
Antibiotic Resistance Prevalence and Trends in Patients Infected with Helicobacter pylori in the Period 2013–2020: Results of the European Registry on H. pylori Management (Hp-EuReg)

 , , ,
, , ,  , , , , and add
Show full author list
, , , , and add
Show full author list
Abstract
:1. Introduction
2. Results
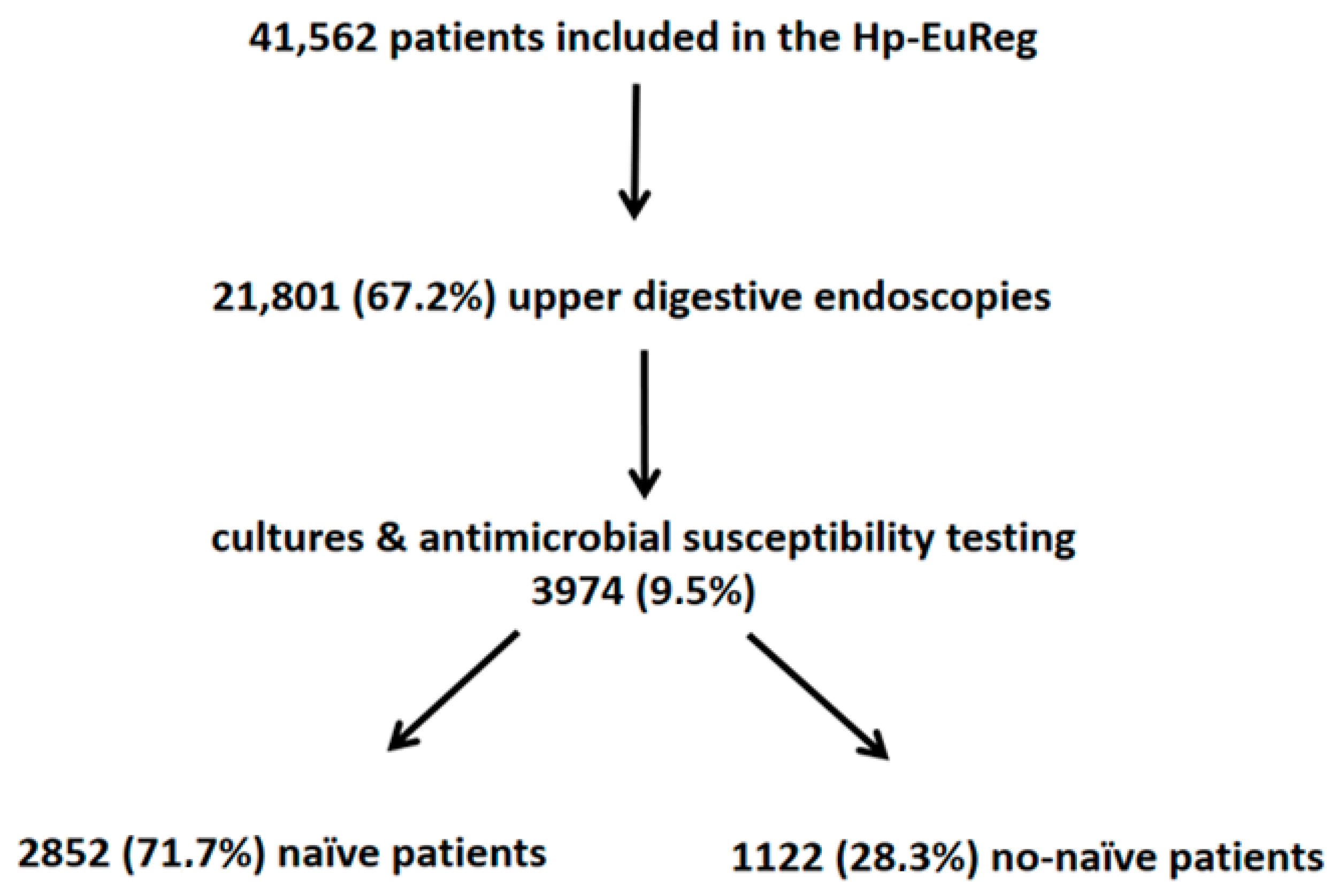
2.1. Characteristics of the Participants
2.2. H. pylori Antibiotic Resistance in Naïve Patients
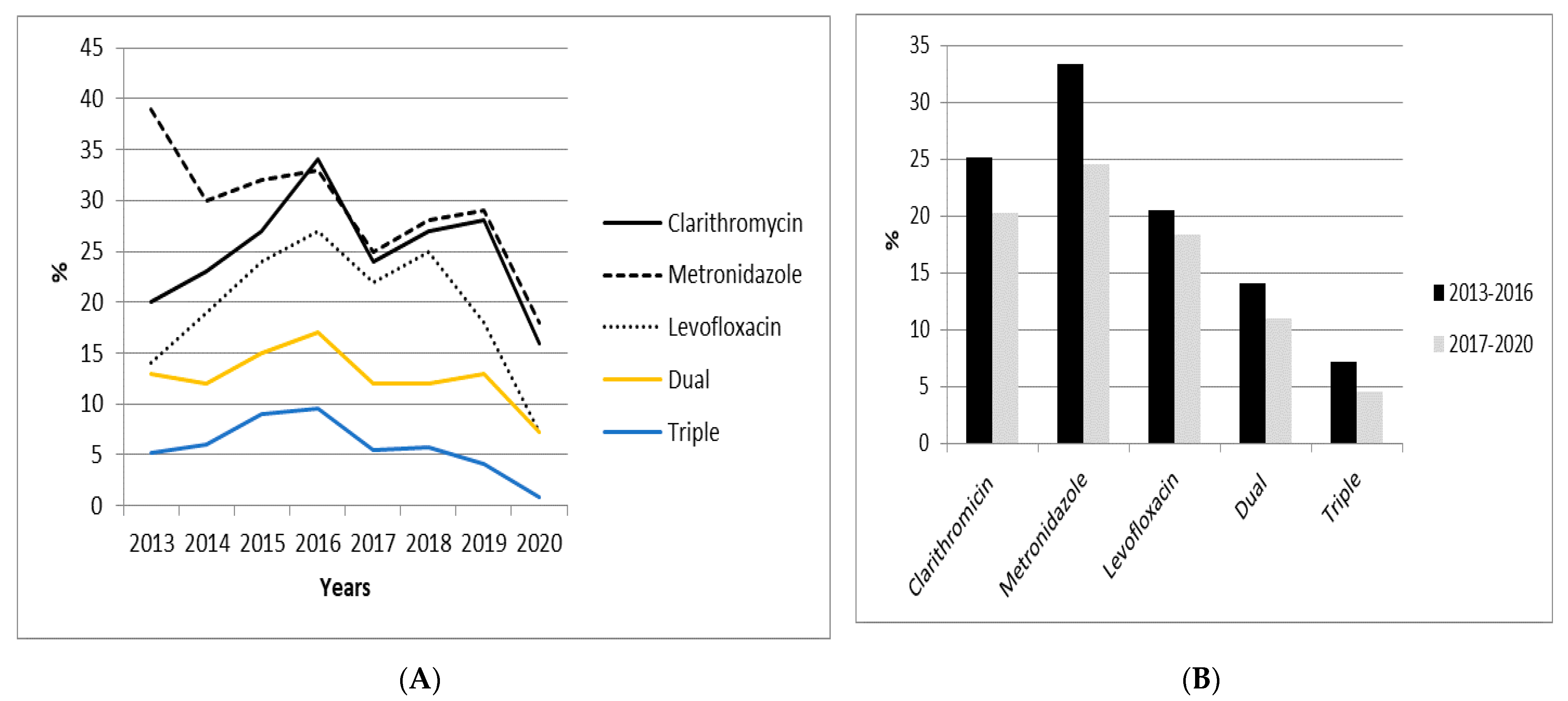
2.3. Evolution of Antibiotic Resistance from 2013 to 2020 in Naïve Patients
2.4. H. pylori Resistance in Naïve Patients per Country and Geographical Area
2.5. H. pylori Antibiotic Resistance in Non-Naïve Patients
3. Discussion
4. Materials and Methods
4.1. European Registry on Helicobacter pylori Management
4.2. Selection Criteria
4.3. Data Management and Analysis
4.4. Statistical Analyses
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Savoldi, A.; Carrara, E.; Graham, D.Y.; Conti, M.; Tacconelli, E. Prevalence of Antibiotic Resistance in Helicobacter pylori: A Systematic Review and Meta-analysis in World Health Organization Regions. Gastroenterology 2018, 155, 1372–1382.e17. [Google Scholar] [CrossRef] [Green Version]
- Hooi, J.K.Y.; Lai, W.Y.; Ng, W.K.; Suen, M.M.Y.; Underwood, F.E.; Tanyingoh, D.; Malfertheiner, P.; Graham, D.Y.; . Wong, V.W.S.; Wu, J.C.Y.; et al. Global Prevalence of Helicobacter pylori Infection: Systematic Review and Meta-Analysis. Gastroenterology 2017, 153, 420–429. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- IARC Working Group on the Evaluation of Carcinogenic Risks to Humans. Biological agents. Volume 100 B. A review of human carcinogens. IARC Monogr. Eval. Carcinog. Risks Hum. 2012, 100, 1–441. [Google Scholar]
- World Health Organization: List of Bacteria for Which New Antibiotics Are Urgently Needed. 2017. Available online: http://who.int/mediacentre/news/releases/2017/bacteria-antibiotics-needed/en/ (accessed on 27 February 2017).
