 Margaret McLean1
Margaret McLean1- 1 Clinical and Counselling Psychology, NHS Grampian, Aberdeen, UK
- 2 School of Medicine and Dentistry, University of Aberdeen, Aberdeen, UK
- 3 Clinical and Health Psychology Research Centre, University of Roehampton, London, UK
- 4 Unité de recherche INSIDE, Université du Luxembourg, Walferdange, Luxembourg
This paper describes a study investigating the provider–patient communication perceptions, experiences, needs, and strategies of doctors and nurses working together in a UK cancer setting. This was a qualitative study using individual interviews and focus group discussions. Interpretative phenomenological analysis was used to underpin data collection and analysis. Twenty-six staff participated in the project (18 nurses and 8 doctors). Both professional groups identified an inherent emotional strain in their daily interactions with patients. The strategies they adopted to reduce this strain fell into two main categories: (1) Handling or managing the patient to keep negative emotion at bay; and (2) Managing self to keep negative emotion at bay. These strategies allowed staff to maintain a sense of control in an emotionally stressful environment. Most believed that their communication skills were sufficient. In conclusion, communicating with and caring for cancer patients causes considerable psychosocial burden for doctors and nurses. Managing this burden influences their communication with patients. Without recognition of the need for staff to protect their own emotional well-being, communication skills training programs, emphasized in current UK cancer care guidelines, may have little impact on practice.
Introduction
Good, patient-centered communication is significantly associated with patient satisfaction, reduced anxiety and depression, and increased quality of life (Thorne, 1999; Dowsett et al., 2000; Arora, 2003; Hack et al., 2005). A good provider–patient relationship aids patient coping; enhances understanding and decision making; allows for better identification of patient needs, values, and expectations in regard to information and treatment; and reduces the possibility of complaints or litigation (Bredart et al., 2005; Mallinger et al., 2005).
While UK published guidelines and standards, including the National Health Service (NHS) Cancer Plan (Department of Health, 2000), the Cancer Reform Strategy (Department of Health, 2007), the Core Standards for Cancer Services (NHS Quality Improvement Scotland, 2008), and Better Cancer Care (Scottish Government, 2008) emphasize the need for good communication in cancer care, problems in communication are well documented in this area. Doctors and nurses often rely on their own judgment to assess patients’ needs (Arora, 2003; Hack et al., 2005) resulting in psychological morbidity and some physical symptoms, including the side-effects of treatment, being frequently under-recognized, and untreated (Ashbury et al., 1998; Maguire, 1999). Moreover, even when patients overtly disclose distress or physical complaints, staff frequently respond with avoidance or blocking behaviors (Wilkinson, 1991; Booth et al., 1996; Butow et al., 2002b). Consequently, staff ratings of patient quality of life and psychological distress are often inaccurate (Bredart et al., 2005).
A range of factors which contribute to the failures in communication in cancer units have been identified. These include patient reticence to engage with busy health professionals, the attitudes, and beliefs among doctors and nurses about the low priority and value of psychosocial communication, and institutional demands and practices which may inhibit good communication (Schofield et al., 2006). In addition, there is some evidence that oncology staff experience high levels of stress and that they maintain emotional distance with patients and relatives in order to protect themselves from this stress (Botti et al., 2006; Blomberg and Sahlberg-Blom, 2007; Ekedahl and Wengstrom, 2007).
With the centrality of multi-professional team in UK NHS cancer care, understanding of the communication process must consider the team as a whole (Cancer Service Collaborative, 2005): but no study to date has investigated the perceptions and experiences of both doctors and nurses within the same unit. Furthermore, although there may be some similarities, findings from the US and other countries cannot necessarily be transferred to other settings where the organization and delivery of care differ.
The aim of this study is to investigate the provider–patient communication perceptions, experiences, needs, and strategies of doctors and nurses working in a UK cancer setting.
