, D., Hamid, O., Robert, C., et al. (2015). Pembrolizumab versus investigator-choice chemotherapy for ipilimumab-refractory melanoma (KEYNOTE-002): a randomised, controlled, phase 2 trial. Lancet Oncol. 16, 908–918. doi: 10.1016/S1470-2045(15)00083-2
Rittmeyer, A., Barlesi, F., Waterkamp, D., Park, K., Ciardiello, F., von Pawel, J., et al. (2017). Atezolizumab versus docetaxel in patients with previously treated non-small-cell lung cancer (OAK): a phase 3, open-label, multicentre randomised controlled trial. Lancet 389, 255–265. doi: 10.1016/S0140-6736(16)32517-X
Rizvi, N. A., Mazieres, J., Planchard, D., Stinchcombe, T. E., Dy, G. K., Antonia, S. J., et al. (2015). Activity and safety of nivolumab, an anti-PD-1 immune checkpoint inhibitor, for patients with advanced, refractory squamous non-small-cell lung cancer (CheckMate 063): a phase 2, single-arm trial. Lancet Oncol. 16, 257–265. doi: 10.1016/S1470-2045(15)70054-9
Robert, C., Long, G. V., Brady, B., Dutriaux, C., Maio, M., Mortier, L., et al. (2015a). Nivolumab in previously untreated melanoma without BRAF mutation. New Eng. J. Med. 372, 311–319. doi: 10.1056/NEJMoa1412082
Robert, C., Ribas, A., Wolchok, J., Hodi, F., Hamid, O., Kefford, R., et al. (2014). Anti-programmed-death-receptor-1 treatment with pembrolizumab in ipilimumab-refractory advanced melanoma: a randomised dose-comparison cohort of a phase 1 trial. Lancet 384, 1109–1117. doi: 10.1016/S0140-6736(14)60958-2
Robert, C., Schachter, J., Long, G., Arance, A., Grob, J., Mortier, L., et al. (2015b). Pembrolizumab versus ipilimumab in advanced melanoma. N. Eng. J. Med. 372, 2521–2532. doi: 10.1056/NEJMoa1503093
Rosenberg, J. E., Hoffman-Censits, J., Powles, T., van der Heijden, M. S., Balar, A. V., Necchi, A., et al. (2016). Atezolizumab in patients with locally advanced and metastatic urothelial carcinoma who have progressed following treatment with platinum-based chemotherapy: a single-arm, multicentre, phase 2 trial. Lancet 387, 1909–1920. doi: 10.1016/S0140-6736(16)00561-4
Seiwert, T. Y., Burtness, B., Mehra, R., Weiss, J., Berger, R., Eder, J. P., et al. (2016). Safety and clinical activity of pembrolizumab for treatment of recurrent or metastatic squamous cell carcinoma of the head and neck (KEYNOTE-012): an open-label, multicentre, phase 1b trial. Lancet Oncol. 17, 956–965. doi: 10.1016/S1470-2045(16)30066-3
Sharma, P., Retz, M., Siefker-Radtke, A., Baron, A., Necchi, A., Bedke, J., et al. (2017). Nivolumab in metastatic urothelial carcinoma after platinum therapy (CheckMate 275): a multicentre, single-arm, phase 2 trial. Lancet Oncol. 18, 312–322. doi: 10.1016/S1470-2045(17)30065-7
Shimizu, T., Seto, T., Hirai, F., Takenoyama, M., Nosaki, K., Tsurutani, J., et al. (2016). Phase 1 study of pembrolizumab (MK-3475; anti-PD-1 monoclonal antibody) in Japanese patients with advanced solid tumors. Invest. New Drugs 34, 347–354. doi: 10.1007/s10637-016-0347-6
Tie, Y., Ma, X., Zhu, C., Mao, Y., Shen, K., Wei, X., et al. (2017). Safety and efficacy of nivolumab in the treatment of cancers: a meta-analysis of 27 prospective clinical trials. Int. J. Cancer 140, 948–958. doi: 10.1002/ijc.30501
Topalian, S., Hodi, F., Brahmer, J., Gettinger, S., Smith, D., McDermott, D., et al. (2012). Safety, activity, and immune correlates of anti-PD-1 antibody in cancer. N. Eng. J. Med. 366, 2443–2454. doi: 10.1056/NEJMoa1200690
Topalian, S. L., Sznol, M., McDermott, D. F., Kluger, H. M., Carvajal, R. D., Sharfman, W. H., et al. (2014). Survival, durable tumor remission, and long-term safety in patients with advanced melanoma receiving nivolumab. J. Clin. Oncol. 32, 1020–1030. doi: 10.1200/JCO.2013.53.0105
Topalian, S. L., Taube, J. M., Anders, R. A., and Pardoll, D. M. (2016). Mechanism-driven biomarkers to guide immune checkpoint blockade in cancer therapy. Nat. Rev. Cancer 16, 275–287. doi: 10.1038/nrc.2016.36
Weber, J., D'Angelo, S., Minor, D., Hodi, F., Gutzmer, R., Neyns, B., et al. (2015). Nivolumab versus chemotherapy in patients with advanced melanoma who progressed after anti-CTLA-4 treatment (CheckMate 037): a randomised, controlled, open-label, phase 3 trial. Lancet. Oncol. 16, 375–384. doi: 10.1016/S1470-2045(15)70076-8
Weber, J., Gibney, G., Kudchadkar, R., Yu, B., Cheng, P., Martinez, A. J., et al. (2016). Phase I/II study of metastatic melanoma patients treated with nivolumab who had progressed after ipilimumab. Cancer Immunol. Res. 4, 345–353. doi: 10.1158/2326-6066.CIR-15-0193
Younes, A., Santoro, A., Shipp, M., Zinzani, P. L., Timmerman, J. M., Ansell, S., et al. (2016). Nivolumab for classical Hodgkin's lymphoma after failure of both autologous stem-cell transplantation and brentuximab vedotin: a multicentre, multicohort, single-arm phase 2 trial. Lancet Oncol. 17, 1283–1294. doi: 10.1016/S1470-2045(16)30167-X
Keywords: Anti-PD-1 antibodies, immune-related adverse events, immunotherapy, oncology, nivolumab
Citation: Wang P-F, Chen Y, Song S-Y, Wang T-J, Ji W-J, Li S-W, Liu N and Yan C-X (2017) Immune-Related Adverse Events Associated with Anti-PD-1/PD-L1 Treatment for Malignancies: A Meta-Analysis. Front. Pharmacol. 8:730. doi: 10.3389/fphar.2017.00730
Received: 25 August 2017; Accepted: 28 September 2017;
Published: 18 October 2017.
Edited by:
Hervé Emonard, University of Reims Champagne-Ardenne, FranceReviewed by:
Ursula Gundert-Remy, Charité Universitätsmedizin Berlin, GermanyCarlo Selmi, IRCCS Clinical Institute Humanitas, Italy
Copyright © 2017 Wang, Chen, Song, Wang, Ji, Li, Liu and Yan. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) or licensor are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Chang-Xiang Yan, yancx65828@sina.com
Ning Liu, liuning301@aliyun.com
†These authors have contributed equally to this work.