- Glupczynski, Y.; Mégraud, F.; Lopez-Brea, M.; Andersen, L.P. European multicenter survey of in vitro antimicrobial resistance in Helicobacter pylori. Eur. J. Clin. Microbiol. Infect. Dis. 2001, 20, 820–823. [Google Scholar] [CrossRef] [PubMed]
- Megraud, F.; Bruyndonckx, R.; Coenen, S.; Wittkop, L.; Huang, T.D.; Hoebeke, M.; Bénéjat, L.; Lehours, P.; Goossens, H.; Glupczynski, Y.; et al. Helicobacter pylori resistance to antibiotics in Europe in 2018 and its relationship to antibiotic consumption in the community. Gut 2021. Available online: https://pubmed.ncbi.nlm.nih.gov/33837118/ (accessed on 26 August 2021).
- Gisbert, J.P.; Molina-Infante, J.; Amador, J.; Bermejo, F.; Bujanda, L.; Calvet, X.; Castro-Fernández, M.; Cuadrado-Lavín, A.; Elizalde, J.I.; Gene, E.; et al. IV Spanish Consensus Conference on Helicobacter pylori infection treatment. Gastroenterol. Hepatol. 2016, 39, 697–721. [Google Scholar] [CrossRef] [PubMed]
- Wu, J.Y.; Liou, J.M.; Graham, D.Y. Evidence-based recommendations for successful Helicobacter pylori treatment. Expert. Rev. Gastroenterol. Hepatol. 2014, 8, 21–28. [Google Scholar] [CrossRef]
- Valle Muñoz, J.; Muñoz Gómez, P.; Sierra Bernal, C.; de Andrés, E.; Gómez Hernando, C.; Gómez Rodríguez, R. Tailored Helicobacter pylori eradication based on prior intake of macrolide antibiotics allows the use of triple therapy with optimal results in an area with high clarithromycin resistance. Rev. Esp. Enferm. Dig. 2019, 111, 655–661. [Google Scholar] [CrossRef]
- Mégraud, F. H pylori antibiotic resistance: Prevalence, importance, and advances in testing. Gut 2004, 53, 1374–1384. [Google Scholar] [CrossRef] [Green Version]
- Van Boeckel, T.P.; Gandra, S.; Ashok, A.; Caudron, Q.; Grenfel, B.T.; Levin, S.A.; Laxminarayan, R. Global antibiotic consumption 2000 to 2010: An analysis of national pharmaceutical sales data. Lancet. Infect. Dis. 2014, 14, 742–750. [Google Scholar] [CrossRef]
- Mégraud, F. Antibiotic Resistance Is the Key Element in Treatment of Helicobacter pylori Infection. Gastroenterology 2018, 155, 1300–1302. [Google Scholar] [CrossRef] [Green Version]
- Megraud, F.; Coenen, S.; Versporten, A.; Kist, M.; Lopez-Brea, M.; Hirschl, A.M.; Andersen, L.P.; Goossens, H.; Glupczynski, Y.; Study Group, participants. Helicobacter pylori resistance to antibiotics in Europe and its relationship to antibiotic consumption. Gut 2013, 62, 34–42. [Google Scholar] [CrossRef]
- Lim, S.G.; Park, R.W.; Shin, S.J.; Yoon, D.; Kang, J.K.; Hwang, J.C.; Kim, S.S.; Kim, J.H.; Lee, K.M. The relationship between the failure to eradicate Helicobacter pylori and previous antibiotics use. Dig. Liver. Dis. 2016, 48, 385–390. [Google Scholar] [CrossRef]
- Liou, J.M.; Chen, P.Y.; Kuo, Y.T.; Wu, M.S.; Taiwan Gastrointestinal Disease and Helicobacter Consortium. Toward population specific and personalized treatment of Helicobacter pylori infection. J. Biomed. Sci. 2018, 25, 70. [Google Scholar] [CrossRef] [PubMed]
- Nyssen, O.P.; McNicholl, A.G.; Gisbert, J.P. Meta-analysis of three-in-one single capsule bismuth-containing quadruple therapy for the eradication of Helicobacter pylori. Helicobacter 2019, 24, e12570. [Google Scholar] [CrossRef] [PubMed]
