 Katarina Howner1,2*
Katarina Howner1,2* Peter Andiné3,4,5
Peter Andiné3,4,5 Göran Engberg6
Göran Engberg6 Emin Hoxha Ekström7
Emin Hoxha Ekström7 Eva Lindström8Mikael Nilsson7
Eva Lindström8Mikael Nilsson7 Susanna Radovic9
Susanna Radovic9 Monica Hultcrantz7
Monica Hultcrantz7- 1Department of Clinical Neuroscience, Centre of Psychiatry Research, Karolinska Institutet, Stockholm, Sweden
- 2Department for Forensic Psychiatry, National Board of Forensic Medicine, Stockholm, Sweden
- 3Department for Forensic Psychiatry, National Board of Forensic Medicine, Gothenburg, Sweden
- 4Centre for Ethics, Law and Mental Health, Department of Psychiatry and Neurochemistry, Institute of Neuroscience and Physiology, The Sahlgrenska Academy at University of Gothenburg, Gothenburg, Sweden
- 5Forensic Psychiatric Clinic, Sahlgrenska University Hospital, Gothenburg, Sweden
- 6Department of Physiology and Pharmacology, Karolinska Institutet, Stockholm, Sweden
- 7Swedish Agency for Health Technology Assessment and Assessment of Social Services (SBU), Stockholm, Sweden
- 8Department of Neuroscience, Psychiatry, Uppsala University, Uppsala, Sweden
- 9Department of Philosophy, Linguistics, Theory of Science, University of Gothenburg, Gothenburg, Sweden
Background: Pharmacological treatment is of great importance in forensic psychiatry, and the vast majority of patients are treated with antipsychotic agents. There are several systematic differences between general and forensic psychiatric patients, e.g. severe violent behavior, the amount of comorbidity, such as personality disorders and/or substance abuse. Based on that, it is reasonable to suspect that effects of pharmacological treatments also may differ. The objective of this systematic review was to investigate the effects of pharmacological interventions for patients within forensic psychiatry.
Methods: The systematic review protocol was pre-registered in PROSPERO (CRD42017075308). Six databases were used for literature search on January 11, 2018. Controlled trials from forensic psychiatric care reporting on the effects of antipsychotic agents, mood stabilizers, benzodiazepines, antidepressants, as well as pharmacological agents used for the treatment of addiction or ADHD, were included. Two authors independently reviewed the studies, evaluated risk of bias and assessed certainty of evidence using Grading of Recommendations Assessment, Development and Evaluation (GRADE).
Results: The literature search resulted in 1783 records (titles and abstracts) out of which 10 studies were included. Most of the studies included were retrospective and non-randomized. Five of them focused on treatment with clozapine and the remaining five on other antipsychotics or mood stabilizers. Five studies with a high risk of bias indicated positive effects of clozapine on time from treatment start to discharge, crime-free time, time from discharge to readmission, improved clinical functioning, and reduction in aggressive behavior. Psychotic symptoms after treatment were more pronounced in the clozapine group. Mainly due to the high risk of bias the reliability of the evidence for all outcomes was assessed as very low.
Conclusion: This systematic review highlights the shortage of knowledge on the effectiveness of pharmacological treatment within forensic psychiatry. Due to very few studies being available in this setting, as well as limitations in their execution and reporting, it is challenging to overview the outcomes of pharmacological interventions in this context. The frequent use of antipsychotics, sometimes in combination with other pharmacological agents, in this complex and heterogeneous patient group, calls for high-quality studies performed in this specific setting.
Introduction
Rationale
In most jurisdictions mentally disordered offenders are given special treatment within the legal system. A criminal offender who due to a mental disorder is judged as not accountable (or legally insane) is generally considered as not responsible for his offence and hence not sentenced to a criminal sanction. In most cases such a person is, if the crime is severe and there is a great need for psychiatric care, transferred to compulsory psychiatric care (1, 2). Sweden, is one of a few exceptions, here all criminal offenders are considered responsible for their actions and forensic psychiatric care is a criminal sanction. Regardless of criminal law regulations, compulsory psychiatric care for mentally disordered offenders is often given in special forensic psychiatric institutions. Most patients have committed violent offences, leading to a potentially high risk of aggression and violent behavior within the care institution. As a result, the staffing levels in forensic wards are high compared to general psychiatric in-patient care. These circumstances result in high care costs, and forensic psychiatry often represents a large part of the overall psychiatry budget, while the population is rather small in terms of the number of patients (3).
