 Hairong Gong1
Hairong Gong1 Guoping Lu1
Guoping Lu1 Jian Ma1Jicui Zheng2Fei Hu1
Jian Ma1Jicui Zheng2Fei Hu1 Jing Liu1
Jing Liu1 Jun Song3Shenjie Hu1Libo Sun1Yang Chen1
Jun Song3Shenjie Hu1Libo Sun1Yang Chen1 Li Xie4
Li Xie4 Xiaobo Zhang5Leilei Duan6
Xiaobo Zhang5Leilei Duan6 Hong Xu7*
Hong Xu7*- 1Emergency Department, Children's Hospital of Fudan University, Shanghai, China
- 2Department of Neurosurgery, Children's Hospital of Fudan University, Shanghai, China
- 3Department of Orthopedics, Children's Hospital of Fudan University, Shanghai, China
- 4Clinical Research Institute, Shanghai Jiao Tong University School of Medicine, Shanghai, China
- 5Department of Respiratory, Children's Hospital of Fudan University, Shanghai, China
- 6Division of Injury Prevention and Mental Health, National Center for Chronic and Non-communicable Disease Control and Prevention, Chinese Center for Disease Control and Prevention, Beijing, China
- 7Department of Nephrology, Children's Hospital of Fudan University, Shanghai, China
Background: Child unintentional injuries have become a hot topic worldwide, and substantial regional disparities existed in causes and characteristics. To date, limited data are available to investigate the causes and characteristics of child unintentional injuries from hospitals for children in China.
Methods: A cross-sectional study was conducted between January 2017 and December 2018 in Shanghai, China. Patients aged <18 years with an unintentional injury presented to the emergency department were enrolled. Demographic information, Pediatric Risk for Mortality III score, and outcome variables were retrieved from electronic health records (EHRs). Frequencies and proportions of categorical variables and means and SDs of continuous variables are presented. Chi-square test and Student's t-test were used for the comparison between groups, as appropriate. Logistic regression analysis was used to estimate potential risk factors for admission to the hospital.
Results: A total of 29,597 cases with unintentional injuries were identified between January 2017 and December 2018, with boys vs. girls ratio of 1.75. Preschool children account for approximately two-thirds of unintentional injuries in the emergency department. A distinctive pattern of mechanisms of unintentional injuries between gender was documented, and sports injury was significantly higher in boys than in girls (10.2 vs. 7.8%). Compared with Canadian Emergency Department Triage and Acuity Scale (CTAS) Grade 3 patients, Grade 2 [odds ratio (OR) = 2.99, 95% CI = 1.93–4.63, P < 0.001] and Grade 1 (OR = 74.85, 95% CI = 12.93–433.14, P < 0.001) patients had higher risk of inhospital admission. For causes of injuries, compared with falling, foreign body and poison had a lower risk of inhospital admission, while transport injury (OR = 1.31, 95% CI = 1.07–1.59, P = 0.008) and high fall injury (OR = 2.58. 95% CI =1.48–4.49, P < 0.001) had a significantly higher risk of admission.
Conclusions: There was a significant relationship between age-groups and unintentional injuries between gender, with decreased injuries among girls growing up older. Preventive measures should be taken to reduce transport injury and high fall injury, which had a significantly higher risk of admission.
Background
Unintentional injuries have become a hot topic worldwide in public health due to the high disability and mortality. Compared with adults, children and adolescents are at higher risk of suffering from unintentional injuries (1, 2). Unintentional injury is one of the leading causes of death for children of all ages; in 2013, it nearly accounted for 15.4% of the 2.6 million deaths of children aged 1–14 years (1, 3). In 2017, more than 6 million children and young adults were injured seriously enough who need to visit a hospital emergency department (4). Unintentional injuries are also a primary cause of disability, which can have a lasting impact on all aspects of the lives of the children, namely, relationships, learning, and games. The severe injury also leads to emotional trauma and financial burden for families and society (5). Caring for the unintentionally injured child requires specialized knowledge, precise management, and scrupulous attention to detail.
