 Helmut Strobl
Helmut Strobl Katharina Ptack
Katharina Ptack Clemens Töpfer
Clemens Töpfer Ralf Sygusch
Ralf Sygusch Susanne Tittlbach
Susanne Tittlbach- 1Institute of Sport Science, University of Bayreuth, Bayreuth, Germany
- 2Department of Sport Science and Sport, Friedrich-Alexander-University Erlangen-Nürnberg (FAU), Erlangen, Germany
Introduction: The development of knowledge and understanding in relation to movement and health is a basic requirement to facilitate lifelong engagement in physical activity with its accompanying possible health benefits. To train teachers in applying adequate strategies, implementation studies have often shown little acceptance of traditional top-down approaches. Thus, the purpose of the Health.edu project was to develop, implement and evaluate effective and feasible measures addressing students' health-related knowledge and understanding (HKU) in physical education (PE) via a participatory approach.
Materials and Methods: For evaluation, a controlled pre-post-test study with 233 students from eight different secondary schools in Germany was carried out. Four schools (with two PE teachers at each school) comprised the intervention group and they participated in a 1-year participatory planning process to conceptualize and implement evidence-based PE lessons addressing students' HKU. Control schools carried out their regular PE lessons. Evaluation followed a mixed-methods research design, assessing program implementation via written documentary technique as well as program effectiveness using a standardized questionnaire.
Results: Results show a significant intervention effect on students' HKU with a medium effect size. However, due to the participatory process, there were considerable differences between the intervention schools that were involved. Student's HKU improved most in schools where program implementation corresponded to relevant principles of fostering HKU.
Discussion: The present study purposefully dispensed with any structured intervention programs for PE teachers to follow. The results show the potential effects of this participatory approach to strengthen student's HKU. However, the participatory planning does not always work in the intended manner, emphasizing that numerous contextual factors influence the implementation process.
Introduction
For all individuals, health is a resource that needs to be maintained and protected. Therefore, against the background of a salutogenic and holistic approach, people should be enabled to increase control over, and to promote, their health (1). This emphasis is the result of an increasing public awareness of health problems such as obesity, cardiovascular diseases, and mental health (2). To comply salutogenic and holistic requirements, concepts of health promotion should focus on salutary rather than risk factors, and always see the entire person rather than the single disease (3). Schools especially are regarded to be ideal settings for health promotion, due to the easy accessibility to children and adolescents as well as the large amount of time students spend at school (4, 5). Thus, health promotion at school must be linked directly to school educational development and school's educational goals (6, 7). Considering physical education (PE), there is currently a broad international discussion about how to link the educational aspects of physical activity and physical activity promotion in current PE curricula (7–11). To achieve the wide range of possible educational outcomes of PE for school-age children, a focus on health outcomes through fitness training, without any reflection concerning educational purposes, is not sufficient. Instead, the overall aim should be to provide young people with the knowledge, skills and understanding necessary to perform various physical activities and maintain healthy lifestyles (9, 12–16). This is a necessary precondition for many health enhancing effects (17) and thus also important from a public health point of view (18).
The notion of physical literacy (PL) provides helpful pedagogical orientation for PE, as it captures the essence of what a quality PE aims to achieve (13, 19, 20). PL is defined as “the motivation, confidence, physical competence, knowledge and understanding to value and take responsibility for engagement in physical activity for life” (21). The concept was introduced by Whitehead (22) and since then PL has gained a growing scholarly interest (13, 19, 23, 24). As definitions adopted from different organizations and research groups differ, Edwards et al. provided a systematic review of core attributes of PL (25). Affective and cognitive properties, as well as physical capabilities emerged as particularly common subthemes of the PL construct. Being physically literate is conceived to be the result of the integrated interaction of these domains (20, 25). PL is further considered a basic requirement to facilitate lifelong engagement in physical activity with its accompanying possible health benefits (13, 23, 26, 27). Focusing on the relationship of the different PL domains, some authors denote the cognitive attributes of knowledge and understanding as fundamental to achieving the other domains and the overall concept of PL (23, 28, 29). In that sense, students should acquire knowledge and understanding in relation to movement and health. This includes for instance a profound knowledge and understanding of the principles of movement and performance, but also of the requirements, antecedents and values of participating in a physically active lifestyle (25, 27, 28).
The concept of PL including its cognitive attributes of knowledge and understanding is also widely accepted in German PE curricula1 and pedagogical concepts (14, 30, 31). In line with the international discussion, students should be enabled to care for their own health and not to produce primarily direct health outcomes (14). The aim is to develop students' knowledge and understanding to practice sport in a healthy way, to assess the health effects of one's own sport activities and, if necessary, to modify the activity in order to be more healthy (32). Thus, the development of knowledge and understanding in relation to health to facilitate students making healthy choices for physical activity (33) is in particular a major concern in German PE.
In order to target health-related knowledge and understanding (HKU) in PE, there is a need for student-centered teaching-learning processes, combining delivery of health-related knowledge with experiences through physical activity (13, 23, 34–37). However, research indicates PE teachers' limited knowledge in defining appropriate learning outcomes for HKU and how to deliver those aspects within their PE lessons (8, 28, 34, 35, 38). To train teachers in applying adequate strategies for delivering health-related knowledge, implementation studies have often shown little acceptance of traditional top-down approaches (36, 37). Instead, there is evidence for the potential of a participatory approach (39). This includes the collaboration of relevant members of a setting (e.g., teachers, principal, and students at school) with a scientific research team in order to plan, implement and evaluate health-promoting measures. The corresponding communication and interaction processes can enhance knowledge and competencies concerning evidence-based and feasible health-promoting measures among all involved stakeholders (40, 41). Furthermore, equal participation of all stakeholders in discussions and decision-making may enhance identification of all participants with the actions taken and increases chances of sustainable implementation (42, 43). For those reasons, the Health.edu project strives to develop, implement and evaluate effective and feasible student-centered measures for the enhancement of HKU in PE via a participatory approach2. The focus of this paper is mainly to report the evaluation of the project's effectiveness, i.e., change of students' HKU due to the intervention. The overall research question is whether it is possible to strengthen students' HKU via a school-based participatory approach.