Materials and Methods
Design
This was a qualitative study using individual interviews and focus group discussions. A qualitative approach was selected because rich descriptive data, not available through quantitative methods, were desired to document the doctors and nurses’ experiences, perceptions, needs, and strategies. Additionally, the close working relationships between staff suggested that the most complete understanding of participant perceptions and experiences could be obtained by interviewing both at the group and individual level as pre-existing groups often create shared meanings and perceptions through repeated interaction (Kitzinger, 2005; Millward, 2006), Focus groups were supplemented by individual interviews to ensure the views of a wide range of staff while acknowledging time constraints and clinical pressures.
Sample and Setting
The study was conducted in 2007 within a NHS cancer unit consisting of a large oncology ward and associated clinic, a hematology ward/clinic, and a nurse-led chemotherapy ward/clinic.
All doctors and nurses who worked within the unit were invited to participate in the study. Recruitment was by poster and email invitations. Staff who expressed interest in taking part were provided with written information about the study, including how confidentiality would be protected, and that participation was entirely voluntary. Written consent was obtained from all participants in advance of data collection.
Data Collection
All interviews and focus groups took place in the ward or clinic environment in which the staff worked to enhance the sense of control and ease among participants (Green and Thorogood, 2004). Interviews were conducted by the first author, who although not trained in focus group facilitation, had training in conducting therapeutic and psychoeducational groups.
The interview schedule, used for both individual interviews and focus groups, was designed with reference to relevant literature about the difficulties in patient–professional communication. Questions related to perceived roles in communicating with patients, how decisions were reached about how/what to communicate, the challenges they faced and how they coped with these, how they assessed for psychological distress (if at all), and what further training or ongoing support was wanted. Particular focus was placed on the experience of professionals in providing information and psychosocial support to patients, and on the exploration of variation of themes across doctors and nurses, and groups. A copy of the interview schedule is available on request from the corresponding author.
Theoretical Approach
Interpretative phenomenological analysis (IPA) was chosen for this study. This approach, rooted within the wider tradition of phenomenology but also drawing from symbolic interactionism and hermeneutics, is increasingly used in healthcare research (Biggerstaff and Thompson, 2008). IPA is concerned with the “lived experience” of individuals and how individuals make sense of their experiences. It is therefore concerned with subjective meanings rather than attempting to create objective accounts of phenomena. However, as in social interactionism, IPA recognizes that meanings are always created through interaction, including interaction with the researcher and research process. Smith and Eatough (2006) refer to this process as a double-hermeneutic in which “the participants are trying to make sense of their world (and) the researcher is trying to make sense of the participants trying to make sense of their world.” (p. 324). Thus IPA draws on hermeneutics (the theory of interpretation) and is both descriptive and interpretative, requiring both empathy and critical analysis. Although most IPA studies have used individual interviews, Millward (2006) suggests that, individual experiences and perceptions can be “parsed out” from the group as long as each group member is adequately engaged in the discussion process.
Data Analysis
Interviews and focus groups were transcribed verbatim and checked for accuracy before being imported into NVivo7 [QSR International (2006), Melbourne: QSR International Ltd.]. MMcL, a counseling psychologist working in oncology, carried out the coding and interpretation of the data. A step-by-step analysis of the data was followed (Dean et al., 2006). All transcripts were read through twice before the first transcript was analyzed. During the third reading, anything considered significant was coded (Smith and Osborn, 2003). At this stage, some text was assigned to more than one code when more than one description could be made, and queries about the meaning of what was being said were recorded in linked-text memos. This process was repeated for two further transcripts.
Each theme was then carefully scrutinized. In depth, iterative exploration of the data led to the creation of other themes which became part of the master list. This list was then used to code subsequent transcripts from which new themes emerged which, in turn, led to further scrutiny and refinement of the master list. Throughout the process of analysis, codes were examined and debated among the authors to reach agreement about what themes most accurately represented participants’ accounts. The final stage of analysis required the master list to be distilled into a concise list of overarching “domains,” each of which contained a small number of subordinate themes.
Ethics Permission
Ethics approval was obtained from the Ethics Boards of the NHS Trust and University through which this study was undertaken.
Results
Participants
A total of 34 staff volunteered to participate in the study and of these, 26 were recruited on the basis of availability during the data collection period. The number recruited was approximately 25% of the total number of doctors and nurses employed within the unit. Participant demographic data is provided in Table 1.