There are substantial regional disparities in causes and characteristics of unintentional pediatric injuries. Previous epidemiologic studies conducted in the United States have reported that unintentional falls are the leading cause of non-fatal injury in children presenting to hospital emergency departments, followed by being struck by or against an object (6). Another study in Nepal reported that falls are the most common cause of unintentional injuries among children (6). Due to the rapid development of the economics of society and the widespread use of comprehensive vaccination programs, the healthcare of children in China has changed significantly over the past 50 years. Although the hospital-based passive surveillance of the national injury surveillance system of medical and health institutions has been well established in China, the monitoring hospitals were not stratified according to hospital for children (7). Considering the majority of younger patients tend to visit the hospitals for children (8), the unstratified national injury surveillance for the hospital for children might cause a potential bias on the report of unintentional pediatric injuries.
A comprehensive assessment of causes and characteristics of child unintentional injury is an essential foundation for selecting and formulating injury prevention strategies and improving emergency and acute care services for injured children. To date, limited data are available to investigate the causes and characteristics of child unintentional injuries from hospitals for children in China. Therefore, we conducted a cross-sectional study to investigate the epidemiologic characteristics and causes of the unintentionally injured child presenting to the emergency department, which is expected to serve as the basis for a piece of in-depth evidence for the child injury prevention control measures.
Methods
Study Design and Participants
A cross-sectional, retrospective study was conducted on patients who visited the Emergency Department of Children's Hospital of Fudan University from January 2017 to December 2018. We included children and adolescents aged under 18 years, with a diagnosis of unintentional injury. An unintentional injury is defined as “an unexpected, unintentional, and violent event, affecting a child, with or without detectable lesions, and subsequently leading to medical attention; the injury may have been caused by a fall, poisoning, drowning, burns, or traffic-related accidents.” We excluded all patients with intentional injuries, such as abuse. The study protocol was approved by the Institutional Review Board and Ethics Committee of Children's Hospital of Fudan University and waived the need for the informed consent of parents due to the retrospective nature of the study design. This study was conducted in accordance with the Declaration of Helsinki and reported in accordance with the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines.
Data Collection and Measurement
Unintentional injuries were identified by using The International Classification of Diseases (ICD-10) codes: S00-S99, T00-T98, V01-V99, W00-W90, X00-X99, and Y00-Y34, which included motor vehicle crash injuries, falls, drowning, poisoning, suffocation, and animal bites. Data were collected based on the inclusion and exclusion criteria, demographics, clinical characteristics, and outcome measures. The medical records and rescue register records of the emergency children were reviewed in detail, and the admission records were reviewed through the electronic health records (EHRs) to determine their outcome.
Statistical Analysis
Descriptive statistics were calculated first, including means, SDs, and percentages. Frequencies and proportions of categorical variables and means and SDs of continuous variables are presented. The chi-square test was used to explore the significance of differences between groups, and Student's t-test was used for the comparison of continuous variables. To explore the risk factors of clinical outcome, unconditional logistic regression models were used to assess the associations between potential factors and outcomes after the emergency. All statistical procedures were performed using R software (version 3.4.4). A two-sided P < 0.05 was considered statistically significant.
Results
Overall Characteristics of Patients With Unintentional Injuries
As shown in Table 1, a total of 29,597 cases with unintentional injuries were identified between January 2017 and December 2018, with boys vs. girls ratio of 1.75. The mean age of patients with unintentional injuries was 5.15 ± 3.79 (mean ± SD). There was a significant relationship between age-groups and injuries between gender, with decreased injuries among girls when growing up older. Preschool children under the age of 6 years old account for approximately 64.6% of unintentional injuries in the emergency department (Table 2).