There are a number of systematic differences between the forensic psychiatric patients and the general psychiatric patients. Firstly, forensic patients are not only patients but also offenders, in many cases offenders of severe violence (4). Even though violent behavior in an acute non-forensic setting is frequently occurring, in the forensic setting many patients have a history of more severe violence and disruptive behavior (5). Therefore, managing aggression and violent behavior are of special concerns here. The responsible clinician must not only consider the patients’ well-being, but also bear in mind the protection of society from potentially violent mentally disordered offenders (6). Secondly, in the forensic setting, all patients are involuntarily admitted and under compulsory treatment which could affect the process of shared decision making and compliance with treatment over time. Even if compulsory care also appears in general psychiatry, the majority of the psychiatric patients is under voluntary treatment. A third difference is the length of inpatient care, since in forensic psychiatric care the duration often lasts years compared to the general psychiatric care, in which the duration of inpatient care mainly is days to months. Another difference is that the proportion of comorbidity is higher compared to general psychiatry (7, 8). Psychotic disorders are the most frequent primary diagnosis in this population, but comorbidity such as personality disorders, substance abuse and neuropsychological disorders, are more common here, compared to in general psychiatry. In the light of these differences it is plausible that effects of pharmacological treatments could differ between the forensic and the general psychiatric setting.
The vast majority of patients in forensic psychiatry are treated with pharmacological agents (9). Psychotic disorders are well represented within the forensic psychiatric population, and pharmacological treatment with antipsychotics is crucial in this regard (10, 11). When comparing the use of traditional versus atypical antipsychotics in Sweden, we found that it was more common to use traditional antipsychotics in the forensic setting and also that combinations of several antipsychotic agents were more frequent (12). A few systematic reviews relevant to the field have been published. A recent review (13) emphasizes the value of clozapine in the treatment of violent and aggressive behaviors also in a forensic population. Another recent study (14) identified two previously published systematic reviews, which in part addressed the effects of pharmacological interventions within forensic psychiatry (15, 16), showing that only a few primary studies had been published, all of which were assessed as being at high risk of bias. However, the reports had methodological limitations and could potentially have resulted in relevant records having been overlooked. Also, and more importantly, as the last literature searches were performed in 2010 (16) and 2012 (15) respectively, an update is needed to ensure that research published over the previous six years is included.
Based on the fact that the general and forensic psychiatric populations differ in many respects, it is reasonable to suspect that effects of pharmacological treatments also may differ. Since there may be relevant studies from the forensic setting published since the latest systematic reviews in the field, we aimed to perform an updated systematic review, searching for pharmacological intervention studies in the specific forensic psychiatric setting.
Objective
The aim of this systematic review was to investigate therapeutic effects and side effects of pharmacological treatment within forensic psychiatry, with a focus on outcomes important to patients as well as society. When searching for relevant literature we chose to focus specifically on forensic psychiatric patients with psychotic disorders, personality disorders, autism spectrum disorders and substance use disorders, as these are the most common diagnoses in this setting.
Materials and Methods
Protocol and Registration
This systematic review was conducted at The Swedish Agency for Health Technology Assessment and Assessment of Social Services (SBU), and a Swedish version was submitted to the Swedish Ministry of Social Affairs (www.sbu.se/258) in June 2018. A peer-reviewed protocol, including pre-specified objectives, was registered in PROSPERO (http://www.crd.york.ac.uk/PROSPERO/display_record.php?ID=CRD42017075308). The systematic review process follows the general concepts covered by PRISMA (17).
Eligibility Criteria
We included studies of adult offenders (over 15 years of age, since that is the cut off for criminal responsibility in Sweden) with severe mental disorder, including psychotic disorders, autism spectrum disorders or personality disorders, in forensic psychiatric care. The interventions were antipsychotic agents, mood stabilizers, benzodiazepines and benzodiazepins-like agents, pharmacological addiction treatment, pharmacological ADHD-treatment, and antidepressants. All primary studies with a control group were included without restrictions as to study type. We tried to include a wide range of different outcomes: symptoms of psychosis (clinical functioning), aggression and violent behavior, adverse events, mortality, reoffending (both violent acts and non-violent offences), mental and physical health, time outside the hospital before readmission, quality of life, and long-term compliance to treatment.
Search Strategy
The literature search was performed by an information specialist and included the databases Cinahl, Cochrane, EMBASE, PsycINFO, PubMed, and Scopus. The search covered studies published in English, Swedish, Norwegian or Danish up to January 11, 2018. In addition, references from narrative reviews and articles published in international journals, not identified in the main search, were also included. This by going through reference list from the articles found in the main search. Grey literature, such as conference abstracts or dissertations, were excluded. Electronic searches were conducted using Medical Subject Headings (MeSH) and relevant text word terms. The detailed search strategy can be found in Supplementary Material.