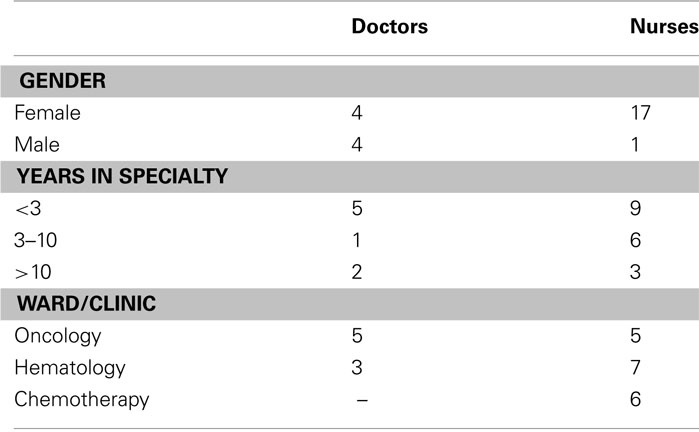
Table 1. Participant demographics (n = 26).
Eight individual interviews (three consultants, the oncology SpR, two charge nurses, one nurse from each ward) and six focus groups were carried out. Most interviews came after the focus groups, in order to obtain views of those unable to attend the group interviews. Interviews lasted on average for 50 min. Data is presented by focus group or interview, with participants also numbered within focus groups (e.g., participant 3-2 is participant number 2 in focus group 3).
Findings
Unfortunately, the numbers in the study do not allow for detailed comparison between colleagues with different levels of work experience, or areas of specialism, or who worked in different parts of the unit. However, in general, there was little variation in responses between specialisms. Nurses tended to feel less confident about their communication skills then doctors, even though both professional groups avoided discussions about psychosocial issues, as discussed below. Indeed, there was wide overlap among the range of staff in the practices and attitudes adopted, which were most explicitly articulated through focus groups discussions compared with individual interviews.
Four domains were identified in the data and three of these domains contained subordinate themes. Table 2 summarizes these domains and themes.
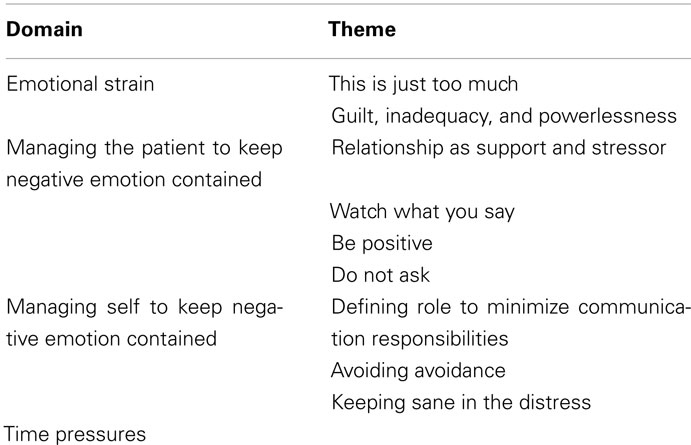
Table 2. Summary of domains and themes.
Domain 1: Emotional Strain
All participants acknowledged the emotional strain of working with patients with cancer. This constant strain influenced all aspects of communication. It resulted from close contact with the relentless suffering of patients and families and from participants’ sense of powerless to relieve this suffering.
Theme 1: This is just too much
Staff discussed the need to shield themselves emotionally by creating communication boundaries and avoiding emotional attachments with patients and families. Most believed that they had learned to deal with the emotional toll of communication and minimize its effect.
Theme 2: Guilt, inadequacy, and powerlessness
A pervasive theme was the vulnerability of staff to feelings of guilt or inadequacy when they felt powerless. Difficulties were expressed over having to witness patients becoming increasingly ill or dying.
because of the nature of the illnesses we’re dealing with there are often times when you think – am I doing the right thing here – what are we doing to these people? (Nurse 5-2)
Staff also spoke of feeling guilty and helpless when they did not have the time, information, or resources to meet patients’ needs. Guilt also arose about being fit and healthy when patients were seriously ill. Feelings of inadequacy, helplessness, and guilt were associated directly with difficulties in communicating with patients.