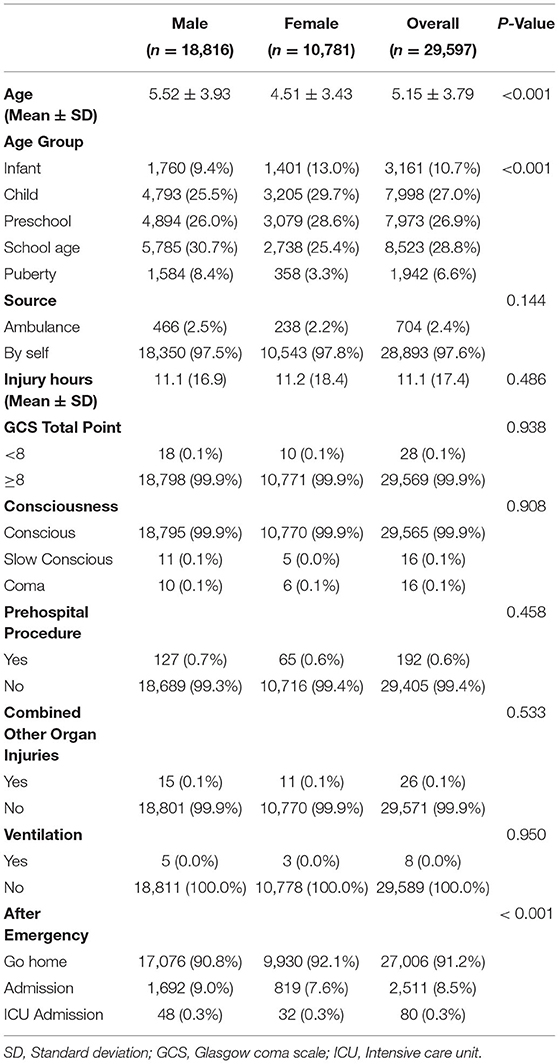
Table 1. Characteristics of child unintentional injury patient in the emergency department.
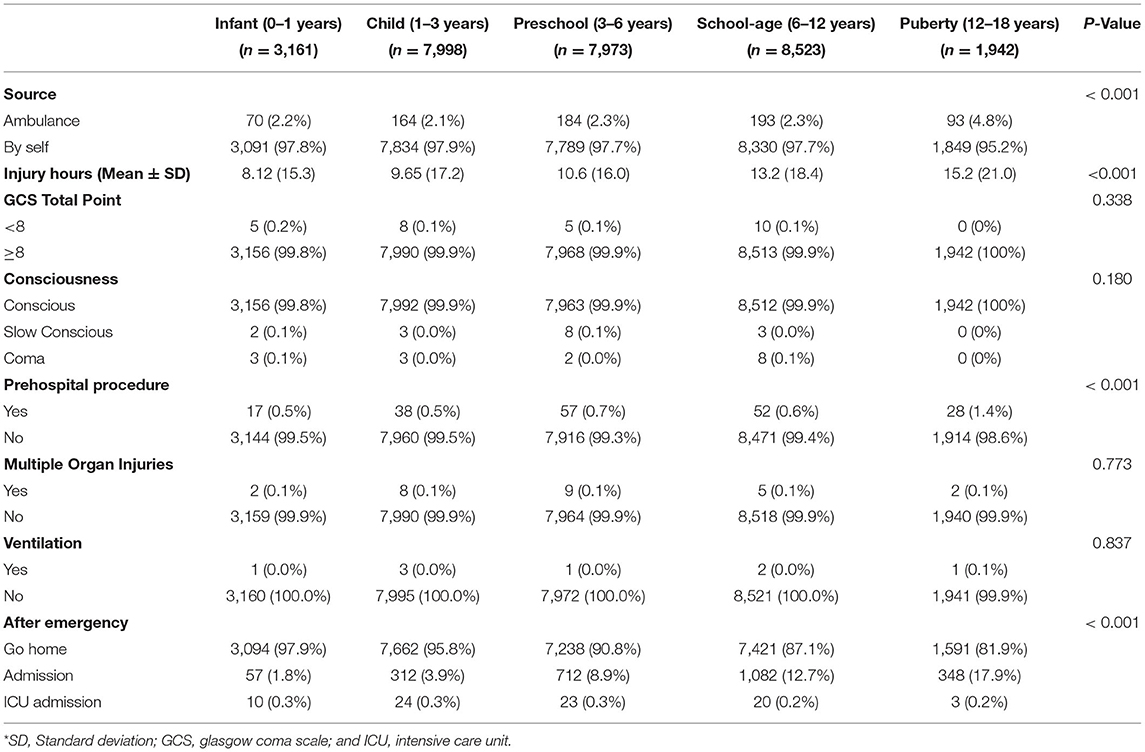
Table 2. Characteristics of child unintentional injury patient in the emergency department by age-group.