Study Selection
Two reviewers independently screened the titles and abstracts identified by the search strategy. All studies of potential relevance according to the inclusion criteria were obtained in full text and two reviewers independently assessed them for inclusion. Any disagreement was resolved by discussions, with involvement of a third review author, when necessary.
Risk of Bias in Individual Studies
Two reviewers independently assessed the risk of bias with the use of tools developed for randomized and non-randomized controlled trials, including signaling questions to address selection bias, performance bias, detection bias, reporting bias and bias due to conflicts of interest. The tools for assessing risk of bias in individual studies were developed at SBU (18) and focus on the same aspects that are included in international guidelines for reporting standards (19, 20). Before starting the assessments, the questions were thoroughly discussed so that all reviewers had a common understanding as to how these criteria could affect the results in this specific research area. Each study was rated as having a low, moderate or high risk of bias.
Data Collection Process
From each included study data were extracted and inserted into tables by one reviewer, followed by auditing of the data extraction by another reviewer. Any disagreement was resolved by discussion. Information concerning study design, setting, population, intervention, control group, outcome and results were extracted from each included study.
Data Analysis
We anticipated that there would be limited scope for meta-analysis because of the range of different outcomes measured across the small number of existing trials. However, if studies would have used the same type of intervention and comparator, with equal outcome measures, we would have pooled the results using a random-effects meta-analysis. The certainty of the evidence for each outcome was assessed using Grading of Recommendations Assessment, Development and Evaluation (GRADE) (21) and we followed the suggested criteria for using GRADE presented on the GRADE working group website (www.gradeworkinggroup.org).
Results
Study Selection and Characteristics
The systematic literature search resulted in 1783 records (titles and abstracts), out of which 10 studies fulfilled the inclusion criteria. The primary reasons for exclusion of studies were that the studied populations were not treated within a forensic setting or the studies did not evaluate the effect of an intervention (list of excluded full-text studies with reasons for exclusion are available on request). All 10 included studies (22–31) were assessed as having a high risk of bias, primarily due to selection bias. The review process and number of reviewed articles are summarized in the flow diagram in Figure 1.
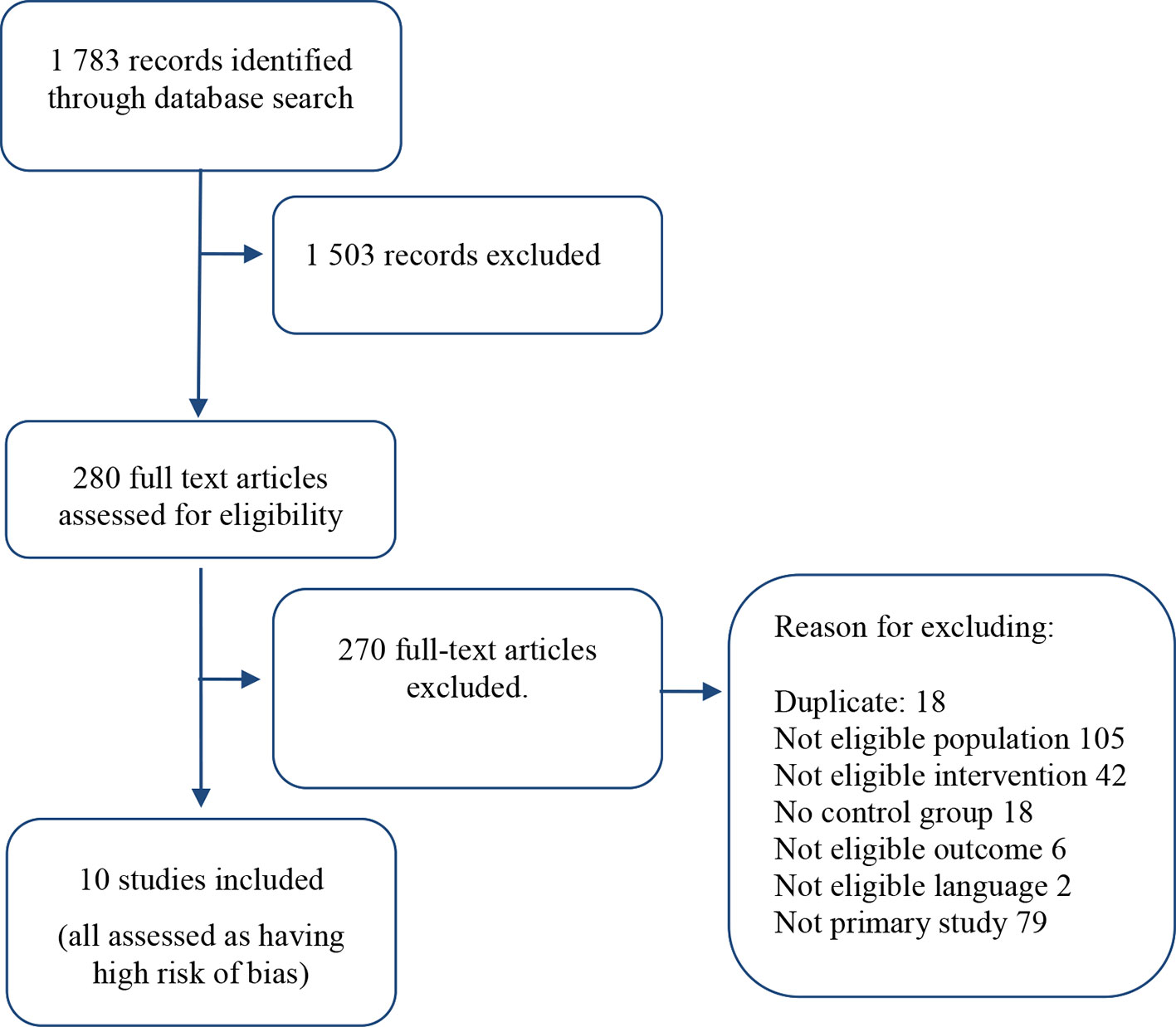
Figure 1 Flowchart over literature search.
