Arginine and Endothelial Function
by
 and
and
Jessica Gambardella
1,2,3,4, 
Wafiq Khondkar
1,
Marco Bruno Morelli
1,2,
Xujun Wang
1,
Gaetano Santulli
1,2,3,4,* and
and
Valentina Trimarco
5 1
Department of Medicine (Division of Cardiology), Wilf Family Cardiovascular Research Institute, Albert Einstein College of Medicine—Montefiore University Hospital, New York City, NY 10461, USA
2
Department of Molecular Pharmacology, Fleischer Institute for Diabetes and Metabolism, Albert Einstein College of Medicine, New York City, NY 10461, USA
3
Department of Advanced Biomedical Sciences, “Federico II” University, 80131 Naples, Italy
4
International Translational Research and Medical Education (ITME), 80100 Naples, Italy
5
Department of Neuroscience, “Federico II” University, 80131 Naples, Italy
*
Author to whom correspondence should be addressed.
Biomedicines 2020, 8(8), 277; https://doi.org/10.3390/biomedicines8080277
Submission received: 30 June 2020
/
Revised: 4 August 2020
/
Accepted: 5 August 2020
/
Published: 6 August 2020
(This article belongs to the Special Issue Endothelial Dysfunction: From Pathophysiology to Novel Therapeutic Approaches)
{kind=link}
{kind=link}
Abstract
:Arginine (L-arginine), is an amino acid involved in a number of biological processes, including the biosynthesis of proteins, host immune response, urea cycle, and nitric oxide production. In this systematic review, we focus on the functional role of arginine in the regulation of endothelial function and vascular tone. Both clinical and preclinical studies are examined, analyzing the effects of arginine supplementation in hypertension, ischemic heart disease, aging, peripheral artery disease, and diabetes mellitus.
1. Pleiotropic Effects of Arginine
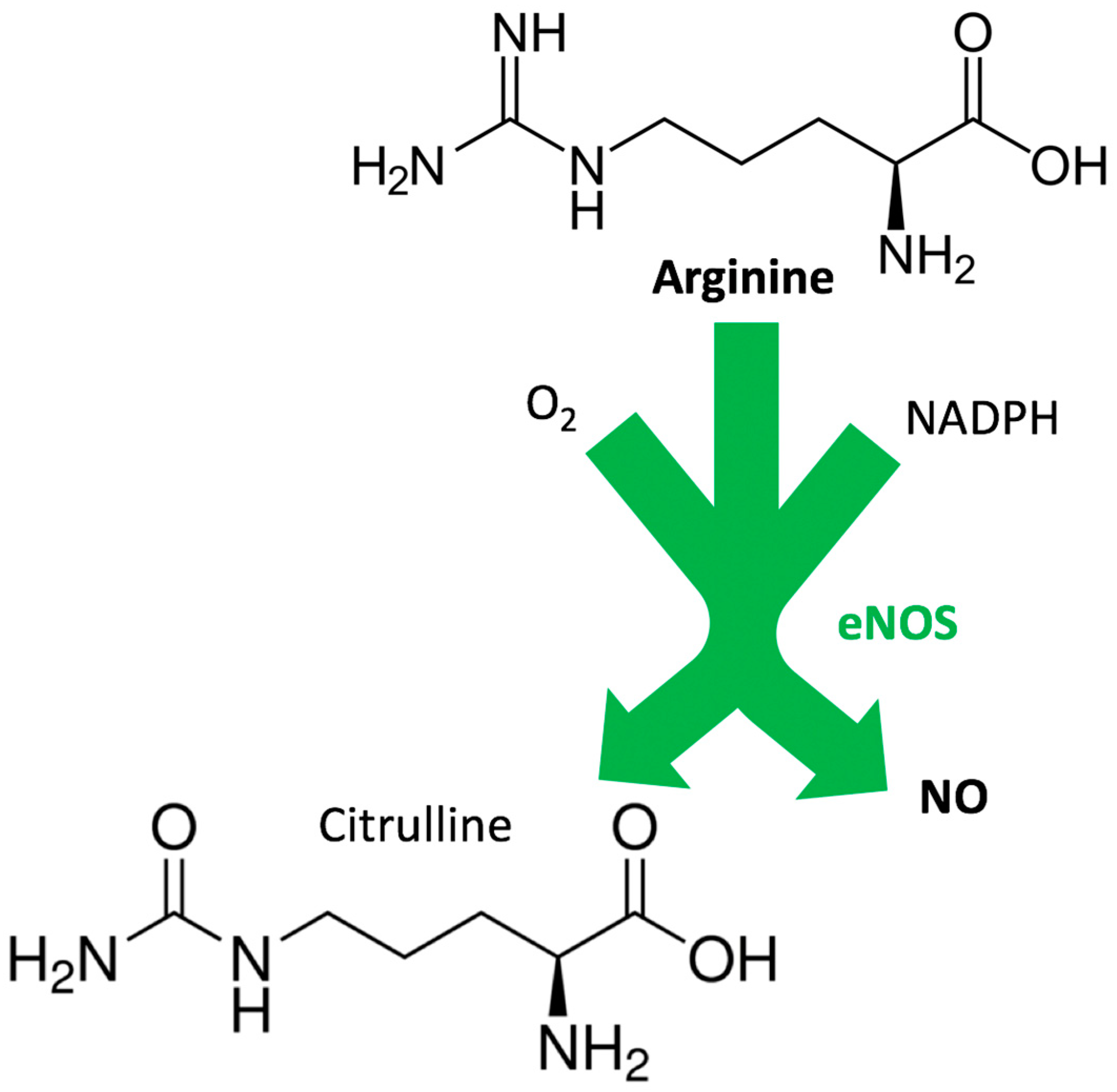
L-arginine, hereinafter referred to as arginine, is a semi-essential or conditionally essential amino acid, since it can be synthetized by healthy individuals but not by preterm infants [1]. From a chemical point of view, arginine is a 2-amino-5-guanidinopentanoic acid (Figure 1). Its name derives from the Greek word ἄργυρος (silver), indicating the color of arginine nitrate crystals.
Arginine is involved in a number of biological processes, it is the substrate for a series of reactions leading to the synthesis of other amino acids, and it is a substrate for two enzymes, namely nitric oxide (NO) synthase (NOS) and arginase, which are fundamental for the generation of NO and urea, respectively. Arginine is known to act as a substrate for NO production by endothelial cells, thus regulating vascular tone and, overall, cardiovascular homeostasis [2]. NO is synthesized from arginine by the enzyme NOS in a reaction that involves the transfer of electrons from nicotinamide adenine dinucleotide phosphate (NADPH)—via the flavin adenine dinucleotide (FAD) and flavin mononucleotide (FMN) in the C-terminal reductase domain [3,4]—to the heme in the N-terminal oxygenase domain, where the substrate arginine is oxidized to citrulline and NO [5,6], as shown in Figure 1. Arginine is also implicated in T-cell proliferation and host immune responses, as well as in creatine and collagen synthesis [7,8,9,10,11].
There are three isoforms of NOS, two of which—endothelial (eNOS) [12,13] and neuronal (nNOS) [14,15,16]—are constitutively expressed, while the third one, inducible NOS (iNOS) [17,18,19], is expressed in response to cytokines and is related to the inflammatory response [6,20]. NO generation occurs in two steps: first, NOS hydroxylates arginine to Nω-hydroxy-arginine (which remains largely bound to the enzyme); in a second step, NOS oxidizes Nω-hydroxy-arginine to citrulline and NO [21,22,23,24,25,26,27,28,29].
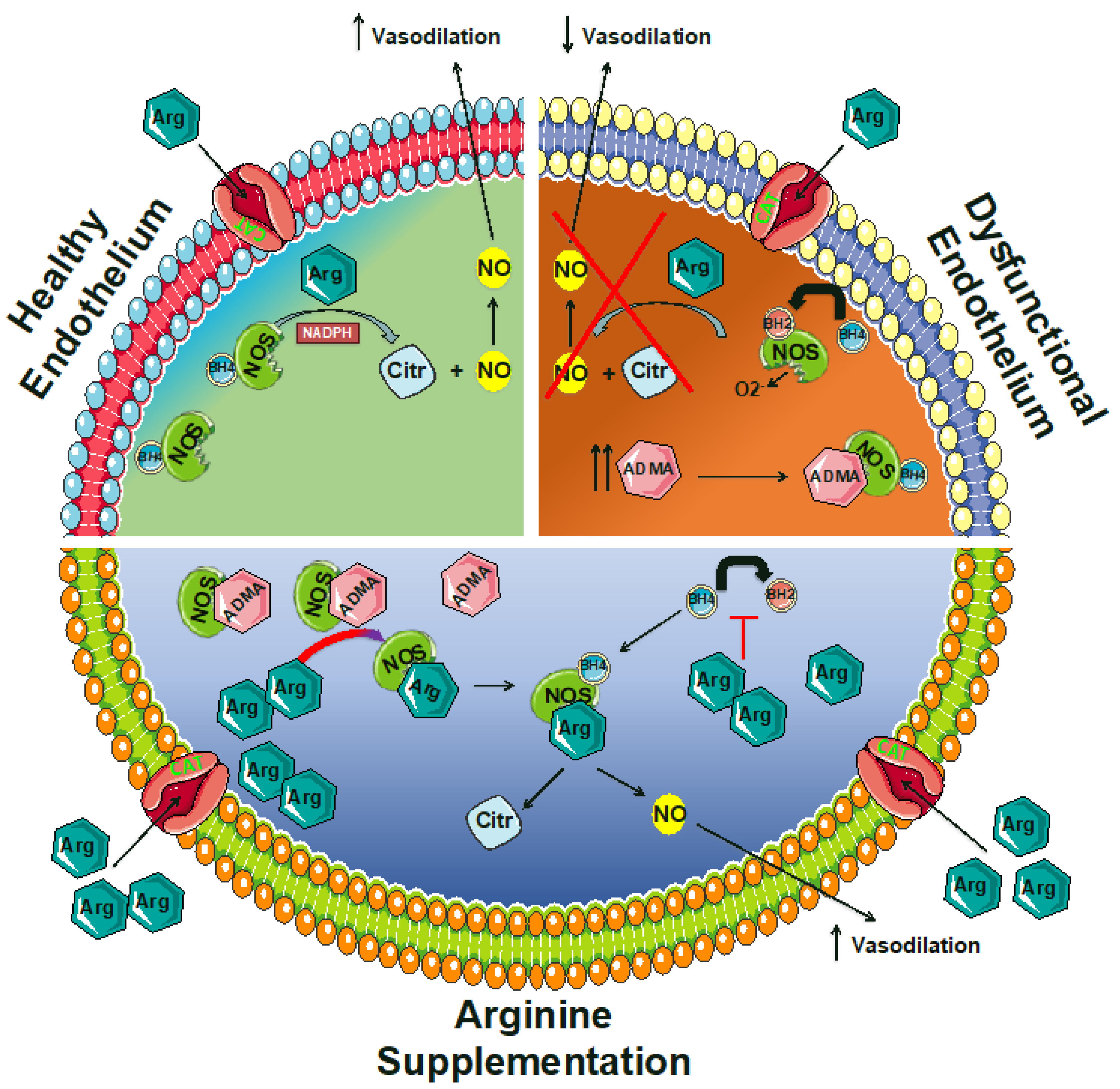
In normal conditions, NOS catalyzes the transformation of arginine, O2, and NADPH-derived electrons to NO and citrulline (Figure 1). However, in the presence of pathologic conditions like atherosclerosis and diabetes, the NOS function is altered, and the enzyme catalyzes the reduction of O2 to superoxide (O2−), a phenomenon that is generally referred to as “NOS uncoupling” [30,31,32,33,34,35,36,37,38,39,40,41], and has been linked to a limited bioavailability of tetrahydrobiopterin (BH4, also known as sapropterin) [42,43,44,45,46,47]. Indeed, the donation of an electron by BH4 to produce a transient BH4•+ radical is required for the oxidation of arginine to citrulline and the associated formation of a ferrous iron–NO complex at the NOS heme catalytic center [48,49,50,51]. BH4 is synthesized from guanosine triphosphate (GTP) by GTP cyclohydrolase I (GTPCH) and recycled from 7,8-dihydrobiopterin (BH2) by dihydrofolate reductase (Figure 2). Of note, NOS is inhibited by arginine analogs that are substituted at the guanidino nitrogen atom, like NG-monomethyl-arginine or NG-nitro-arginine [52,53,54,55,56,57,58].
As mentioned above, in the urea cycle arginine is converted by arginase, a manganese metalloenzyme, in ornithine and urea; this cycle is crucial not only for allowing urea excretion, but also for producing bicarbonate, which is critical for maintaining acid/base homeostasis [59,60,61,62,63]. Arginase exists in two distinct isoforms, arginase I and II, that share ~60% sequence homology; arginase I is a cytosolic enzyme mainly localized in the liver, whereas arginase II is a mitochondrial enzyme with a wide distribution and is expressed in the kidney, prostate, gastrointestinal tract, and the vasculature [64,65,66,67].
The enzyme arginase is a key modulator of NO production by competing for arginine: in other words, NO generation is dependent on the relative expression and activities of arginase and NOS. More specifically, increased arginase activity may lead to a decreased bioavailability of arginine for NOS, thereby diminishing NO production. This mechanism has emerged as an essential factor underlying impaired endothelial functions [68,69]. Specifically, an increased arginase activity has been associated with endothelial dysfunction in a number of experimental models of hypertension, atherosclerosis, diabetes, and aging [70,71,72,73,74,75,76,77,78,79,80,81,82,83,84,85,86,87,88,89,90,91,92].
2. Arginine and NO Production in Physiological Conditions: The Arginine Paradox
Indeed, endothelial dysfunction is a leading cause of several pathological conditions affecting the cardiovascular system, including hypertension, atherosclerosis, diabetes, and atherothrombosis [46,93,94,95,96,97,98,99,100,101,102,103,104,105,106,107,108,109,110,111,112,113,114,115,116,117,118,119]. Moreover, in April 2020, we were the first group to show that the systemic manifestations observed in coronavirus disease (COVID-19), caused by the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), could be explained by endothelial dysfunction [120]. Indeed, alterations in endothelial function have been linked to hypertension, diabetes, thromboembolism, and kidney failure, all featured, to different extents, in COVID-19 patients [121,122,123]. Other investigators have later confirmed our view [124,125,126,127,128,129,130,131,132,133]. On these grounds, based on the positive effects of arginine on endothelial function, we can also speculate that arginine supplementation could be helpful, while not being harmful, for contrasting endothelial dysfunction in COVID-19 patients.
An increasing interest in the potential therapeutic effects of arginine supplementation, especially in cardiovascular disorders, has recently emerged. An impaired NO synthesis is considered a main feature of a dysfunctional endothelium [107,134,135,136]; however, several studies suggest that arginine supplementation in healthy subjects does not lead to a significant increase in NO production [11,137,138,139,140]. For instance, the daily administration of arginine for 1 week did not affect the serum concentration of two established indicators of NO production, namely NO2− and NO3−, in twelve healthy subjects [138]. In another study, 20 healthy subjects received daily arginine supplementation in both sustained-release or immediate-release form; despite the significant increase in the plasma arginine concentration, which proved the effectiveness of the administration protocol, the authors did not observe significant differences in urinary extraction of nitrate [141].
One reason for the absence of significant results in normal conditions could be that the NO synthesis machinery seems to be saturated by the endogenous arginine. Indeed, the Michaelis–Menten constant (Km) of NO synthase is in the micromolar range, specifically 2.9 μmol/L, as demonstrated by Bredt and colleagues [142]. Arginine plasma levels measured in healthy humans are 15–30-fold higher than this Km, thereby making the levels of the substrate a non-limiting factor in the enzymatic reaction leading to NO production. Despite such a biochemical ratio, which in fact makes the enzyme physiologically saturated, various studies are also showing beneficial effects of arginine supplementation in healthy subjects. For instance, arginine supplementation has been tested in athletes, as vasodilation favors muscle perfusion and nutrient/oxygen delivery during exercise, enhancing muscle strength and recovery [143]. Controversial results come from these studies, sometimes yielding no effects of arginine supplementation on muscle performance, and sometimes demonstrating a significant improvement in exercise capability [137,144,145,146,147,148].
The phenomenon known as “arginine paradox” is born from this scenario, and indicates that we were losing part of the story concerning the alternative ways by which arginine can act on endothelial NO production. The arginine paradox refers to the fact that despite intracellular physiological concentrations of arginine being several hundred micromoles per liter, thereby exceeding the Km of eNOS, the acute provision of exogenous arginine still increases NO production [149,150,151].
