
Prevalence of Musculoskeletal Disorders in Germany—A Comparison between Dentists and Dental Assistants

 , , , ,
, , , , 
Abstract
:1. Introduction
2. Methods
2.1. Participants
2.2. Questionnaire
2.3. Recruitment
2.4. Statistical Evaluation
3. Results
3.1. Individual Characteristics and Sociodemographic DATA
3.2. Differences in Occupational Parameters and Physical Activity
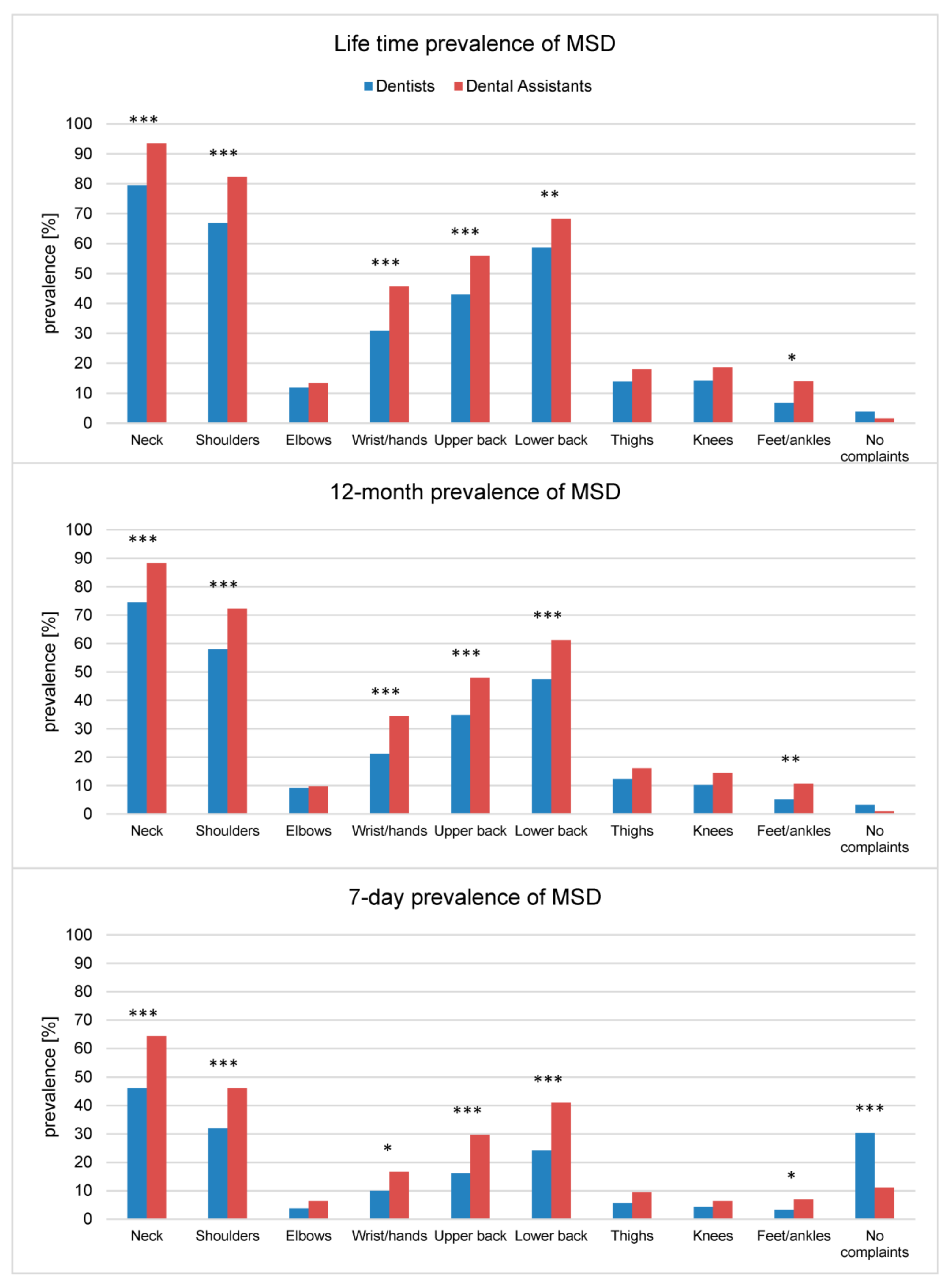
3.3. Prevalence of MSD—Comparison between Dentists and Dental Assistants
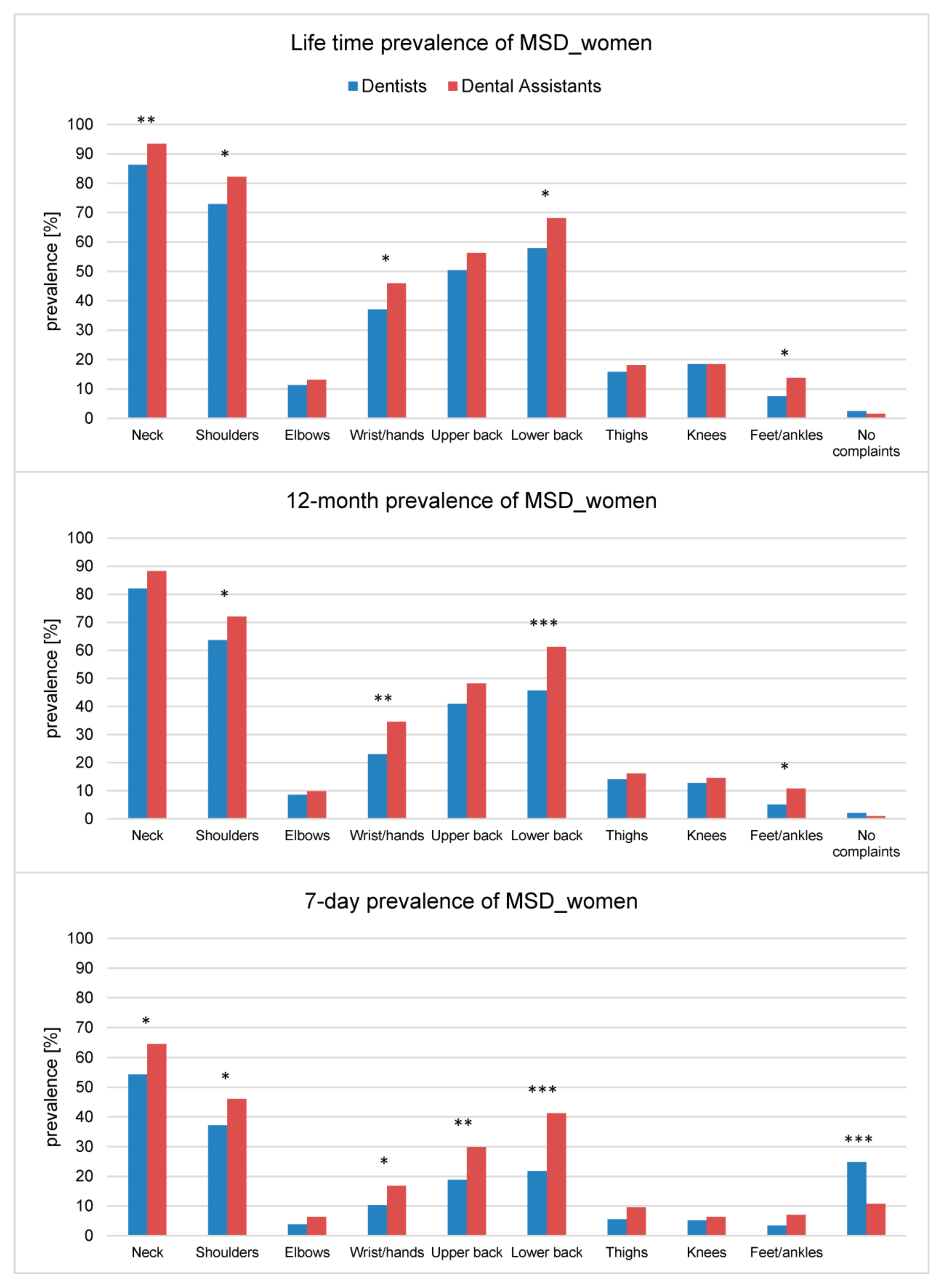
3.4. Prevalence of MSD—Comparison between Female Dentists and Dental Assistants
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| MSD | musculoskeletal disorders |
| SOpEZ | study for the optimization of ergonomics in the dental practice |
| IQR | interquartile range |
References
- Lietz, J.; Kozak, A.; Nienhaus, A. Prevalence and occupational risk factors of musculoskeletal diseases and pain among dental professionals in Western countries: A systematic literature review and meta-analysis. PLoS ONE 2018, 13, e0208628. [Google Scholar] [CrossRef] [Green Version]
- Ohlendorf, D.; Haas, Y.; Naser, A.; Haenel, J.; Maltry, L.; Holzgreve, F.; Erbe, C.; Betz, W.; Wanke, E.M.; Brüggmann, D.; et al. Prevalence of Muscular Skeletal Disorders among Qualified Dental Assistants. Int. J. Environ. Res. Public Health 2020, 17, 3490. [Google Scholar] [CrossRef]
- Ohlendorf, D.; Naser, A.; Haas, Y.; Haenel, J.; Fraeulin, L.; Holzgreve, F.; Erbe, C.; Betz, W.; Wanke, E.M.; Brueggmann, D.; et al. Prevalence of Musculoskeletal Disorders among Dentists and Dental Students in Germany. Int. J. Environ. Res. Public Health 2020, 17, 8740. [Google Scholar] [CrossRef]
- Morse, T.; Bruneau, H.; Dussetschleger, J. Musculoskeletal disorders of the neck and shoulder in the dental professions. Work 2010, 35, 419–429. [Google Scholar] [CrossRef]
- Partido, B.B.; Henderson, R.; Washington, H. Relationships between the postures of dentists and chairside dental assistants. J. Dent. Educ. 2020, 84, 1025–1031. [Google Scholar] [CrossRef]
- Proteau, R.-A. Prevention of Work-Related Musculoskeletal Disorders (MSDs) in Dental Clinics; ASSTSAS: Montreal, QC, Canada, 2009; Available online: http://asstsas.qc.ca/sites/default/files/publications/documents/Guides_Broch_Depl/GP50A_MSDs_dental_clinics2009.pdf (accessed on 27 July 2021).