Mechanisms of Unintentional Injuries by Gender
Unintentionally fall was the most common reason for unintentional injuries among both the gender, accounting for 72.2% cases of unintentional injury, with 71.8% and 72.9% for boys and girls, respectively (Table 3, Figure 1). Following fall, the frequency of observed mechanism of injury was sports (9.3%), foreign body (6.4%), struck (4.9%), transport (4.1%), poison (1.2%), cut or pierce (0.9%), and high fall (0.4%). A distinctive pattern of mechanisms of unintentional injuries between gender was documented, and sports were significantly higher in boys than in girls (10.2 vs. 7.8%).
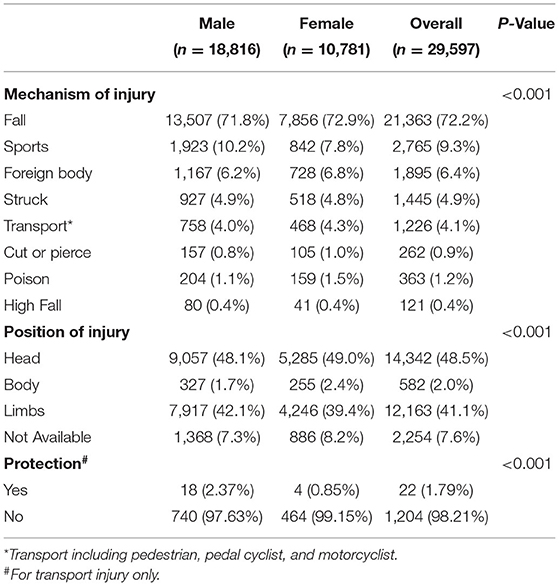
Table 3. Mechanism of child unintentional injury in the emergency department.
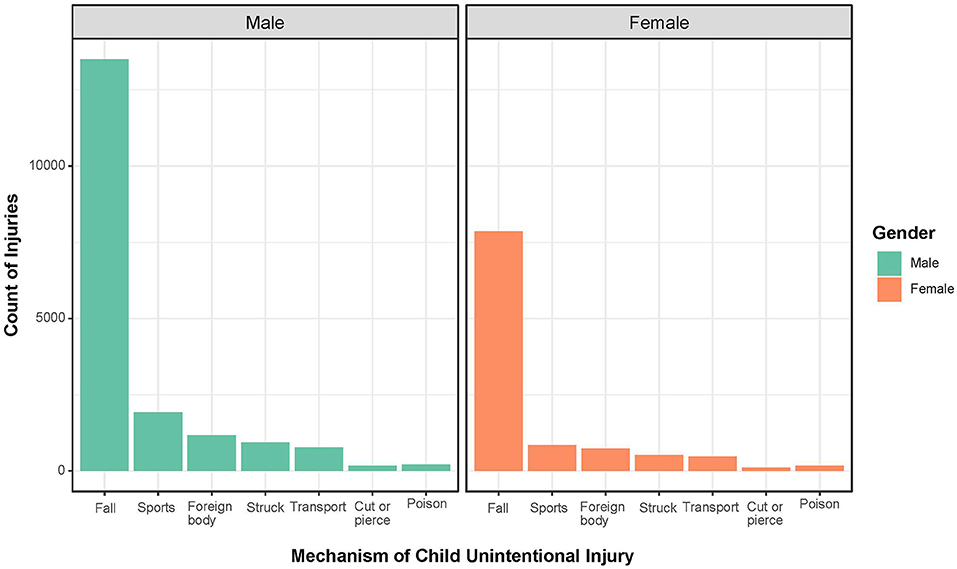
Figure 1. Mechanism of child unintentional injuries by gender in the emergency department. Gender was colored by green (boys) and orange (girls). X row represents the mechanism of child unintentional injuries. Y row represents the count of injuries.
Mechanisms of Unintentional Injuries by Age-Groups
There was a significantly different pattern of the mechanism of injury among age-groups (Table 4, Figure 2). As they grow up older, there was a decreased prevalence of falls among age-groups, with 85.8% among 0–1 year old vs. 49.7% among 12–18 years of puberty. Fall (85.5%), foreign body (7.4%), and struck (1.5%) were the top three reasons for unintentional injury among 0–1-year age-group. Among the age-group of 1–3 years, the common reasons for unintentional injury were fall (77.7%), foreign body (10.2%), and transport (3.6%). Similarly, in the preschool group (aged 3–6 years), fall (76.8%), foreign body (6.4%), and transport (6.0%) were the top three reasons for unintentional injury. Among school-age (6–12 years) and puberty (12–18) groups, the top three reasons for unintentional injury were fall, sports, and transport.