One of the mechanisms that may help explain the arginine paradox comes from the discovery of asymmetric dimethylarginine (ADMA), an endogenous inhibitor of NOS [152,153,154,155]. Given its own structure similar to arginine, ADMA is a direct competitor for NOS binding. Moreover, both ADMA and arginine are both transported into the cell via the cationic amino acid transporter (CAT, also known as “y+ system”), a high-affinity, Na+-independent transporter of the basic amino acids [156,157], and therefore also compete with each other on this level (Figure 2). Since ADMA competes with arginine for NOS and for cell transport, the bioavailability of NO depends on the balance between the two [158]. Plasma levels of ADMA increase during hypertension, hypercholesterolemia, diabetes, and atherosclerosis [95,159,160,161,162,163,164,165,166,167,168,169,170]. Hence, despite the range of endogenous arginine levels, they could still be sufficient to guarantee eNOS saturation, and so the arginine/ADMA ratio would be reduced, resulting in a net inhibition of NO production [171,172,173].
The arginine/ADMA ratio is widely considered to be an important indicator of NO bioavailability as well as of the risk of formation of atherosclerotic plaques [174]. The ratio has been shown to be a better predictor for all-cause mortality compared to ADMA alone [174,175]. Similarly, although plasma ADMA levels were a significant predictor of all-cause mortality in an elderly population, the effect disappeared in subjects with higher arginine levels [176], and the arginine/ADMA ratio (but not ADMA alone) was a significant risk factor for microangiopathy-related cerebral damage in an elderly population [177].
Arginine supplementation can equilibrate the arginine/ADMA ratio, recovering the production of NO. In other terms, the increased arginine availability, resulting from supplementation, competes with ADMA in binding eNOS (Figure 2). This interesting mechanism sheds light on the effectiveness of the increased arginine availability, implicating further therapeutic options for arginine supplementation. Furthermore, this phenomenon can explain some conflicting results about arginine supplementation studies, as ADMA levels should be considered in the study populations. Specifically, cardiovascular patients with increased ADMA plasma levels could be the best target of arginine supplementation.
Another potential explanation of the arginine paradox may be that arginine could be compartmentalized in the cytoplasm, and local concentrations in the vicinity of NOS may be lower than expected from arginine levels in whole-cell homogenates [178].
3. Impaired NO Production as a Mechanism of Endothelial Dysfunction and Arginine Intervention
The major determinants of cardiovascular risk, including dyslipidemia, glucose intolerance, smoking, hypercholesterolemia, and aging, have a direct impact on the endothelium [179,180,181]. Exposing the vasculature to these conditions induces endothelial dysfunction and alterations as an early phenomenon, able to evolve and contribute to the progression towards clinically relevant disorders like hypertension, atherosclerosis, and diabetes mellitus. Hence, the endothelium plays a key role in cardiovascular physiology and pathophysiology [182,183,184,185,186,187,188,189,190,191,192,193,194]. Fervent research has been conducted in recent years in order to understand the underlying mechanisms and identify therapeutic strategies to prevent or counteract endothelial dysfunction.
The ability of the endothelium to regulate vascular homeostasis is largely dependent on NO production, making endothelial vasodilator failure the main sign of endothelial dysfunction and a hot point to be targeted. The impaired endothelial NO availability in perturbed vasculature can be attributable to a diminished synthesis of NO or, indirectly, to an increased ROS production, which inactivates the NO source [195,196]. In addition to counteracting oxidative stress, the stimulation of NO synthesis represents an alternative and a potentially effective approach [197,198], for instance, by providing further substrates to NO synthase. Theoretically, arginine supplementation meets these needs, and thus, it has been tested in many cardiovascular disorders as a potential therapeutic strategy [199]. However, human studies on arginine supplementation have often been a source of debate. Indeed, in healthy subjects as well as in patients suffering from cardiovascular disorders, levels of plasma arginine range from ~45 to ~100 μmol/L [137,200,201,202], significantly higher than the eNOS Km of 2.9 μmol/L [203]. Endocrine mechanisms may also contribute to vasodilation induced by arginine. Indeed, arginine stimulates the release of both insulin [204,205,206] and glucagon [207] from pancreatic islets of Langerhans. Interestingly, an intravenous infusion of arginine has been shown to induce vasodilation and insulin release in healthy humans, but when insulin secretion was blocked by octreotide co-infusion, no vasodilation occurred, whereas vasodilation was restored by insulin co-administration [208]. Since high intravenous doses of arginine (30 g) have also been shown to induce growth hormones (GHs), and secretion [209], the vasodilation induced by arginine could also be mediated by GHs via a signaling pathway that includes insulin-like growth factor-1 [210,211].
Substantial data indicate that endothelial dysfunction is highly prevalent in elderly individuals [212,213]. Endothelial dysfunction has also been implicated in age-associated declines in cognitive function, physical function, as well as in the pathogenesis of stroke, erectile dysfunction, and renal dysfunction. Clinical trials testing the effects of arginine in aging-induced endothelial dysfunction have yielded controversial results. An acute intravenous infusion of arginine (1 g/min for 30 min) had no effect on endothelial-dependent vasodilation in healthy older individuals [214]. Similarly, the intravenous infusion of arginine induced a significant increase in the renal plasma flow, glomerular filtration rate, natriuresis, and kaliuresis, in young but not in aged hypertensives [215]. Another study conducted in healthy postmenopausal women taking 9 g of arginine per day for 1 month confirmed that plasma arginine increased without a concomitant significant change in flow-mediated dilation [216]. On the contrary, in a prospective, double-blind, randomized crossover trial in 12 healthy, old participants (age 73.8 ± 2.7 years), chronic arginine supplementation (16 g/day for 2 weeks) markedly increased their plasma levels of arginine (114.9 ± 11.6 vs. 57.4 ± 5.0 mM) and significantly improved endothelial-dependent vasodilation [217].
4. Arginine Supplementation in Hypertension
The majority of studies in animal models supports a beneficial effect of arginine supplementation in hypertension, especially in the presence of salt-sensitive hypertension. For instance, both oral [218,219,220] and intraperitoneal [221,222] arginine administration in Dahl salt-sensitive (DSS) rats was shown to prevent the increase in blood pressure induced by a high salt diet. However, arginine was not effective in DSS pretreated with high salt for three weeks [218], suggesting that arginine is able to prevent and counteract hypertension when it is in the early stages, but probably not when some changes and pathological remodeling have already occurred.
The outcome of arginine supplementation could also depend on the method of administration. For instance, renal medullary interstitial infusion of arginine prevents the increase in blood pressure in high salt-treated rats, while the intravenous dose necessary to obtain a similar increase in plasma arginine does not affect blood pressure [223]. A rat model of type 1 diabetes mellitus shows an important reduction in blood pressure after 4 weeks of oral arginine treatment [224]; oral arginine administration prevents fructose-induced hypertension [225]. Oral arginine administration does not correct hypertension in spontaneously hypertensive rats, although markedly reduces renal damage [226].
Although the beneficial effect of arginine supplementation in hypertension appears to be largely attributable to its impact on NO synthesis, arginine has also been shown to have antioxidant properties, thus affecting the activity of redox-sensitive proteins and lowering blood pressure [227,228,229,230,231,232,233,234]. Indeed, supplementation with 3 g/day arginine for two months increases the serum total antioxidant capacity in obese patients with prediabetes [235]; of note, in vitro experiments performed in endothelial cells have revealed that arginine reduces superoxide release and the cell-mediated breakdown of NO [236].
In the clinical scenario, the oral administration of arginine acutely improves endothelium-dependent, flow-mediated dilatation of the brachial artery in patients with essential hypertension [237]; however, the long-term effects of arginine were not investigated in this study [237]. In a Japanese population, the acute intravenous infusion of arginine (500 mg/kg for 30 min) is able to decrease arterial pressure of both salt-sensitive and salt-insensitive patients [238]. In a similar study, conducted on African-Americans, the same amount of arginine administration reduces blood pressure with a greater effect in the salt-sensitive population [239]. Interestingly, in hypertensive patients in which the control of blood pressure with angiotensin converting enzyme (ACE)-inhibitors and diuretics for three months was unsuccessful, the addition of oral arginine (6 g/day) was effective in reducing both systolic and diastolic blood pressure levels [240]. Unfortunately, many of the findings on the effects of arginine supplementation in hypertension derive from small clinical studies and, despite the promising efficacy, further investigations are needed, especially large, randomized, and controlled trials. The ability to modulate the renin-angiotensin-aldosterone system (RAAS) is another mechanism by which arginine can regulate blood pressure: specifically, arginine inhibits ACE activity, reducing angiotensin II production and its effects on vascular tone [241].
5. Arginine Supplementation in Ischemic Heart Disease and Peripheral Artery Disease
Alongside the preservation of endothelial-dependent vasodilation, the enhanced bioavailability of NO reduces the activation of pro-inflammatory genes and the expression of endothelial adhesion molecules [242]. These events strongly regulate the development and the fate of atherosclerosis [243,244,245]. For these reasons, it is not surprising that arginine has a powerful effect on atherogenesis and its evolution. In particular, preclinical investigations have shown that chronic arginine administration in LDL-receptor KO mice significantly reduces the extension of atherosclerotic plaques [246]. Similarly, arginine supplementation in humans reverses the increased monocyte–endothelial adhesion, mirrored by a normalization of platelet aggregation [247]. These effects make arginine a promising drug for disorders like coronary artery disease (CAD), heart failure, and peripheral artery disease (PAD).
In 1997, two important studies investigating the effects of arginine in CAD were published [248,249]. In a placebo-controlled study, Adams and collaborators showed that oral administration of arginine (21 g/day for 3 days) significantly improved the vasodilatory response of the brachial artery in premature CAD [248]. A double-blind placebo-controlled study conducted on 22 patients with stable angina pectoris revealed that the administration of arginine was able to improve their exercise capacity in just 3 days [249]. The following year, a clinical study confirmed the beneficial effects of long-term arginine supplementation (9 g for 6 months), showing significantly enhanced vascular responses to acetylcholine in patients with coronary atherosclerosis [250]. Preclinical studies were consistent with these findings. For instance, oral administration of arginine reduced the intimal hyperplasia in balloon-injured carotid arteries in spontaneously hypertensive rats [251]. This first encouraging evidence prompted further investigations about arginine’s effects on CAD. Again, arginine treatment for 4 weeks preserved endothelial function in CAD patients, markedly reducing LDL oxidation [252]. Another study highlighted the method of administration as a major determinant of the efficacy of high dose arginine supplementation: intra-arterial infusion, but not oral administration, was able to improve endothelial-dependent vasodilation in patients with stable angina pectoris [253].
The therapeutic potential of arginine has been also investigated in heart failure [254,255,256,257,258] and ischemia-reperfusion injury [259,260,261], often yielding controversial results. Endothelium-dependent vasodilation in response to acetylcholine and ischemic vasodilation during reactive hyperemia is attenuated in the forearm of patients with heart failure [262]. In a seminal paper, Hirooka and collaborators demonstrated that the intra-arterial infusion of arginine was effective in reversing the blunted endothelium-dependent vasodilation observed in heart failure [263]. Moreover, oral arginine supplementation (6 g twice a day for 6 weeks) enhanced endurance exercise tolerance in heart failure patients, an important determinant of daily-life activity in patients with chronic stable heart failure [264]. In line with these results, a clinical study carried out in 21 patients with class II/III heart failure (New York Heart Association, NYHA) established that improved endothelial function following exercise training is associated with increased arginine transport [265]. However, another investigation in 20 patients with NYHA class III/IV heart failure demonstrated that responses to acetylcholine and sodium nitroprusside determined using forearm plethysmography were not affected by arginine (20 g/day every day for 28 days), although the actual levels of arginine in the blood were not measured [266]. Exogenous arginine (3 g three times a day for 6 months) administered to patients after an acute myocardial infarction did not improve vascular stiffness measurements or ejection fractions; this clinical trial had to be interrupted due to excess mortality in the treated patients [267].
The improvement in peripheral circulation is critical in patients with PAD, as in severe cases the extensive damage of leg tissues can result in gangrene and amputation [268,269,270]. Intravenous arginine administration to PAD patients is able to increase the calf blood flow and walking distance [271]. Similarly, an acute intravenous arginine infusion (30 g in 60 min) improves NO production and blood flow of the femoral artery in PAD patients [272]. The oral consumption of arginine for 2 weeks is able to increase the pain-free walking distance, improving the quality of life of patients with hypercholesterolemia [273]. Nevertheless, if the short-term arginine administration seems to be effective in treating PAD, the results on long-term administration are less consistent. A randomized clinical trial testing the long-term (6 months) effects of arginine supplementation was conducted on 133 subjects. Despite an increase in plasma levels of arginine, the study revealed no significant effect of arginine treatment on NO-dependent vasodilation, as well as on the relative functional phenotype of PAD patients [274].
6. Arginine Supplementation in Diabetes Mellitus
Given the fundamental pathogenic role of endothelial dysfunction in diabetes and its complications [275,276], the therapeutic use of arginine supplementation has been tested. In addition to the direct impact of arginine on endothelial vasodilator capacity, a crosstalk with the insulin pathway has been suggested [150,277]. In particular, as mentioned above, arginine can induce the release of insulin from pancreatic beta cells [204,205,206]. On the other hand, insulin is able to reduce ADMA concentrations [278] and to stimulate the secretion of arginine [279,280]. The stimulation of insulin receptors induces NO release, producing an insulin-dependent vasodilation [281,282,283,284,285]. Of note, such a protective effect of insulin on arginine mobility and endothelial NO production is compromised in diabetes [286]. Henceforth, diabetic patients could be an optimal target population for arginine supplementation.
Preclinical studies corroborate this theory: in diabetic rats, the oral administration of arginine reverses endothelial dysfunction [287], restoring endothelium-dependent relaxation and decreasing oxidative stress [224]. Arginine administration in tap water (free base, 50 mg/kg/day) for 4 months has been shown to reduce both cardiac [288] and renal [289] fibrosis in db/db mice, by the interaction of arginine with reactive carbonyl residues of glycosylation adducts of collagen, thereby inhibiting glucose-mediated abnormal cross-linking of collagenous structures. These results were later confirmed in a clinical setting, showing that 2 g of arginine free base administered orally as two daily doses of 1 g each reduced the lipid peroxidation product malondialdehyde in diabetic patients [290].
Clinical studies confirmed the reduction in blood pressure, platelet aggregation, and hemodynamic function in diabetic patients treated with intravenous arginine [291]. While in healthy subjects arginine treatment does not seem to affect insulin receptor sensitivity or density [292], in conditions of insulin resistance, arginine improves insulin sensitivity; indeed, the intravenous injection of arginine in obese or type 2 diabetic patients stimulates insulin responsiveness, restoring insulin-dependent vasodilation [151,293]. Similarly, the oral administration of arginine improves hepatic and peripheral insulin sensitivity in a cGMP dependent fashion [294]. A prospective, crossover clinical trial conducted in mildly hypertensive type 2 diabetic patients revealed a significant decrease in blood pressure in response to arginine, occurring two hours after the oral administration; the effect of lowering blood pressure was associated with increased plasma levels of citrulline, whereas no significant changes in insulin levels were detected, suggesting that the observed phenotype was dependent on arginine-induced NO synthesis [295].
Overall, the mentioned studies substantiate the use of arginine in the diabetic population, at least as a prophylactic treatment able to prevent cardiovascular complications of diabetes. One potential limitation for the use of arginine is the risk of reaction with precursors of advanced glycosylated products [296], which are particularly abundant in diabetes. Since the addition of methylglyoxal (abundant in diabetic patients [297]) to arginine has been shown in vitro to produce potent superoxide radicals in a dose-dependent manner [298], arginine supplementation has been suggested to be combined with antioxidants. A double-blind study on 24 diabetic patients verified this assumption evaluating the combination of N-acetylcysteine and arginine oral treatments: the combined treatment was able to reduce systolic and diastolic blood pressure, total cholesterol, C-reactive proteins, vascular adhesion molecules, and improved the intima-media thickness during endothelial post-ischemic vasodilation [299]. This last evidence indicates that the combination of arginine with an antioxidant agent should be potentially effective and well-tolerated.
7. Conclusions and Perspective: Arginine as a Therapeutic Tool
Overall, data available in the literature support and encourage the use of arginine supplementation in cardiovascular disorders, especially in preventing the evolution of hypertension and atherosclerosis. One limitation of using arginine supplementation remains the selection of the optimal target population. In this sense, we believe that ADMA levels could be very useful in selecting the target population, and patients with increased ADMA/arginine ratios are probably the most suitable population, in which arginine supplementation can actually be effective. Another limitation about arginine use concerns its dose. Indeed, available studies suggest a number of different doses, sometimes effective, sometimes not. For instance, the acute oral administration of arginine (9 g/day) has been shown to be not successful in inducing an effective NO production [216]. Instead, chronic administration of oral arginine (e.g., vials containing arginine salts-free 1.66 g/20 mL), has been shown to favor the utilization of arginine for NO synthesis [300], and we have data showing that oral arginine (3 g/day of Bioarginina®, Farmaceutici Damor, 2 vials/day) improves endothelial function in hypertensive patients via the regulation of non-coding RNAs (Gambardella et al., personal communication). Large, prospective randomized clinical trials are needed to better define the target population for arginine supplementation, alongside with correct dosage definitions. To date, a dose of ~3 g/day of arginine (e.g., Bioarginina®, 2 vials/day) seems to be effective in favoring the utilization of arginine for NO synthesis, without toxic effects.