Materials and Methods
Design
We carried out a quasi-experimental pre-post-test study design over one academic year with eight secondary schools (four intervention schools and four control schools), evaluating program implementation as well as program effectiveness (44, 45). Evaluation followed a mixed methods design. The effectiveness of the intervention was assessed by a standardized paper and pencil questionnaire. However, as differences between intervention schools may occur due to the participatory process, we also took the evaluation of program implementation via qualitative methodology into account. Therefore, written documentary technique was used additionally to document and analyses the processes throughout the intervention.
Intervention
The goal of the intervention was to enable students to make healthy choices regarding physical activity by strengthening their HKU. To match scientific evidence concerning delivery of health-related knowledge in PE with actual prerequisites within schools, an effective way of exchanging knowledge between scientists and school stakeholders (e.g., principals, students, and PE teachers) is necessary. Therefore, we used a participatory approach since this has been shown to be effective in previous studies concerning health promotion (46–48). To ensure knowledge exchange processes, we facilitated so-called cooperative planning groups (consisting of scientists, students, principal and PE teachers) at each of the four intervention schools. Planning groups were maintained throughout the academic year. The schedule of the single planning group meetings (see Table 1) was similar at each school.
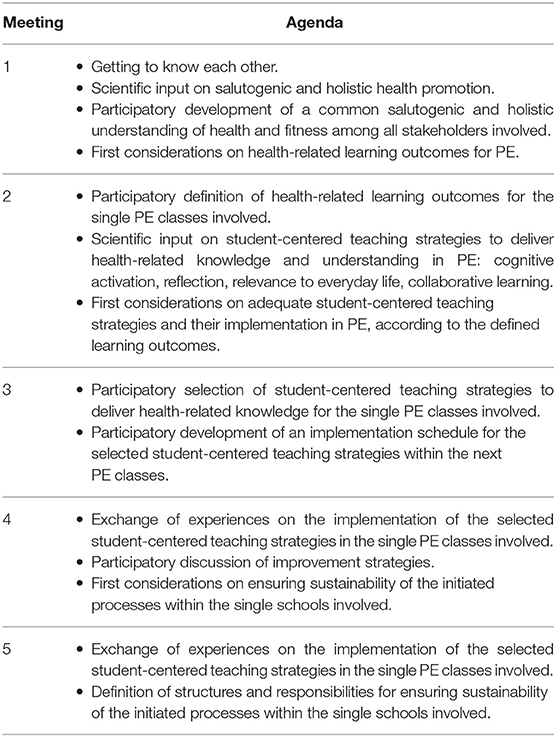
Table 1. Schedule of the single planning group meetings.
In the first two meetings, participants of planning groups discussed and defined health-related learning-outcomes for their PE lessons. Learning outcomes should follow a holistic understanding of health and fitness, integrating physical as well as psychosocial aspects (14, 28, 33). On the one hand, students should learn how to apply the short- and long-term benefits of physical activity regarding improvement of physical fitness at school as well as in their spare time. They also should gain knowledge and understanding about their activity-related behavior in terms of risk factors, injuries and illnesses. On the other hand, PE should improve students' knowledge and understanding of how social and mental well-being are interrelated with physical activity and how personal well-being can be developed by means of physical activity.
In the second meeting, the research group additionally provided scientific input on student-centered teaching strategies (cognitive activation, reflection, relevance to everyday life, collaborative learning). Research shows, that the application of student-centered teaching-strategies during PE lessons best supports students' cognitive processes of accessing, understanding and appraising health-related information (8, 49, 50). “Cognitive activation” means to ask students for previous activity-related experiences and link it to new content (e.g., asking students for known warm-up exercises and discussing their relevance to the subsequent sport activities). “Reflection” refers to providing students with stimuli, which let them think about their experiences following the pursued activities (e.g., reflecting the effects of a High-Intensity-Training on heart rate and subjective exhaustion or reflecting the effects of different stretching exercises on mental well-being). “Relevance of everyday life” means to consider topics in PE lessons that are relevant for the students (such as fitness training for a forthcoming ski course). “Collaborative learning” finally refers to giving the students a task, which has to be solved by working together (e.g., providing sheets with information on a muscle building training circuit and instructing the students to organize single circuit stations).
The participants of the planning groups jointly selected in meetings two and three adequate student-centered teaching strategies for the previous defined learning outcomes and discussed their implementation within the next PE classes. In the discussions, great importance was attached to ensure that the tasks set by PE teachers are always combined with experiences through physical activity. That is, teachers should not only deliver health-related knowledge theoretically, but also combine it directly with physical experiences (e.g., different kinds of running intensity and its effects on heart pulse in combination with pulse monitoring or different methods of muscle stretching and its effects on relaxation).
Finally, PE teachers implemented these conceptualized lessons in their PE classes and afterwards a discussion of their experiences took place among all participants of the planning groups. The stakeholders involved also discussed how to ensure sustainability of the initiated processes with the single schools concerned (meetings four and five).
Participants
Recruitment of eight secondary schools occurred by contacting school principals via email, phone, or in-person. To account for similar socio-economic characteristics, schools were recruited in the same administrative district in Bavaria, Germany. To account for different cognitive abilities of the students, four secondary modern schools and four grammar schools were part of the study3. After agreeing to participate in the study, schools were placed–according to their willingness–into either the control or the intervention group (two grammar and two secondary modern schools, respectively). In each intervention school, two PE teachers (one female and one male respectively) participated with their corresponding PE classes voluntarily in the study. The total pre-post-sample of the students included 233 students with the age range of 11–17 years (M = 14.66, SD = 1.27). Table 2 provides an overview of participants pertaining to either intervention or control group.
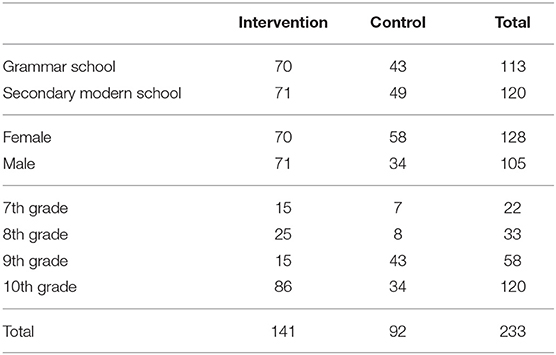
Table 2. Number of students pertaining to intervention or control group.