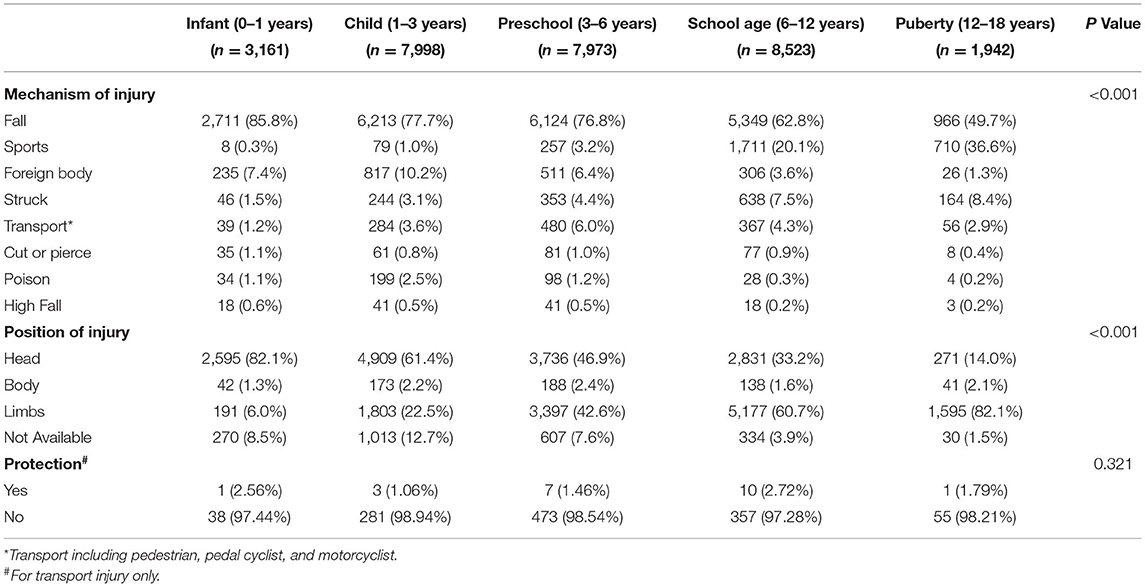
Table 4. Mechanism of child unintentional injury in the emergency department by age-group.
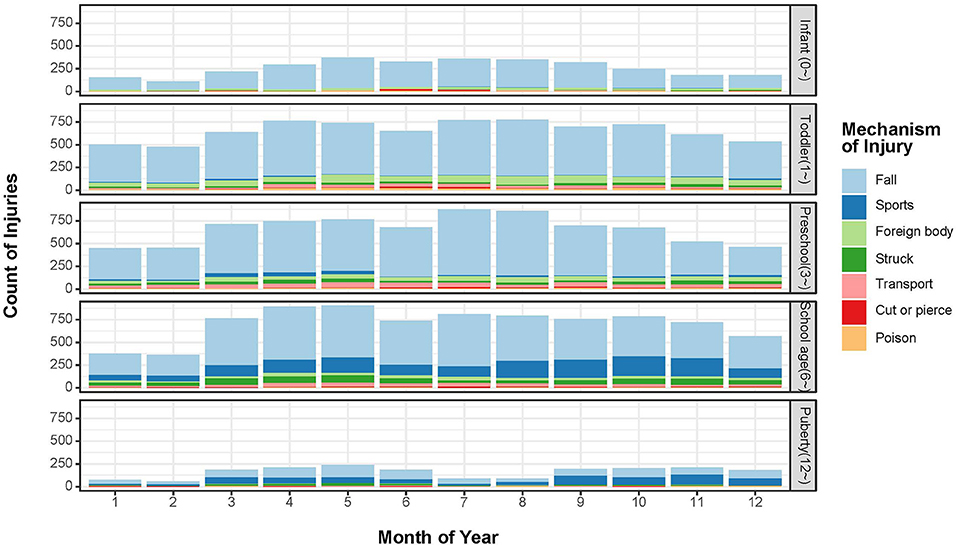
Figure 2. Time trends of child unintentional injury mechanisms by age-group. X row represents the month of the year. Y row represents the count of injuries. Child unintentional injury mechanisms were stacked by different colors.