Synthesized Findings
The 10 included studies, which are further described in Table 1, were conducted in the United Kingdom (24, 25, 30, 31), USA (23, 29), and Canada (22, 26–28). Seven of the studies were retrospective. The study populations were exclusively from high security hospitals. One study followed the patients from in- to outpatient care (28). Half of the studies investigated the specific anti-psychotic clozapine with regard to effect on aggressive behavior, psychotic symptoms, time of treatment inside the hospital before release and time outside the hospital before readmission (22, 25, 28–30).
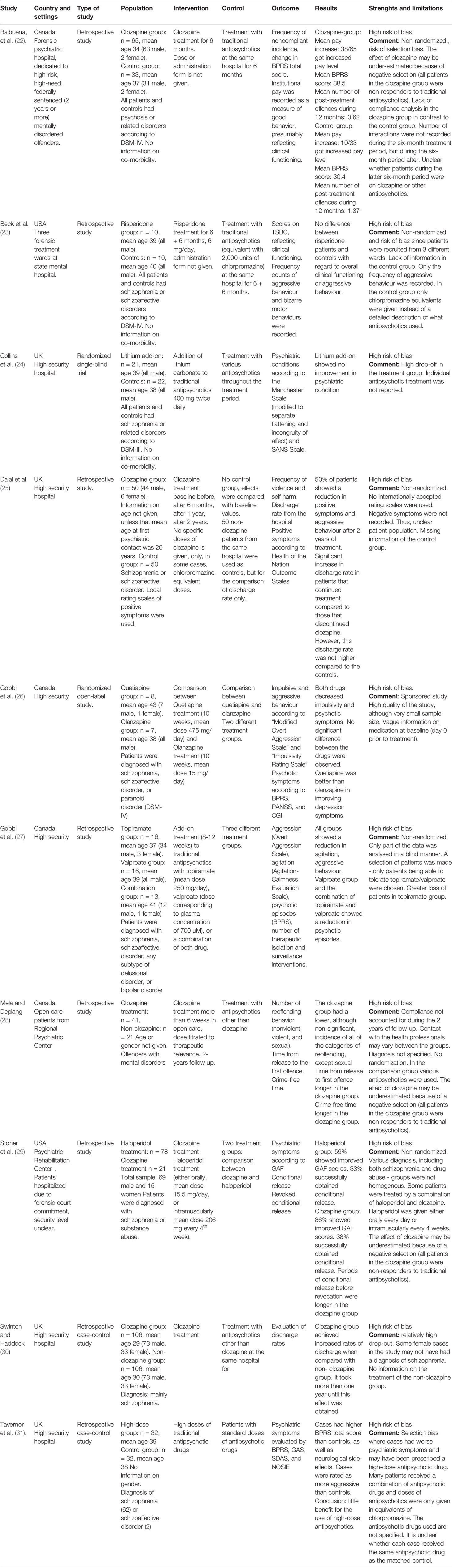
Table 1 Characteristics of included studies.