Once it starts to get a bit deeper and you know they’re dying, then you are constantly thinking, well what am I going to say here? What are they going to say next? (Nurse 4)
Domain 2: Handling or Managing the Patient to Keep Negative Emotion Contained
A major concern of staff was how to carry out tasks without becoming too involved with patients and becoming emotionally burdened by any involvement. Handling the patient in such a way as to minimize the emotional exchange was a key consideration in almost all communication.
Theme 1: Relationship as support and stressor
Staff derived satisfaction from the relationships they built with patients, partly because through them, they could help patients feel less anxious and more secure. However, relationships were also inherently risky for staff because of the potential of attachment with the patient. Rapport was primarily achieved by providing patients with information and reassurance. Asking patients about how they were coping or providing direct emotional support were not identified as key ingredients in building rapport.
Staff found it easiest to build rapport with those patients who were least distressed. Important factors were the degree to which patients had a positive outlook or, if in the final stages of illness, the degree of acceptance they had reached about their situation.
When there’s still hope and a positive attitude amongst the patients as well, then it’s easier then. But once they get really low and they’ve given up then it’s more difficult. (Nurse 3-3)
Walking the tightrope of balancing their desire to build relationships and their need to maintain distance was a source of strain for participants. The dilemma faced about ensuring their own self protection, particularly in light of the sheer number of patients for which they were responsible and the time pressures under which they operated, could be a constant daily struggle.
It’s sort of self preservation in a way isn’t it? You want to give them the support but if you get too involved it becomes like an even bigger burden on your shoulders and you’ve got x amount of other patients to look after (Nurse 1)
Theme 2: Watch what you say
A common concern for staff in their communication with patients was that they would say “the wrong thing” which might cause distress for the patient or family. They were fearful of revealing something that patients neither knew nor wanted to know or finding themselves face to face with patients’ emotions or questions for which they felt ill-prepared. This was particularly true for nurses and junior doctors.
It would be quite easy to put your foot in it and mention a word that perhaps they haven’t heard about before. (Nurse 2-2)
Nevertheless, the vast majority of participants felt happy about their ability to provide information in a way that was understandable and sensitive to patients’ needs although they usually reported relying on their own judgments and assumptions about these needs rather than enquiring directly.
You’ll maybe see them for fifteen minutes while you’re taking clinical history and then you’ll examine them … you have a fair idea of how you can pitch it in terms of what you can tell and often it’s not really a very conscious process. It’s something that I would do automatically without thinking about it at all. (Consultant 1)
While acknowledging that each patient was different, there were indications that the manner in which participants delivered information was a “one size fits all” approach. Many described a style of providing information that avoided the uncertainty and complexity of having to ascertain what any individual needed or wanted. This allowed them to maintain a degree of distance from the patient.
Theme 3: Be positive
A common strategy staff used to contain patients’ distress was to adopt a positive perspective. Often, they believed that this was what patients wanted and that by being economical with the truth, they were allowing patients to maintain hope.
I mean I think that they are worried that they are going to die and they’re right … I think we are quite good at trying to empathise the positive outcomes and to keep people focused on the likely positive outcome of what can happen but I think we do see it as one of our jobs to allay their worries. (C 1)
Participants suspected that they were ignoring patients’ distress because maintaining a cheerful outlook was a coping strategy for them, one that intentionally made them less responsive to patient needs.
I don’t know whether that’s a defence mechanism for ourselves as well. If you’re pessimistic they’re going to need more counselling and we simply don’t have the time. (Nurse 3-3)
Theme 4: Do not ask
Another way that staff contained patient distress was to avoid asking questions which might elicit distress. Most staff said that they would generally only enquire about a patient’s worries or concerns if the patient was visibly upset and would shy away from exploring an emotional issue in depth.