Measures
Regarding the evaluation of program implementation, protocols of each planning group meeting were compiled (in total 19 protocols). An assistant documented relevant statements and resolutions over the course of the meeting. The assistant was not directly involved in the research project, warranting a “neutral” view on the discussions. At the end, all participants of the planning group had the opportunity to add their most important findings throughout the discussions. The protocols allow an analysis of how a holistic understanding of health and student-centered teaching methods were addressed within the PE lessons.
Concerning the evaluation of program effectiveness, the HKU of the students was measured at the beginning (t0) and the end (t1) of the school year through a standardized paper and pencil test. As there is a lack of an accurate empirical assessment of the outcomes of implemented teaching learning processes (23, 26), we used a well-developed and well-validated questionnaire (for further information on the validation process see next section 2.5) (33). The questionnaire consisted of 25 items including three different item formats: short text (8), single choice (10) and multiple choice (7). The questions follow a holistic understanding of health and fitness, integrating physical as well as psychosocial aspects, and are derived from current requirements in German PE curricula. One short text item was, for example, to describe a way of measuring heart rate without a pulse monitor. A second item was to name different perceived reactions of the body, while executing relaxation techniques. Figures 1, 2 give further examples for single choice and multiple-choice items.

Figure 1. Example for a single choice item of the standardized paper and pencil test.

Figure 2. Example for a multiple choice item of the standardized paper and pencil test.
Test instructors followed a predefined procedure (33). As the test is designed to be a power test and not a speed test, students had enough time to answer the questions: students were given 30 min to fill in the questionnaire. Item responses were assessed according to a coding guideline (33). Answers to the short text items needed to be rated on a four-step ordinal rating scale (0–3). Single and multiple-choice items were rated dichotomously (0–1). The inter-rater reliability (Kendalls Tau-c) proves a good or even very good level of congruence within the coding process (τ = 0,813). Missing data was treated as wrong answers (0) linking back to the fact that the person's individual HKU-level may be on a rather low level.
Data Analysis
Qualitative data was analyzed via thematic content analysis (51–53) using MaxQDA12 software. In order to guarantee rigor and quality of the data analysis, attention was paid to the fact that the evaluation process is designed to be inter-subjectively comprehensive by documenting the process in detail (including the description of the theoretical grasp, the intervention, the context and the methodological approach) (54). At the beginning of the analysis, the data from the documentary techniques was coded according to the main categories “understanding of health” and “student-centered approaches.” The coding guide is successively generated by several rework loops and revisions with regard to definitions, anchor examples and coding rules. After grouping the codes to the corresponding main categories, another researcher encoded ~25% of randomly selected contributions to estimate intercoder–reliability (intercoder-reliability of 78%). Afterwards, all research members of the Health.edu project discussed and revised the coding guide. Intercoder–reliability subsequently increased up to 93%.
For the analysis of the quantitative data, values reflecting students' HKU were estimated upon the responsive behavior of the students using the Rasch Model (Partial Credit Model). Those values concern the probability that the students that were involved may correctly solve the questionnaire tasks. The applicability of the Rasch Model (Partial Credit Model) was successfully proved in a previous study (LR-test: Chi2 = 50.81; df = 40; p = 0.118) (33). The test exhibited an acceptable level of reliability (EAP/PV = 0.79). All items showed good values for item fit based on Weighted Mean Square (WMNSQ) within the range 0.8–1.2. Values for student's HKU were finally transformed into standard values (M = 500, SD = 100). Descriptive statistics for changes of student's HKU between t0 and t1 were calculated. An analysis of covariance was conducted to evaluate the treatment effect of the intervention on student's HKU at the end of the school year (HKU_t1) in contrast to the control group whilst adjusting for the effects of the educational level (i.e., type of school), gender and age. Those co-variates were chosen due their established association with literacy levels (55, 56). People with lower educational levels, older age and male gender tend to have lower health literacy levels. Among several social determinants of health literacy, education represents a very strong predictor, followed by age and gender (56). Additionally, students' HKU at the beginning of the school year (HKU_to) was integrated as a covariate. By doing this, each student's score after the intervention is adjusted to his or her baseline score, which provides the advantage of being unaffected by baseline differences (57). Effect sizes (i.e., partial η2) were calculated for the F statistics. Statistical assumptions for ANCOVA were examined according to Field (58) and showed no major problems with kurtosis, skewness or homogeneity of variance.
The calculation of changes in students' HKU between pre- and post-test for each school of the intervention group and their corresponding 95% confidence intervals serve to illustrate the changes that occurred in every school. Effect sizes (i.e., Cohen's d) were calculated for mean differences. To consider dependency of the pre-post-data, calculation of d was based on mean differences between HKU_t0 and HKU_t1, divided by the standard deviation of HKU_t0, which was corrected by the correlation between pre- and post-test data (59). All quantitative data analyses were completed using R 3.3.0 and SPSS 25. Significance was set a priori at an alpha-value of < 0.05.
Results
Evaluation of Program Implementation
Altogether, 10 teaching units were developed and implemented in the four school specific planning groups (schools A, B, C, and D; Table 3). The teaching units showed differences in relation to the understanding of health. The majority of teaching units exclusively considered physical aspects of health (units 2, 3, 5, 6, and 8), whereby the other units (units 1, 5, 7, 9, and 10)–at least partly–also addressed psychosocial aspects of health. There were further substantial differences concerning student-centered approaches. Teaching units of schools A and B (units 1–5) were highly student-centered, as they considered all criteria such as cognitive activation, reflection, relevance to everyday life, and collaborative learning. They also consistently combined delivery of health-related knowledge with physical experiences. PE teachers of school D (units 8–10) neglected reflection and collaborative learning. However, as well as teachers of schools A and B, they prioritized educational aspects in contrast to direct health outcomes, attached great importance to cognitive activation via an intensive knowledge transfer and combined delivery of health-related knowledge with physical experiences. In contrast, teaching units of school C (units 6 and 7) only showed slight tendencies to consider cognitive activation and did not establish a link between delivery of health-related knowledge and physical experiences.