In Table 2 we present the different outcomes according to GRADE. Some of our defined outcomes, survival, compliance to treatment and quality of life, were not present in any of the selected studies. The outcomes that we did find in the included studies were psychotic symptoms, side-effects of pharmacological treatment, reoffending, time outside the hospital before readmission, clinical functioning, aggressive behavior and length of stay in hospital. When measuring psychotic symptoms after treatment, the clozapine group showed more psychotic symptoms compared to the control group (22), while there were no differences between groups studying ad-on treatment with lithium (24) or quetiapine versus olanzapine (26). In one study there were three groups with mood stabilizers, which found reduction on psychotic symptoms in the group with valproate and the combination valproate and topiramate after treatment (27). When studying crime-free time and time in the community between discharge from hospital to reoffending or readmission, two studies showed valuable effects in the clozapine group (28, 29) compared to other antipsychotics. Regarding measures of time spent in hospital after the start of treatment, two studies showed positive effects of clozapine (29, 30), while a third study did not find any differences between clozapine and other antipsychotics (25). Two studies found improvement in clinical functioning in the clozapine group compared to other antipsychotics (22, 29), while a study comparing risperidone compared to traditional antipsychotics did not find any differences (23). We found two studies showing positive effects of clozapine on aggressive episodes (22, 28), while there were no group differences when comparing risperidone with traditional antipsychotic (23), quetiapine with olanzapine (26) or topiramate with valproate (27).The only study comparing high with standard doses of antipsychotics showed more pronounced psychotic symptoms and more side effects in the high dose-group after the treatment period (31).
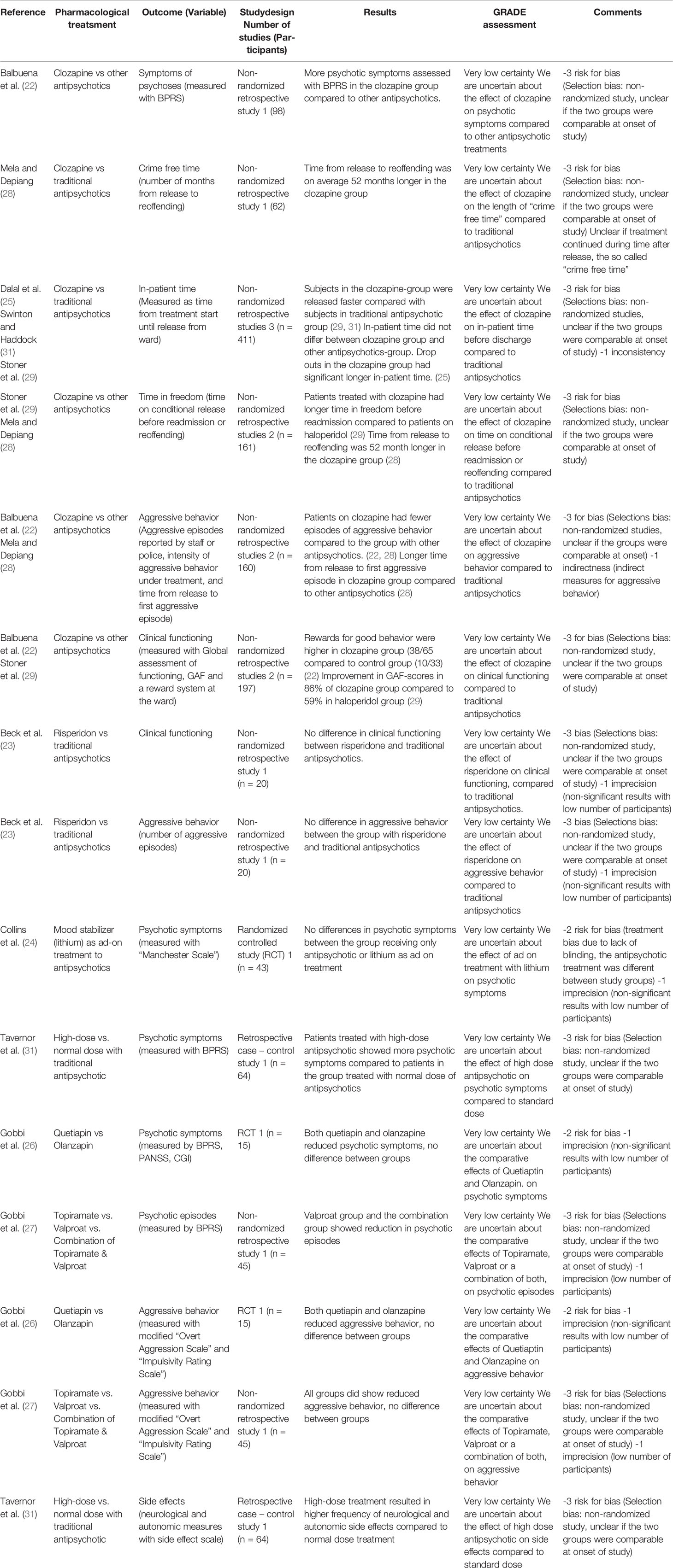
Table 2 Summary of findings according to GRADE.