- Moodley, R.; Naidoo, S.; Van Wyk, J. The prevalence of occupational health-related problems in dentistry: A review of the literature. J. Occup. Health 2018, 60, 111–125. [Google Scholar] [CrossRef]
- Berkley, K.J. Sex differences in pain. Behav. Brain Sci. 1997, 20, 371–380. [Google Scholar] [CrossRef]
- Bento, T.P.F.; Genebra, C.V.D.S.; Maciel, N.M.; Cornelio, G.P.; Simeão, S.F.A.P.; de Vitta, A. Low back pain and some associated factors: Is there any difference between genders? Braz. J. Phys. Ther. 2020, 24, 79–87. [Google Scholar] [CrossRef]
- Kim, R.; Wiest, C.; Clark, K.; Cook, C.; Horn, M. Identifying risk factors for first-episode neck pain: A systematic review. Musculoskelet. Sci. Pract. 2018, 33, 77–83. [Google Scholar] [CrossRef]
- Bundesagentur für Arbeit. Beschäftigte nach Berufen (KldB 2010) (Quartalszahlen); Bundesagentur für Arbeit: Nürnberg, Germany, 2020; Available online: https://statistik.arbeitsagentur.de/SiteGlobals/Forms/Suche/Einzelheftsuche_Formular.html;jsessionid=ECD17DA4B4697D55D23B9200B0B73800?nn=1523064&topic_f=beschaeftigung-sozbe-bo-heft (accessed on 27 July 2021).
- Hayes, M.J.; Cockrell, D.; Smith, D. A systematic review of musculoskeletal disorders among dental professionals. Int. J. Dent. Hyg. 2009, 7, 159–165. [Google Scholar] [CrossRef]
- Valachi, B.; Valachi, K. Mechanisms leading to musculoskeletal disorders in dentistry. J. Am. Dent. Assoc. 2003, 134, 1344–1350. [Google Scholar] [CrossRef]
- Yamalik, N. Musculoskeletal disorders (MSDs) and dental practice Part 2. Risk factors for dentistry, magnitude of the problem, prevention, and dental ergonomics. Int. Dent. J. 2007, 57, 45–54. [Google Scholar] [CrossRef]
- Zitzmann, N.U.; Chen, M.D.; Zenhäusern, R. Frequency and manifestations of back pain in the dental profession. Schweiz. Monatsschrift Zahnmed. 2008, 118, 610–618. [Google Scholar]
- Åkesson, I.; Johnsson, B.; Rylander, L.; Moritz, U.; Skerfving, S. Musculoskeletal disorders among female dental personnel--clinical examination and a 5-year follow-up study of symptoms. Int. Arch. Occup. Environ. Health 1999, 72, 395–403. [Google Scholar] [CrossRef]