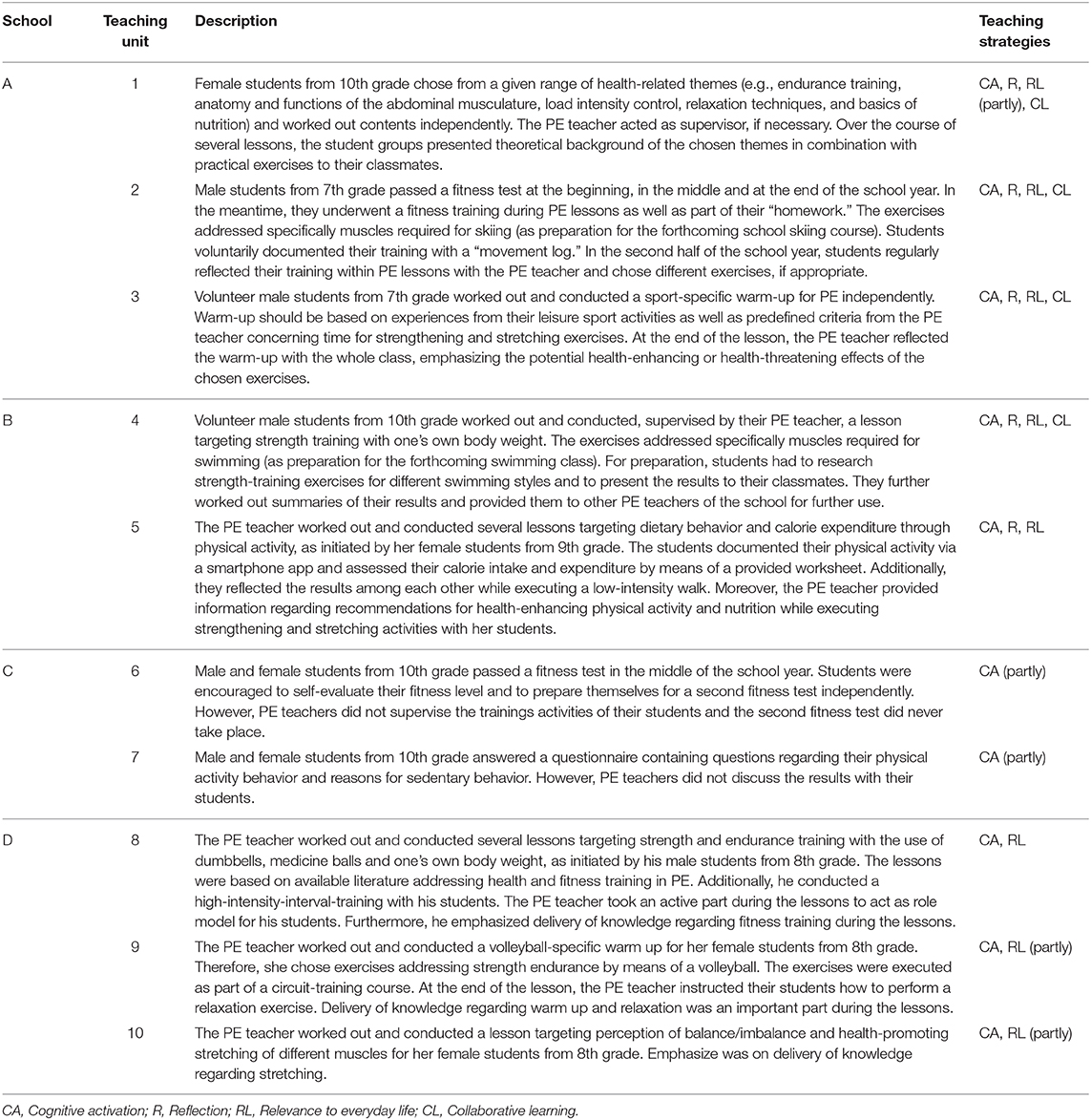
Table 3. Developed and implemented measures within PE in intervention schools (schools A, B, C, and D), including consideration of student-centered teaching strategies.
Evaluation of Program Effectiveness
According to Table 4, students' HKU generally improved across group, type of school, grade and gender. In detail, students from intervention schools (Δ55) improved their HKU more than students from control schools (Δ26). Greater improvements in HKU are also apparent in students from grammar schools (Δ60) in comparison to secondary modern schools (Δ29) and females (Δ48) in comparison to males (Δ38). Finally, students from lower grades realized greater HKU-improvements than students from higher grades (7th grade Δ58, 8th grade Δ52, 9th grade Δ48, 10th grade Δ37).
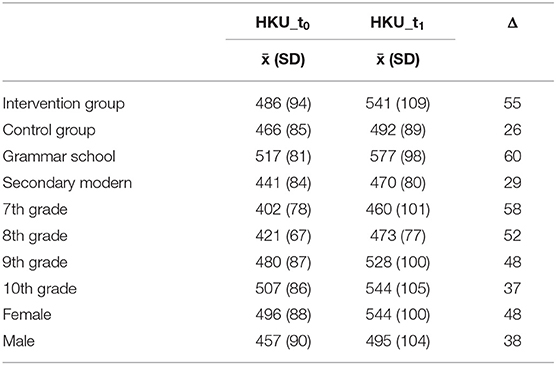
Table 4. Descriptive statistics (x, SD, and Δ for mean differences) for student's health-related knowledge and understanding at the beginning (HKU_t0) and at the end of the school year (HKU_t1) across group, type of school, grade, and gender.
Table 5 shows the results of the ANCOVA. Except for age (F(1, 227) = 0.169, p = 0.692, η2 = 0.001), there is a significant relation to HKU_t1 for all covariates: HKU_t0 (F(1, 227) = 134.250, p < 0.001, η2 = 0.372), type of school (F(1, 227) = 26.840, p < 0.001, η2 = 0.106) and gender (F(1, 227) = 4.414, p = 0.037, η2 = 0.019). While adjusting for the covariates, students in intervention schools had a significantly greater score of HKU_t1 in contrast to the control group (F(1, 227) = 16.046, p < 0.001, η2 = 0.066; medium effect).
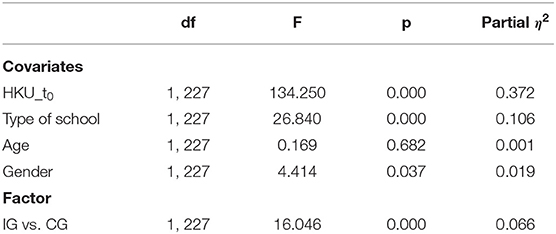
Table 5. Analysis of covariance (dependent variable: HKU_t1) with the factor intervention vs. control group and the covariates HKU_t0, type of school, age, and gender.