Risk of Bias
All outcomes were assessed as very low certainty due to a severe or critical risk of bias, imprecision and/or indirectness and inconsistency. There were problems with selection bias in all the included studies. As all the studies were conducted in clinical settings and only a few had randomization (24, 26), there were potential differences between comparison groups of patients. In many studies there was also a lack of transparency as to how the patients were selected (23, 27) and a lack of information about essential characteristics of the groups, such as comorbidity and substance abuse (22–24, 28, 30). Due to the non-randomized study design, as well as severe additional concerns about selection bias, the certainty of the evidence was assessed as very low.
Discussion
The limited findings from this systematic review reveal a knowledge gap in pharmacological treatment within forensic psychiatric care. Even though the use of pharmacological agents is high in forensic psychiatric settings, these patients are seldom included in pharmacological trials. As in the two previous systematic reviews we did not find any primary studies of high quality (15, 16). Rather, all selected studies had a high risk of bias. Compared to these two previous reviews, we included four primary studies which had not previously been included. One study compared the effect of add-on treatment with lithium (24) and another compared clozapine to haloperidol (29). Two studies were published later than both of these reviews; one compared treatment with quetiapine versus clozapine (26), the other followed inpatients through to outpatient care comparing clozapine with other antipsychotics (28).
Most of the studies found were retrospective (22, 23, 25, 27–31) and performed in a clinical context, which resulted in a high risk of selection bias. Only two of them were prospective (24, 26). Half of the studies analyzed the therapeutic effects of clozapine (22, 25, 28–30). As clozapine is a third-hand choice in guidelines for treatment of psychotic disorders, all the patients receiving clozapine were non-responders to traditional antipsychotics. Potentially these patients could have been suffering from more severe psychotic symptoms, or other kinds of symptoms, resistant to traditional antipsychotics. For example, psychotic symptoms before treatment have been more pronounced in the clozapine group, indicating a selection bias (22).
Guidelines for forensic psychiatric treatment have been proposed, although, the authors found that the evidence base for forensic-psychiatric practice is weak (32). In another study presenting guidelines for aggressive psychiatric patients in California, these guidelines were developed from a collection of prescribing recommendations, clinical trial results, and years of clinical experience in treating patients who are persistently violent or aggressive in the California Department of State Hospital System, and included recommendations provided off-label prescribing of pharmacological agents (33).
We think that the specific circumstances within the forensic psychiatric care; forensic patients in general being suffering more often suffer from comorbidity as well as aggression and violent behavior and the fact that one objective of the care is coetail protection may influence the outcome of pharmacological treatment. Therefore, we maintain that there is an urgent need for studies performed in this unique context. Randomized prospective studies in forensic psychiatric samples should be prioritized. Forensic populations ought to be studied with higher precision, with regard to their particular context. Also, there are specific outcomes of special interest to forensic settings compared to the general psychiatry, such as reoffending and violent behavior. Clearly, any pharmacological treatment with a potential effect on offending and violent behavior would be of great interest not only for the patients but also society at large. Since most forensic patients are treated involuntarily for a long time period, which entails a major infringement of several human rights, interventions shortening the length of stay in hospital would also be of great ethical value. It would also be of great interest from a health economic point of view, as the cost of pharmacological treatment is almost negligible in comparison to all other costs of forensic psychiatric care.
Limitations
This systematic review only included studies produced within the specific setting of forensic psychiatry. However, there could be studies produced in other settings, such as in general psychiatry or in correctional samples, that could have added evidence, for example those focusing on pharmacological effects on patients with comorbid conditions. Our study selection was also limited to studies written in English, Swedish, Norwegian or Danish language, and we did not include gray literature. Therefore, there is always a potential that studies only published as reports etc., or in other languages were missed. Studies which may have been published after the original literature search in January 2018 were not included in this review.
Conclusions
This systematic review highlights the scarcity of knowledge on the effectiveness of pharmacological treatment within a forensic psychiatric population. Thus, due to the very few studies available in this setting, as well as limitations in their execution and reporting, it is challenging to overview the outcomes of pharmacological interventions in this regard. The frequent use of antipsychotics, with or without a combination of other pharmacological agents, in this complex and heterogeneous patient group, calls for high-quality studies performed in specific settings. Such strategies are also highly warranted from an ethical as well as health economics standpoint.
Author Contributions
KH, PA, EL, GE, MH, and MN defined PICO, assessed relevance of abstracts and full text articles, extracted data, assessed the risk of bias in individual studies, analyzed and interpreted the results, and wrote the manuscript. EE and SR defined PICO, analyzed and interpreted the results, and wrote the manuscript.
Funding
This systematic review was conducted at The Swedish Agency for Health Technology Assessment and Assessment of Social Services (SBU). The funding agency had no role in study design, data collection, data analysis, data interpretation or writing of the report.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as potential conflicts of interest.