- Al Wassan, K.; Almas, K.; Al Shethri, S.; Al Qahtani, M. Back & neck problems among dentists and dental auxiliaries. J. Contemp. Dent. Pract. 2001, 2, 17–30. [Google Scholar]
- Dajpratham, P.; Ploypetch, T.; Kiattavorncharoen, S.; Boonsiriseth, K. Prevalence and associated factors of musculoskeletal pain among the dental personnel in a dental school. J. Med. Assoc. Thai. 2010, 93, 714–721. [Google Scholar] [PubMed]
- Ohlendorf, D.; Maltry, L.; Hänel, J.; Betz, W.; Erbe, C.; Maurer-Grubinger, C.; Holzgreve, F.; Wanke, E.M.; Brüggmann, D.; Nienhaus, A.; et al. SOPEZ: Study for the optimization of ergonomics in the dental practice-musculoskeletal disorders in dentists and dental assistants: A study protocol. J. Occup. Med. Toxicol. 2020, 15, 1–9. [Google Scholar] [CrossRef]
- Leiner, D.J. SoSci Survey (Version 3.1.06). Computer Software; SoSci Survey GmbH: München, Germany, 2019. [Google Scholar]
- Kuorinka, I.; Jonsson, B.; Kilbom, A.; Vinterberg, H.; Biering-Sørensen, F.; Andersson, G.; Jørgensen, K. Standardised Nordic questionnaires for the analysis of musculoskeletal symptoms. Appl. Ergon. 1987, 18, 233–237. [Google Scholar] [CrossRef]
- López-Aragón, L.; López-Liria, R.; Callejón-Ferre, Á.-J.; Gómez-Galán, M. Applications of the standardized Nordic questionnaire: A review. Sustainability 2017, 9, 1514. [Google Scholar] [CrossRef] [Green Version]
- Morgan, G.A.; Barrett, K.C.; Leech, N.L.; Gloeckner, G.W. IBM SPSS for Introductory Statistics: Use and Interpretation; Routledge: New York, NY, USA, 2019. [Google Scholar]
- Meyer, P.V.; Micheelis, W. Arbeitsbelastungen bei Zahnärzten in niedergelassener Praxis: Eine Arbeitsmedizinische Bestandsaufnahme zu Wirbelsäulenbelastungen, Berufsdermatosen und Stressfaktoren; Deutscher Zahnärzte Verl. DÄV-Hanser: Breme, Germany, 2001. [Google Scholar]
- Radanović, B.; Vučinić, P.; Janković, T.; Mahmutović, E.; Penjašković, D. Musculoskeletal symptoms of the neck and shoulder among dental practitioners. J. Back Musculoskelet. Rehabil. 2017, 30, 675–679. [Google Scholar] [CrossRef]
- Šćepanović, D.; Klavs, T.; Verdenik, I.; Oblak, Č. The Prevalence of Musculoskeletal Pain of Dental Workers Employed in Slovenia. Workplace Health Saf. 2019, 67, 461–469. [Google Scholar] [CrossRef] [PubMed]
- RKI. Gesundheitsberichterstattung des Bundes—Gemeinsam Getragen von RKI und Destatis; RKI: Berlin, Germany, 2015. [Google Scholar]