Association Between Characteristics of Unintentional Injuries and Clinical Outcomes
We analyze the association between characteristics of unintentional injuries and inhospital admission by multivariable logistic regression. We found that there was no statistical difference between male and female patients. Patients transferred by ambulance had elevated the risk of inhospital admission than the patient who came by themselves [odds ratio (OR) = 2.30, 95% CI = 1.51–3.51, P < 0.001]. Compared with Grade 3 of CTAS patients in the emergency department, Grade 2 (OR = 2.99, 95% CI = 1.93–4.63, P < 0.001) and Grade 1 of CTAS (OR = 74.85, 95% CI = 12.93–433.14, P < 0.001) patients had statistically higher risk of inhospital admission. For different mechanisms of injuries, compared with fall, foreign body (OR = 0.37, 95% CI = 0.27–0.51, P < 0.001) and poison (OR = 0.10, 95% CI = 0.04–0.29, P < 0.001) had lower risk of inhospital admission, while transport (OR = 1.31, 95% CI = 1.07–1.59, P = 0.008) and high fall (OR = 2.58. 95% CI = 1.48–4.49, P < 0.001) had a significantly higher risk of admission. The results of the multivariate analysis are shown in Table 5.
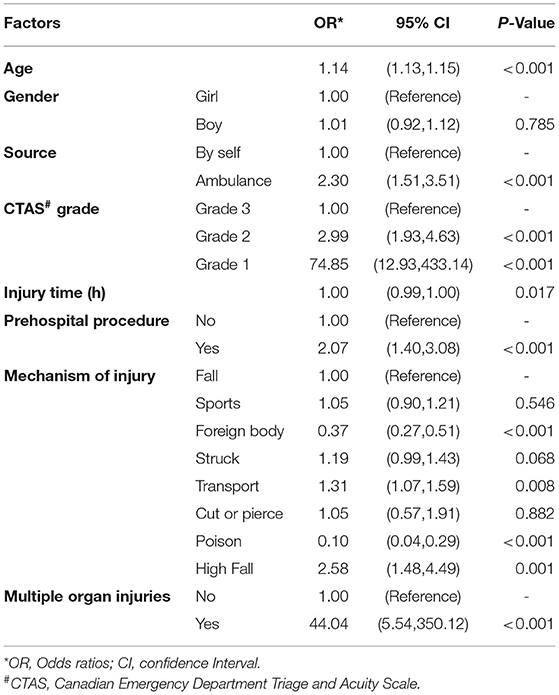
Table 5. Risk factors of admission in hospital among child unintentional injury patient in the emergency department.
Discussion
In this study, we observed the variation in causes and characteristics of child unintentional injury by age-group and gender in the emergency department. Preschool children under the age of 6 years old account for approximately 64.6% of unintentional injuries in the emergency department. The CTAS Grade 2 and Grade 1 patients had a statistically higher risk of inhospital admission.
Among all age-group, our study found that the proportion of unintentional injuries was significantly higher in boys than girls, which is in agreement with the previous studies (9). The elevated risk might associate with a higher level of activates and a different pattern of behaviors among boys and girls. Consistent with the previous studies, unintentional falls are the leading cause of non-fatal injuries in emergency department visits among children under the age of 14 years old (10–12). A previous study that has examined falls in children provided some information on young children who experience fall injuries and the circumstances of the fall. Compared to older children, children under the age of 5 years old are more likely to sustain head injuries, be hospitalized, or die from falls (13). Child protection strategies have been widely recognized and publicly supported. Child unintentional injuries are one of the most prominent global health threats, and parents may play a vital role in preventing these injuries. There has been speculation that the one-child policy has led to greater parental attention to children, thus resulting in considerable improvements in the younger age-groups, as many injuries may be due to a lack of supervision or dangerous circumstances (14, 15). In addition, the behaviors of children should be taken into consideration when developing prevention measures.
Most unintentional injuries are mild and do not require extra treatment such as inhospital admission. However, a small proportion of patients might present as having mild injuries but have clinically significant injuries. Although CT provides a definitive and rapid diagnosis to confirm or exclude intracranial injuries, there is concern about radiation-induced cancer, particularly in young patients. A national-wide injury surveillance study found that although the incidence of injuries increased between 1990 and 2017 in China, the injury burden in terms of mortality and disability-adjusted life year greatly improved (16).