Acknowledgments
The authors would like to thank SBU for methodological support and the opportunity to carry out this work. We especially thank Hanna Olofsson for performing the literature searches and Caroline Jungner for administrative support. We also would like to thank Kristina Sygel for English language revision.
Supplementary Material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpsyt.2019.00963/full#supplementary-material
References
1. Svennerlind C, Nilsson T, Kerekes N, Andine P, Lagerkvist M, Forsman A, et al. Mentally disordered criminal offenders in the Swedish criminal system. Int J Law Psychiatry (2010) 33(4):220–6. doi: 10.1016/j.ijlp.2010.06.003
2. Edworthy R, Sampson S, Völlm B. Inpatient forensic-psychiatric care: legal frameworks and service provision in three European countries. Int J Law Psychiatry (2016) 47:18–27. doi: 10.1016/j.ijlp.2016.02.027
3. Fazel S, Wolf A, Fiminska Z, Larsson H. Mortality, rehospitalisation and violent crime in forensic psychiatric patients discharged from hospital: rates and risk factors. PloS One (2016) 11(5):e0155906. doi: 10.1371/journal.pone.0155906
4. Gunn J, Taylor PJ. Forensic Psychiatry: Clinical, Legal and Ethical Issues, Second Edition. 2nd ed. UK: CRC Press: Taylor and Francis Group; (2014). 1035 p.
5. Flynn G, O’Neill C, McInerney C, Kennedy HG. The DUNDRUM-1 structured professional judgment for triage to appropriate levels of therapeutic security: retrospective-cohort validation study. BMC Psychiatry (2011) 11:43. doi: 10.1186/1471-244X-11-43
6. Buchanan A, Grounds A. Forensic psychiatry and public protection. Br J Psychiatry (2018) 198(6):420–3.
7. Palijan TZ, Muzinic L, Radeljak S. Psychiatric comorbidity in forensic psychiatry. Psychiatr Danub (2009) 21(3):429–36.
8. Goethals KR, Vorstenbosch ECW, van Marle HJC. Diagnostic comorbidity in psychotic offenders and their criminal history: a review of the literature. Int J Forensic Ment Health (2008) 7(2):147–56.
9. Degl’ Innocenti A, Hassing LB, Lindqvist A-S, Andersson H, Eriksson L, Hanson FH, et al. First report from the Swedish National Forensic Psychiatric Register (SNFPR). Int J Law Psychiatry (2014) 37(3):231–7. doi: 10.1016/j.ijlp.2013.11.013
10. Torniainen M, Mittendorfer-Rutz E, Tanskanen A, Bjorkenstam C, Suvisaari J, Alexanderson K, et al. Antipsychotic treatment and mortality in schizophrenia. Schizophr Bull (2015) 41(3):656–63. doi: 10.1093/schbul/sbu164
11. Tiihonen J, Wahlbeck K, Lonnqvist J, Klaukka T, Ioannidis JP, Volavka J, et al. Effectiveness of antipsychotic treatments in a nationwide cohort of patients in community care after first hospitalisation due to schizophrenia and schizoaffective disorder: observational follow-up study. Bmj (2006) 333(7561):224. doi: 10.1136/bmj.38881.382755.2F
12. Nationellt rättspsykiatriskt kvalitetsregister (RättspsyK). Årsrapport 2017. Nationellt rättspsykiatriskt kvalitetsregister: Göteborg (2018).
13. Patchan K, Vyas G, Hackman AL, Mackowick M, Richardson CM, Love RC, et al. Clozapine in reducing aggression and violence in forensic populations. Psychiatr Q (2018) 89(1):157–68. doi: 10.1007/s11126-017-9521-z
14. Howner K, Andine P, Bertilsson G, Hultcrantz M, Lindstrom E, Mowafi F, et al. Mapping systematic reviews on forensic psychiatric care: a systematic review identifying knowledge gaps. Front Psychiatry (2018) 9:452.
15. Fontanarosa J, Uhl S, Oyesanmi O, Schoelles KM. Interventions for Adult Offenders With Serious Mental Illness. Comparative Effectiveness Review No. 121. (Prepared by the ECRI Institute Evidence-based Practice Center under Contract No. 290-2007-10063-I.) (2013)AHRQ Publication No. 13-EHC107-EF. Rockville, MD: Agency for Healthcare Research and Quality; August 2013. www.effectivehealthcare.ahrq.gov/reports/final.cfm
16. Tapp J, Perkins D, Warren F, Fife-Schaw C, Moore E. A critical analysis of clinical evidence from high secure forensic inpatient services. Int J Forensic Ment Health (2013) 12(1):68–82.