I’m sure what I do is agree with them. I would never try and say no, that’s not right. I say yeah, but not go further… I suppose you just don’t pursue it (Nurse 5-2)
Reasons for this reluctance to engage with patients’ distress included lack of time, and fear of starting conversations which they could not control and which might therefore impede on their work schedule. Both doctors and nurses saw their work as task orientated. Their priority was on the physical and technological aspects of illness and care and they were disinclined to engage in a discussion that might divert them from this focus. There was some evidence that the focus on physical care provided some security in the face of endless patient needs.
it would be great to go round the patients and ask how are you feeling, you got a bit of bad news recently, what’s been happening?, but most of the time you have got to deal with the day to day running of the ward. (SHO 1-1)
Because many patients did not openly discuss their distress or concerns, most staff assumed that these discussions were not wanted. Staff did not consider how their own task orientation and lack of active enquiry might be affecting patients’ willingness to communicate with them.
Sometimes they will tell you something and other times they’ll show some emotion and then quickly they’ll retract within themselves and say Oh, I’m fine, it’s OK. And that’s obviously saying, well to me, it’s saying no I don’t want to talk about this anymore. (Nurse 2)
Domain 3: Managing Self to Keep Negative Emotion Contained
In addition to coping with the emotionally charged ward/clinic environment by attempting to control or contain their relationships with patients, participants also adopted beliefs and behaviors which served the function of keeping their own negative emotion contained.
Theme 1: Defining role to minimize communication responsibilities
Participants blocked patients from expressing distress by not enquiring directly about their feelings and/or by creating a cheerful atmosphere. They did not view these strategies as failing patients or leaving patients with unmet support needs as they believe the wider team addressed patients’ needs even if they were not personally doing so. Doctors believed that, if a patient was anxious or depressed, then this would be detected by the nursing staff. They saw their own role as dealing with medical matters while nurses (or other staff such as chaplains, occupational therapists, etc.) had the role of speaking with patients about wider concerns.
I think the patients probably develop some sort of schema for who they think they should discuss certain things with. I think senior doctors are probably bottom of the list when it comes to things that are considered a bit touchy-touchy (Consultant 1)
In a similar manner, nurses also delegated the responsibility for speaking with patients to other professional groups including auxiliaries and chaplains, indicating that there was little team discussion about where responsibility was placed.
The auxiliary does spend more quality time with patients than we do and they will tell you all sorts of stuff that you never knew (CN 2)
Both doctors and nurses relied on the clinical nurse specialists (CNSs) to support patients emotionally as the CNSs were seen as having more time and skills.
We tend to actually refer them to the specialist nurse or the Macmillan team to do the emotional side of things. (Nurse 3-1)
Theme 2: Avoiding avoidance
There was a general sense of satisfaction with the communication with patients and a general belief that the information and emotional needs of patients were sufficiently addressed.
When people are having difficulties or worried about something, I don’t think anyone here would ignore it. (SHO 2-1)
At the same time, when staff (usually nurses) did reflect on the possibility that they might be failing to address patients’ needs by avoiding emotionally focused discussions, some expressed feelings of guilt (particularly if they believed this avoidance was due to their own self protection), or frustration (toward external constraints such as competing demands). However, there was also a widespread belief that anxiety and depression was very uncommon among patients and that, if present, it would be detected by staff.
I don’t think that there’s anything that I have come across personally that I would think, oh I need to sit down one to one or in a small group to discuss. (Nurse 4)
Few staff felt that they had any need for further training in communication or psychosocial assessment skills.
Theme 3: Keeping sane in the face of distress
Many staff emphasized the importance of being able to “switch off” from the work in order to prevent emotional overload and burnout. There were a number of personal strategies identified as a means of dealing with this stress, including exercise, socializing, and the development of perspective in one’s own life.
You learn to switch off. (Nurse 3-3)
Virtually all participants mentioned the unit’s internal support system: they valued being able to speak with each other openly about their emotional reactions.
Without even realising they do it, I think people counsel each other all the time on this ward. Every day we counsel each other in a very informal way. It’s nice just being there because it’s actually quite a friendly place. (Nurse 2-2)
Only a small minority expressed a desire for more formal support systems such as supervision or team debriefing sessions.
Domain 4: Time Pressures
The greatest pressure identified by participants was shortage of time. Staff felt that they were always busy and having time to communicate with patients was generally considered as something “nice” to do, but not an essential component of care.