- Cosme, A.; Montes, M.; Martos, M.; Gil, I.; Mendarte, U.; Salicio, Y.; Piñeiro, L.; Recasens, M.T.; Ibarra, B.; Sarasqueta, C.; et al. Usefulness of antimicrobial susceptibility in the eradication of Helicobacter pylori. Clin. Microbiol. Infect. 2013, 19, 379–383. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cosme, A.; Lizasoan, J.; Montes, M.; Tamayo, E.; Alonso, H.; Mendarte, U.; Martos, M.; Fernández-Reyes, M.; Saraqueta, C.; Bujanda, L. Antimicrobial Susceptibility-Guided Therapy Versus Empirical Concomitant Therapy for Eradication of Helicobacter pylori in a Region with High Rate of Clarithromycin Resistance. Helicobacter 2016, 21, 29–34. [Google Scholar] [CrossRef] [PubMed]
- Cosme, A.; Montes, M.; Ibarra, B.; Tamayo, E.; Alonso, H.; Mendarte, U.; Lizasoan, J.; Herreros-Villanueva, M.; Bujanda, L. Antimicrobial susceptibility testing before first-line treatment for Helicobacter pylori infection in patients with dual or triple antibiotic resistance. World J. Gastroenterol. 2017, 23, 3367–3373. [Google Scholar] [CrossRef]
- Wenzhen, Y.; Yumin, L.; Quanlin, G.; Kehu, Y.; Lei, J.; Donghai, W.; Lijuan, Y. Is antimicrobial susceptibility testing necessary before first-line treatment for Helicobacter pylori infection? Meta-analysis of randomized controlled trials. Intern. Med. 2010, 49, 1103–1109. [Google Scholar] [CrossRef] [Green Version]
- Cammarota, G.; Ianiro, G.; Bibbò, S.; Di Rienzo, T.A.; Masucci, L.; Sanguinetti, M.; Gasbarrini, A. Culture-guided treatment approach for Helicobacter pylori infection: Review of the literature. World J. Gastroenterol. 2014, 20, 5205–5211. [Google Scholar] [CrossRef]
- Hulten, K.G.; Lamberth, L.B.; Kalfus, I.N.; Graham, D.Y. National and Regional United States Antibiotic Resistance to Helicobacter pylori Resistance to Helicobacter pylori. Lessons from a Clinical Trial. Gastroenterology 2021, 161, 342–344. [Google Scholar] [CrossRef]
- Morilla, A.M.; Álvarez-Argüelles, M.E.; Duque, J.M.; Armesto, E.; Villar, H.; Melón, S. Primary antimicrobial resistance rates and prevalence of Helicobacter pylori infection in the north of Spain. A 13-year retrospective study. Gastroenterol. Hepatol. 2019, 42, 76–485. [Google Scholar] [CrossRef]
- Choi, J.H.; Yang, Y.J.; Bang, C.S.; Lee, J.J.; Baik, G.H. Current Status of the Third-Line Helicobacter pylori Eradication. Gastroenterol. Res. Pract. 2018, 2, 6523653. [Google Scholar]
- Perez-Trallero, E.; Montes, M.; Alcorta, M.; Zubillaga, P.; Telleria, E. Non-endoscopic method to obtain Helicobacter pylori for culture. Lancet 1995, 345, 622–623. [Google Scholar] [CrossRef]
- Bénéjat, L.; Ducournau, A.; Lehours, P.; Mégraud, F. Real-time PCR for Helicobacter pylori diagnosis. The best tools available. Helicobacter 2018, 23, e12512. [Google Scholar] [CrossRef] [PubMed]
- Pichon, M.; Pichard, B.; Barrioz, T.; Plouzeau, C.; Croquet, V.; Fotsing, G.; Chéron, A.; Vuillemin, É.; Wangermez, M.; Haineaux, P.A.; et al. Diagnostic Accuracy of a Noninvasive Test for Detection of Helicobacter pylori and Resistance to Clarithromycin in Stool by the Amplidiag, H. pylori+ClariR Real-Time PCR Assay. J. Clin. Microbiol. 2020, 58, e01787-19. [Google Scholar] [CrossRef]