Author Contributions
Conceptualization, G.S.; data curation, writing—original draft preparation, J.G., W.K., M.B.M., X.W. and G.S.; writing—review and editing, J.G., X.W.; G.S. and V.T.; supervision, G.S.; funding acquisition, G.S. and J.G. All authors have read and agreed to the published version of the manuscript.
Funding
The Santulli’s lab is supported in part by the NIH (R01-DK123259, R01-HL146691, R01-DK033823, and R00-DK107895 to G.S.) and by the American Heart Association (AHA-20POST35211151 to J.G.).
Conflicts of Interest
The authors declare no conflict of interest. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript, or in the decision to publish the paper.
References
- Lopez, M.J.; Mohiuddin, S.S. Biochemistry, Essential Amino Acids. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2020. [Google Scholar]
- Luiking, Y.C.; Ten Have, G.A.; Wolfe, R.R.; Deutz, N.E. Arginine de novo and nitric oxide production in disease states. Am. J. Physiol. Endocrinol. Metab. 2012, 303, E1177–E1189. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Agapie, T.; Suseno, S.; Woodward, J.J.; Stoll, S.; Britt, R.D.; Marletta, M.A. NO formation by a catalytically self-sufficient bacterial nitric oxide synthase from Sorangium cellulosum. Proc. Natl. Acad. Sci. USA 2009, 106, 16221–16226. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jachymova, M.; Martasek, P.; Panda, S.; Roman, L.J.; Panda, M.; Shea, T.M.; Ishimura, Y.; Kim, J.J. Masters, B.S. Recruitment of governing elements for electron transfer in the nitric oxide synthase family. Proc. Natl. Acad. Sci. USA 2005, 102, 15833–15838. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Serpe, M.J.; Zhang, X. The Principles, Development and Application of Microelectrodes for the In Vivo Determination of Nitric Oxide. In Electrochemical Methods for Neuroscience; Michael, A.C., Borland, L.M., Eds.; CRC Press/Taylor & Francis: Boca Raton, FL, USA, 2007. [Google Scholar]
- Andrew, P.J.; Mayer, B. Enzymatic function of nitric oxide synthases. Cardiovasc. Res. 1999, 43, 521–531. [Google Scholar] [CrossRef]
- Sax, H.C. Arginine stimulates wound healing and immune function in elderly human beings. JPEN J. Parenter. Enteral. Nutr. 1994, 18, 559–560. [Google Scholar] [CrossRef]
- Barbul, A.; Lazarou, S.A.; Efron, D.T.; Wasserkrug, H.L.; Efron, G. Arginine enhances wound healing and lymphocyte immune responses in humans. Surgery 1990, 108, 331–336. [Google Scholar]
- Durante, W.; Liao, L.; Reyna, S.V.; Peyton, K.J.; Schafer, A.I. Physiological cyclic stretch directs L-arginine transport and metabolism to collagen synthesis in vascular smooth muscle. FASEB J. 2000, 14, 1775–1783. [Google Scholar] [CrossRef]
- Da Silva, R.P.; Nissim, I.; Brosnan, M.E.; Brosnan, J.T. Creatine synthesis: Hepatic metabolism of guanidinoacetate and creatine in the rat in vitro and in vivo. Am. J. Physiol. Endocrinol. Metab. 2009, 296, E256–E261. [Google Scholar] [CrossRef]
- Bai, Y.; Sun, L.; Yang, T.; Sun, K.; Chen, J.; Hui, R. Increase in fasting vascular endothelial function after short-term oral L-arginine is effective when baseline flow-mediated dilation is low: A meta-analysis of randomized controlled trials. Am. J. Clin. Nutr. 2009, 89, 77–84. [Google Scholar] [CrossRef] [Green Version]
- Raman, C.S.; Li, H.; Martasek, P.; Kral, V.; Masters, B.S.; Poulos, T.L. Crystal structure of constitutive endothelial nitric oxide synthase: A paradigm for pterin function involving a novel metal center. Cell 1998, 95, 939–950. [Google Scholar] [CrossRef] [Green Version]
- Garthwaite, J.; Charles, S.L.; Chess-Williams, R. Endothelium-derived relaxing factor release on activation of NMDA receptors suggests role as intercellular messenger in the brain. Nature 1988, 336, 385–388. [Google Scholar] [CrossRef] [PubMed]
- Bec, N.; Gorren, A.C.; Voelker, C.; Mayer, B.; Lange, R. Reaction of neuronal nitric-oxide synthase with oxygen at low temperature. Evidence for reductive activation of the oxy-ferrous complex by tetrahydrobiopterin. J. Biol. Chem. 1998, 273, 13502–13508. [Google Scholar] [CrossRef] [Green Version]
- Iwai, N.; Hanai, K.; Tooyama, I.; Kitamura, Y.; Kinoshita, M. Regulation of neuronal nitric oxide synthase in rat adrenal medulla. Hypertension 1995, 25, 431–436. [Google Scholar] [CrossRef] [PubMed]
- O’Dell, T.J.; Huang, P.L.; Dawson, T.M.; Dinerman, J.L.; Snyder, S.H.; Kandel, E.R.; Fishman, M.C. Endothelial NOS and the blockade of LTP by NOS inhibitors in mice lacking neuronal NOS. Science 1994, 265, 542–546. [Google Scholar] [CrossRef] [PubMed]
- Geller, D.A.; Lowenstein, C.J.; Shapiro, R.A.; Nussler, A.K.; Di Silvio, M.; Wang, S.C.; Nakayama, D.K.; Simmons, R.L.; Snyder, S.H.; Billiar, T.R. Molecular cloning and expression of inducible nitric oxide synthase from human hepatocytes. Proc. Natl. Acad. Sci. USA 1993, 90, 3491–3495. [Google Scholar] [CrossRef] [Green Version]
- Geller, D.A.; Nussler, A.K.; Di Silvio, M.; Lowenstein, C.J.; Shapiro, R.A.; Wang, S.C.; Simmons, R.L.; Billiar, T.R. Cytokines, endotoxin, and glucocorticoids regulate the expression of inducible nitric oxide synthase in hepatocytes. Proc. Natl. Acad. Sci. USA 1993, 90, 522–526. [Google Scholar] [CrossRef] [Green Version]
- Hokari, A.; Zeniya, M.; Esumi, H. Cloning and functional expression of human inducible nitric oxide synthase (NOS) cDNA from a glioblastoma cell line A-172. J. Biochem. 1994, 116, 575–581. [Google Scholar] [CrossRef]
- Forstermann, U.; Sessa, W.C. Nitric oxide synthases: Regulation and function. Eur. Heart J. 2012, 33, 829–837, 837a–837d. [Google Scholar] [CrossRef] [Green Version]
- Rafikov, R.; Fonseca, F.V.; Kumar, S.; Pardo, D.; Darragh, C.; Elms, S.; Fulton, D.; Black, S.M. eNOS activation and NO function: Structural motifs responsible for the posttranslational control of endothelial nitric oxide synthase activity. J. Endocrinol. 2011, 210, 271–284. [Google Scholar] [CrossRef] [Green Version]
- Alderton, W.K.; Cooper, C.E.; Knowles, R.G. Nitric oxide synthases: Structure, function and inhibition. Biochem. J. 2001, 357 Pt 3, 593–615. [Google Scholar] [CrossRef]
- Stuehr, D.J. Enzymes of the L-arginine to nitric oxide pathway. J. Nutr. 2004, 134 (Suppl. 10), 2748S–2751S. [Google Scholar] [CrossRef] [PubMed]
- Meulemans, A. Electrochemical detection of nitroso-arginine as an intermediate between N-hydroxy-arginine and citrulline. An in vitro versus in vivo study using microcarbon electrodes in neuronal nitric oxide synthase and mice brain. Neurosci. Lett. 2000, 294, 125–129. [Google Scholar] [CrossRef]
- Tsuboi, T.; Maeda, M.; Hayashi, T. Administration of L-arginine plus L-citrulline or L-citrulline alone successfully retarded endothelial senescence. PLoS ONE 2018, 13, e0192252. [Google Scholar] [CrossRef] [PubMed]
- De Betue, C.T.I.; Garcia Casal, X.C.; van Waardenburg, D.A.; Schexnayder, S.M.; Joosten, K.F.M.; Deutz, N.E.P.; Engelen, M. 24-Hour protein, arginine and citrulline metabolism in fed critically ill children—A stable isotope tracer study. Clin. Nutr. 2017, 36, 876–887. [Google Scholar] [CrossRef]
- Arnett, D.C.; Persechini, A.; Tran, Q.K.; Black, D.J.; Johnson, C.K. Fluorescence quenching studies of structure and dynamics in calmodulin-eNOS complexes. FEBS Lett. 2015, 589, 1173–1178. [Google Scholar] [CrossRef] [Green Version]
- Li, H.; Raman, C.S.; Glaser, C.B.; Blasko, E.; Young, T.A.; Parkinson, J.F.; Whitlow, M.; Poulos, T.L. Crystal structures of zinc-free and -bound heme domain of human inducible nitric-oxide synthase. Implications for dimer stability and comparison with endothelial nitric-oxide synthase. J. Biol. Chem. 1999, 274, 21276–21284. [Google Scholar] [CrossRef] [Green Version]
- Crane, B.R.; Rosenfeld, R.J.; Arvai, A.S.; Ghosh, D.K.; Ghosh, S.; Tainer, J.A.; Stuehr, D.J.; Getzoff, E.D. N-terminal domain swapping and metal ion binding in nitric oxide synthase dimerization. EMBO J. 1999, 18, 6271–6281. [Google Scholar] [CrossRef] [Green Version]
- Daiber, A.; Kroller-Schon, S.; Oelze, M.; Hahad, O.; Li, H.; Schulz, R.; Steven, S.; Munzel, T. Oxidative stress and inflammation contribute to traffic noise-induced vascular and cerebral dysfunction via uncoupling of nitric oxide synthases. Redox Biol. 2020, 34, 101506. [Google Scholar] [CrossRef]
- Jayaram, R.; Goodfellow, N.; Zhang, M.H.; Reilly, S.; Crabtree, M.; De Silva, R.; Sayeed, R.; Casadei, B. Molecular mechanisms of myocardial nitroso-redox imbalance during on-pump cardiac surgery. Lancet 2015, 385 (Suppl. 1), S49. [Google Scholar] [CrossRef]
- Siu, K.L.; Lotz, C.; Ping, P.; Cai, H. Netrin-1 abrogates ischemia/reperfusion-induced cardiac mitochondrial dysfunction via nitric oxide-dependent attenuation of NOX4 activation and recoupling of NOS. J. Mol. Cell Cardiol. 2015, 78, 174–185. [Google Scholar] [CrossRef] [Green Version]
- Gebhart, V.; Reiss, K.; Kollau, A.; Mayer, B.; Gorren, A.C.F. Site and mechanism of uncoupling of nitric-oxide synthase: Uncoupling by monomerization and other misconceptions. Nitric Oxide 2019, 89, 14–21. [Google Scholar] [CrossRef] [PubMed]
- Yang, Y.M.; Huang, A.; Kaley, G.; Sun, D. eNOS uncoupling and endothelial dysfunction in aged vessels. Am. J. Physiol. Heart Circ. Physiol. 2009, 297, H1829–H1836. [Google Scholar] [CrossRef] [Green Version]
- Musicki, B.; Burnett, A.L. Constitutive NOS uncoupling and NADPH oxidase upregulation in the penis of type 2 diabetic men with erectile dysfunction. Andrology 2017, 5, 294–298. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bohmer, A.; Gambaryan, S.; Flentje, M.; Jordan, J.; Tsikas, D. [Ureido-(1)(5)N]citrulline UPLC-MS/MS nitric oxide synthase (NOS) activity assay: Development, validation, and applications to assess NOS uncoupling and human platelets NOS activity. J. Chromatogr. B Analyt. Technol. Biomed. Life Sci. 2014, 965, 173–182. [Google Scholar] [CrossRef] [PubMed]
- Kietadisorn, R.; Juni, R.P.; Moens, A.L. Tackling endothelial dysfunction by modulating NOS uncoupling: New insights into its pathogenesis and therapeutic possibilities. Am. J. Physiol. Endocrinol. Metab. 2012, 302, E481–E495. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xie, L.; Liu, Z.; Lu, H.; Zhang, W.; Mi, Q.; Li, X.; Tang, Y.; Chen, Q.; Ferro, A.; Ji, Y. Pyridoxine inhibits endothelial NOS uncoupling induced by oxidized low-density lipoprotein via the PKCalpha signalling pathway in human umbilical vein endothelial cells. Br. J. Pharmacol. 2012, 165, 754–764. [Google Scholar] [CrossRef] [Green Version]
- Crijns, H.J.; Schotten, U.; Moens, A.L. Is NOS uncoupling the missing link between atrial fibrillation and chronic non-ischaemic cardiomyopathy? Cardiovasc. Res. 2011, 91, 556. [Google Scholar] [CrossRef]
- Moens, A.L.; Leyton-Mange, J.S.; Niu, X.; Yang, R.; Cingolani, O.; Arkenbout, E.K.; Champion, H.C.; Bedja, D.; Gabrielson, K.L.; Chen, J.; et al. Adverse ventricular remodeling and exacerbated NOS uncoupling from pressure-overload in mice lacking the beta3-adrenoreceptor. J. Mol. Cell Cardiol. 2009, 47, 576–585. [Google Scholar] [CrossRef] [Green Version]
- Mollnau, H.; Schulz, E.; Daiber, A.; Baldus, S.; Oelze, M.; August, M.; Wendt, M.; Walter, U.; Geiger, C.; Agrawal, R.; et al. Nebivolol prevents vascular NOS III uncoupling in experimental hyperlipidemia and inhibits NADPH oxidase activity in inflammatory cells. Arterioscler. Thromb. Vasc. Biol. 2003, 23, 615–621. [Google Scholar] [CrossRef]
- Dikalova, A.; Aschner, J.L.; Kaplowitz, M.R.; Cunningham, G.; Summar, M.; Fike, C.D. Combined l-citrulline and tetrahydrobiopterin therapy improves NO signaling and ameliorates chronic hypoxia-induced pulmonary hypertension in newborn pigs. Am. J. Physiol. Lung Cell Mol. Physiol. 2020, 318, L762–L772. [Google Scholar] [CrossRef]
- Picciano, A.L.; Crane, B.R. A nitric oxide synthase-like protein from Synechococcus produces NO/NO3 (-) from l-arginine and NADPH in a tetrahydrobiopterin- and Ca(2+)-dependent manner. J. Biol. Chem. 2019, 294, 10708–10719. [Google Scholar] [CrossRef]
- Nagarkoti, S.; Sadaf, S.; Awasthi, D.; Chandra, T.; Jagavelu, K.; Kumar, S.; Dikshit, M. L-Arginine and tetrahydrobiopterin supported nitric oxide production is crucial for the microbicidal activity of neutrophils. Free Radic. Res. 2019, 53, 281–292. [Google Scholar] [CrossRef] [PubMed]
- Latini, A.; de Bortoli da Silva, L.; da Luz Scheffer, D.; Pires, A.C.S.; de Matos, F.J.; Nesi, R.T.; Ghisoni, K.; de Paula Martins, R.; de Oliveira, P.A.; Prediger, R.D.; et al. Tetrahydrobiopterin improves hippocampal nitric oxide-linked long-term memory. Mol. Genet. Metab. 2018, 125, 104–111. [Google Scholar] [CrossRef] [PubMed]
- Chuaiphichai, S.; Rashbrook, V.S.; Hale, A.B.; Trelfa, L.; Patel, J.; McNeill, E.; Lygate, C.A.; Channon, K.M.; Douglas, G. Endothelial Cell Tetrahydrobiopterin Modulates Sensitivity to Ang (Angiotensin) II-Induced Vascular Remodeling, Blood Pressure, and Abdominal Aortic Aneurysm. Hypertension 2018, 72, 128–138. [Google Scholar] [CrossRef] [PubMed]
- Ramasamy, S.; Haque, M.M.; Gangoda, M.; Stuehr, D.J. Tetrahydrobiopterin redox cycling in nitric oxide synthase: Evidence supports a through-heme electron delivery. FEBS J. 2016, 283, 4491–4501. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stuehr, D.J.; Kwon, N.S.; Nathan, C.F.; Griffith, O.W.; Feldman, P.L.; Wiseman, J. N omega-hydroxy-L-arginine is an intermediate in the biosynthesis of nitric oxide from L-arginine. J. Biol. Chem. 1991, 266, 6259–6263. [Google Scholar]