To better perform prevention measures of unintentional injuries in children, it is essential to take more consideration of child development and parental supervision when designing prevention efforts. Prevention of unintentional injury for children should be included in all survival, maternal, and child health programs and integrated into all primary healthcare systems, both in high-income and low-income countries or intermediate-income countries. In China, with the improvement of the living conditions and the development of healthcare, the deaths of children caused by infectious diseases have been effectively controlled and unintentional injuries are gradually becoming the main cause of death among children under the age of 5 years old (17, 18). In addition to injury prevention, programs should improve emergency and acute care services for the injured children and strengthen rehabilitation programs. Also, parents teaching safety rules could reduce risks of unintentional child injuries and modestly improve child safety behaviors (19).
Strengths and Weaknesses of the Study
Our study had some strengths, such as collecting data from the emergency department is a reliable and efficient way to obtain information on the unintentional injury of children and has a relatively large sample size. This study had several limitations. First, this cross-sectional study in nature had no long-time follow-up of unintentional injuries patients. Outcomes were determined by a review of EHRs in detail. Second, we failed to collect data on risk factors related to unintentional injuries, such as physical and mental health conditions of children before the accident, family characteristics, family income, and educational level of parents. As a result, we cannot quantify the other risk factors for unintentional injuries. Future studies should measure these factors relating to unintentional injuries among children more explicitly. Third, our study was based on the data of a single hospital, which might restrict the generalizability of findings from this study.
Conclusions
Our study found that significant variation exists in causes and characteristics of child unintentional injury by age-group and gender in the emergency department. There was a significant relationship between age-groups and unintentional injuries between gender, with decreased injuries among girls growing up older. Preventive measures should be taken to reduce transport injury and high fall injury, which had a significantly higher risk of admission.
Data Availability Statement
The raw data supporting the conclusions of this article are available from the corresponding author by request.
Ethics Statement
The studies involving human participants were reviewed and approved by Institutional Review Board and Ethics Committee of Children's Hospital of Fudan University. Written informed consent from the participants' legal guardian/next of kin was waived due to the retrospective nature of the study design, which in accordance with the national legislation and the institutional requirements.
Author Contributions
HG and HX conceptualized and designed the study, coordinated and supervised data collection, contributed to data interpretation, drafted the initial manuscript, and reviewed and revised the manuscript. GL, JM, JZ, FH, JL, JS, SH, LS, YC, and LX designed the data collection instruments and collected data. LX carried out the statistical and formal analysis and interpretation. XZ and LD critically reviewed the manuscript for important intellectual content. All authors revised the manuscript and approved the final manuscript as submitted and agreed to be accountable for all aspects of the work.
Funding
This study was supported by the Children's Hospital of Fudan University Grant (Grant No. 2020ZBDL12).
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's Note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Abbreviations
EHR, Electronic health records; CTAS, Canadian Emergency Department Triage and Acuity Scale; ICD-10, The International Classification of Diseases 10; OR, Odds ratio; CI, Confidence interval; SD, Standard deviations.
References
1. Alonge O, Hyder AA. Reducing the global burden of childhood unintentional injuries. Arch Dis Child. (2014) 99:62–9. doi: 10.1136/archdischild-2013-304177
2. Lao Z, Gifford M, Dalal K. Economic cost of childhood unintentional injuries. Int J Prev Med. (2012):3:303–12.
3. Alonge O, Khan UR, Hyder AA. Our Shrinking globe: implications for child unintentional injuries. Pediatr Clin N Am. (2016) 63:167–81. doi: 10.1016/j.pcl.2015.08.009
4. National Center for Health Statistics (US). Health, United States, 2017: With Special Feature on Mortality [Internet]. Hyattsville (MD): National Center for Health Statistics (US) (2018).
5. Sleet D. The Global Challenge of Child Injury Prevention. Int J Env Res Pub He. (2018) 15:1921. doi: 10.3390/ijerph15091921
6. Pant P, Towner E, Ellis M, Manandhar D, Pilkington P, Mytton J. Epidemiology of Unintentional Child Injuries in the Makwanpur District of Nepal: A Household Survey. Int J Env Res Pub He. (2015) 12:15118–28. doi: 10.3390/ijerph121214967
7. Yang C. Research on the Monitoring Point Adjustment of the National Injury Surveillance System of Medical and Health Institutions [Master]. Chinese Center for Disease Control and Prevention (2016).