- Lee, J.Y.; Kim, N.; Nam, R.H.; In Choi, S.; Lee, J.W.; Lee, D.H. Primary and secondary antibiotic resistance of Helicobacter pylori in Korea from 2003 to 2018. Helicobacter 2019, 24, e12660. [Google Scholar] [CrossRef] [PubMed]
- Kuo, Y.T.; Liou, J.M.; El-Omar, E.M.; Wu, J.Y.; Leow, A.H.R.; Goh, K.L.; Das, R.; Lu, H.; Lin, J.T.; Tu, Y.K.; et al. Primary antibiotic resistance in Helicobacter pylori in the Asia-Pacific region: A systematic review and meta-analysis. Lancet Gastroenterol. Hepatol. 2017, 2, 707–715. [Google Scholar] [CrossRef]
- Leitsch, D. A review on metronidazole: An old warhorse in antimicrobial chemotherapy. Parasitology 2019, 146, 1167–1178. [Google Scholar] [CrossRef]
- Saracino, I.M.; Fiorini, G.; Zullo, A.; Pavoni, M.; Saccomanno, L.; Vaira, D. Trends in Primary Antibiotic Resistance in H. pylori Strains Isolated in Italy between 2009 and 2019. Antibiotics 2020, 9, 26. [Google Scholar] [CrossRef] [Green Version]
- Gatta, L.; Scarpignato, C.; Fiorini, G.; Belsey, J.; Saracino, I.M.; Ricci, C.; Vaira, D. Impact of primary antibiotic resistance on the effectiveness of sequential therapy for Helicobacter pylori infection: Lessons from a 5-year study on a large number of strains. Aliment. Pharmacol. Ther. 2018, 47, 1261–1269. [Google Scholar] [CrossRef] [Green Version]
- McNicholl, A.G.; O’Morain, C.A.; Megraud, F.; Gisbert, J.P.; As Scientific Committee of the Hp-Eureg on Behalf of the National C. Protocol of the European Registry on the management of Helicobacter pylori infection (Hp-EuReg). Helicobacter 2019, 24, e12630. [Google Scholar] [CrossRef] [PubMed]
- Nyssen, O.P.; Bordin, D.; Tepes, B.; Pérez-Aisa, Á.; Vaira, D.; Caldas, M.; Bujanda, L.; Castro-Fernandez, M.; Lerang, F.; Leja, M.; et al. European Registry on Helicobacter pylori management (Hp-EuReg): Patterns and trends in first-line empirical eradication prescription and outcomes of 5 years and 21 533 patients. Gut 2021, 70, 40–54. [Google Scholar] [CrossRef] [PubMed]
- Harris, P.A.; Taylor, R.; Thielke, R.; Payne, J.; Gonzalez, N.; Conde, J.G. Research electronic data capture (REDCap)—A metadata-driven methodology and workflow process for providing translational research informatics support. J. Biomed. Inform. 2009, 42, 377–381. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
| Resistance | Years—Number of Patients (%) | Total | |||||||
|---|---|---|---|---|---|---|---|---|---|
| 2013 | 2014 | 2015 | 2016 | 2017 | 2018 | 2019 | 2020 | ||
| No resistance | 209 (49%) | 260 (50%) | 245 (49%) | 120 (44%) | 188 (55%) | 135 (48%) | 130 (48%) | 78 (36%) | 1365 (48%) |
| Clarithromycin | 85 (20%) | 119 (23%) | 136 (27%) | 91 (34%) | 83 (24%) | 76 (27%) | 76 (28%) | 35 (16%) | 701 (25%) |
| Metronidazole | 165 (39%) | 155 (30%) | 162 (32%) | 90 (33%) | 84 (25%) | 78 (28%) | 77 (29%) | 40 (18%) | 852 (30%) |
| Levofloxacin | 58 (14%) | 100 (19%) | 121 (24%) | 73 (27%) | 75 (22%) | 69 (25%) | 48 (18%) | 16 (7%) | 561 (20%) |