- Vasquez-Vivar, J.; Kalyanaraman, B.; Martasek, P.; Hogg, N.; Masters, B.S.; Karoui, H.; Tordo, P.; Pritchard, K.A., Jr. Superoxide generation by endothelial nitric oxide synthase: The influence of cofactors. Proc. Natl. Acad. Sci. USA 1998, 95, 9220–9225. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xia, Y.; Tsai, A.L.; Berka, V.; Zweier, J.L. Superoxide generation from endothelial nitric-oxide synthase. A Ca2+/calmodulin-dependent and tetrahydrobiopterin regulatory process. J. Biol. Chem. 1998, 273, 25804–25808. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Landmesser, U.; Dikalov, S.; Price, S.R.; McCann, L.; Fukai, T.; Holland, S.M.; Mitch, W.E.; Harrison, D.G. Oxidation of tetrahydrobiopterin leads to uncoupling of endothelial cell nitric oxide synthase in hypertension. J. Clin. Invest. 2003, 111, 1201–1209. [Google Scholar] [CrossRef] [PubMed]
- Moore, P.K.; al-Swayeh, O.A.; Chong, N.W.; Evans, R.A.; Gibson, A. L-NG-nitro arginine (L-NOARG), a novel, L-arginine-reversible inhibitor of endothelium-dependent vasodilatation in vitro. Br. J. Pharmacol. 1990, 99, 408–412. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gibson, A.; Mirzazadeh, S.; Hobbs, A.J.; Moore, P.K. L-NG-monomethyl arginine and L-NG-nitro arginine inhibit non-adrenergic, non-cholinergic relaxation of the mouse anococcygeus muscle. Br. J. Pharmacol. 1990, 99, 602–606. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- O’Kane, K.P.; Webb, D.J.; Collier, J.G.; Vallance, P.J. Local L-NG-monomethyl-arginine attenuates the vasodilator action of bradykinin in the human forearm. Br. J. Clin. Pharmacol. 1994, 38, 311–315. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fukuda, N.; Izumi, Y.; Soma, M.; Watanabe, Y.; Watanabe, M.; Hatano, M.; Sakuma, I.; Yasuda, H. L-NG-monomethyl arginine inhibits the vasodilating effects of low dose of endothelin-3 on rat mesenteric arteries. Biochem. Biophys. Res. Commun. 1990, 167, 739–745. [Google Scholar] [CrossRef]
- Gaw, A.J.; Aberdeen, J.; Humphrey, P.P.; Wadsworth, R.M.; Burnstock, G. Relaxation of sheep cerebral arteries by vasoactive intestinal polypeptide and neurogenic stimulation: Inhibition by L-NG-monomethyl arginine in endothelium-denuded vessels. Br. J. Pharmacol. 1991, 102, 567–572. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Toda, N.; Minami, Y.; Okamura, T. Inhibitory effects of L-NG-nitro-arginine on the synthesis of EDRF and the cerebroarterial response to vasodilator nerve stimulation. Life Sci. 1990, 47, 345–351. [Google Scholar] [CrossRef]
- Cozzi, M.R.; Guglielmini, G.; Battiston, M.; Momi, S.; Lombardi, E.; Miller, E.C.; De Zanet, D.; Mazzucato, M.; Gresele, P.; De Marco, L. Visualization of nitric oxide production by individual platelets during adhesion in flowing blood. Blood 2015, 125, 697–705. [Google Scholar] [CrossRef] [Green Version]
- Haussinger, D.; Gerok, W.; Sies, H. The effect of urea synthesis on extracellular pH in isolated perfused rat liver. Biochem. J. 1986, 236, 261–265. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mavri-Damelin, D.; Eaton, S.; Damelin, L.H.; Rees, M.; Hodgson, H.J.; Selden, C. Ornithine transcarbamylase and arginase I deficiency are responsible for diminished urea cycle function in the human hepatoblastoma cell line HepG2. Int. J. Biochem. Cell Biol. 2007, 39, 555–564. [Google Scholar] [CrossRef]
- Callery, E.M.; Elinson, R.P. Developmental regulation of the urea-cycle enzyme arginase in the direct developing frog Eleutherodactylus coqui. J. Exp. Zool. 1996, 275, 61–66. [Google Scholar] [CrossRef]
- Snellman, K.; Aperia, A.; Broberger, O. Studies of renal urea cycle enzymes. II. Human renal arginase activity and location of the adaptive changes of renal arginase in the protein deprived rat. Scand. J. Clin. Lab. Invest. 1979, 39, 337–342. [Google Scholar] [CrossRef]
- Chan, P.Y.; Cossins, E.A. Regulation of arginase levels by urea and intermediates of the Krebs-Henseleit cycle in Saccharomyces cerevisiae. FEBS Lett. 1972, 19, 335–339. [Google Scholar] [CrossRef] [Green Version]
- Pernow, J.; Jung, C. Arginase as a potential target in the treatment of cardiovascular disease: Reversal of arginine steal? Cardiovasc. Res. 2013, 98, 334–343. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pandey, D.; Romer, L.; Berkowitz, D.E. Arginase II: Atherogenesis beyond enzyme activity. J. Am. Heart Assoc. 2013, 2, e000392. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kuhn, N.J.; Ward, S.; Piponski, M.; Young, T.W. Purification of human hepatic arginase and its manganese (II)-dependent and pH-dependent interconversion between active and inactive forms: A possible pH-sensing function of the enzyme on the ornithine cycle. Arch. Biochem. Biophys. 1995, 320, 24–34. [Google Scholar] [CrossRef]
- Sumitani, A. Immunological studies of liver arginase in man and various kinds of vertebrates. Part I: Microquantification of arginase enzyme in liver tissue by quantitative immunoelectrophoresis. Part II: Immunological studies of human liver arginase. Hiroshima J. Med. Sci. 1977, 26, 59. [Google Scholar]
- Kim, J.H.; Bugaj, L.J.; Oh, Y.J.; Bivalacqua, T.J.; Ryoo, S.; Soucy, K.G.; Santhanam, L.; Webb, A.; Camara, A.; Sikka, G.; et al. Arginase inhibition restores NOS coupling and reverses endothelial dysfunction and vascular stiffness in old rats. J. Appl. Physiol. (1985) 2009, 107, 1249–1257. [Google Scholar] [CrossRef] [Green Version]
- Romero, M.J.; Platt, D.H.; Tawfik, H.E.; Labazi, M.; El-Remessy, A.B.; Bartoli, M.; Caldwell, R.B.; Caldwell, R.W. Diabetes-induced coronary vascular dysfunction involves increased arginase activity. Circ. Res. 2008, 102, 95–102. [Google Scholar] [CrossRef]
- Mahdi, A.; Kovamees, O.; Pernow, J. Improvement in endothelial function in cardiovascular disease—Is arginase the target? Int. J. Cardiol. 2020, 301, 207–214. [Google Scholar] [CrossRef]
- Wernly, B.; Pernow, J.; Kelm, M.; Jung, C. The role of arginase in the microcirculation in cardiovascular disease. Clin. Hemorheol. Microcirc. 2020, 74, 79–92. [Google Scholar] [CrossRef]
- Chandrasekharan, U.M.; Wang, Z.; Wu, Y.; Wilson Tang, W.H.; Hazen, S.L.; Wang, S.; Elaine Husni, M. Elevated levels of plasma symmetric dimethylarginine and increased arginase activity as potential indicators of cardiovascular comorbidity in rheumatoid arthritis. Arthritis Res. Ther. 2018, 20, 123. [Google Scholar] [CrossRef] [Green Version]
- Yang, Z.; Ming, X.F. Functions of arginase isoforms in macrophage inflammatory responses: Impact on cardiovascular diseases and metabolic disorders. Front. Immunol. 2014, 5, 533. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bagnost, T.; Ma, L.; da Silva, R.F.; Rezakhaniha, R.; Houdayer, C.; Stergiopulos, N.; Andre, C.; Guillaume, Y.; Berthelot, A.; Demougeot, C. Cardiovascular effects of arginase inhibition in spontaneously hypertensive rats with fully developed hypertension. Cardiovasc. Res. 2010, 87, 569–577. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Huang, J.; Liu, C.; Ming, X.F.; Yang, Z. Inhibition of p38mapk Reduces Adipose Tissue Inflammation in Aging Mediated by Arginase-II. Pharmacology 2020, 1–14. [Google Scholar] [CrossRef] [PubMed]
- Masi, S.; Colucci, R.; Duranti, E.; Nannipieri, M.; Anselmino, M.; Ippolito, C.; Tirotta, E.; Georgiopoulos, G.; Garelli, F.; Nericcio, A.; et al. Aging Modulates the Influence of Arginase on Endothelial Dysfunction in Obesity. Arterioscler. Thromb. Vasc. Biol. 2018, 38, 2474–2483. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cecilio, C.A.; Costa, E.H.; Simioni, P.U.; Gabriel, D.L.; Tamashiro, W.M. Aging alters the production of iNOS, arginase and cytokines in murine macrophages. Braz. J. Med. Biol. Res. 2011, 44, 671–681. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Katusic, Z.S. Mechanisms of endothelial dysfunction induced by aging: Role of arginase I. Circ. Res. 2007, 101, 640–641. [Google Scholar] [CrossRef] [Green Version]
- Sakai, Y.; Masuda, H.; Kihara, K.; Kurosaki, E.; Yamauchi, Y.; Azuma, H. Involvement of increased arginase activity in impaired cavernous relaxation with aging in the rabbit. J. Urol. 2004, 172, 369–373. [Google Scholar] [CrossRef]
- Berkowitz, D.E.; White, R.; Li, D.; Minhas, K.M.; Cernetich, A.; Kim, S.; Burke, S.; Shoukas, A.A.; Nyhan, D.; Champion, H.C.; et al. Arginase reciprocally regulates nitric oxide synthase activity and contributes to endothelial dysfunction in aging blood vessels. Circulation 2003, 108, 2000–2006. [Google Scholar] [CrossRef] [Green Version]
- Cheng, H.; Lu, T.; Wang, J.; Xia, Y.; Chai, X.; Zhang, M.; Yao, Y.; Zhou, N.; Zhou, S.; Chen, X.; et al. HuangqiGuizhiWuwu Decoction Prevents Vascular Dysfunction in Diabetes via Inhibition of Endothelial Arginase 1. Front. Physiol 2020, 11, 201. [Google Scholar] [CrossRef]
- Folley, S.J.; Greenbaum, A.L. Effect of experimental diabetes on tissue arginase levels. J. Endocrinol. 1949, 6. [Google Scholar] [PubMed]
- Yang, J.; Zheng, X.; Mahdi, A.; Zhou, Z.; Tratsiakovich, Y.; Jiao, T.; Kiss, A.; Kovamees, O.; Alvarsson, M.; Catrina, S.B.; et al. Red Blood Cells in Type 2 Diabetes Impair Cardiac Post-Ischemic Recovery Through an Arginase-Dependent Modulation of Nitric Oxide Synthase and Reactive Oxygen Species. JACC Basic Transl. Sci. 2018, 3, 450–463. [Google Scholar] [CrossRef] [PubMed]
- Zhou, Z.; Mahdi, A.; Tratsiakovich, Y.; Zahoran, S.; Kovamees, O.; Nordin, F.; Uribe Gonzalez, A.E.; Alvarsson, M.; Ostenson, C.G.; Andersson, D.C.; et al. Erythrocytes From Patients With Type 2 Diabetes Induce Endothelial Dysfunction Via Arginase, I.J. Am. Coll. Cardiol. 2018, 72, 769–780. [Google Scholar] [CrossRef] [PubMed]
- Zhang, H.; Liu, J.; Qu, D.; Wang, L.; Wong, C.M.; Lau, C.W.; Huang, Y.; Wang, Y.F.; Huang, H.; Xia, Y.; et al. Serum exosomes mediate delivery of arginase 1 as a novel mechanism for endothelial dysfunction in diabetes. Proc. Natl. Acad. Sci. USA 2018, 115, E6927–E6936. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shosha, E.; Xu, Z.; Narayanan, S.P.; Lemtalsi, T.; Fouda, A.Y.; Rojas, M.; Xing, J.; Fulton, D.; Caldwell, R.W.; Caldwell, R.B. Mechanisms of Diabetes-Induced Endothelial Cell Senescence: Role of Arginase 1. Int. J. Mol. Sci. 2018, 19, 1215. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kovamees, O.; Shemyakin, A.; Checa, A.; Wheelock, C.E.; Lundberg, J.O.; Ostenson, C.G.; Pernow, J. Arginase Inhibition Improves Microvascular Endothelial Function in Patients with Type 2 Diabetes Mellitus. J. Clin. Endocrinol. Metab. 2016, 101, 3952–3958. [Google Scholar] [CrossRef]
- Yao, L.; Chandra, S.; Toque, H.A.; Bhatta, A.; Rojas, M.; Caldwell, R.B.; Caldwell, R.W. Prevention of diabetes-induced arginase activation and vascular dysfunction by Rho kinase (ROCK) knockout. Cardiovasc. Res. 2013, 97, 509–519. [Google Scholar] [CrossRef] [Green Version]
- Elms, S.C.; Toque, H.A.; Rojas, M.; Xu, Z.; Caldwell, R.W.; Caldwell, R.B. The role of arginase I in diabetes-induced retinal vascular dysfunction in mouse and rat models of diabetes. Diabetologia 2013, 56, 654–662. [Google Scholar] [CrossRef] [Green Version]
- Shemyakin, A.; Kovamees, O.; Rafnsson, A.; Bohm, F.; Svenarud, P.; Settergren, M.; Jung, C.; Pernow, J. Arginase inhibition improves endothelial function in patients with coronary artery disease and type 2 diabetes mellitus. Circulation 2012, 126, 2943–2950. [Google Scholar] [CrossRef] [Green Version]
- Ren, B.; Van Kampen, E.; Van Berkel, T.J.; Cruickshank, S.M.; Van Eck, M. Hematopoietic arginase 1 deficiency results in decreased leukocytosis and increased foam cell formation but does not affect atherosclerosis. Atherosclerosis 2017, 256, 35–46. [Google Scholar] [CrossRef] [Green Version]
- Teupser, D.; Burkhardt, R.; Wilfert, W.; Haffner, I.; Nebendahl, K.; Thiery, J. Identification of macrophage arginase I as a new candidate gene of atherosclerosis resistance. Arterioscler. Thromb. Vasc. Biol. 2006, 26, 365–371. [Google Scholar] [CrossRef] [Green Version]
- Gimbrone, M.A., Jr.; Garcia-Cardena, G. Endothelial Cell Dysfunction and the Pathobiology of Atherosclerosis. Circ. Res. 2016, 118, 620–636. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rajendran, P.; Rengarajan, T.; Thangavel, J.; Nishigaki, Y.; Sakthisekaran, D.; Sethi, G.; Nishigaki, I. The vascular endothelium and human diseases. Int. J. Biol. Sci. 2013, 9, 1057–1069. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chirinos, J.A.; David, R.; Bralley, J.A.; Zea-Diaz, H.; Munoz-Atahualpa, E.; Corrales-Medina, F.; Cuba-Bustinza, C.; Chirinos-Pacheco, J.; Medina-Lezama, J. Endogenous nitric oxide synthase inhibitors, arterial hemodynamics, and subclinical vascular disease: The Prevencion Study. Hypertension 2008, 52, 1051–1059. [Google Scholar] [CrossRef] [PubMed]
- Bermejo-Martin, J.F.; Almansa, R.; Torres, A.; Gonzalez-Rivera, M.; Kelvin, D.J. COVID-19 as a cardiovascular disease: The potential role of chronic endothelial dysfunction. Cardiovasc. Res. 2020, 116, e132–e133. [Google Scholar] [CrossRef]
- Daiber, A.; Chlopicki, S. Revisiting pharmacology of oxidative stress and endothelial dysfunction in cardiovascular disease: Evidence for redox-based therapies. Free Radic. Biol. Med. 2020. [Google Scholar] [CrossRef]
- Lima, B.B.; Hammadah, M.; Kim, J.H.; Uphoff, I.; Shah, A.; Levantsevych, O.; Almuwaqqat, Z.; Moazzami, K.; Sullivan, S.; Ward, L.; et al. Association of Transient Endothelial Dysfunction Induced by Mental Stress With Major Adverse Cardiovascular Events in Men and Women With Coronary Artery Disease. JAMA Cardiol. 2019, 4, 988–996. [Google Scholar] [CrossRef]
- Yepuri, G.; Ramasamy, R. Significance and Mechanistic Relevance of SIRT6-Mediated Endothelial Dysfunction in Cardiovascular Disease Progression. Circ. Res. 2019, 124, 1408–1410. [Google Scholar] [CrossRef]
- Daiber, A.; Xia, N.; Steven, S.; Oelze, M.; Hanf, A.; Kroller-Schon, S.; Munzel, T.; Li, H. New Therapeutic Implications of Endothelial Nitric Oxide Synthase (eNOS) Function/Dysfunction in Cardiovascular Disease. Int. J. Mol. Sci. 2019, 20, 187. [Google Scholar] [CrossRef] [Green Version]