8. Zhang X, Shi P, Zheng S, et al. An analysis of characteristics and trends of outpatient visits and medical services in a tertiary pediatric hospital in Shanghai from 2009 to 2018. Chinese Journal of Evidence-Based Pediatrics. (2019) 14:161–8. doi: 10.3969/j.issn.1673-5501.2019.03.001
9. Wang Y, Ye P, Duan L. Characteristics of unintentional and intentional injuries among children from emergency and outpatient rooms in China, 2006-2014. Chinese Journal of Disease Control & Prevention. (2016) 20:670–74.
10. Taylor CA, Bell JM, Breiding MJ, Xu L. Traumatic Brain Injury-Related Emergency Department Visits, Hospitalizations, and Deaths - United States, 2007 and 2013. MMWR Surveill Summ. (2017) 66:1–16. doi: 10.15585/mmwr.ss6609a1
11. Wang D, Zhao W, Wheeler K, Yang G, Xiang H. Unintentional fall injuries among US children: a study based on the National Emergency Department Sample. Int J Inj Contr Saf Promot. (2013) (1):27–35. doi: 10.1080/17457300.2012.656316
12. Centers for Disease Control and Prevention. Web-based Injury Statistics Query and Reporting System (WISQARS). Leading Causes of Nonfatal Injury Reports (2003). Available online at: https://www.cdc.gov/injury/wisqars/nonfatal.html (accessed July 15, 2021).
13. Pomerantz WJ, Gittelman MA, Hornung R, Husseinzadeh H. Falls in children birth to 5 years: different mechanisms lead to different injuries. J Trauma Acute Care Surg. (2012) 73:S254–7. doi: 10.1097/TA.0b013e31826b017c
14. Li L, Yang J. Injury prevention in china: government-supported initiatives on the leading causes of injury-related deaths. Am J Public Health. (2019) 109:557–558. doi: 10.2105/AJPH.2019.304954
15. Hesketh T, Lu L, Xing ZW. The effect of China's one-child family policy after 25 years. N Engl J Med. (2005) 353:1171–6. doi: 10.1056/NEJMhpr051833
16. Leilei D, Pengpeng Y, Haagsma JA, Ye J, Yuan W, Yuliang E, et al. The burden of injury in China, 1990–2017: findings from the Global Burden of Disease Study 2017. The Lancet Public Health. (2019) 4:e449–61. doi: 10.1016/S2468-2667(19)30125-2
17. He C, Liu L, Chu Y, Perin J, Dai L, Li X, et al. National and subnational all-cause and cause-specific child mortality in China, 1996-2015: a systematic analysis with implications for the Sustainable Development Goals. Lancet Glob Health. (2017) 5:e186–7. doi: 10.1016/S2214-109X(16)30334-5
18. He C, Kang L, Miao L, Li Q, Liang J, Li x, et al. Pneumonia Mortality among Children under 5 in China from 1996 to 2013: An Analysis from National Surveillance System. Plos ONE. (2015) 10:e133620. doi: 10.1371/journal.pone.0133620
Keywords: unintentional injury, children, characteristics, emergency department, prevention
Citation: Gong H, Lu G, Ma J, Zheng J, Hu F, Liu J, Song J, Hu S, Sun L, Chen Y, Xie L, Zhang X, Duan L and Xu H (2021) Causes and Characteristics of Children Unintentional Injuries in Emergency Department and Its Implications for Prevention. Front. Public Health 9:669125. doi: 10.3389/fpubh.2021.669125
Received: 18 February 2021; Accepted: 30 June 2021;
Published: 05 August 2021.
Edited by:
Paolo Vineis, Imperial College London, United KingdomReviewed by:
Cihad Dundar, Ondokuz Mayis University, TurkeySelda Rizalar, University of Health Sciences (Turkey), Turkey
Copyright © 2021 Gong, Lu, Ma, Zheng, Hu, Liu, Song, Hu, Sun, Chen, Xie, Zhang, Duan and Xu. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Hong Xu, hxu@shmu.edu.cn