- Dehghan, N.; Aghilinejad, M.; Nassiri-Kashani, M.H.; Amiri, Z.; Talebi, A. The effect of a multifaceted ergonomic intervention program on reducing musculoskeletal disorders in dentists. Med. J. Islam. Repub. Iran 2016, 30, 472. [Google Scholar]
- Droeze, E.H.; Jonsson, H. Evaluation of ergonomic interventions to reduce musculoskeletal disorders of dentists in the Netherlands. Work 2005, 25, 211–220. [Google Scholar] [PubMed]
- Faust, A.M.; Ahmed, S.N.; Johnston, L.B.; Harmon, J.B. Teaching methodologies for improving dental students’ implementation of ergonomic operator and patient positioning. J. Dent. Educ. 2021, 85, 370–378. [Google Scholar] [CrossRef] [PubMed]
- Van Eerd, D.; Munhall, C.; Irvin, E.; Rempel, D.; Brewer, S.; Van Der Beek, A.; Dennerlein, J.; Tullar, J.; Skivington, K.; Pinion, C. Effectiveness of workplace interventions in the prevention of upper extremity musculoskeletal disorders and symptoms: An update of the evidence. Occup. Environ. Med. 2016, 73, 62–70. [Google Scholar] [CrossRef]
- da Costa, B.R.; Vieira, E.R. Risk factors for work-related musculoskeletal disorders: A systematic review of recent longitudinal studies. Am. J. Ind. Med. 2010, 53, 285–323. [Google Scholar] [CrossRef]
- Tuček, M.; Vaněček, V. Musculoskeletal disorders and working risk factors. Central Eur. J. Public Health 2020, 28, S06–S11. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Dentists | Dental Assistants | |||||||
|---|---|---|---|---|---|---|---|---|
| Total | Missing | Females | Males | Total | Missing | Females | Males | |
| [Median ( (IQR)) or %] | ||||||||
| Participants (n) | 389 | 240 | 149 | 322 | 320 | 2 | ||
| Sex (% female) | 61.7 *** | 0 | - | - | 99.4 | 0 | - | - |
| Age (years, (IQR)) | 39(22) *** | 1 | 35 (17) *** | 50 (24) | 32(15) | 0 | 32 (15) | 25 |
| Height (cm, (IQR)) | 172 (12.3) *** | 3 | 168 (8) *** | 182 (9) | 166 (9) | 2 | 166(9) | 166.5 |
| Weight (kg, (IQR)) | 70 (23) | 3 | 62 (14) *** | 83.5 (15) | 68 (18) | 2 | 68 (18) | 50 |
| BMI (kg/m2, (IQR)) | 23.03 (5.16) *** | 3 | 21.5 (4.16) *** | 24.81 (4.12) | 24.19 (5.88) | 2 | 24.22 (5.89) | 18.1 |
| Smoking (% non-smoker) | 90.5 *** | 1 | 91.7 *** | 88.5 | 71.6 | 2 | 72.0 | 0 |