Results of the intervention differ considerably between schools (see Figure 3, Table 6). Significant mean differences with strong effect sizes of pre- and post-test data for students' HKU are apparent in schools A (d = 1.3), B (d = 1.0), and D (d = 1.3), but not for school C (non-significant mean difference with a small effect size, d = 0.2).
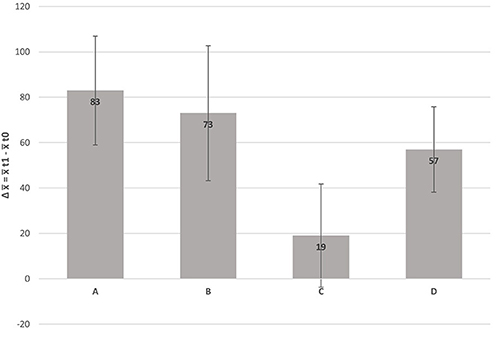
Figure 3. Average change (Δ) of student's health-related knowledge and understanding (HKU) between the beginning (t0) and the end of the school year (t1) and corresponding 95% confidence intervals, separated for each intervention school.
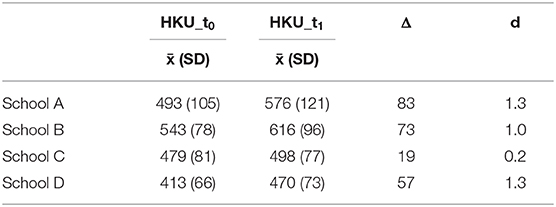
Table 6. Descriptive statistics (x, SD, and Δ for Mean Differences) for student's health-related knowledge and understanding at the beginning (HKU_t0) and at the end of the school year (HKU_t1) across intervention schools with adjusted Cohen's d.
Discussion
Health.edu strives to develop, implement and evaluate effective and feasible measures addressing health-related knowledge and understanding (HKU) in physical education (PE) via a participatory approach. The current paper investigates whether strengthening students' HKU via participatory developed and implemented PE lessons is possible. In total, 233 students from eight different secondary schools took part in the study. Four schools (with two PE teachers at each school) comprised the intervention group and they participated in a 1-year participatory planning process to conceptualize and implement various PE lessons. PE teachers in the planning groups were advised to conceptualize their PE lessons in order to develop students' health-related knowledge and understanding. Meanwhile, the control schools carried out their regular PE lessons. Evaluation followed a mixed-methods approach, assessing program implementation as well as program effectiveness.
In relation to program effectiveness, results showed a significant intervention effect with a medium effect size, demonstrating the HKU-strengthening effect of the developed and implemented lessons. The results are in line with other studies addressing health-related knowledge and understanding. The majority (79,4%) of the studies investigated by Demetriou et al. (26) revealed significant positive intervention effects on students' health-related fitness knowledge. Effect sizes vary from small to large, depending on the nature of moderator variables such as defined learning outcomes and implementation of PE lessons.
Due to the participatory process in our intervention, those moderator variables also varied considerably in the involved schools. Therefore, we looked at school specific differences in the development of HKU. Students of intervention schools A, B, and D improved their HKU significantly, those at school C did not. The significant HKU-improvement of students in the intervention schools A, B, and D came along with large effect sizes (dA = 1.3 / dB = 1.0 / dD = 1.3). According to Hattie (60) an average increase of d = 0.4 (hinge point) across different subjects is regarded as a general development of students' ability over one school year whilst attending regular lessons. Thus, students at the interventions schools evidently over-performed. In contrary, students at intervention school C (dC = 0.2) improved their HKU less than the hinge point.
Differences match with findings in relation to the evaluation of program implementation. In all schools teaching units were implemented that–besides physical aspects–at least partly also addressed psychosocial aspects of health and thereby followed the required holistic understanding of health (14, 28). However, there were considerable differences concerning other principles of fostering HKU in PE (28), such as the inclusion and empowerment of all pupils via student-centered teaching approaches (49, 60) and the delivery of health-related knowledge with experiences through physical activity (61–63). Teaching units of schools A and B were fully compliant to those principles. Teachers of school D neglected some criteria of student-centered teaching approaches. However, they also prioritized educational aspects over direct health outcomes and combined delivery of health-related knowledge with physical experiences. In contrary, teachers from school C conceptualized and implemented PE lessons that were only marginally compliant to the aforementioned pedagogical principles. They only partly included cognitive activation as a student-centered teaching approach, but they did not consider elements of reflection, relevance to everyday life or collaborative learning. Furthermore, they only marginally delivered health-related knowledge, but did not combine this knowledge with physical experiences.
In summary, a participatory planning process involving teachers, principals, students and scientists is an adequate approach to conceptualize and implement evidence-based teaching methods within the school setting. Due to this intervention, students' HKU increased. An insight, which confirms existing findings from participatory approaches, which addresses active lifestyles in PE (64) or health promotion in the whole school context (65). The present study purposefully dispensed with any structured intervention programs for teachers to follow. Instead, students as well as teachers had the chance to articulate their specific needs and interests, but also their concerns about factors hindering the implementation of planned lessons. Thereby, teachers developed an understanding of effective teachings strategies in PE and carefully reflected on their current teaching methods and the existing practices at their schools. This is regarded as an important factor influencing the contribution of staff to health education at schools (66). Additionally, the integration of students in a partnership of equals in the planning groups increased their satisfaction with the process and their motivation to learn–important effects, which already have been found in other school health promotion interventions (67). However, the participatory planning does not always work in the intended manner (see results from school C), emphasizing that numerous contextual factors influence the implementation process (68, 69). In the context of the present study, the issue of individual readiness for organizational change arose particularly (70). It turned out that the readiness of the involved stakeholders to invest personal resources to change existing processes and beliefs is crucial. In that sense, teachers of school C were not willing to reflect and change their current teaching methods.