I think again it’s the time thing. I think it’s nice to be able to do that and it should be done really, how much time can you spend doing things like, it’s the time aspect that is the problem. (SpR)
Nevertheless, many staff also recognized that they avoided conversations with patients for other reasons, particularly because of fears of losing control and feeling out of their depth. When staff were able to overcome these fears, it seemed that they were more willing to enter into conversations proactively, indicating that time was not the only barrier to communication.
But when you do sit and talk and someone opens up to you it really doesn’t take that long. You just have to make the time and get more confident in doing it (Nurse 3-2)
Discussion
This study investigated provider–patient communication in a cancer unit. The data indicated that doctors and nurses working in this environment communicated with their patients in a predominantly professional-centered way, in which they control the level of intimacy with patients in order to protect themselves from emotional distress. The ways in which they control communication minimizes, and indeed avoids, identifying and addressing the psychological care needs of patients, as has been found in other studies (Wilkinson, 1991; Booth et al., 1996; Arora, 2003). The focus of patient care was on the more technical aspects of cancer care.
The fact that cancer is often highly anxiety-provoking for patients is well documented (Mills and Sullivan, 1999; Evans et al., 2005). This study adds that communicating with and caring for cancer patients also causes considerable psychosocial burden for doctors and nurses, and (minimizing) this burden influences their communication with patients. The reasons for this are understandable – emotional attachment heightens staff vulnerability to distress as patients deteriorate [(Blomberg and Sahlberg-Blom, 2007). However, participants denied avoiding emotional attachment with patients through use of communication strategies (e.g., optimism; Delvecchio Good and Good, 1990; Jarrett and Payne, 2000), avoidance, task focus (Blomberg and Sahlberg-Blom, 2007; Ekedahl and Wengstrom, 2007), regarding communication as someone else’s job, denial of the prevalence of patients’ emotional distress] – perhaps in itself demonstrating how effectively they had created emotional boundaries to enable them to function effectively. Those interviewed had a high level of satisfaction with their communication skills and practice, believed patients had the same perception, and did not see the need for further training on provider–patient communication. Participants could not easily reflect on the potential impact on patients of the psychosocial neglect resulting from their communication strategies.
There was a tension between maintaining emotional distance yet having level of relationship with patients. Some level of relationship was necessary to participants feeling that they were contributing positively to patients’ well-being. This contributed to their feelings of control and power and helped to ease their own feelings of vulnerability (Chant et al., 2002; Corner, 2002). Furthermore, it seemed that task focus provided staff with a sense of utility in an environment in which a sense of futility abounded. Although completing the workload was another source of stress, it provided staff with clear boundaries about their role and function (as well as minimizing the time available for communication with patients). In fact, despite recognition that optimal care was not just disease management, there was little value placed on psychosocial care which was often equated with not getting on with work or “doing nothing” (Corner, 2002).
We must also acknowledge potential participant bias: only those with an interest in the topic under discussion may have volunteered to take part in the study. Participants’ accounts are also likely to have been influenced by whether they were interviewed individually or in focus groups (which are infrequently used in IPA studies).
The practice of professional-centered communication within oncology settings is well documented. This study demonstrates that, from the point of view of doctors and nurses, there is good reason for poor provider–patient communication. The emotional toll of cancer care is not only a patient phenomena – minimizing their own emotional distress underpins staff communication with patients. An underlying principle in their interaction, therefore, is to maintain distance and to control the expression of patient distress. Their own vulnerability to negative emotion is further protected by minimizing their awareness of the detrimental consequences of this strategy for patient care.
This is one study from a single unit, in a particular national health system. The findings may be reflective of the particular unit and may not generalize across other cancer settings. However, the results are in agreement with previous research from other countries (e.g., Blomberg and Sahlberg-Blom, 2007; Botti et al., 2006; Ekedahl and Wengstrom, 2007) suggesting that the findings and the interpretations made of them reach beyond the local context. However, comparative work in other NHS settings is required to explore this phenomenon further. Exploration of how patients might perceive their caregivers attitudes is also required.