| Handedness (% right) | 93.6 | 1 | 93.8 | 93.2 | 93.5 | 0 | 93.4 | 100 |
| Dentists Missing (n) | Dental Assistants Missing (n) | ||||
|---|---|---|---|---|---|
| [Median ( (IQR)) or %] | |||||
| Occupational parameters | |||||
| Working years since approbation or end of apprenticeship | 11 (20) | 1 | 12 (17) | 2 | |
| Working hours per week | 40 (10) | 24 | *** | 38 (10) | 22 |
| of which treatment time | 30 (9) | 25 | *** | 30 (15) | 24 |
| of which administration time | 6 (6) | 25 | *** | 4 (7) | 27 |
| Hours per week spent at desk | 8 (10) | 2 | *** | 3 (7) | 15 |
| Relative sitting time | 94.9% | 2 | *** | 82.0% | 1 |
| Regular breaks (e.g., every hour) between treatments | 41.9% | 3 | *** | 28.9% | 3 |
| Physical activity | |||||
| Corrective exercises between treatments | 11.3% | 3 | * | 5.9% | 3 |
| “back education program” participation | 30.9% | 0 | 30.7% | 0 | |
| Ergonomics training course participation | 26.2% | 0 | * | 18.6% | 0 |
| Ergonomics as part of study or apprenticeship | 9.8% | 289 | 8.1% | 262 | |
| Sports in leisure time | 83.0% | 0 | *** | 62.1% | 0 |
| Hours per week performing sports | 4 (2) | 69 | 3.5 (3) | 125 | |
| Strength training | 47.8% | 0 | *** | 31.4% | 0 |
| Hours per week performing strength training | 2 (2) | 205 | 2 (2) | 224 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Holzgreve, F.; Haas, Y.; Naser, A.; Haenel, J.; Fraeulin, L.; Erbe, C.; Betz, W.; Wanke, E.M.; Brueggmann, D.; Nienhaus, A.; et al. Prevalence of Musculoskeletal Disorders in Germany—A Comparison between Dentists and Dental Assistants. Appl. Sci. 2021, 11, 6956. https://doi.org/10.3390/app11156956
Holzgreve F, Haas Y, Naser A, Haenel J, Fraeulin L, Erbe C, Betz W, Wanke EM, Brueggmann D, Nienhaus A, et al. Prevalence of Musculoskeletal Disorders in Germany—A Comparison between Dentists and Dental Assistants. Applied Sciences. 2021; 11(15):6956. https://doi.org/10.3390/app11156956
Chicago/Turabian StyleHolzgreve, Fabian, Yvonne Haas, Antonia Naser, Jasmin Haenel, Laura Fraeulin, Christina Erbe, Werner Betz, Eileen M. Wanke, Doerthe Brueggmann, Albert Nienhaus, and et al. 2021. "Prevalence of Musculoskeletal Disorders in Germany—A Comparison between Dentists and Dental Assistants" Applied Sciences 11, no. 15: 6956. https://doi.org/10.3390/app11156956