Strengths and Limitations
There are several strengths of this study. Through the participatory approach, we ensured that there was consideration of the students' voice and individual school requirements in health-promotion interventions within the school setting (7, 9). Furthermore, as there is a lack of an accurate empirical assessment of the outcomes of implemented teaching learning processes (23, 26), we used a well-developed and validated questionnaire for assessing the effects of our intervention on HKU. For data analysis, we used triangulation of techniques (i.e., comparison of data obtained by differing information collection techniques) and triangulation of analysis (contrasting and comparing the data analyses performed by different analysts to strengthen the credibility and confirmability of the study results) (71). However, some limitations do also exist. First, schools were not randomly assigned to either intervention or control group and the allocation was based on their willingness. However, criteria of randomization may be difficult to achieve within the school setting (5). Additionally, measurement of students' physical activity as well as school's climate, culture and ethos4 were not included, which could have provided further details for interpreting the results (72).
Conclusion
This study contributes to existing research on strengthening health-related knowledge and understanding in PE. It specifically investigates a participatory approach to develop and implement evidence-based teaching units for PE. The results are encouraging, showing the potential effects of this approach, if relevant principles of fostering HKU in PE are considered.
As strengthening of HKU is an accepted demand in German as well as international PE curricula, future efforts should focus on enabling PE teachers to consistently align their teaching with those PE curricula demands. Therefore, the follow-up project Health.edu PLUS will specifically address the participatory elaboration of a variety of best-practice examples in cooperation with different stakeholders concerned. Those exemplary teaching units will specifically address how to combine the delivery of health-related knowledge with physical experiences in PE. This can help to mitigate concerns expressed by some PE teachers that an intensified delivery of health-related knowledge could significantly reduce time for movement in PE (73). The elaborated examples will be linked to an Bavarian online platform, where all interested teachers can find information about PE curricula demands and can download exemplary teaching units to fulfill those demands. The provision and dissemination of agreed-upon examples of good practice will serve as a trigger for further development and implementation of strengthening HKU in PE.
Data Availability Statement
The datasets generated for this study are available on request to the corresponding author.
Ethics Statement
Ethical approval was obtained from the data security official of the University of Erlangen-Nuremberg and the Bavarian State Ministry for Education and Cultural Affairs (reference number X.7-BO4106/459/8). Parents and teachers provided written informed consent; additionally, all students provided written informed consent to participate in the study as well.
Author Contributions
HS was a major contributor in writing the manuscript and contributed to data collection. KP managed the data collection of the study and wrote a first draft of some sections of the manuscript. CT contributed to critical revision of the manuscript. RS contributed to the conception and design of this study. ST contributed to the conception and design of this study, wrote a first draft of some sections of the manuscript and contributed to critical revision of the manuscript. All authors read and approved the final manuscript.
Funding
The research network Capital4Health [grant number 01EL1421A] and the associated subproject Health.edu [grant number: 01EL1421D] in which the study took place, are funded by the German Federal Ministry for Education and Research (BMBF). This publication was funded by the German Research Foundation (DFG) and the University of Bayreuth in the funding programme Open Access Publishing.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Abbreviations
HKU, Health-related knowledge and understanding; PE, Physical education; PL, Physical literacy.
Footnotes
1. ^In Germany, there are 16 state-specific curricula, since education is a matter of federal states.
2. ^The project is part of a transdisciplinary research network Capital4Health (https://www.capital4health.de), which aims at fostering health enhancing physical activity in various population segments and settings.
3. ^In Germany, there are differences between secondary modern schools and grammar schools in relation to their educational level. Secondary modern schools are for practical-minded students and prepare for vocational training. Grammar schools are attended by students with above-average abilities and motivation and lead to the exam required for studies at university/college.
4. ^This is due to a very restrictive approval procedure of the Bavarian State Ministry of Education and Cultural Affairs.
References
2. World Health Organization Regional Office for Europe [WHO]. Closing the Gap in a Generation: Health Equity through Action on the Social Determinants of Health. Final Report of the Commission on Social Determinants of Health. Geneva: WHO (2008).
3. Antonovsky A. The salutogenetic model as a theory to guide health promotion. Health Promot Int. (1996) 11:11–8. doi: 10.1093/heapro/11.1.11
4. Centers for Disease Control and Prevention (CDC). School health guidelines to promote healthy eating and physical activity. MMWR Recomm Rep. (2011) 60:1–76.
5. Demetriou Y, Höner O. Physical activity interventions in the school setting: a systematic review. Psychol Sport Exercise. (2012) 13:186–96. doi: 10.1016/j.psychsport.2011.11.006
6. Paulus P. 20 Years of health promotion research in and on settings in Europe–the case of school health promotion. IJPH. (2007). 5:248–54.
7. Turunen H, Sormunen M, Jourdan D, von Seelen J, Buijs G. Health promoting schools-a complex approach and a major means to health improvement. Health Promot Int. (2017) 32:177–84. doi: 10.1093/heapro/dax001
8. Haerens L, Kirk D, Cardon G, de Bourdeaudhuij I. Toward the development of a pedagogical model for health-based physical education. Quest. (2011). 63:321–38. doi: 10.1080/00336297.2011.10483684
9. McCuaig L, Quennerstedt M, Macdonald D. A salutogenic, strengths-based approach as a theory to guide HPE curriculum change. Asia Pac J Health Sport Phys Educ. (2013) 4:109–25. doi: 10.1080/18377122.2013.801105
10. Australian Curriculum, Assessment and Reporting Authority. The Shape of the Australian Curriculum: Health and Physical Education. Sydney: ACARA Copyright Administration (2012).
11. Ministry of Education and Research, Government Offices of Sweden. Curriculum for the Compulsory School, Preschool Class and the Leisure-Time Centre. (2011). Stockholm (2011).
12. Gard M, Wright J. Managing uncertainty: obesity discourses and physical education in a risk society. Stud Philos Educ. (2001) 20:535–49. doi: 10.1023/A:1012238617836
13. Kirk D. Educational value and models-based practice in physical education. Educ Philos Theory. (2013) 45:973–86. doi: 10.1080/00131857.2013.785352
14. Ptack K, Tittlbach S. Pedagogical state of knowledge about health as a topic in physical education–a literature review. Int J Phys Educ. (2018) 2:28–41.