17. Moher D, Shamseer L, Clarke M, Ghersi D, Liberati A, Petticrew M, et al. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015 statement. Syst Rev (2015) 4(1):1. doi: 10.1186/2046-4053-4-1
18. SBU. Assessment of methods in health care Stockholm - a handbook. Retrieved from Stockholm, Swedish Agency for Health Technology Assessment and Assessment of Social Services (2018).
19. Schulz K F, Altman D, Moher D. CONSORT 2010 statement: updated guidelines for reporting parallel group randomised. Trials (2010) 8:18. doi: 10.1186/1741-7015-8-18
20. von Elm E, Altman DG, Egger M, Pocock SJ, Gotzsche PC, Vandenbroucke JP. The strengthening the reporting of observational studies in epidemiology (STROBE) statement: guidelines for reporting observational studies. J Clin Epidemiol (2008) 61(4):344–9. doi: 10.1016/j.jclinepi.2007.11.008
21. Balshem H, Helfand M, Schünemann HJ, Oxman AD, Kunz R, Brozek J, et al. GRADE guidelines: 3. rating the quality of evidence. J Clin Epidemiol (2011) 64(4):401–6.
22. Balbuena L, Mela M, Wong S, Gu D, Adelugba O, Tempier R. Does clozapine promote employability and reduce offending among mentally disordered offenders? Can J Psychiatry (2010) 55(1):50–6.
23. Beck NC, Greenfield SR, Gotham H, Menditto AA, Stuve P, Hemme CA. Risperidone in the management of violent, treatment-resistant schizophrenics hospitalized in a maximum security forensic facility. J Am Acad Psychiatry Law (1997) 25(4):461–8.
24. Collins PJ, Larkin EP, Shubsachs APW. Lithium carbonate in chronic schizophrenia — a brief trial of lithium carbonate added to neuroleptics for treatment of resistant schizophrenic patients. Acta Psychiatr Scandinavica (1991) 84(2):150–4.
25. Dalal B, Larkin E, Leese M, Taylor PJ. Clozapine treatment of long-standing schizophrenia and serious violence: a two-year follow-up study of the first 50 patients treated with clozapine in Rampton high security hospital. Criminal Behav Ment Health (1999) 9(2):168–78.
26. Gobbi G, Comai S, Debonnel G. Effects of quetiapine and olanzapine in patients with psychosis and violent behavior: a pilot randomized, open-label, comparative study. Neuropsychiatr Dis Treat (2014) 10:757–65.
27. Gobbi G, Gaudreau P-O, Leblanc N. Efficacy of topiramate, valproate, and their combination on aggression/agitation behavior in patients with psychosis. J Clin Psychopharmacol (2006) 26(5):467–73.
28. Mela M, Depiang G. Clozapine’s effect on recidivism among offenders with mental disorders. J Am Acad Psychiatry Law (2016) 44(1):82–90.
29. Stoner S, Wehner Lea J, Dubisar B, Roebuck-Colgan K, Vlach D. Impact of clozapine versus haloperidol on conditional release time and rates of revocation in a forensic psychiatric population. J Pharm Technol (2002) 18:182–6. doi: 10.1177/875512250201800403
30. Swinton M, Haddock A. Clozapine in special hospital: a retrospective case-control study. J Forensic Psychiatry (2000) 11(3):587–96. doi: 10.1080/09585180010006205
31. Tavernor R, Swinton M, Tavernor S. High-dose antipsychotic medication in maximum security. J Forensic Psychiatry (2000) 11:36–48.
32. Vollm BA, Clarke M, Herrando VT, Seppanen AO, Gosek P, Heitzman J, et al. European Psychiatric Association (EPA) guidance on forensic psychiatry: Evidence based assessment and treatment of mentally disordered offenders. Eur Psychiatry (2018) 51:58–73.
Keywords: forensic psychiatric care, mentally disordered offenders, pharmacological treatment, systematic review, antipsychotics
Citation: Howner K, Andiné P, Engberg G, Ekström EH, Lindström E, Nilsson M, Radovic S and Hultcrantz M (2020) Pharmacological Treatment in Forensic Psychiatry—A Systematic Review. Front. Psychiatry 10:963. doi: 10.3389/fpsyt.2019.00963
Received: 17 December 2018; Accepted: 05 December 2019;
Published: 16 January 2020.
Edited by:
Harry G. Kennedy, Trinity College Dublin, IrelandReviewed by:
Birgit Angela Völlm, University of Rostock, GermanyVivek Anthony Furtado, University of Warwick, United Kingdom
Copyright © 2020 Howner, Andiné, Engberg, Ekström, Lindström, Nilsson, Radovic and Hultcrantz. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Katarina Howner, katarina.howner@ki.se