- Maruhashi, T.; Soga, J.; Fujimura, N.; Idei, N.; Mikami, S.; Iwamoto, Y.; Iwamoto, A.; Kajikawa, M.; Matsumoto, T.; Oda, N.; et al. Endothelial Dysfunction, Increased Arterial Stiffness, and Cardiovascular Risk Prediction in Patients with Coronary Artery Disease: FMD-J (Flow-Mediated Dilation Japan) Study A. J. Am. Heart Assoc. 2018, 7, e008588. [Google Scholar] [CrossRef] [Green Version]
- Akasaka, T.; Sueta, D.; Tabata, N.; Takashio, S.; Yamamoto, E.; Izumiya, Y.; Tsujita, K.; Kojima, S.; Kaikita, K.; Matsui, K.; et al. Effects of the Mean Amplitude of Glycemic Excursions and Vascular Endothelial Dysfunction on Cardiovascular Events in Nondiabetic Patients With Coronary Artery Disease. J. Am. Heart Assoc. 2017, 6, e004841. [Google Scholar] [CrossRef]
- Chello, M.; Nenna, A. Ethnicity, ABO group, endothelial dysfunction and cardiovascular disease: Multiple connections, multiple implications. Atherosclerosis 2016, 251, 514–515. [Google Scholar] [CrossRef] [PubMed]
- Erqou, S.; Kip, K.E.; Mulukutla, S.R.; Aiyer, A.N.; Reis, S.E. Endothelial Dysfunction and Racial Disparities in Mortality and Adverse Cardiovascular Disease Outcomes. Clin. Cardiol. 2016, 39, 338–344. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bodolay, E.; Prohaszka, Z.; Paragh, G.; Csipo, I.; Nagy, G.; Laczik, R.; Demeter, N.; Zold, E.; Nakken, B.; Szegedi, G.; et al. Increased levels of anti-heat-shock protein 60 (anti-Hsp60) indicate endothelial dysfunction, atherosclerosis and cardiovascular diseases in patients with mixed connective tissue disease. Immunol. Res. 2014, 60, 50–59. [Google Scholar] [CrossRef] [PubMed]
- Moody, W.E.; Edwards, N.C.; Madhani, M.; Chue, C.D.; Steeds, R.P.; Ferro, C.J.; Townend, J.N. Endothelial dysfunction and cardiovascular disease in early-stage chronic kidney disease: Cause or association? Atherosclerosis 2012, 223, 86–94. [Google Scholar] [CrossRef] [PubMed]
- Versari, D.; Daghini, E.; Virdis, A.; Ghiadoni, L.; Taddei, S. Endothelial dysfunction as a target for prevention of cardiovascular disease. Diabetes Care 2009, 32 (Suppl. 2), S314–S321. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nozaki, T.; Sugiyama, S.; Koga, H.; Sugamura, K.; Ohba, K.; Matsuzawa, Y.; Sumida, H.; Matsui, K.; Jinnouchi, H.; Ogawa, H. Significance of a multiple biomarkers strategy including endothelial dysfunction to improve risk stratification for cardiovascular events in patients at high risk for coronary heart disease. J. Am. Coll. Cardiol. 2009, 54, 601–608. [Google Scholar] [CrossRef] [Green Version]
- Martin, B.J.; Anderson, T.J. Risk prediction in cardiovascular disease: The prognostic significance of endothelial dysfunction. Can. J. Cardiol. 2009, 25 (Suppl. A), 15A–20A. [Google Scholar] [CrossRef] [Green Version]
- Nin, J.W.; Ferreira, I.; Schalkwijk, C.G.; Prins, M.H.; Chaturvedi, N.; Fuller, J.H.; Stehouwer, C.D.; EURODIAB Prospective Complications Study Group. Levels of soluble receptor for AGE are cross-sectionally associated with cardiovascular disease in type 1 diabetes, and this association is partially mediated by endothelial and renal dysfunction and by low-grade inflammation: The Eurodiab Prospective Complications Study. Diabetologia 2009, 52, 705–714. [Google Scholar]
- Friedewald, V.E.; Giles, T.D.; Pool, J.L.; Yancy, C.W.; Roberts, W.C. The Editor’s Roundtable: Endothelial dysfunction in cardiovascular disease. Am. J. Cardiol. 2008, 102, 418–423. [Google Scholar] [CrossRef]
- Rodford, J.L.; Torrens, C.; Siow, R.C.; Mann, G.E.; Hanson, M.A.; Clough, G.F. Endothelial dysfunction and reduced antioxidant protection in an animal model of the developmental origins of cardiovascular disease. J. Physiol. 2008, 586, 4709–4720. [Google Scholar] [CrossRef]
- Xu, Y.; Buikema, H.; van Gilst, W.H.; Henning, R.H. Caveolae and endothelial dysfunction: Filling the caves in cardiovascular disease. Eur. J. Pharmacol. 2008, 585, 256–260. [Google Scholar] [CrossRef] [PubMed]
- Subah Packer, C. Estrogen protection, oxidized LDL, endothelial dysfunction and vasorelaxation in cardiovascular disease: New insights into a complex issue. Cardiovasc. Res. 2007, 73, 6–7. [Google Scholar] [CrossRef] [PubMed]
- Ruef, J.; Marz, W.; Winkelmann, B.R. Markers for endothelial dysfunction, but not markers for oxidative stress correlate with classical risk factors and the severity of coronary artery disease. (A subgroup analysis from the Ludwigshafen Risk and Cardiovascular Health Study). Scand. Cardiovasc. J. 2006, 40, 274–279. [Google Scholar] [CrossRef] [PubMed]
- Hanson, M.; Gluckman, P. Endothelial dysfunction and cardiovascular disease: The role of predictive adaptive responses. Heart 2005, 91, 864–866. [Google Scholar] [CrossRef] [Green Version]
- Brevetti, G.; Silvestro, A.; Schiano, V.; Chiariello, M. Endothelial dysfunction and cardiovascular risk prediction in peripheral arterial disease: Additive value of flow-mediated dilation to ankle-brachial pressure index. Circulation 2003, 108, 2093–2098. [Google Scholar] [CrossRef]
- Gokce, N.; Keaney, J.F., Jr.; Hunter, L.M.; Watkins, M.T.; Nedeljkovic, Z.S.; Menzoian, J.O.; Vita, J.A. Predictive value of noninvasively determined endothelial dysfunction for long-term cardiovascular events in patients with peripheral vascular disease. J. Am. Coll. Cardiol. 2003, 41, 1769–1775. [Google Scholar] [CrossRef] [Green Version]
- Erhardt, L.R. Endothelial dysfunction and cardiovascular disease: The promise of blocking the renin-angiotensin system. Int. J. Clin. Pract. 2003, 57, 211–218. [Google Scholar]
- Sardu, C.; Gambardella, J.; Morelli, M.B.; Wang, X.; Marfella, R.; Santulli, G. Is COVID-19 an Endothelial Disease? Clinical and Basic Evidence. Preprints 2020. [Google Scholar] [CrossRef]
- Sardu, C.; Gambardella, J.; Morelli, M.B.; Wang, X.; Marfella, R.; Santulli, G. Hypertension, Thrombosis, Kidney Failure, and Diabetes: Is COVID-19 an Endothelial Disease? A Comprehensive Evaluation of Clinical and Basic Evidence. J. Clin. Med. 2020, 9, 1417. [Google Scholar] [CrossRef]
- Paules, C.I.; Marston, H.D.; Fauci, A.S. Coronavirus Infections-More Than Just the Common Cold. JAMA 2020, 323, 707–708. [Google Scholar] [CrossRef] [Green Version]
- Hui, D.S.; Azhar, E.; Madani, T.A.; Ntoumi, F.; Kock, R.; Dar, O.; Ippolito, G.; McHugh, T.D.; Memish, Z.A.; Drosten, C.; et al. The continuing 2019-nCoV epidemic threat of novel coronaviruses to global health—The latest 2019 novel coronavirus outbreak in Wuhan, China. Int. J. Infect. Dis. 2020, 91, 264–266. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Colmenero, I.; Santonja, C.; Alonso-Riano, M.; Noguera-Morel, L.; Hernandez-Martin, A.; Andina, D.; Wiesner, T.; Rodriguez-Peralto, J.L.; Requena, L.; Torrelo, A. SARS-CoV-2 endothelial infection causes COVID-19 chilblains: Histopathological, immunohistochemical and ultraestructural study of 7 paediatric cases. Br. J. Dermatol. 2020. [Google Scholar] [CrossRef]
- Hanafi, R.; Roger, P.A.; Perin, B.; Kuchcinski, G.; Deleval, N.; Dallery, F.; Michel, D.; Hacein-Bey, L.; Pruvo, J.P.; Outteryck, O.; et al. COVID-19 Neurologic Complication with CNS Vasculitis-Like Pattern. AJNR Am. J. Neuroradiol. 2020. [Google Scholar] [CrossRef] [PubMed]
- Mosleh, W.; Chen, K.; Pfau, S.E.; Vashist, A. Endotheliitis and Endothelial Dysfunction in Patients with COVID-19: Its Role in Thrombosis and Adverse Outcomes. J. Clin. Med. 2020, 9, 1862. [Google Scholar] [CrossRef] [PubMed]
- Pons, S.; Fodil, S.; Azoulay, E.; Zafrani, L. The vascular endothelium: The cornerstone of organ dysfunction in severe SARS-CoV-2 infection. Crit. Care 2020, 24, 353. [Google Scholar] [CrossRef]
- Konopka, K.E.; Nguyen, T.; Jentzen, J.M.; Rayes, O.; Schmidt, C.J.; Wilson, A.M.; Farver, C.F.; Myers, J.L. Diffuse Alveolar Damage (DAD) from Coronavirus Disease 2019 Infection is Morphologically Indistinguishable from Other Causes of DAD. Histopathology 2020. [Google Scholar] [CrossRef]
- Benger, M.; Williams, O.; Siddiqui, J.; Sztriha, L. Intracerebral haemorrhage and COVID-19: Clinical characteristics from a case series. Brain Behav. Immun. 2020, 88, 940–944. [Google Scholar] [CrossRef]
- Wang, J.; Saguner, A.M.; An, J.; Ning, Y.; Yan, Y.; Li, G. Dysfunctional Coagulation in COVID-19: From Cell to Bedside. Adv. Ther. 2020, 37, 3033–3039. [Google Scholar] [CrossRef]
- Ackermann, M.; Verleden, S.E.; Kuehnel, M.; Haverich, A.; Welte, T.; Laenger, F.; Vanstapel, A.; Werlein, C.; Stark, H.; Tzankov, A.; et al. Pulmonary Vascular Endothelialitis, Thrombosis, and Angiogenesis in Covid-19. N. Engl. J. Med. 2020. [Google Scholar] [CrossRef]
- Varga, Z.; Flammer, A.J.; Steiger, P.; Haberecker, M.; Andermatt, R.; Zinkernagel, A.S.; Mehra, M.R.; Schuepbach, R.A.; Ruschitzka, F.; Moch, H. Endothelial cell infection and endotheliitis in COVID-19. Lancet 2020, 395, 1417–1418. [Google Scholar] [CrossRef]
- Jones, V.G.; Mills, M.; Suarez, D.; Hogan, C.A.; Yeh, D.; Bradley Segal, J.; Nguyen, E.L.; Barsh, G.R.; Maskatia, S.; Mathew, R. COVID-19 and Kawasaki Disease: Novel Virus and Novel Case. Hosp. Pediatr. 2020, 10, 537–540. [Google Scholar] [CrossRef] [PubMed]
- Cyr, A.R.; Huckaby, L.V.; Shiva, S.S.; Zuckerbraun, B.S. Nitric Oxide and Endothelial Dysfunction. Crit. Care Clin. 2020, 36, 307–321. [Google Scholar] [CrossRef] [PubMed]
- Chen, J.; Zhang, J.; Shaik, N.F.; Yi, B.; Wei, X.; Yang, X.F.; Naik, U.P.; Summer, R.; Yan, G.; Xu, X.; et al. The histone deacetylase inhibitor tubacin mitigates endothelial dysfunction by up-regulating the expression of endothelial nitric oxide synthase. J. Biol. Chem. 2019, 294, 19565–19576. [Google Scholar] [CrossRef] [PubMed]
- Lomeli, O.; Perez-Torres, I.; Marquez, R.; Criales, S.; Mejia, A.M.; Chiney, C.; Hernandez-Lemus, E.; Soto, M.E. The Evaluation of Flow-Mediated Vasodilation in the Brachial Artery Correlates With Endothelial Dysfunction Evaluated by Nitric Oxide Synthase Metabolites in Marfan Syndrome Patients. Front. Physiol. 2018, 9, 965. [Google Scholar] [CrossRef]
- Evans, R.W.; Fernstrom, J.D.; Thompson, J.; Morris, S.M., Jr.; Kuller, L.H. Biochemical responses of healthy subjects during dietary supplementation with L-arginine. J. Nutr. Biochem. 2004, 15, 534–539. [Google Scholar] [CrossRef]
- Alvares, T.S.; Conte-Junior, C.A.; Silva, J.T.; Paschoalin, V.M. Acute L-Arginine supplementation does not increase nitric oxide production in healthy subjects. Nutr. Metab. 2012, 9, 54. [Google Scholar] [CrossRef] [Green Version]
- Meirelles, C.M.; Matsuura, C.; Silva, R.S., Jr.; Guimaraes, F.F.; Gomes, P.S.C. Acute Effects of L-Arginine Supplementation on Oxygen Consumption Kinetics and Muscle Oxyhemoglobin and Deoxyhemoglobin during Treadmill Running in Male Adults. Int. J. Exerc. Sci. 2019, 12, 444–455. [Google Scholar]
- Liu, T.H.; Wu, C.L.; Chiang, C.W.; Lo, Y.W.; Tseng, H.F.; Chang, C.K. No effect of short-term arginine supplementation on nitric oxide production, metabolism and performance in intermittent exercise in athletes. J. Nutr. Biochem. 2009, 20, 462–468. [Google Scholar] [CrossRef]
- Schwedhelm, E.; Maas, R.; Freese, R.; Jung, D.; Lukacs, Z.; Jambrecina, A.; Spickler, W.; Schulze, F.; Boger, R.H. Pharmacokinetic and pharmacodynamic properties of oral L-citrulline and L-arginine: Impact on nitric oxide metabolism. Br. J. Clin. Pharmacol. 2008, 65, 51–59. [Google Scholar] [CrossRef]
- Bredt, D.S.; Snyder, S.H. Isolation of nitric oxide synthetase, a calmodulin-requiring enzyme. Proc. Natl. Acad. Sci. USA 1990, 87, 682–685. [Google Scholar] [CrossRef] [Green Version]
- Joyner, M.J.; Casey, D.P. Regulation of increased blood flow (hyperemia) to muscles during exercise: A hierarchy of competing physiological needs. Physiol. Rev. 2015, 95, 549–601. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alvares, T.S.; Meirelles, C.M.; Bhambhani, Y.N.; Paschoalin, V.M.; Gomes, P.S. L-Arginine as a potential ergogenic aid in healthy subjects. Sports Med. 2011, 41, 233–248. [Google Scholar] [CrossRef] [PubMed]
- Doutreleau, S.; Rouyer, O.; Di Marco, P.; Lonsdorfer, E.; Richard, R.; Piquard, F.; Geny, B. L-arginine supplementation improves exercise capacity after a heart transplant. Am. J. Clin. Nutr. 2010, 91, 1261–1267. [Google Scholar] [CrossRef] [PubMed]
- Maughan, R.J. Nutritional ergogenic aids and exercise performance. Nutr. Res. Rev. 1999, 12, 255–280. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Suzuki, I.; Sakuraba, K.; Horiike, T.; Kishi, T.; Yabe, J.; Suzuki, T.; Morita, M.; Nishimura, A.; Suzuki, Y. A combination of oral L-citrulline and L-arginine improved 10-min full-power cycling test performance in male collegiate soccer players: A randomized crossover trial. Eur. J. Appl. Physiol. 2019, 119, 1075–1084. [Google Scholar] [CrossRef] [Green Version]
- Andrade, W.B.; Jacinto, J.L.; da Silva, D.K.; Roveratti, M.C.; Estoche, J.M.; Oliveira, D.B.; Balvedi, M.C.W.; da Silva, R.A.; Aguiar, A.F. l-Arginine supplementation does not improve muscle function during recovery from resistance exercise. Appl. Physiol. Nutr. Metab. 2018, 43, 928–936. [Google Scholar] [CrossRef]
- Dioguardi, F.S. To give or not to give? Lessons from the arginine paradox. J. Nutrigenet. Nutrige. 2011, 4, 90–98. [Google Scholar] [CrossRef]
- Ueda, S.; Petrie, J.R.; Cleland, S.J.; Elliott, H.L.; Connell, J.M. Insulin vasodilatation and the “arginine paradox”. Lancet 1998, 351, 959–960. [Google Scholar] [CrossRef]
- Kurz, S.; Harrison, D.G. Insulin and the arginine paradox. J. Clin. Investig. 1997, 99, 369–370. [Google Scholar] [CrossRef]
- Vallance, P.; Leone, A.; Calver, A.; Collier, J.; Moncada, S. Endogenous dimethylarginine as an inhibitor of nitric oxide synthesis. J. Cardiovasc. Pharmacol. 1992, 20 (Suppl. 12), S60–S62. [Google Scholar] [CrossRef]