There are practice implications to our findings. Staff needs are an essential element in communication and must be addressed if communication is to improve (Feldman-Stewart et al., 2005) but the UK guidelines advocating communication skills training do not recognize this very real issue (Department of Health, 2007; NHS Quality Improvement Scotland, 2008). The findings from this study indicate an urgent need to develop a framework to provide doctors and nurses with both skill development and ongoing support in order to improve their ability to integrate psychosocial aspects of care and optimize patient outcomes. Attempts to improve communication practice are unlikely to be successful through skills training alone and should take staff need for self protection as a starting point. Indeed, although lack of confidence in communication skills and inadequate skills training have been have been identified as risk factors in burnout amongst doctors (Ramirez et al., 1995), evidence about the effectiveness of skills training has only been undertaken with self selected participants who are likely to take greater interest in communication (e.g., Fallowfield et al., 2002). Mandatory communication training has not had the same success (Merckaert et al., 2005), potentially because of stronger self protection strategies among this group.
Conflict of Interest Statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Acknowledgments
Our thanks to NHS Grampian for supporting this research, and to the healthcare professionals who took part in the study.
References
Arora, N. K. (2003). Interacting with cancer patients: the significance of physicians’ communication behaviour. Soc. Sci. Med. 57, 791–806.
Ashbury, F., Findlay, H., Reynolds, B., and McKerracher, K. (1998). A Canadian survey of cancer patients’ experiences: are their needs being met? J. Pain Symptom Manage. 16, 298–306.
Biggerstaff, D., and Thompson, A. (2008). Interpretative phenomenological analysis (APA): a qualitative methodology of choice in healthcare research. Qual. Res. Psychol. 5, 173–183.
Blomberg, K., and Sahlberg-Blom, E. (2007). Closeness and distance: a way of handling difficult situations in daily care. J. Clin. Nurs. 16, 244–254.
Booth, K., Maguire, P. M., Butterworth, T., and Hilher, V. F. (1996). Perceived professional support and the use of blocking behaviours by hospice nurses. J. Adv. Nurs. 24, 522–527.
Botti, M., Endacott, R., Watts, R., Cairns, J., Lewis, K., and Kenny, A. (2006). Barriers in providing psychosocial support for patients with cancer. Cancer Nurs. 29, 309–316.
Bredart, A., Bouleuc, C., and Dolbeault, S. (2005). Doctor-patient communication and satisfaction with care in oncology. Curr. Opin. Oncol. 14, 351–354.
Butow, P., Brown, R. F., Cogar, S., and Tattersall, M. H. N. (2002b). Oncologists’ reactions to cancer patients’ verbal cues. Psychooncology 11, 47–58.
Cancer Service Collaborative. (2005). How to Guide: Achieving Cancer Waiting Times. Leicester: Cancer Service Collaborative.
Chant, S., Jenkinson, T., Randle, J., and Russell, G. (2002). Communication skills: some problems in nursing education and practice. J. Clin. Nurs. 11, 12–21.
Dean, S., Smith, J., and Payne, S. (2006). “Low back pain: exploring the meaning of exercise management through interpretative phenomenological analysis,” in Qualitative Research for Allied Health Professionals: Challenging Choices, eds L. Finlay, C. Ballinger, and J. Wiley (Chichester: John Wiley & Sons).
Delvecchio Good, M., and Good, B. (1990). American oncology and the discourse of hope. Cult. Med. Psychiatry 14, 59–79.
Department of Health. (2000). The NHS Cancer Plan: A Plan for Investment, A Plan for Reform. London: Department of Health.
Dowsett, S. M., Saul, J. L., Butow, P. N., Dunn, S. M., Boyer, M. J., Findlow, R., and Dunsmore, J. (2000). Communication styles in the cancer consultation: preferences for a patient-centered approach. Psychooncology 9, 147–156.
Ekedahl, M., and Wengstrom, Y. (2007). Nurses in cancer care – stress when encountering existential issues. Eur. J. Oncol. Nurs. 11, 228–237.
Evans, D., Sharney, D., Lewis, L., Golden, R. N., and Gorman, J. M. (2005). Mood disorders in the medically ill: scientific review and recommendations. Biol. Psychiatry 58, 175–189.