15. Bailey R, Armour K, Kirk D, Jess M, Pickup I, Sandford R, et al. The educational benefits claimed for physical education and school sport: an academic review. Res Pap Educ. (2009) 24:1–27. doi: 10.1080/02671520701809817
16. Palmer SE, Behrens TK. At the crossroads: how physical education can succeed in a public health paradigm. Quest. (2017) 69:467–79. doi: 10.1080/00336297.2017.1288145
17. Warburton DER, Bredin SSD. Health benefits of physical activity: a systematic review of current systematic reviews. Curr Opin Cardiol. (2017) 32:541–56. doi: 10.1097/HCO.0000000000000437
18. Guthold R, Stevens GA, Riley LM, Bull FC. Worldwide trends in insufficient physical activity from 2001 to 2016: a pooled analysis of 358 population-based surveys with 1·9 million participants. Lancet Global Health. (2018) 6:e1077–86. doi: 10.1016/S2214-109X(18)30357-7
19. Edwards LC, Bryant AS, Keegan RJ, Morgan K, Cooper S-M, Jones AM. 'Measuring' physical literacy and related constructs: a systematic review of empirical findings. Sports Med. (2018). 48:659–82. doi: 10.1007/s40279-017-0817-9
20. Lloyd M, Colley RC, Tremblay MS. Advancing the debate on ‘fitness testing' for 9 children: perhaps we're riding the wrong animal. Pediatr Exercise Sci. (2010) 22:176–82. doi: 10.1123/pes.22.2.176
21. Whitehead M. Definition of physical literacy and clarification of related issues. Bullet ICSSPE. (2013) 2013:28–33.
22. Whitehead M. The concept of physical literacy. Eur J Phys Educ. (2001) 6:127–38. doi: 10.1080/1740898010060205
23. Lundvall S. Physical literacy in the field of physical education–a challenge and a possibility. J Sport Health Sci. (2015) 4:113–8. doi: 10.1016/j.jshs.2015.02.001
24. Jurbala P. What is physical literacy, really? Quest. (2015) 67:367–83. doi: 10.1080/00336297.2015.1084341
25. Edwards LC, Bryant AS, Keegan RJ, Morgan K, Jones AM. Definitions, foundations and associations of physical literacy: a systematic review. Sports Med. (2017) 47:113–26. doi: 10.1007/s40279-016-0560-7
26. Demetriou Y, Sudeck G, Thiel A, Höner O. The effects of school-based physical activity interventions on students' health-related fitness knowledge: a systematic review. Educ Res Rev. (2015) 16:19–40. doi: 10.1016/j.edurev.2015.07.002
27. Whitehead M. Physical Literacy: Throughout the Lifecourse. 1st ed. London, New York, NY: Routledge. (2010). doi: 10.4324/9780203881903
28. Cale L, Harris J. The role of knowledge and understanding in fostering physical literacy. J Teaching Phys Educ. (2018) 37:280–7. doi: 10.1123/jtpe.2018-0134
29. Ennis C. Knowledge, transfer, and innovation in physical literacy curricula. J Sport Health Sci. 2015) 4:119–24. doi: 10.1016/j.jshs.2015.03.001
30. Balz E, Neumann P. Physical education in Germany. In: Pühse U, Gerber M, editors. International Comparison of Physical Education: Concepts - Problems - Prospects. Aachen: Meyer & Meyer. (2005) p. 292–309.
31. Kurz D. Von der Vielfalt sportlichen Sinns zu den pädagogischen Perspektiven im Schulsport. In: Neumann P, Balz E, editors. Mehrperspektivischer Sportunterricht. Orientierungen und Beispiele. Schorndorf: Hofmann. (2004) p. 57–70.
32. Brandl-Bredenbeck HP, Sygusch R. Highway to health – an innovative way to address health in Physical Education Teacher Education (PETE). Retos. (2017) 31:321–7.
33. Töpfer C. Sportbezogene Gesundheitskompetenz. Kompetenzmodellierung und Testentwicklung für den Sportunterricht [Sport-related health competence: Competence modelling and test development for physical education]. Hamburg: Feldhaus Edition Czwalina. (2019)
34. Hodges MG, Hodges Kulinna P. Teaching healthy behaviour knowledge in primary school physical education. Biomed Hum Kinetics. (2014) 6:33–9. doi: 10.2478/bhk-2014-0006
35. Armour K, Harris J. Making the case for developing new PE-for-health pedagogies. Quest. (2013) 65:201–19. doi: 10.1080/00336297.2013.773531
36. World Health Organization. Research to Improve Implementation and Effectiveness of School Health Programmes. Geneva: WHO (1996).
38. Pühse U, Barker D, Brettschneider W-D, Feldmeth AK, Gerlach E, McCuaig L, et al. International approaches to health-oriented physical education: local health debates and differing conceptions of health. Int J Phys Educ. (2011) 3:4–16.
39. Bisset S, Potvin L. Expanding our conceptualization of program implementation: lessons from the genealogy of a school-based nutrition program. Health Educ Res. (2007) 22:737–46. doi: 10.1093/her/cyl154
40. Hawe P, Noort M, King L, Jordens C. Multiplying health gains: the critical role of capacity- building within health promotion programs. Health Policy. (1997) 39:29–42. doi: 10.1016/S0168-8510(96)00847-0
41. Hawe P. Capacity building: for what? N S W Public Health Bull. (2000) 11:22–4. doi: 10.1071/NB00012
42. Leask CF, Sandlund M, Skelton DA, Altenburg TM, Cardon G, Chinapaw MJM, et al. Framework, principles and recommendations for utilising participatory methodologies in the co-creation and evaluation of public health interventions. Res Involv Engagem. (2019) 5:2. doi: 10.1186/s40900-018-0136-9
43. Laverack G, Wallerstein N. Measuring community empowerment: a fresh look at organizational domains. Health Promot Int. (2001) 16:179–85. doi: 10.1093/heapro/16.2.179
44. Sygusch R, Bähr I, Gerlach E, Bund A. Orientierungspunkte einer programmevaluation in der sportpädagogik [Orientation of a program evaluation in sports pedagogy]. Zeitschrift für sportpädagogische Forschung. (2013) 1:31–54.