- Bartnicki, P.; Kowalczyk, M.; Franczyk-Skora, B.; Baj, Z.; Rysz, J. Evaluation of Endothelial (dys)Function, Left Ventricular Structure and Function in Patients with Chronic Kidney Disease. Curr. Vasc. Pharmacol. 2016, 14, 360–367. [Google Scholar] [CrossRef] [PubMed]
- Bouras, G.; Deftereos, S.; Tousoulis, D.; Giannopoulos, G.; Chatzis, G.; Tsounis, D.; Cleman, M.W.; Stefanadis, C. Asymmetric Dimethylarginine (ADMA): A promising biomarker for cardiovascular disease? Curr. Top. Med. Chem. 2013, 13, 180–200. [Google Scholar] [CrossRef] [PubMed]
- Janes, F.; Cifu, A.; Pessa, M.E.; Domenis, R.; Gigli, G.L.; Sanvilli, N.; Nilo, A.; Garbo, R.; Curcio, F.; Giacomello, R.; et al. ADMA as a possible marker of endothelial damage. A study in young asymptomatic patients with cerebral small vessel disease. Sci. Rep. 2019, 9, 14207. [Google Scholar] [CrossRef] [PubMed]
- Strobel, J.; Muller, F.; Zolk, O.; Endress, B.; Konig, J.; Fromm, M.F.; Maas, R. Transport of asymmetric dimethylarginine (ADMA) by cationic amino acid transporter 2 (CAT2), organic cation transporter 2 (OCT2) and multidrug and toxin extrusion protein 1 (MATE1). Amino Acids 2013, 45, 989–1002. [Google Scholar] [CrossRef] [PubMed]
- Closs, E.I.; Basha, F.Z.; Habermeier, A.; Forstermann, U. Interference of L-arginine analogues with L-arginine transport mediated by the y+ carrier hCAT-2B. Nitric Oxide 1997, 1, 65–73. [Google Scholar] [CrossRef]
- Wijnands, K.A.; Hoeksema, M.A.; Meesters, D.M.; van den Akker, N.M.; Molin, D.G.; Briede, J.J.; Ghosh, M.; Kohler, S.E.; van Zandvoort, M.A.; de Winther, M.P.; et al. Arginase-1 deficiency regulates arginine concentrations and NOS2-mediated NO production during endotoxemia. PLoS ONE 2014, 9, e86135. [Google Scholar] [CrossRef] [Green Version]
- Boger, R.H.; Bode-Boger, S.M.; Szuba, A.; Tsao, P.S.; Chan, J.R.; Tangphao, O.; Blaschke, T.F.; Cooke, J.P. Asymmetric dimethylarginine (ADMA): A novel risk factor for endothelial dysfunction: Its role in hypercholesterolemia. Circulation 1998, 98, 1842–1847. [Google Scholar] [CrossRef] [Green Version]
- Nijveldt, R.J.; Teerlink, T.; Van Der Hoven, B.; Siroen, M.P.; Kuik, D.J.; Rauwerda, J.A.; van Leeuwen, P.A. Asymmetrical dimethylarginine (ADMA) in critically ill patients: High plasma ADMA concentration is an independent risk factor of ICU mortality. Clin. Nutr. 2003, 22, 23–30. [Google Scholar] [CrossRef] [Green Version]
- Abedini, S.; Meinitzer, A.; Holme, I.; Marz, W.; Weihrauch, G.; Fellstrom, B.; Jardine, A.; Holdaas, H. Asymmetrical dimethylarginine is associated with renal and cardiovascular outcomes and all-cause mortality in renal transplant recipients. Kidney Int. 2010, 77, 44–50. [Google Scholar] [CrossRef] [Green Version]
- Krzyzanowska, K.; Mittermayer, F.; Wolzt, M.; Schernthaner, G. Asymmetric dimethylarginine predicts cardiovascular events in patients with type 2 diabetes. Diabetes Care 2007, 30, 1834–1839. [Google Scholar] [CrossRef] [Green Version]
- Nanayakkara, P.W.; Teerlink, T.; Stehouwer, C.D.; Allajar, D.; Spijkerman, A.; Schalkwijk, C.; ter Wee, P.M.; van Guldener, C. Plasma asymmetric dimethylarginine (ADMA) concentration is independently associated with carotid intima-media thickness and plasma soluble vascular cell adhesion molecule-1 (sVCAM-1) concentration in patients with mild-to-moderate renal failure. Kidney Int. 2005, 68, 2230–2236. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zoccali, C.; Bode-Boger, S.; Mallamaci, F.; Benedetto, F.; Tripepi, G.; Malatino, L.; Cataliotti, A.; Bellanuova, I.; Fermo, I.; Frolich, J.; et al. Plasma concentration of asymmetrical dimethylarginine and mortality in patients with end-stage renal disease: A prospective study. Lancet 2001, 358, 2113–2117. [Google Scholar] [CrossRef]
- Abbasi, F.; Asagmi, T.; Cooke, J.P.; Lamendola, C.; McLaughlin, T.; Reaven, G.M.; Stuehlinger, M.; Tsao, P.S. Plasma concentrations of asymmetric dimethylarginine are increased in patients with type 2 diabetes mellitus. Am. J. Cardiol. 2001, 88, 1201–1203. [Google Scholar] [CrossRef]
- Furuki, K.; Adachi, H.; Matsuoka, H.; Enomoto, M.; Satoh, A.; Hino, A.; Hirai, Y.; Imaizumi, T. Plasma levels of asymmetric dimethylarginine (ADMA) are related to intima-media thickness of the carotid artery: An epidemiological study. Atherosclerosis 2007, 191, 206–210. [Google Scholar] [CrossRef]
- Valkonen, V.P.; Paiva, H.; Salonen, J.T.; Lakka, T.A.; Lehtimaki, T.; Laakso, J.; Laaksonen, R. Risk of acute coronary events and serum concentration of asymmetrical dimethylarginine. Lancet 2001, 358, 2127–2128. [Google Scholar] [CrossRef]
- Surdacki, A.; Nowicki, M.; Sandmann, J.; Tsikas, D.; Boeger, R.H.; Bode-Boeger, S.M.; Kruszelnicka-Kwiatkowska, O.; Kokot, F.; Dubiel, J.S.; Froelich, J.C. Reduced urinary excretion of nitric oxide metabolites and increased plasma levels of asymmetric dimethylarginine in men with essential hypertension. J. Cardiovasc. Pharmacol. 1999, 33, 652–658. [Google Scholar] [CrossRef]
- Maas, R.; Xanthakis, V.; Polak, J.F.; Schwedhelm, E.; Sullivan, L.M.; Benndorf, R.; Schulze, F.; Vasan, R.S.; Wolf, P.A.; Boger, R.H.; et al. Association of the endogenous nitric oxide synthase inhibitor ADMA with carotid artery intimal media thickness in the Framingham Heart Study offspring cohort. Stroke 2009, 40, 2715–2719. [Google Scholar] [CrossRef] [Green Version]
- Bai, Y.; Sun, L.; Du, L.; Zhang, T.; Xin, W.; Lan, X.; Du, G. Association of circulating levels of asymmetric dimethylarginine (ADMA) with carotid intima-media thickness: Evidence from 6168 participants. Ageing Res. Rev. 2013, 12, 699–707. [Google Scholar] [CrossRef]
- Sundar, U.M.; Ugusman, A.; Chua, H.K.; Latip, J.; Aminuddin, A. Piper sarmentosum Promotes Endothelial Nitric Oxide Production by Reducing Asymmetric Dimethylarginine in Tumor Necrosis Factor-alpha-Induced Human Umbilical Vein Endothelial Cells. Front. Pharmacol 2019, 10, 1033. [Google Scholar] [CrossRef] [Green Version]
- Arlouskaya, Y.; Sawicka, A.; Glowala, M.; Giebultowicz, J.; Korytowska, N.; Talalaj, M.; Nowicka, G.; Wrzosek, M. Asymmetric Dimethylarginine (ADMA) and Symmetric Dimethylarginine (SDMA) Concentrations in Patients with Obesity and the Risk of Obstructive Sleep Apnea (OSA). J. Clin. Med. 2019, 8, 897. [Google Scholar] [CrossRef] [Green Version]
- Hsu, C.P.; Zhao, J.F.; Lin, S.J.; Shyue, S.K.; Guo, B.C.; Lu, T.M.; Lee, T.S. Asymmetric Dimethylarginine Limits the Efficacy of Simvastatin Activating Endothelial Nitric Oxide Synthase. J. Am. Heart Assoc. 2016, 5, e003327. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Notsu, Y.; Yano, S.; Shibata, H.; Nagai, A.; Nabika, T. Plasma arginine/ADMA ratio as a sensitive risk marker for atherosclerosis: Shimane CoHRE study. Atherosclerosis 2015, 239, 61–66. [Google Scholar] [CrossRef] [PubMed]
- Boger, R.H.; Endres, H.G.; Schwedhelm, E.; Darius, H.; Atzler, D.; Luneburg, N.; von Stritzky, B.; Maas, R.; Thiem, U.; Benndorf, R.A.; et al. Asymmetric dimethylarginine as an independent risk marker for mortality in ambulatory patients with peripheral arterial disease. J. Intern. Med. 2011, 269, 349–361. [Google Scholar] [CrossRef] [PubMed]
- Pizzarelli, F.; Maas, R.; Dattolo, P.; Tripepi, G.; Michelassi, S.; D’Arrigo, G.; Mieth, M.; Bandinelli, S.; Ferrucci, L.; Zoccali, C. Asymmetric dimethylarginine predicts survival in the elderly. Age 2013, 35, 2465–2475. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Notsu, Y.; Nabika, T.; Bokura, H.; Suyama, Y.; Kobayashi, S.; Yamaguchi, S.; Masuda, J. Evaluation of asymmetric dimethylarginine and homocysteine in microangiopathy-related cerebral damage. Am. J. Hypertens. 2009, 22, 257–262. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McDonald, K.K.; Zharikov, S.; Block, E.R.; Kilberg, M.S. A caveolar complex between the cationic amino acid transporter 1 and endothelial nitric-oxide synthase may explain the “arginine paradox”. J. Biol. Chem. 1997, 272, 31213–31216. [Google Scholar] [CrossRef] [Green Version]
- Kim, J.A.; Montagnani, M.; Chandrasekran, S.; Quon, M.J. Role of lipotoxicity in endothelial dysfunction. Heart Fail. Clin. 2012, 8, 589–607. [Google Scholar] [CrossRef] [Green Version]
- Benowitz, N.L. Cigarette smoking and cardiovascular disease: Pathophysiology and implications for treatment. Prog. Cardiovasc. Dis. 2003, 46, 91–111. [Google Scholar] [CrossRef]
- Januzzi, J. Cardiac Biomarkers in Clinical Practice; Jones & Bartlett Learning: Burlington, MA, USA, 2009. [Google Scholar]
- Rohde, D.; Busch, M.; Volkert, A.; Ritterhoff, J.; Katus, H.A.; Peppel, K.; Most, P. Cardiomyocytes, endothelial cells and cardiac fibroblasts: S100A1’s triple action in cardiovascular pathophysiology. Future Cardiol. 2015, 11, 309–321. [Google Scholar] [CrossRef] [Green Version]
- Davies, P.F. Hemodynamic shear stress and the endothelium in cardiovascular pathophysiology. Nat. Clin. Pract. Cardiovasc. Med. 2009, 6, 16–26. [Google Scholar] [CrossRef] [Green Version]
- Santulli, G. microRNAs Distinctively Regulate Vascular Smooth Muscle and Endothelial Cells: Functional Implications in Angiogenesis, Atherosclerosis, and In-Stent Restenosis. Adv. Exp. Med. Biol. 2015, 887, 53–77. [Google Scholar] [PubMed] [Green Version]
- Foster, W.; Carruthers, D.; Lip, G.Y.; Blann, A.D. Relationships between endothelial, inflammatory and angiogenesis markers in rheumatoid arthritis: Implications for cardiovascular pathophysiology. Thromb. Res. 2009, 123, 659–664. [Google Scholar] [CrossRef] [PubMed]
- Ciccarelli, M.; Santulli, G.; Campanile, A.; Galasso, G.; Cervero, P.; Altobelli, G.G.; Cimini, V.; Pastore, L.; Piscione, F.; Trimarco, B.; et al. Endothelial alpha1-adrenoceptors regulate neo-angiogenesis. Br. J. Pharmacol. 2008, 153, 936–946. [Google Scholar] [CrossRef] [PubMed]
- Luksha, L.; Agewall, S.; Kublickiene, K. Endothelium-derived hyperpolarizing factor in vascular physiology and cardiovascular disease. Atherosclerosis 2009, 202, 330–344. [Google Scholar] [CrossRef]
- Santulli, G.; Cipolletta, E.; Sorriento, D.; Del Giudice, C.; Anastasio, A.; Monaco, S.; Maione, A.S.; Condorelli, G.; Puca, A.; Trimarco, B.; et al. CaMK4 Gene Deletion Induces Hypertension. J. Am. Heart Assoc. 2012, 1, e001081. [Google Scholar] [CrossRef] [Green Version]
- Deedwania, P.C. Diabetes is a vascular disease: The role of endothelial dysfunction in pathophysiology of cardiovascular disease in diabetes. Cardiol. Clin. 2004, 22, 505–509. [Google Scholar] [CrossRef]
- Sorriento, D.; Santulli, G.; Del Giudice, C.; Anastasio, A.; Trimarco, B.; Iaccarino, G. Endothelial cells are able to synthesize and release catecholamines both in vitro and in vivo. Hypertension 2012, 60, 129–136. [Google Scholar] [CrossRef] [Green Version]
- Li, J.M.; Shah, A.M. Endothelial cell superoxide generation: Regulation and relevance for cardiovascular pathophysiology. Am. J. Physiol. Regul. Integr. Comp. Physiol. 2004, 287, R1014–R1030. [Google Scholar] [CrossRef]
- Ciccarelli, M.; Cipolletta, E.; Santulli, G.; Campanile, A.; Pumiglia, K.; Cervero, P.; Pastore, L.; Astone, D.; Trimarco, B.; Iaccarino, G. Endothelial beta2 adrenergic signaling to AKT: Role of Gi and SRC. Cell Signal. 2007, 19, 1949–1955. [Google Scholar] [CrossRef]
- Sellke, F.W.; Boyle, E.M., Jr.; Verrier, E.D. Endothelial cell injury in cardiovascular surgery: The pathophysiology of vasomotor dysfunction. Ann. Thorac. Surg. 1996, 62, 1222–1228. [Google Scholar] [CrossRef]
- Iaccarino, G.; Ciccarelli, M.; Sorriento, D.; Galasso, G.; Campanile, A.; Santulli, G.; Cipolletta, E.; Cerullo, V.; Cimini, V.; Altobelli, G.G.; et al. Ischemic neoangiogenesis enhanced by beta2-adrenergic receptor overexpression: A novel role for the endothelial adrenergic system. Circ. Res. 2005, 97, 1182–1189. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ogita, H.; Liao, J. Endothelial function and oxidative stress. Endothelium 2004, 11, 123–132. [Google Scholar] [CrossRef] [PubMed]
- Skrypnyk, I.; Maslova, G.; Lymanets, T.; Gusachenko, I. L-arginine is an effective medication for prevention of endothelial dysfunction, a predictor of anthracycline cardiotoxicity in patients with acute leukemia. Exp. Oncol. 2017, 39, 308–311. [Google Scholar] [CrossRef]
- Ignarro, L.J.; Napoli, C. Novel features of nitric oxide, endothelial nitric oxide synthase, and atherosclerosis. Curr. Diab. Rep. 2005, 5, 17–23. [Google Scholar] [CrossRef]
- Nguyen, M.C.; Park, J.T.; Jeon, Y.G.; Jeon, B.H.; Hoe, K.L.; Kim, Y.M.; Lim, H.K.; Ryoo, S. Arginase Inhibition Restores Peroxynitrite-Induced Endothelial Dysfunction via L-Arginine-Dependent Endothelial Nitric Oxide Synthase Phosphorylation. Yonsei Med. J. 2016, 57, 1329–1338. [Google Scholar] [CrossRef] [Green Version]
- Wu, G.; Meininger, C.J. Arginine nutrition and cardiovascular function. J. Nutr. 2000, 130, 2626–2629. [Google Scholar] [CrossRef] [Green Version]
- Scaglia, F.; Brunetti-Pierri, N.; Kleppe, S.; Marini, J.; Carter, S.; Garlick, P.; Jahoor, F.; O’Brien, W.; Lee, B. Clinical consequences of urea cycle enzyme deficiencies and potential links to arginine and nitric oxide metabolism. J. Nutr. 2004, 134 (Suppl. 10), 2775S–2782S. [Google Scholar] [CrossRef]
- Luneburg, N.; Xanthakis, V.; Schwedhelm, E.; Sullivan, L.M.; Maas, R.; Anderssohn, M.; Riederer, U.; Glazer, N.L.; Vasan, R.S.; Boger, R.H. Reference intervals for plasma L-arginine and the L-arginine:asymmetric dimethylarginine ratio in the Framingham Offspring Cohort. J. Nutr. 2011, 141, 2186–2190. [Google Scholar] [CrossRef] [Green Version]
- Contreras, M.T.; Gallardo, M.J.; Betancourt, L.R.; Rada, P.V.; Ceballos, G.A.; Hernandez, L.E.; Hernandez, L.F. Correlation between plasma levels of arginine and citrulline in preterm and full-term neonates: Therapeutical implications. J. Clin. Lab. Anal. 2017, 31, e22134. [Google Scholar] [CrossRef]