Fallowfield, L., Jenkins, V., Farewell, V., and Saul, J. (2002). Efficacy of a cancer research UK communication skills training model for oncologists: a randomised controlled trial. Lancet 359, 650–657.
Feldman-Stewart, D., Brundage, M. D., and Tishelman, C. (2005). A conceptual framework for patient-professional communication: an application to the cancer context. Psychooncology 14, 801–809.
Hack, T., Degner, L., and Parker, P. (2005). The communication goals and needs of cancer patients: a review. Psychooncology 14, 831–845.
Jarrett, N. J., and Payne, S. A. (2000). Creating and maintaining ‘optimism’ in cancer care communication. Int. J. Nurs. Stud. 37, 81–90.
Kitzinger, J. (2005). “Focus group research: using group dynamics to explore perceptions, experiences and understandings,” in Qualitative Research in Healthcare, ed. I. Holloway (Maidenhead: O. U. Press), 56–70.
Mallinger, J. B., Griggs, J. J., and Shields, C. G. (2005). Patient-centered care and breast cancer survivors’ satisfaction with information. Patient Educ. Couns. 57, 342–349.
Merckaert, I., Libert, Y., and Razavi, D. (2005). Communication skills training in cancer care: where are we and where are we going? Curr. Opin. Oncol. 17, 319–330.
Mills, M., and Sullivan, K. (1999). The importance of information giving with patients newly diagnosed with cancer: a review of the literature. J. Clin. Nurs. 8, 631–642.
Millward, L. J. (2006). “Focus groups,” in Research Methods in Psychology, 3rd Edn, eds G. M. Breakwell, S. Hammond, C. Fife-Schaw, and J. A. Smith (London: Sage), 276–299.
NHS Quality Improvement Scotland. (2008). Management of Core Cancer Services. Available at: http://www.healthcareimprovementscotland.org/programmes/cancer_care_improvement/cancer_resources/standards_ for_cancer_services.aspx
Ramirez, A. J., Graham, J., Richards, M. A., Cull, A., Gregory, W. M., Leaning, M. S., Snashall, D. C., and Timothy, A. R. (1995). Burnout and psychiatric disorder among cancer clinicians. Br. J. Cancer 71, 1263–1269.
Schofield, P., Carey, M., Bonevski, B., and Sanson-Fisher, R. (2006). Barriers to the provision of evidence-based psychosocial care in oncology. Psychooncology 15, 863–872.
Smith, J. A., and Eatough, V. (2006). “Interpretative phenomenological analysis,” in Research Methods in Psychology, 3rd Edn, eds G. M. Breaknell, S. Hammond, C. Fife-Schaw, and J. Smith (London: Sage), 322–341.
Smith, J. A., and Osborn, M. (2003). “Interpretative phenomenological analysis,” in Qualitative Psychology: A Practical Guide to Research Methods, ed. J. A. Smith (London: Sage), 51–79.
Thorne, S. (1999). Communication in cancer care: what science can and cannot teach us. Cancer Nurs. 22, 370–379.
Keywords: cancer – communication, physician and patient, nurse and patient, oncology, stress (psychology), IPA
Citation: McLean M, Cleland JA, Worrell M and Vögele C (2011) “What am i going to say here?” The experiences of doctors and nurses communicating with patients in a cancer unit. Front. Psychology 2:339. doi: 10.3389/fpsyg.2011.00339
Received: 25 August 2011;
Accepted: 01 November 2011;
Published online: 30 November 2011.
Edited by:
Chris J. Gibbons, University of Liverpool, UKReviewed by:
Chris J. Gibbons, University of Liverpool, UKBeth Grunfeld, University of Birmingham, UK
Copyright: © 2011 McLean, Cleland, Worrell and Vögele. This is an open-access article subject to a non-exclusive license between the authors and Frontiers Media SA, which permits use, distribution and reproduction in other forums, provided the original authors and source are credited and other Frontiers conditions are complied with.
*Correspondence: Jennifer A. Cleland, Division of Medical and Dental Education, University of Aberdeen, Polwarth Building, Foresterhill, Aberdeen AB25 2ZD, UK. e-mail: jen.cleland@abdn.ac.uk