45. Moore GF, Audrey S, Barker M, Bond L, Bonell C, Hardeman W, et al. Process evaluation of complex interventions: medical research council guidance. BMJ. (2015) 350:h1258. doi: 10.1136/bmj.h1258
46. Rütten A, Frahsa A, Abel T, Bergmann M, de Leeuw E, Hunter D, et al. Co-producing active lifestyles as whole-system-approach: theory, intervention and knowledge-to-action implications. Health Promot Int. (2019) 34:47–59. doi: 10.1093/heapro/dax053
47. Rütten A, Gelius P. Building policy capacities: an interactive approach for linking knowledge to action in health promotion. Health Promot Int. (2013) 29:569-82. doi: 10.1093/heapro/dat006
48. Frahsa A, Rütten A, Roeger U, Abu-Omar K, Schow D. Enabling the powerful? Participatory action research with local policymakers and professionals for physical activity promotion with women in difficult life situations. Health Promot Int. (2012) 29:171–84. doi: 10.1093/heapro/das050
49. Goodyear V, Dudley D. “I'm a facilitator of learning!” Understanding what teachers and students do within student-centered physical education models. Quest. (2015) 274–89. doi: 10.1080/00336297.2015.1051236
50. Hassandra M, Goudas M, Chroni S. Examining factors associated with intrinsic motivation in physical education: a qualitative approach. Psychol Sport Exercise. (2003) 4:211–23. doi: 10.1016/S1469-0292(02)00006-7
51. Mayring P. Qualitative Inhaltsanalyse: Grundlagen und Techniken. 12th ed. Weinheim: Beltz (2015).
52. Pope C, Ziebland S, Mays N. Qualitative research in health care. Analysing qualitative data. BMJ. (2000) 320:114–6. doi: 10.1136/bmj.320.7227.114
53. Richards L, Morse JM. Readme First for a user's Guide to Qualitative Methods. Los Angeles, London, New Dehli, Singapore, Wahsington DC: SAGE. (2013)
54. Tuckett AG. Part II. rigour in qualitative research: complexities and solutions. Nurse Res. (2005) 13:29–42. doi: 10.7748/nr2005.07.13.1.29.c5998
55. Berens E-M, Vogt D, Messer M, Hurrelmann K, Schaeffer D. Health literacy among different age groups in Germany: results of a cross-sectional survey. BMC Public Health. (2016) 16:1151. doi: 10.1186/s12889-016-3810-6
56. Sørensen K, Pelikan JM, Röthlin F, Ganahl K, Slonska Z, Doyle G, et al. Health literacy in Europe: comparative results of the European health literacy survey (HLS-EU). Eur J Public Health. (2015) 25:1053–8. doi: 10.1093/eurpub/ckv043
57. Vickers AJ, Altman DG. Statistics notes: analysing controlled trials with baseline and follow up measurements. BMJ. (2001) 323:1123–4. doi: 10.1136/bmj.323.7321.1123
58. Field A. Discovering Statistics using IBM SPSS Statistics: and Sex and Drugs and Rock'n'Roll. 4th ed. Los Angeles, Calif, London, New Delhi: SAGE (2015).
59. Morris SB. Estimating effect sizes from pretest-posttest-control group designs. Organ Res Methods. (2008) 11:364–86. doi: 10.1177/1094428106291059
60. Hattie J. Visible Learning for Teachers: Maximizing Impact on Learning. London, New York: Routledge Taylor & Francis Group. (2012) doi: 10.4324/9780203181522
61. Rink J. Teaching Physical Education for Learning. 6th ed. Boston: McGraw-Hill Higher Education. (2010).
63. Almond L, Myers L. Physical literacy and the primacy of movement. Physical Education Matters. (2017) 12:19–21.
64. Harris J, Cale L, Casey A, Tyne A, Samaria B. Promoting active lifestyles in schools: the PAL project. Phys Educ Matters. (2016) 11:52–3.
65. Pike J, Ioannou S. Evaluating school-community health in Cyprus. Health Promot Int. (2017) 32:185–94. doi: 10.1093/heapro/dat044
66. Jourdan D, Mannix McNamara P, Simar C, Geary T, Pommier J. Factors influencing the contribution of staff to health education in schools. Health Educ Res. (2010) 25:519–30. doi: 10.1093/her/cyq012
67. Griebler U, Rojatz D, Simovska V, Forster R. Effects of student participation in school health promotion: a systematic review. Health Promot Int. (2017) 32:195–206. doi: 10.1093/heapro/dat090
68. Durlak JA, DuPre EP. Implementation matters: a review of research on the influence of implementation on program outcomes and the factors affecting implementation. Am J Community Psychol. (2008) 41:327–50. doi: 10.1007/s10464-008-9165-0
69. Darlington EJ, Violon N, Jourdan D. Implementation of health promotion programmes in schools: an approach to understand the influence of contextual factors on the process? BMC Public Health. (2018) 18:163. doi: 10.1186/s12889-017-5011-3
70. Choi M, Ruona WEA. Individual readiness for organizational change and its implications for human resource and organization development. Hum Resour Dev Rev. (2011) 10:46–73. doi: 10.1177/1534484310384957
71. Pons-Vigués M, Berenguera A, Coma-Auli N, March S, Pombo H, Masluk B, et al. Qualitative evaluation of a complex intervention to implement health promotion activities according to healthcare attendees and health professionals: EIRA study (phase II). BMJ Open. (2019) 9:e023872. doi: 10.1136/bmjopen-2018-023872
72. St Leger L. Schools, health literacy and public health: possibilities and challenges. Health Promot Int. (2001) 16:197–205. doi: 10.1093/heapro/16.2.197
Keywords: physical literacy, physical activity (exercise), secondary school, physical education (P.E.), questionnaire, Health.edu
Citation: Strobl H, Ptack K, Töpfer C, Sygusch R and Tittlbach S (2020) Effects of a Participatory School-Based Intervention on Students' Health-Related Knowledge and Understanding. Front. Public Health 8:122. doi: 10.3389/fpubh.2020.00122
Received: 13 January 2020; Accepted: 26 March 2020;
Published: 24 April 2020.
Edited by:
Sunjoo Kang, Yonsei University, South KoreaReviewed by:
Miodraga Stefanovska-Petkovska, University of Lisbon, PortugalStacie Craft DeFreitas, University of Houston–Downtown, United States
Copyright © 2020 Strobl, Ptack, Töpfer, Sygusch and Tittlbach. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Helmut Strobl, helmut.strobl@uni-bayreuth.de