- Fernandez Diaz-Rullo, F.; Zamberlan, F.; Mewis, R.E.; Fekete, M.; Broche, L.; Cheyne, L.A.; Dall’Angelo, S.; Duckett, S.B.; Dawson, D.; Zanda, M. Synthesis and hyperpolarisation of eNOS substrates for quantification of NO production by (1)H NMR spectroscopy. Bioorg. Med. Chem. 2017, 25, 2730–2742. [Google Scholar] [CrossRef] [Green Version]
- Schmidt, H.H.; Warner, T.D.; Ishii, K.; Sheng, H.; Murad, F. Insulin secretion from pancreatic B cells caused by L-arginine-derived nitrogen oxides. Science 1992, 255, 721–723. [Google Scholar] [CrossRef] [PubMed]
- Fajans, S.S.; Floyd, J.C., Jr.; Knopf, R.F.; Conn, F.W. Effect of amino acids and proteins on insulin secretion in man. Recent Prog. Horm. Res. 1967, 23, 617–662. [Google Scholar] [PubMed]
- Sener, A.; Best, L.C.; Yates, A.P.; Kadiata, M.M.; Olivares, E.; Louchami, K.; Jijakli, H.; Ladriere, L.; Malaisse, W.J. Stimulus-secretion coupling of arginine-induced insulin release: Comparison between the cationic amino acid and its methyl ester. Endocrine 2000, 13, 329–340. [Google Scholar] [CrossRef]
- Gerich, J.E.; Lorenzi, M.; Schneider, V.; Kwan, C.W.; Karam, J.H.; Guillemin, R.; Forsham, P.H. Inhibition of pancreatic glucagon responses to arginine by somatostatin in normal man and in insulin-dependent diabetics. Diabetes 1974, 23, 876–880. [Google Scholar] [CrossRef]
- Giugliano, D.; Marfella, R.; Verrazzo, G.; Acampora, R.; Coppola, L.; Cozzolino, D.; D’Onofrio, F. The vascular effects of L-Arginine in humans. The role of endogenous insulin. J. Clin. Investig. 1997, 99, 433–438. [Google Scholar] [CrossRef]
- Merimee, T.J.; Rabinowitz, D.; Riggs, L.; Burgess, J.A.; Rimoin, D.L.; McKusick, V.A. Plasma growth hormone after arginine infusion. Clinical experiences. N. Engl. J. Med. 1967, 276, 434–439. [Google Scholar] [CrossRef]
- Fryburg, D.A. NG-monomethyl-L-arginine inhibits the blood flow but not the insulin-like response of forearm muscle to IGF- I: Possible role of nitric oxide in muscle protein synthesis. J. Clin. Investig. 1996, 97, 1319–1328. [Google Scholar] [CrossRef] [Green Version]
- Bode-Boger, S.M.; Boger, R.H.; Loffler, M.; Tsikas, D.; Brabant, G.; Frolich, J.C. L-arginine stimulates NO-dependent vasodilation in healthy humans--effect of somatostatin pretreatment. J. Investig. Med. 1999, 47, 43–50. [Google Scholar]
- Taddei, S.; Virdis, A.; Mattei, P.; Ghiadoni, L.; Gennari, A.; Fasolo, C.B.; Sudano, I.; Salvetti, A. Aging and endothelial function in normotensive subjects and patients with essential hypertension. Circulation 1995, 91, 1981–1987. [Google Scholar] [CrossRef]
- Celermajer, D.S.; Sorensen, K.E.; Gooch, V.M.; Spiegelhalter, D.J.; Miller, O.I.; Sullivan, I.D.; Lloyd, J.K.; Deanfield, J.E. Non-invasive detection of endothelial dysfunction in children and adults at risk of atherosclerosis. Lancet 1992, 340, 1111–1115. [Google Scholar] [CrossRef]
- Gates, P.E.; Boucher, M.L.; Silver, A.E.; Monahan, K.D.; Seals, D.R. Impaired flow-mediated dilation with age is not explained by L-arginine bioavailability or endothelial asymmetric dimethylarginine protein expression. J. Appl. Physiol. 2007, 102, 63–71. [Google Scholar] [CrossRef] [PubMed]
- Campo, C.; Lahera, V.; Garcia-Robles, R.; Cachofeiro, V.; Alcazar, J.M.; Andres, A.; Rodicio, J.L.; Ruilope, L.M. Aging abolishes the renal response to L-arginine infusion in essential hypertension. Kidney Int. Suppl. 1996, 55, S126–S128. [Google Scholar] [PubMed]
- Blum, A.; Hathaway, L.; Mincemoyer, R.; Schenke, W.H.; Kirby, M.; Csako, G.; Waclawiw, M.A.; Panza, J.A.; Cannon, R.O., III. Effects of oral L-arginine on endothelium-dependent vasodilation and markers of inflammation in healthy postmenopausal women. J. Am. Coll. Cardiol. 2000, 35, 271–276. [Google Scholar] [CrossRef] [Green Version]
- Bode-Boger, S.M.; Muke, J.; Surdacki, A.; Brabant, G.; Boger, R.H.; Frolich, J.C. Oral L-arginine improves endothelial function in healthy individuals older than 70 years. Vasc. Med. 2003, 8, 77–81. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, P.Y.; St John, P.L.; Kirk, K.A.; Abrahamson, D.R.; Sanders, P.W. Hypertensive nephrosclerosis in the Dahl/Rapp rat. Initial sites of injury and effect of dietary L-arginine supplementation. Lab. Investig. 1993, 68, 174–184. [Google Scholar] [PubMed]
- Zhou, M.S.; Kosaka, H.; Tian, R.X.; Abe, Y.; Chen, Q.H.; Yoneyama, H.; Yamamoto, A.; Zhang, L. L-Arginine improves endothelial function in renal artery of hypertensive Dahl rats. J. Hypertens. 2001, 19, 421–429. [Google Scholar] [CrossRef]
- Fujii, S.; Zhang, L.; Igarashi, J.; Kosaka, H. L-arginine reverses p47phox and gp91phox expression induced by high salt in Dahl rats. Hypertension 2003, 42, 1014–1020. [Google Scholar] [CrossRef] [Green Version]
- Patel, A.; Layne, S.; Watts, D.; Kirchner, K.A. L-arginine administration normalizes pressure natriuresis in hypertensive Dahl rats. Hypertension 1993, 22, 863–869. [Google Scholar] [CrossRef] [Green Version]
- Chen, P.Y.; Sanders, P.W. L-arginine abrogates salt-sensitive hypertension in Dahl/Rapp rats. J. Clin. Investig. 1991, 88, 1559–1567. [Google Scholar] [CrossRef]
- Miyata, N.; Zou, A.P.; Mattson, D.L.; Cowley, A.W., Jr. Renal medullary interstitial infusion of L-arginine prevents hypertension in Dahl salt-sensitive rats. Am. J. Physiol. 1998, 275, R1667–R1673. [Google Scholar] [CrossRef]
- Ozcelikay, A.T.; Tay, A.; Guner, S.; Tasyaran, V.; Yildizoglu-Ari, N.; Dincer, U.D.; Altan, V.M. Reversal effects of L-arginine treatment on blood pressure and vascular responsiveness of streptozotocin-diabetic rats. Pharmacol. Res. 2000, 41, 201–209. [Google Scholar] [CrossRef] [PubMed]
- Tay, A.; Ozcelikay, A.T.; Altan, V.M. Effects of L-arginine on blood pressure and metabolic changes in fructose-hypertensive rats. Am. J. Hypertens. 2002, 15 Pt 1, 72–77. [Google Scholar] [CrossRef] [Green Version]
- Ono, H.; Ono, Y.; Frohlich, E.D. L-arginine reverses severe nephrosclerosis in aged spontaneously hypertensive rats. J. Hypertens. 1999, 17, 121–128. [Google Scholar] [CrossRef] [PubMed]
- Shan, L.; Wang, B.; Gao, G.; Cao, W.; Zhang, Y. L-Arginine supplementation improves antioxidant defenses through L-arginine/nitric oxide pathways in exercised rats. J. Appl. Physiol. 2013, 115, 1146–1155. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lin, W.T.; Yang, S.C.; Chen, K.T.; Huang, C.C.; Lee, N.Y. Protective effects of L-arginine on pulmonary oxidative stress and antioxidant defenses during exhaustive exercise in rats. Acta Pharmacol. Sin. 2005, 26, 992–999. [Google Scholar] [CrossRef] [PubMed]
- Huang, C.C.; Tsai, S.C.; Lin, W.T. Potential ergogenic effects of L-arginine against oxidative and inflammatory stress induced by acute exercise in aging rats. Exp. Gerontol. 2008, 43, 571–577. [Google Scholar] [CrossRef] [PubMed]
- de Nigris, F.; Lerman, L.O.; Ignarro, S.W.; Sica, G.; Lerman, A.; Palinski, W.; Ignarro, L.J.; Napoli, C. Beneficial effects of antioxidants and L-arginine on oxidation-sensitive gene expression and endothelial NO synthase activity at sites of disturbed shear stress. Proc. Natl. Acad. Sci. USA 2003, 100, 1420–1425. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ahmad, A.; Sattar, M.Z.; Rathore, H.A.; Hussain, A.I.; Khan, S.A.; Fatima, T.; Afzal, S.; Abdullah, N.A.; Johns, E.J. Antioxidant Activity and Free Radical Scavenging Capacity of L-Arginine and Nahs: A Comparative in Vitro Study. Acta Pol. Pharm. 2015, 72, 245–252. [Google Scholar]
- Wallner, S.; Hermetter, A.; Mayer, B.; Wascher, T.C. The alpha-amino group of L-arginine mediates its antioxidant effect. Eur. J. Clin. Investig. 2001, 31, 98–102. [Google Scholar] [CrossRef]
- Suliburska, J.; Bogdanski, P.; Krejpcio, Z.; Pupek-Musialik, D.; Jablecka, A. The effects of L-arginine, alone and combined with vitamin C, on mineral status in relation to its antidiabetic, anti-inflammatory, and antioxidant properties in male rats on a high-fat diet. Biol. Trace Elem. Res. 2014, 157, 67–74. [Google Scholar] [CrossRef] [Green Version]
- Zheng, P.; Yu, B.; He, J.; Tian, G.; Luo, Y.; Mao, X.; Zhang, K.; Che, L.; Chen, D. Protective effects of dietary arginine supplementation against oxidative stress in weaned piglets. Br. J. Nutr. 2013, 109, 2253–2260. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fazelian, S.; Hoseini, M.; Namazi, N.; Heshmati, J.; Sepidar Kish, M.; Mirfatahi, M.; Some Olia, A.S. Effects of L-Arginine Supplementation on Antioxidant Status and Body Composition in Obese Patients with Pre-diabetes: A Randomized Controlled Clinical Trial. Adv. Pharm. Bull. 2014, 4 (Suppl. 1), 449–454. [Google Scholar] [PubMed]
- Wascher, T.C.; Posch, K.; Wallner, S.; Hermetter, A.; Kostner, G.M.; Graier, W.F. Vascular effects of L-arginine: Anything beyond a substrate for the NO-synthase? Biochem Biophys Res. Commun 1997, 234, 35–38. [Google Scholar] [CrossRef] [PubMed]
- Lekakis, J.P.; Papathanassiou, S.; Papaioannou, T.G.; Papamichael, C.M.; Zakopoulos, N.; Kotsis, V.; Dagre, A.G.; Stamatelopoulos, K.; Protogerou, A.; Stamatelopoulos, S.F. Oral L-arginine improves endothelial dysfunction in patients with essential hypertension. Int. J. Cardiol. 2002, 86, 317–323. [Google Scholar] [CrossRef]
- Higashi, Y.; Oshima, T.; Watanabe, M.; Matsuura, H.; Kajiyama, G. Renal response to L-arginine in salt-sensitive patients with essential hypertension. Hypertension 1996, 27 Pt 2, 643–648. [Google Scholar] [CrossRef]
- Campese, V.M.; Amar, M.; Anjali, C.; Medhat, T.; Wurgaft, A. Effect of L-arginine on systemic and renal haemodynamics in salt-sensitive patients with essential hypertension. J. Hum. Hypertens 1997, 11, 527–532. [Google Scholar] [CrossRef] [Green Version]
- Pezza, V.; Bernardini, F.; Pezza, E.; Pezza, B.; Curione, M. Study of supplemental oral l-arginine in hypertensives treated with enalapril + hydrochlorothiazide. Am. J. Hypertens 1998, 11, 1267–1270. [Google Scholar]
- Higashi, Y.; Oshima, T.; Ono, N.; Hiraga, H.; Yoshimura, M.; Watanabe, M.; Matsuura, H.; Kambe, M.; Kajiyama, G. Intravenous administration of L-arginine inhibits angiotensin-converting enzyme in humans. J. Clin. Endocrinol. Metab. 1995, 80, 2198–2202. [Google Scholar]
- De Caterina, R.; Libby, P.; Peng, H.B.; Thannickal, V.J.; Rajavashisth, T.B.; Gimbrone, M.A., Jr.; Shin, W.S.; Liao, J.K. Nitric oxide decreases cytokine-induced endothelial activation. Nitric oxide selectively reduces endothelial expression of adhesion molecules and proinflammatory cytokines. J. Clin. Investig. 1995, 96, 60–68. [Google Scholar] [CrossRef]
- Sperone, A.; Dryden, N.H.; Birdsey, G.M.; Madden, L.; Johns, M.; Evans, P.C.; Mason, J.C.; Haskard, D.O.; Boyle, J.J.; Paleolog, E.M.; et al. The transcription factor Erg inhibits vascular inflammation by repressing NF-kappaB activation and proinflammatory gene expression in endothelial cells. Arterioscler. Thromb. Vasc. Biol. 2011, 31, 142–150. [Google Scholar] [CrossRef] [Green Version]
- Gambardella, J.; Santulli, G. Integrating diet and inflammation to calculate cardiovascular risk. Atherosclerosis 2016, 253, 258–261. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Huo, Y.; Ley, K. Adhesion molecules and atherogenesis. Acta Physiol. Scand. 2001, 173, 35–43. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Blum, A.; Miller, H.; Blum, A.; Miller, H. The effects of L-arginine on atherosclerosis and heart disease. Int. J. Cardiovasc. Intervent. 1999, 2, 97–100. [Google Scholar] [CrossRef] [PubMed]
- Adams, M.R.; Jessup, W.; Hailstones, D.; Celermajer, D.S. L-arginine reduces human monocyte adhesion to vascular endothelium and endothelial expression of cell adhesion molecules. Circulation 1997, 95, 662–668. [Google Scholar] [CrossRef]
- Adams, M.R.; McCredie, R.; Jessup, W.; Robinson, J.; Sullivan, D.; Celermajer, D.S. Oral L-arginine improves endothelium-dependent dilatation and reduces monocyte adhesion to endothelial cells in young men with coronary artery disease. Atherosclerosis 1997, 129, 261–269. [Google Scholar] [CrossRef]
- Ceremuzynski, L.; Chamiec, T.; Herbaczynska-Cedro, K. Effect of supplemental oral L-arginine on exercise capacity in patients with stable angina pectoris. Am. J. Cardiol. 1997, 80, 331–333. [Google Scholar] [CrossRef]
- Lerman, A.; Burnett, J.C., Jr.; Higano, S.T.; McKinley, L.J.; Holmes, D.R., Jr. Long-term L-arginine supplementation improves small-vessel coronary endothelial function in humans. Circulation 1998, 97, 2123–2128. [Google Scholar] [CrossRef] [Green Version]
- Chen, C.; Mattar, S.G.; Lumsden, A.B. Oral administration of L-arginine reduces intimal hyperplasia in balloon-injured rat carotid arteries. J. Surg. Res. 1999, 82, 17–23. [Google Scholar] [CrossRef]
- Yin, W.H.; Chen, J.W.; Tsai, C.; Chiang, M.C.; Young, M.S.; Lin, S.J. L-arginine improves endothelial function and reduces LDL oxidation in patients with stable coronary artery disease. Clin. Nutr. 2005, 24, 988–997. [Google Scholar] [CrossRef]
- Walker, H.A.; McGing, E.; Fisher, I.; Boger, R.H.; Bode-Boger, S.M.; Jackson, G.; Ritter, J.M.; Chowienczyk, P.J. Endothelium-dependent vasodilation is independent of the plasma L-arginine/ADMA ratio in men with stable angina: Lack of effect of oral L-arginine on endothelial function, oxidative stress and exercise performance. J. Am. Coll. Cardiol. 2001, 38, 499–505. [Google Scholar] [CrossRef] [Green Version]
- Padilla, F.; Garcia-Dorado, D.; Agullo, L.; Inserte, J.; Paniagua, A.; Mirabet, S.; Barrabes, J.A.; Ruiz-Meana, M.; Soler-Soler, J. L-Arginine administration prevents reperfusion-induced cardiomyocyte hypercontracture and reduces infarct size in the pig. Cardiovasc. Res. 2000, 46, 412–420. [Google Scholar] [CrossRef] [Green Version]