| Amoxicillin | 6 (1%) | 0 (0%) | 0 (0%) | 0 (0%) | 4 (1.2%) | 1 (0.4%) | 0 (0%) | 0 (0%) | 11 (0,4%) |
| Tetracycline | 2 (0.5%) | 1 (0.2%) | 0 (0%) | 1 (0.4%) | 0 (0%) | 0 (0%) | 1 (0.4%) | 0 (0%) | 5 (0,2%) |
| Dual (C+M) | 56 (13%) | 64 (12%) | 77 (15%) | 45 (17%) | 41 (12%) | 34 (12%) | 35 (13%) | 16 (7%) | 368 (13%) |
| Triple (C+M+L) | 22 (5%) | 31 (6%) | 45 (9%) | 26 (10%) | 19 (5.5%) | 19 (6%) | 11 (4%) | 2 (0.9%) | 172 (6%) |
| Resistance | 2013–2016 Period N (%) | 2017–2020 Period N (%) | p-Value |
|---|---|---|---|
| No resistance | 834 (49%) | 531 (47%) | 0.4 |
| Clarithromycin | 431 (25%) | 230 (20%) | 0.3 |
| Metronidazole | 572 (33%) | 279 (24.5%) | 0.02 |
| Levofloxacin | 352 (20.5%) | 208 (18%) | 0.4 |
| Amoxicillin | 6 (0.3%) | 5 (0.4%) | 0.5 |
| Tetracycline | 4 (0.2%) | 1 (0.08%) | 0.4 |
| Dual (C+M) | 242 (14%) | 126 (11%) | 0.3 |
| Triple (C+M+L) | 124 (7.2%) | 51 (4.5%) | 0.4 |
| Resistance | Southern Europe N (%) | Northern Europe N (%) | p-Value |
|---|---|---|---|
| No resistance | 996 (44%) | 218 (68.5%) | 0.03 |
| Clarithromycin | 631 (28%) | 22 (7%) | 0.001 |
| Metronidazole | 687 (30.5%) | 83 (26%) | 0.4 |
| Levofloxacin | 530 (23.5%) | 8 (2.5%) | 0.001 |
| Amoxicillin | 5 (0.2%) | 0 (0%) | 0.3 |
| Tetracycline | 3 (0.1%) | 1 (0.3%) | 0.4 |
| Dual (C+M) | 333 (15%) | 11 (3.5%) | 0.02 |
| Triple (C+M+L) | 168 (7.5%) | 1 (0.3%) | 0.02 |
| Resistance | Naïve N (%) | Non-Naïve N (%) | p-Value |
|---|---|---|---|
| No resistance | 1365 (48%) | 93 (16%) | 0.001 |
| Clarithromycin | 701 (25%) | 380 (66%) | 0.01 |
| Metronidazole | 852 (30%) | 309 (54%) | 0.02 |
| Levofloxacin | 561 (20%) | 164 (28%) | 0.03 |
| Amoxicillin | 11 (0.4%) | 4 (0.7%) | 0.3 |
| Tetracycline | 5 (0.2%) | 0 (0%) | 0.4 |
| Dual (C+M) | 368 (13%) | 248 (43%) | 0.02 |
| Triple (C+M+L) | 172 (6%) | 109 (19%) | 0.01 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bujanda, L.; Nyssen, O.P.; Vaira, D.; Saracino, I.M.; Fiorini, G.; Lerang, F.; Georgopoulos, S.; Tepes, B.; Heluwaert, F.; Gasbarrini, A.; et al. Antibiotic Resistance Prevalence and Trends in Patients Infected with Helicobacter pylori in the Period 2013–2020: Results of the European Registry on H. pylori Management (Hp-EuReg). Antibiotics 2021, 10, 1058. https://doi.org/10.3390/antibiotics10091058
Bujanda L, Nyssen OP, Vaira D, Saracino IM, Fiorini G, Lerang F, Georgopoulos S, Tepes B, Heluwaert F, Gasbarrini A, et al. Antibiotic Resistance Prevalence and Trends in Patients Infected with Helicobacter pylori in the Period 2013–2020: Results of the European Registry on H. pylori Management (Hp-EuReg). Antibiotics. 2021; 10(9):1058. https://doi.org/10.3390/antibiotics10091058
Chicago/Turabian StyleBujanda, Luis, Olga P. Nyssen, Dino Vaira, Ilaria M. Saracino, Giulia Fiorini, Frode Lerang, Sotirios Georgopoulos, Bojan Tepes, Frederic Heluwaert, Antonio Gasbarrini, and et al. 2021. "Antibiotic Resistance Prevalence and Trends in Patients Infected with Helicobacter pylori in the Period 2013–2020: Results of the European Registry on H. pylori Management (Hp-EuReg)" Antibiotics 10, no. 9: 1058. https://doi.org/10.3390/antibiotics10091058