- Rector, T.S.; Bank, A.J.; Mullen, K.A.; Tschumperlin, L.K.; Sih, R.; Pillai, K.; Kubo, S.H. Randomized, double-blind, placebo-controlled study of supplemental oral L-arginine in patients with heart failure. Circulation 1996, 93, 2135–2141. [Google Scholar] [CrossRef] [PubMed]
- Bednarz, B.; Jaxa-Chamiec, T.; Gebalska, J.; Herbaczynska-Cedro, K.; Ceremuzynski, L. L-arginine supplementation prolongs exercise capacity in congestive heart failure. Kardiol. Pol. 2004, 60, 348–353. [Google Scholar] [PubMed]
- Rodrigues-Krause, J.; Krause, M.; Rocha, I.; Umpierre, D.; Fayh, A.P.T. Association of l-Arginine Supplementation with Markers of Endothelial Function in Patients with Cardiovascular or Metabolic Disorders: A Systematic Review and Meta-Analysis. Nutrients 2018, 11, 15. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hambrecht, R.; Hilbrich, L.; Erbs, S.; Gielen, S.; Fiehn, E.; Schoene, N.; Schuler, G. Correction of endothelial dysfunction in chronic heart failure: Additional effects of exercise training and oral L-arginine supplementation. J. Am. Coll. Cardiol. 2000, 35, 706–713. [Google Scholar] [CrossRef] [Green Version]
- Weyrich, A.S.; Ma, X.L.; Lefer, A.M. The role of L-arginine in ameliorating reperfusion injury after myocardial ischemia in the cat. Circulation 1992, 86, 279–288. [Google Scholar] [CrossRef] [Green Version]
- Huk, I.; Nanobashvili, J.; Orljanski, W.; Neumayer, C.; Punz, A.; Holzaepfel, A.; Fuegl, A.; Mittlboeck, M.; Polterauer, P.; Roth, E. L-arginine treatment in ischemia/reperfusion injury. Cas. Lek. Cesk. 1998, 137, 496–499. [Google Scholar]
- Takeuchi, K.; McGowan, F.X.; Danh, H.C.; Glynn, P.; Simplaceanu, E.; del Nido, P.J. Direct detrimental effects of L-arginine upon ischemia--reperfusion injury to myocardium. J. Mol. Cell Cardiol. 1995, 27, 1405–1414. [Google Scholar] [CrossRef]
- Kubo, S.H.; Rector, T.S.; Bank, A.J.; Williams, R.E.; Heifetz, S.M. Endothelium-dependent vasodilation is attenuated in patients with heart failure. Circulation 1991, 84, 1589–1596. [Google Scholar] [CrossRef] [Green Version]
- Hirooka, Y.; Imaizumi, T.; Tagawa, T.; Shiramoto, M.; Endo, T.; Ando, S.; Takeshita, A. Effects of L-arginine on impaired acetylcholine-induced and ischemic vasodilation of the forearm in patients with heart failure. Circulation 1994, 90, 658–668. [Google Scholar] [CrossRef] [Green Version]
- Doutreleau, S.; Mettauer, B.; Piquard, F.; Rouyer, O.; Schaefer, A.; Lonsdorfer, J.; Geny, B. Chronic L-arginine supplementation enhances endurance exercise tolerance in heart failure patients. Int. J. Sports Med. 2006, 27, 567–572. [Google Scholar] [CrossRef] [PubMed]
- Parnell, M.M.; Holst, D.P.; Kaye, D.M. Augmentation of endothelial function following exercise training is associated with increased L-arginine transport in human heart failure. Clin. Sci. 2005, 109, 523–530. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chin-Dusting, J.P.; Kaye, D.M.; Lefkovits, J.; Wong, J.; Bergin, P.; Jennings, G.L. Dietary supplementation with L-arginine fails to restore endothelial function in forearm resistance arteries of patients with severe heart failure. J. Am. Coll. Cardiol. 1996, 27, 1207–1213. [Google Scholar] [CrossRef] [Green Version]
- Schulman, S.P.; Becker, L.C.; Kass, D.A.; Champion, H.C.; Terrin, M.L.; Forman, S.; Ernst, K.V.; Kelemen, M.D.; Townsend, S.N.; Capriotti, A.; et al. L-arginine therapy in acute myocardial infarction: The Vascular Interaction With Age in Myocardial Infarction (VINTAGE MI) randomized clinical trial. JAMA 2006, 295, 58–64. [Google Scholar] [CrossRef] [Green Version]
- Shu, J.; Santulli, G. Update on peripheral artery disease: Epidemiology and evidence-based facts. Atherosclerosis 2018, 275, 379–381. [Google Scholar] [CrossRef]
- Azab, S.M.; Zamzam, A.; Syed, M.H.; Abdin, R.; Qadura, M.; Britz-McKibbin, P. Serum Metabolic Signatures of Chronic Limb-Threatening Ischemia in Patients with Peripheral Artery Disease. J. Clin. Med. 2020, 9, 1877. [Google Scholar] [CrossRef]
- Misra, S.; Shishehbor, M.H.; Takahashi, E.A.; Aronow, H.D.; Brewster, L.P.; Bunte, M.C.; Kim, E.S.H.; Lindner, J.R.; Rich, K.; American Heart Association Council on Peripheral Vascular Disease; et al. Perfusion Assessment in Critical Limb Ischemia: Principles for Understanding and the Development of Evidence and Evaluation of Devices: A Scientific Statement From the American Heart Association. Circulation 2019, 140, e657–e672. [Google Scholar] [CrossRef] [Green Version]
- Boger, R.H.; Bode-Boger, S.M.; Thiele, W.; Junker, W.; Alexander, K.; Frolich, J.C. Biochemical evidence for impaired nitric oxide synthesis in patients with peripheral arterial occlusive disease. Circulation 1997, 95, 2068–2074. [Google Scholar] [CrossRef] [Green Version]
- Maxwell, A.J.; Cooke, J.P. Cardiovascular effects of L-arginine. Curr. Opin. Nephrol. Hypertens. 1998, 7, 63–70. [Google Scholar] [CrossRef]
- Maxwell, A.J.; Anderson, B.E.; Cooke, J.P. Nutritional therapy for peripheral arterial disease: A double-blind, placebo-controlled, randomized trial of HeartBar. Vasc. Med. 2000, 5, 11–19. [Google Scholar]
- Wilson, A.M.; Harada, R.; Nair, N.; Balasubramanian, N.; Cooke, J.P. L-arginine supplementation in peripheral arterial disease: No benefit and possible harm. Circulation 2007, 116, 188–195. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Avogaro, A.; Albiero, M.; Menegazzo, L.; de Kreutzenberg, S.; Fadini, G.P. Endothelial dysfunction in diabetes: The role of reparatory mechanisms. Diabetes Care 2011, 34 (Suppl. 2), S285–S290. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sena, C.M.; Pereira, A.M.; Seica, R. Endothelial dysfunction—A major mediator of diabetic vascular disease. Biochim. Biophys. Acta 2013, 1832, 2216–2231. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bogdanski, P.; Suliburska, J.; Grabanska, K.; Musialik, K.; Cieslewicz, A.; Skoluda, A.; Jablecka, A. Effect of 3-month L-arginine supplementation on insulin resistance and tumor necrosis factor activity in patients with visceral obesity. Eur. Rev. Med. Pharmacol. Sci. 2012, 16, 816–823. [Google Scholar]
- Eid, H.M.; Reims, H.; Arnesen, H.; Kjeldsen, S.E.; Lyberg, T.; Seljeflot, I. Decreased levels of asymmetric dimethylarginine during acute hyperinsulinemia. Metabolism 2007, 56, 464–469. [Google Scholar] [CrossRef]
- Sobrevia, L.; Nadal, A.; Yudilevich, D.L.; Mann, G.E. Activation of L-arginine transport (system y+) and nitric oxide synthase by elevated glucose and insulin in human endothelial cells. J. Physiol. 1996, 490 Pt 3, 775–781. [Google Scholar] [CrossRef] [Green Version]
- Mann, G.E.; Yudilevich, D.L.; Sobrevia, L. Regulation of amino acid and glucose transporters in endothelial and smooth muscle cells. Physiol. Rev. 2003, 83, 183–252. [Google Scholar] [CrossRef]
- Lembo, G.; Iaccarino, G.; Vecchione, C.; Barbato, E.; Morisco, C.; Monti, F.; Parrella, L.; Trimarco, B. Insulin enhances endothelial alpha2-adrenergic vasorelaxation by a pertussis toxin mechanism. Hypertension 1997, 30, 1128–1134. [Google Scholar] [CrossRef]
- Zeng, G.; Nystrom, F.H.; Ravichandran, L.V.; Cong, L.N.; Kirby, M.; Mostowski, H.; Quon, M.J. Roles for insulin receptor, PI3-kinase, and Akt in insulin-signaling pathways related to production of nitric oxide in human vascular endothelial cells. Circulation 2000, 101, 1539–1545. [Google Scholar] [CrossRef] [Green Version]
- Vecchione, C.; Aretini, A.; Maffei, A.; Marino, G.; Selvetella, G.; Poulet, R.; Trimarco, V.; Frati, G.; Lembo, G. Cooperation between insulin and leptin in the modulation of vascular tone. Hypertension 2003, 42, 166–170. [Google Scholar] [CrossRef] [Green Version]
- Scherrer, U.; Randin, D.; Vollenweider, P.; Vollenweider, L.; Nicod, P. Nitric oxide release accounts for insulin’s vascular effects in humans. J. Clin. Investig. 1994, 94, 2511–2515. [Google Scholar] [CrossRef] [PubMed]
- Iaccarino, G.; Ciccarelli, M.; Sorriento, D.; Cipolletta, E.; Cerullo, V.; Iovino, G.L.; Paudice, A.; Elia, A.; Santulli, G.; Campanile, A.; et al. AKT participates in endothelial dysfunction in hypertension. Circulation 2004, 109, 2587–2593. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Muniyappa, R.; Montagnani, M.; Koh, K.K.; Quon, M.J. Cardiovascular actions of insulin. Endocr. Rev. 2007, 28, 463–491. [Google Scholar] [CrossRef] [PubMed]
- Pieper, G.M.; Siebeneich, W.; Dondlinger, L.A. Short-term oral administration of L-arginine reverses defective endothelium-dependent relaxation and cGMP generation in diabetes. Eur. J. Pharmacol. 1996, 317, 317–320. [Google Scholar] [CrossRef]
- Khaidar, A.; Marx, M.; Lubec, B.; Lubec, G. L-arginine reduces heart collagen accumulation in the diabetic db/db mouse. Circulation 1994, 90, 479–483. [Google Scholar] [CrossRef] [Green Version]
- Lubec, G.; Bartosch, B.; Mallinger, R.; Adamiker, D.; Graef, I.; Frisch, H.; Hoger, H. The effect of substance L on glucose-mediated cross-links of collagen in the diabetic db/db mouse. Nephron 1990, 56, 281–284. [Google Scholar] [CrossRef]
- Lubec, B.; Hayn, M.; Kitzmuller, E.; Vierhapper, H.; Lubec, G. L-Arginine reduces lipid peroxidation in patients with diabetes mellitus. Free Radic. Biol. Med. 1997, 22, 355–357. [Google Scholar] [CrossRef]
- Pieper, G.M. Review of alterations in endothelial nitric oxide production in diabetes: Protective role of arginine on endothelial dysfunction. Hypertension 1998, 31, 1047–1060. [Google Scholar] [CrossRef] [Green Version]
- De Pirro, R.; Tamburrano, G.; Fusco, A.; Lauro, R. Arginine does not influence insulin binding on circulating monocytes. Endokrinologie 1980, 75, 243–246. [Google Scholar]
- Wascher, T.C.; Graier, W.F.; Dittrich, P.; Hussain, M.A.; Bahadori, B.; Wallner, S.; Toplak, H. Effects of low-dose L-arginine on insulin-mediated vasodilatation and insulin sensitivity. Eur. J. Clin. Investig. 1997, 27, 690–695. [Google Scholar] [CrossRef]
- Piatti, P.M.; Monti, L.D.; Valsecchi, G.; Magni, F.; Setola, E.; Marchesi, F.; Galli-Kienle, M.; Pozza, G.; Alberti, K.G. Long-term oral L-arginine administration improves peripheral and hepatic insulin sensitivity in type 2 diabetic patients. Diabetes Care 2001, 24, 875–880. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Huynh, N.T.; Tayek, J.A. Oral arginine reduces systemic blood pressure in type 2 diabetes: Its potential role in nitric oxide generation. J. Am. Coll. Nutr. 2002, 21, 422–427. [Google Scholar] [CrossRef] [PubMed]
- Lai, Y.L.; Aoyama, S.; Nagai, R.; Miyoshi, N.; Ohshima, H. Inhibition of L-arginine metabolizing enzymes by L-arginine-derived advanced glycation end products. J. Clin. Biochem. Nutr. 2010, 46, 177–185. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fiory, F.; Lombardi, A.; Miele, C.; Giudicelli, J.; Beguinot, F.; Van Obberghen, E. Methylglyoxal impairs insulin signalling and insulin action on glucose-induced insulin secretion in the pancreatic beta cell line INS-1E. Diabetologia 2011, 54, 2941–2952. [Google Scholar] [CrossRef] [Green Version]
- Polykretis, P.; Luchinat, E.; Boscaro, F.; Banci, L. Methylglyoxal interaction with superoxide dismutase 1. Redox Biol. 2020, 30, 101421. [Google Scholar] [CrossRef]
- Martina, V.; Masha, A.; Gigliardi, V.R.; Brocato, L.; Manzato, E.; Berchio, A.; Massarenti, P.; Settanni, F.; Della Casa, L.; Bergamini, S.; et al. Long-term N-acetylcysteine and L-arginine administration reduces endothelial activation and systolic blood pressure in hypertensive patients with type 2 diabetes. Diabetes Care 2008, 31, 940–944. [Google Scholar] [CrossRef] [Green Version]
- Deveaux, A.; Fouillet, H.; Petzke, K.J.; Hermier, D.; Andre, E.; Bunouf, P.; Lantoine-Adam, F.; Benamouzig, R.; Mathe, V.; Huneau, J.F.; et al. A Slow-Compared with a Fast-Release Form of Oral Arginine Increases Its Utilization for Nitric Oxide Synthesis in Overweight Adults with Cardiometabolic Risk Factors in a Randomized Controlled Study. J. Nutr. 2016, 146, 1322–1329. [Google Scholar] [CrossRef] [Green Version]
Figure 1.
Functional role of arginine in the synthesis of nitric oxide (NO). NADPH: nicotinamide adenine dinucleotide phosphate; eNOS: endothelial NO synthase.
Figure 1.
Functional role of arginine in the synthesis of nitric oxide (NO). NADPH: nicotinamide adenine dinucleotide phosphate; eNOS: endothelial NO synthase.

Figure 2.
Functional role of arginine in endothelial (dys)function. ADMA: asymmetric dimethylarginine; Arg: arginine; BH2: 7,8-dihydrobiopterin; BH4: tetrahydrobiopterin; CAT: cationic amino acid transporter; Citr: citrulline; NADPH: nicotinamide adenine dinucleotide phosphate; NO: nitric oxide; NOS: NO synthase.
Figure 2.
Functional role of arginine in endothelial (dys)function. ADMA: asymmetric dimethylarginine; Arg: arginine; BH2: 7,8-dihydrobiopterin; BH4: tetrahydrobiopterin; CAT: cationic amino acid transporter; Citr: citrulline; NADPH: nicotinamide adenine dinucleotide phosphate; NO: nitric oxide; NOS: NO synthase.

© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Gambardella, J.; Khondkar, W.; Morelli, M.B.; Wang, X.; Santulli, G.; Trimarco, V. Arginine and Endothelial Function. Biomedicines 2020, 8, 277. https://doi.org/10.3390/biomedicines8080277
AMA Style
Gambardella J, Khondkar W, Morelli MB, Wang X, Santulli G, Trimarco V. Arginine and Endothelial Function. Biomedicines. 2020; 8(8):277. https://doi.org/10.3390/biomedicines8080277
Chicago/Turabian StyleGambardella, Jessica, Wafiq Khondkar, Marco Bruno Morelli, Xujun Wang, Gaetano Santulli, and Valentina Trimarco. 2020. "Arginine and Endothelial Function" Biomedicines 8, no. 8: 277. https://doi.org/10.3390/biomedicines8080277
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.